
Abstract
Objectives
Louisiana extended Medicaid coverage on July 1, 2016, to previously ineligible populations. We aimed to estimate the effect of Louisiana’s Medicaid expansion on self-reported affordability of health care.
Methods
We used 2011-2019 data from the Behavioral Risk Factor Surveillance System (BRFSS). The BRFSS measured affordability of health care by asking respondents 2 questions: (1) whether they could not see a doctor due to cost in the previous 12 months and (2) whether they could not get a prescribed medication due to cost in the previous 12 months. We estimated difference-in-differences and difference-in-difference-in-differences analytical models using multivariable linear regression that compared trends in Louisiana with trends in states that did not expand Medicaid during the study period.
Results
Compared with adults aged <65 with annual household income >138% of the federal poverty level (FPL) in nonexpansion states, Medicaid expansion in Louisiana decreased the percentage of adults aged <65 with annual household income ≤138% FPL who reported being unable to see a doctor due to cost by 5.1 percentage points (95% CI, −6.5 to −3.6; P < .001) and unable to afford prescribed medication by 7.9 percentage points (95% CI, −9.2 to −6.6; P < .001). We found similar estimates when we limited the comparison group to Southern nonexpansion states.
Conclusions
Louisiana’s Medicaid expansion lowered cost barriers to health care. Further research may find improvements in health care affordability in states that have not yet expanded Medicaid.
Enacted in 2010, the Affordable Care Act provided support for states to expand their Medicaid benefits to provide health insurance coverage for residents whose annual household income was ≤138% of the federal poverty level (FPL), regardless of age, parental status, or disability status. 1 On July 1, 2016, Louisiana implemented Medicaid expansion to cover the low-income, uninsured population aged <65. After Medicaid expansion, during fiscal year 2016-2017, 38.3% of Louisiana residents were enrolled in Medicaid, and the overall number of enrollees had increased by 11.7% from the previous fiscal year, from 1.6 million to 1.8 million, largely because of Medicaid expansion. 2,3
This expansion of health insurance coverage is expected to translate into better affordability of health care services, because health insurance coverage has been found to be significantly associated with a reduction in challenges to health care affordability. 4 -9 Millions of adults have gained health insurance coverage, increased their use of health services, seen improvements in health care quality, and reported better health at the national and state levels under the Affordable Care Act Medicaid expansion. 7,8,10 -13 Consistent with significant declines in the percentage of the population who lack health insurance, the access to and affordability of health care improved. However, a comparison of early adopting states and nonexpansion states showed that although Medicaid expansion had no significant effect immediately after Medicaid expansion, 7,8 it did have a significant lagged effect on affordability. 11,14 The measurement of affordability in these studies was based on survey questions referring to the previous 12 months. The length of this retrospective period may attenuate the associations of early Medicaid expansion with affordability. Recent studies further demonstrated a positive effect of Medicaid expansion on affordability of health care at the national level. 15 -17 Generally, Medicaid expansion has expanded health insurance coverage and improved access to and affordability of health care at the national level.
Although previous research evaluated the effect of Medicaid expansion across states on various measures of affordability, most research focused on states that expanded Medicaid in 2014 and included all expansion states in the treatment group. Less research has assessed such expansion in individual states; results of a study of a single state may differ from results of a study of all expansion states. Therefore, our study aimed to evaluate the effect of Louisiana’s Medicaid expansion on the affordability of health care. To our knowledge, our study is the first to evaluate the effect of Louisiana’s Medicaid expansion on health care affordability by using nonexpansion states in the South as a comparison group. This comparison group is especially important because these states generally have a high percentage of low-income and uninsured residents in their populations, and these factors are important in extrapolating the effect of Medicaid expansion. As of January 2021, 9 of the 14 states that had not expanded Medicaid are in the South (a US Census Bureau–defined region), and policy makers continue to debate whether to implement Medicaid expansion in this region. 18,19
Methods
Our study explored the causal association between Louisiana’s Medicaid expansion and improvement in health care affordability by using difference-in-differences (DD) and difference-in-difference-in-differences (DDD) models. In addition to comparing Louisiana’s experience with all 17 nonexpansion states (as of December 2019), we also compared Louisiana with a group of nonexpansion states in the South because their geographic and socioeconomic characteristics are similar to those of Louisiana.
We used data from the Behavioral Risk Factor Surveillance System (BRFSS) from 2011 through 2019. The BRFSS is a telephone survey that collects data on health-related risk behaviors, health insurance coverage, health care access, chronic health conditions, and use of preventive services, covering the 50 states and the District of Columbia. 20 The BRFSS is a repeated, cross-sectional survey that does not follow individual respondents from wave to wave.
This study included respondents aged ≥18 in Louisiana and 17 states (Alabama, Florida, Georgia, Idaho, Kansas, Mississippi, Missouri, Nebraska, North Carolina, Oklahoma, South Carolina, South Dakota, Tennessee, Texas, Utah, Wisconsin, and Wyoming) that had not implemented Medicaid expansion as of December 2019. We treated 2 states (Missouri, Oklahoma) that had adopted but not implemented Medicaid expansion as nonexpansion states. Nine of the nonexpansion states included in our study are in the South: Alabama, Florida, Georgia, Mississippi, North Carolina, Oklahoma, South Carolina, Tennessee, and Texas. We limited our main sample to respondents aged <65 with annual household income ≤138% FPL. To comprehensively evaluate the effect of Louisiana Medicaid expansion, we also included 2 expanded samples: one with respondents aged <65 and a second with respondents who self-reported an annual household income ≤138% FPL. The BRFSS reports annual household income in prespecified ranges; we then assigned each respondent an income equal to the midpoint of the income range reported by the survey. Previous studies used this midpoint method to assess the effect of Medicaid expansion when using BRFSS data. 21 We calculated household size following BRFSS guidelines. 22 We compared the resulting fraction with annual federal poverty guidelines to calculate the respondent’s FPL. This process is described elsewhere. 6,23
Outcome Variables
Our study had 2 primary outcomes in health care affordability, measured by using responses from 2 survey questions asked in the BRFSS: (1) “Was there a time in the past 12 months when you needed to see a doctor but could not because of cost?” and (2) “Was there a time in the past 12 months when you did not take your medication as prescribed because of cost?” We then coded these 2 outcomes as dummy variables: “could not see a doctor due to cost” and “could not get prescribed medicine due to cost.” The BRFSS asked the question about doctor-related cost barriers annually, but it asked the question about medicine-related cost barriers only in 2013, 2014, 2016, 2017, and 2018. We included 2011-2019 surveys for the first outcome and surveys from 2013, 2014, 2016, and 2018 for the second outcome; we did not use 2017 BRFSS data on medicine-related cost barriers because <10% of respondents in Louisiana answered the question in that year.
Statistical Analysis
First, we used a DD analytical model to compare changes in outcomes between respondents in Louisiana versus nonexpansion states before and after Louisiana Medicaid expansion, in July 2016. A similar approach has been widely used in previous studies of Medicaid expansion. 6 -8,11,12,15,16 To match trends more finely between Louisiana and our control unit, we divided the data into 18 half-year time units spanning January–June and July–December of each year. We coded periods before July 2017 as preperiod and periods starting with the second half of 2017 (July–December) as postperiod. We used a multivariable linear regression to analyze each defined outcome, controlling for individual- and state-level factors:

The valid estimates of Louisiana Medicaid expansion effects using the DD model rely on the assumption of parallel trends. Although the parallel trend assumption cannot be directly tested, we indirectly tested the assumption by using an event-study analysis, which estimates a set of interaction terms between dummy variables for each relative-time unit and a dummy variable of the expansion state. 6,26,29 The parallel trends assumption would be satisfied if there were no significant coefficients during the preperiod. We also conducted 2 falsification tests for the DD model using samples that should not experience the effects of Medicaid expansion, respondents with annual household income ≥400% FPL and respondents aged ≥65.
To obtain the causal estimates of effects of Medicaid expansion in Louisiana, we then adopted an alternative model that did not rely on assumptions of parallel trends across states using a DDD model. 25,30 The principal advantage of this model is that it allowed us to specify state-by-time fixed effects that absorb any nonparallel trends at the state level. Medicaid expansion affected residents only in Louisiana (first difference) after mid-2016 (second difference) with annual household income ≤138% FPL (third difference). To make residents more comparable across the 138% FPL threshold, we restricted the comparison sample to respondents with an annual household income <400% FPL. We also used an alternative DDD model that used state, year, and whether the respondent was aged <65 as the third difference. Respondents aged ≥65 are eligible for Medicare and are not expected to experience the effects of Medicaid expansion.
We weighted all estimates using the final survey weights to account for the survey design and nonresponse to the survey. SEs were clustered at the state level in both DD and DDD models to allow for arbitrary within-state correlations in error terms. We excluded from analysis respondents with any missing data for outcome and control variables. We considered effects with P values < .05 using a 2-tailed hypothesis test to be significant. We followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) reporting guideline. 31 We performed all analyses using Stata version 15.1 (StataCorp LLC).
Results
The unadjusted percentage of people who could not see a doctor due to cost in Louisiana declined from 41.0% in 2011 to 24.1% in 2019 (Figure 1). This decline was larger than the decline (42.9% to 34.5%) in nonexpansion states. We also found a decline in the percentage of people who could not get prescribed medicine due to cost in Louisiana, from 28.1% in 2013 to 16.6% in 2018. However, the trends fluctuated slightly in both percentages of affordability of a doctor and affordability of prescribed medicine in Louisiana, whereas trends in nonexpansion states were relatively stable before July 2016. The unadjusted trends between Louisiana and nonexpansion states were not parallel before July 2016.
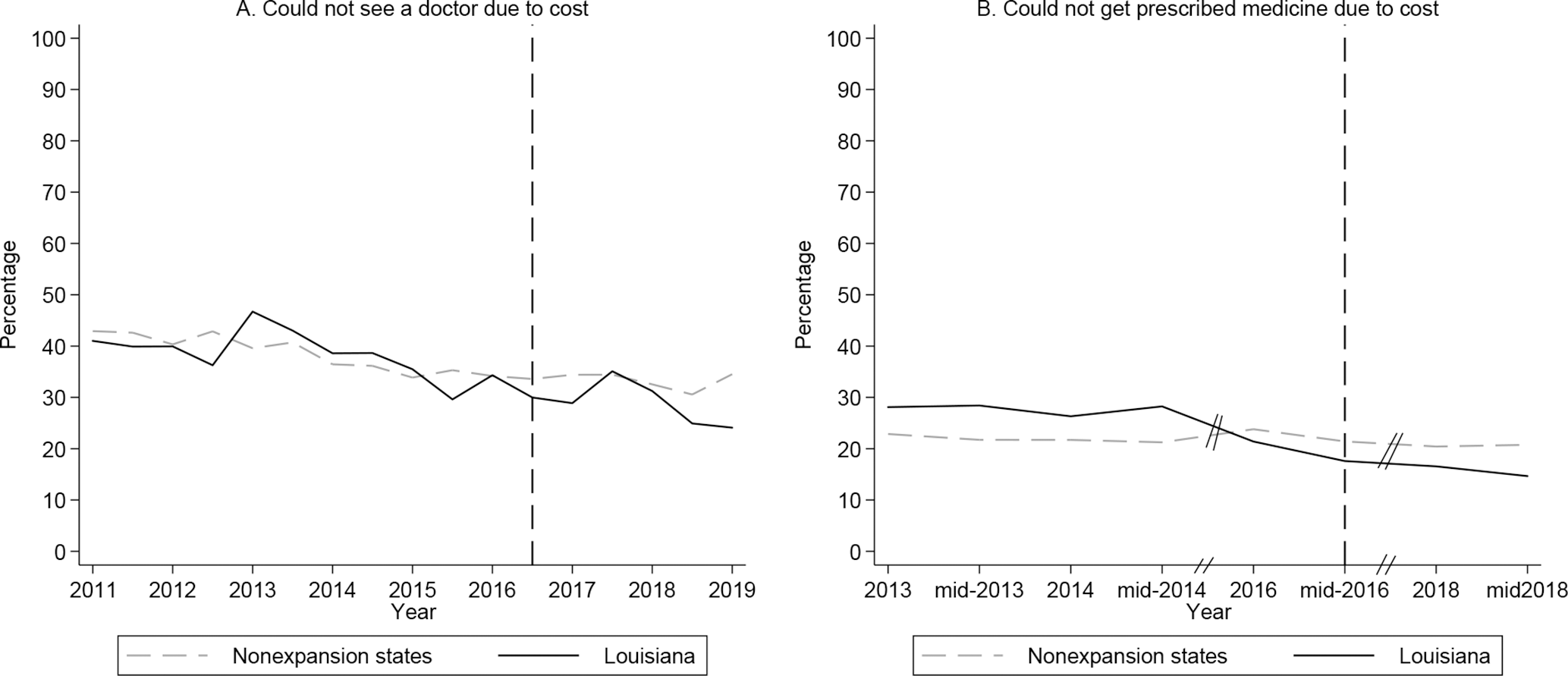
Unadjusted percentages of outcomes among adults aged <65 with annual household income ≤138% of the federal poverty level, by Medicaid expansion status, Behavioral Risk Factor Surveillance System (BRFSS), 2011-2019. 20 Nonexpansion states include Alabama, Florida, Georgia, Idaho, Kansas, Mississippi, Missouri, Nebraska, North Carolina, Oklahoma, South Carolina, South Dakota, Tennessee, Texas, Utah, Wisconsin, and Wyoming. The vertical dashed line represents July 1, 2016, when Louisiana implemented Medicaid expansion. Data source: 2011-2019 BRFSS surveys were used for “could not see a doctor due to cost”; 2013, 2014, 2016, and 2018 BRFSS surveys were used for “could not get prescribed medicine due to cost.” BRFSS data on prescribed medicine not used in 2017 because <10% of respondents in Louisiana answered the question in that year. BRFSS survey weights were applied to percentages.
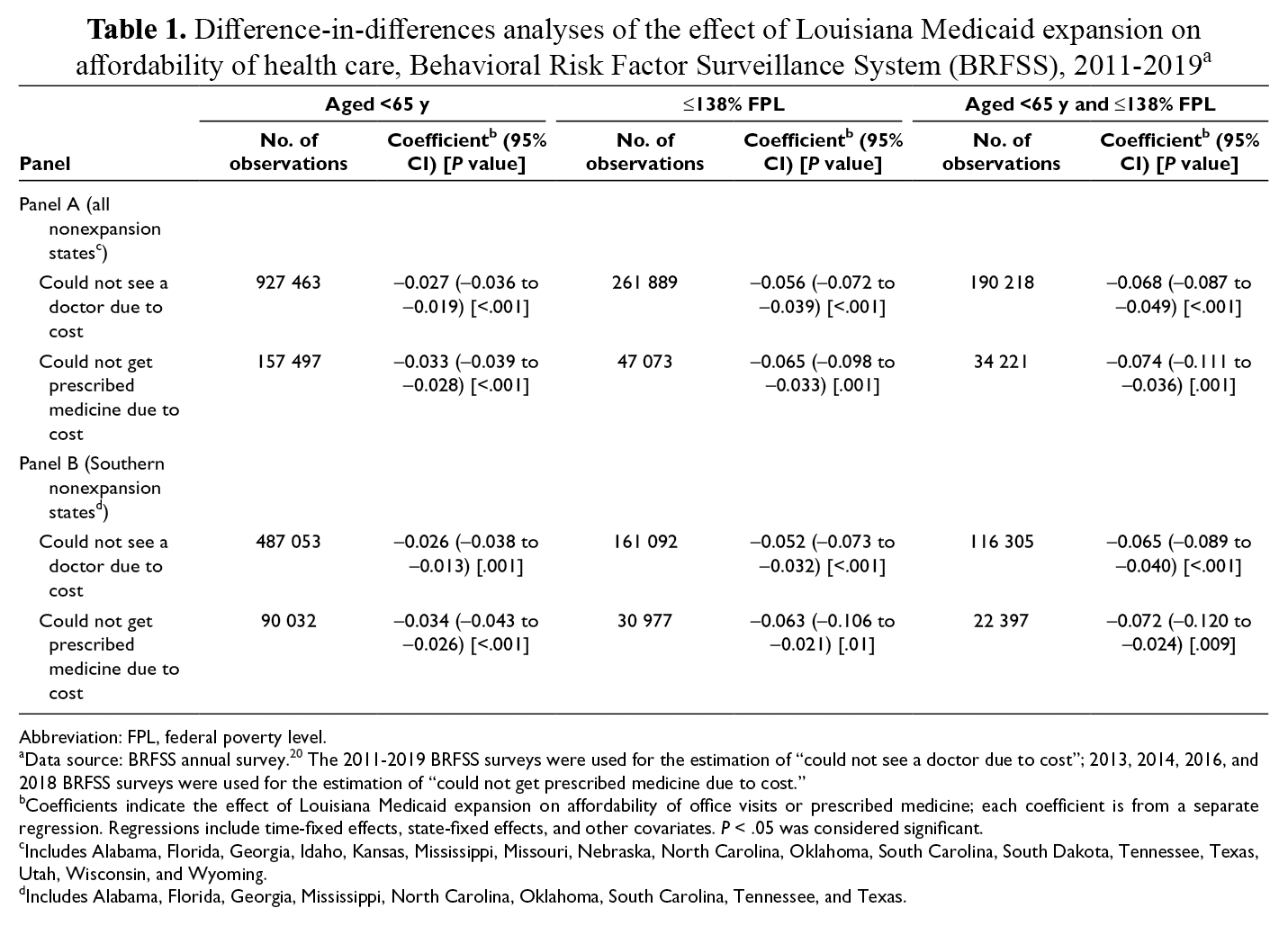
In the DD model limited to adults aged <65, Louisiana had a larger decline than nonexpansion states in the percentage of respondents who reported being unable to see a doctor because of cost (2.7 [95% CI, −3.6 to −1.9] percentage-point difference; P < .001) and in the percentage of respondents who reported being unable to afford medication (3.3 [95% CI, −3.9 to −2.8] percentage-point difference; P < .001; Table 1). The DD specifications that attempted to limit the sample to adults who were imputed to be eligible for Medicaid based on income data were significant, and the point estimates indicated a diminishing of cost barriers for these groups. Among respondents aged <65 with annual household income ≤138% FPL, Louisiana had a larger decline than nonexpansion states among respondents who reported they could not see a doctor because of cost: the difference was 6.8 percentage points (95% CI, −8.7 to −4.9; P < .001). Louisiana also had a larger decline than nonexpansion states in the percentage of respondents who could not get prescribed medicine; the difference in decline was 7.4 percentage points (95% CI, −11.1 to −3.6; P < .001) among respondents aged <65 with annual household income ≤138% FPL.
Difference-in-differences analyses of the effect of Louisiana Medicaid expansion on affordability of health care, Behavioral Risk Factor Surveillance System (BRFSS), 2011-2019 a
Abbreviation: FPL, federal poverty level.
aData source: BRFSS annual survey. 20 The 2011-2019 BRFSS surveys were used for the estimation of “could not see a doctor due to cost”; 2013, 2014, 2016, and 2018 BRFSS surveys were used for the estimation of “could not get prescribed medicine due to cost.”
bCoefficients indicate the effect of Louisiana Medicaid expansion on affordability of office visits or prescribed medicine; each coefficient is from a separate regression. Regressions include time-fixed effects, state-fixed effects, and other covariates. P < .05 was considered significant.
cIncludes Alabama, Florida, Georgia, Idaho, Kansas, Mississippi, Missouri, Nebraska, North Carolina, Oklahoma, South Carolina, South Dakota, Tennessee, Texas, Utah, Wisconsin, and Wyoming.
dIncludes Alabama, Florida, Georgia, Mississippi, North Carolina, Oklahoma, South Carolina, Tennessee, and Texas.
Before Medicaid expansion, among respondents aged <65 with annual household income ≤138% FPL in Louisiana, the average affordability was 61.5% for doctor visits and 73.5% for prescribed medicine. We found nearly the same effect of Medicaid expansion on these outcomes when we compared respondents in Louisiana with respondents in nonexpansion states in the South (Table 1). However, it is likely that we did not fully satisfy the parallel trend assumption for the DD estimates on the affordability of a doctor visit because we found several significant point estimates before July 2016 (Figure 2A). The estimate on the affordability of prescribed medicine was likely validated because we found no evidence of nonparallel trends before July 2016 (Figure 2), although we tested only 2 time points during that period.
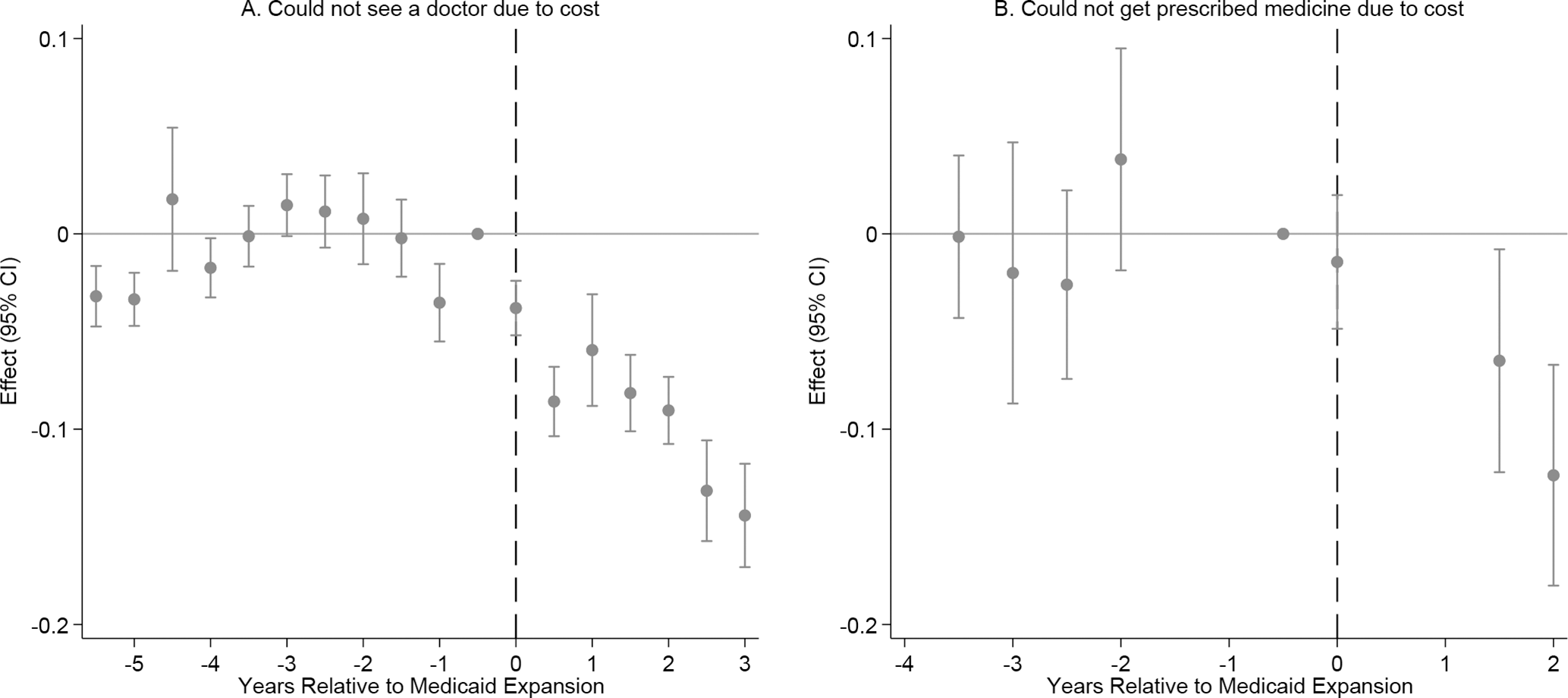
Event study for dynamic associations between Louisiana’s Medicaid expansion and outcomes among Medicaid expansion–eligible adults aged <65 with annual household income ≤138% of the federal poverty level, Behavioral Risk Factor Surveillance System (BRFSS), 2011-2019. 20 Nonexpansion states include Alabama, Florida, Georgia, Idaho, Kansas, Mississippi, Missouri, Nebraska, North Carolina, Oklahoma, South Carolina, South Dakota, Tennessee, Texas, Utah, Wisconsin, and Wyoming. BRFSS survey weights were applied to percentages. The vertical dashed line represents when Louisiana implemented Medicaid expansion. Unit of time was half-year. Data source: 2011-2019 BRFSS surveys were used for “could not see a doctor due to cost”; 2013, 2014, 2016, and 2018 BRFSS surveys were used for “could not get prescribed medicine due to cost.”
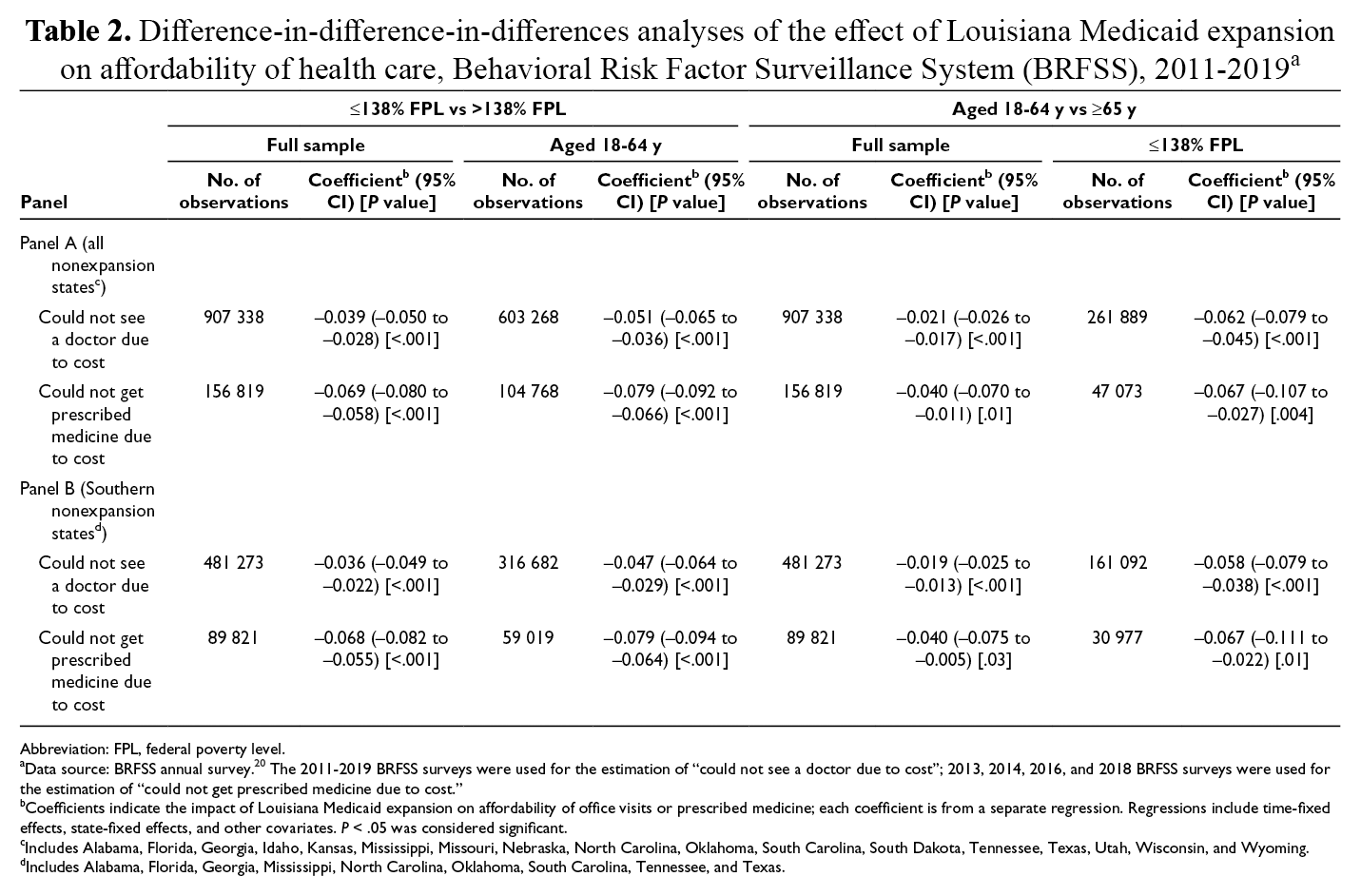
In the first DDD model, which used income level as the third difference (≤138% FPL vs >138% FPL), Medicaid expansion was associated with significant declines in the percentage of respondents unable to see a doctor due to cost (3.9 percentage points; 95% CI, −5.0 to −2.8; P < .001) or unable to get a prescription due to cost (6.9 percentage points; 95% CI, −8.0 to −5.8; P < .001). These effects increased to 5.1 percentage points (95% CI, −6.5 to −3.6; P < .001) and 7.9 percentage points (95% CI, −9.2 to −6.6; P < .001) among respondents aged <65, respectively. In the second DDD model, which used respondent age as the third difference (<65 vs ≥65), Medicaid expansion was associated with significant declines in the percentage of respondents unable to see a doctor due to cost (2.1 percentage points; 95% CI, −2.6 to −1.7; P < .001) and unable to get a prescription due to cost (4.0 percentage points; 95% CI, −7.0 to −1.1; P = .01). These effects increased to 6.2 percentage points (P < .001) and 6.7 percentage points (P = .004) among respondents with annual household income ≤138% FPL, respectively. We found similar estimates when limiting the control group to nonexpansion states in the South (Table 2).
Difference-in-difference-in-differences analyses of the effect of Louisiana Medicaid expansion on affordability of health care, Behavioral Risk Factor Surveillance System (BRFSS), 2011-2019 a
Abbreviation: FPL, federal poverty level.
aData source: BRFSS annual survey. 20 The 2011-2019 BRFSS surveys were used for the estimation of “could not see a doctor due to cost”; 2013, 2014, 2016, and 2018 BRFSS surveys were used for the estimation of “could not get prescribed medicine due to cost.”
bCoefficients indicate the impact of Louisiana Medicaid expansion on affordability of office visits or prescribed medicine; each coefficient is from a separate regression. Regressions include time-fixed effects, state-fixed effects, and other covariates. P < .05 was considered significant.
cIncludes Alabama, Florida, Georgia, Idaho, Kansas, Mississippi, Missouri, Nebraska, North Carolina, Oklahoma, South Carolina, South Dakota, Tennessee, Texas, Utah, Wisconsin, and Wyoming.
dIncludes Alabama, Florida, Georgia, Mississippi, North Carolina, Oklahoma, South Carolina, Tennessee, and Texas.
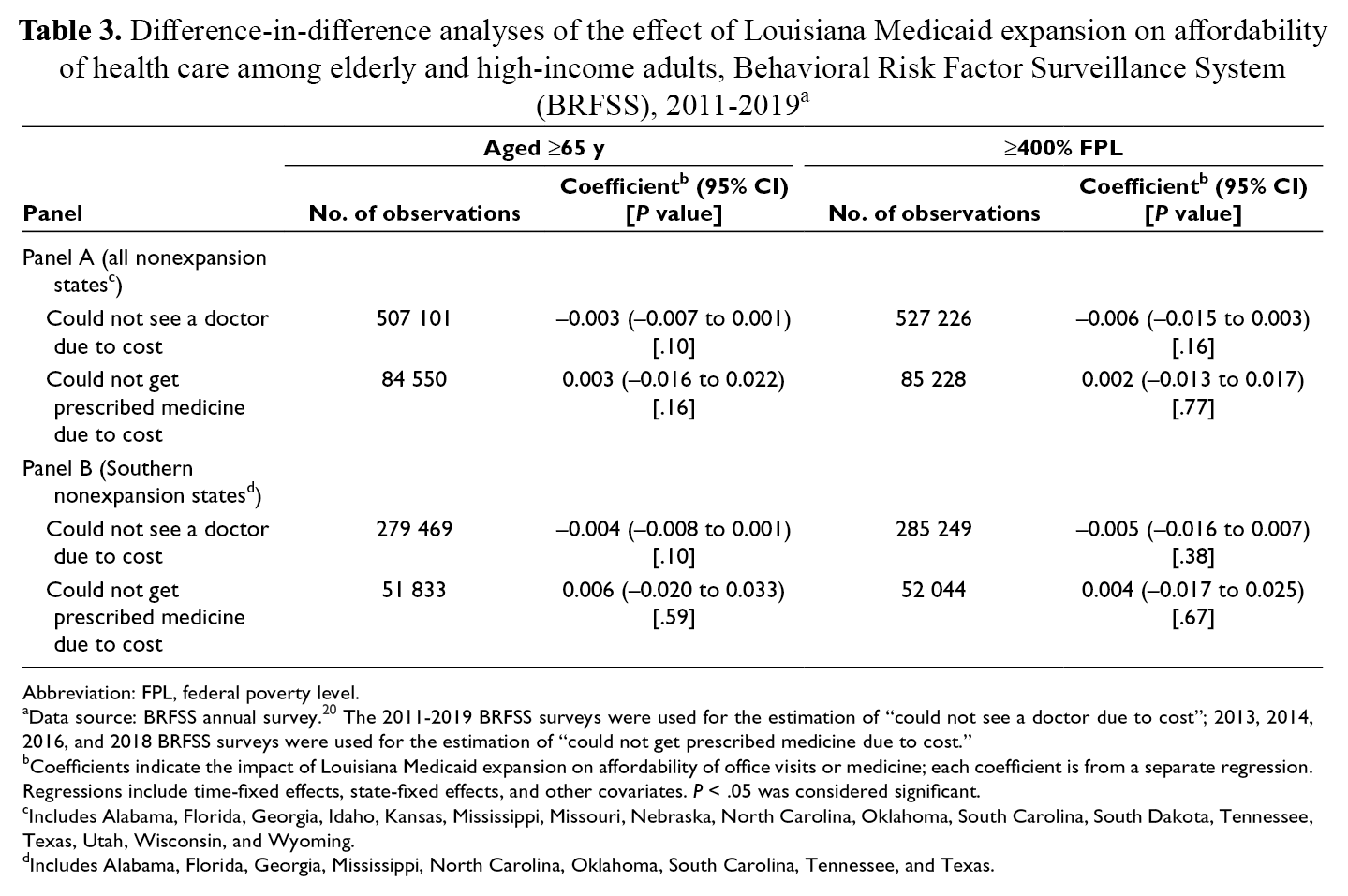
Among 2 samples (one consisting of respondents aged ≥65 and another consisting of respondents with annual household income ≥400% FPL), comparing respondents in Louisiana with respondents in nonexpansion states, we found no evidence that Medicaid expansion improved the affordability of a doctor visit or prescribed medicine (Table 3).
Difference-in-difference analyses of the effect of Louisiana Medicaid expansion on affordability of health care among elderly and high-income adults, Behavioral Risk Factor Surveillance System (BRFSS), 2011-2019 a
Abbreviation: FPL, federal poverty level.
aData source: BRFSS annual survey. 20 The 2011-2019 BRFSS surveys were used for the estimation of “could not see a doctor due to cost”; 2013, 2014, 2016, and 2018 BRFSS surveys were used for the estimation of “could not get prescribed medicine due to cost.”
bCoefficients indicate the impact of Louisiana Medicaid expansion on affordability of office visits or medicine; each coefficient is from a separate regression. Regressions include time-fixed effects, state-fixed effects, and other covariates. P < .05 was considered significant.
cIncludes Alabama, Florida, Georgia, Idaho, Kansas, Mississippi, Missouri, Nebraska, North Carolina, Oklahoma, South Carolina, South Dakota, Tennessee, Texas, Utah, Wisconsin, and Wyoming.
dIncludes Alabama, Florida, Georgia, Mississippi, North Carolina, Oklahoma, South Carolina, Tennessee, and Texas.
Discussion
Louisiana’s Medicaid expansion improved the affordability of health care significantly, likely because overall health insurance coverage increased. We found significant decreases in the percentage of people who could not afford to see a doctor or get prescriptions due to cost after implementation of Medicaid expansion. We verified in the DDD model that this result was driven by people whom we expected to be enrolled in Medicaid because of income eligibility and who were not likely to be enrolled in Medicare because they were aged <65. Louisiana’s Medicaid expansion was successful in removing cost barriers, and this success was detectable in national survey data.
Our study contributes to the literature that examines the experience of states with Medicaid expansion by comparing changes in the affordability of doctor visits and prescription medicine in Louisiana. In a 2020 study, Lee and Porell 6 found a significant decrease of 3.8 percentage points in the percentage of low-income childless adults with unmet care needs due to cost after Medicaid expansion, using 2011-2016 BRFSS data to compare expansion states with nonexpansion states at the national level. We found larger effects in Louisiana’s Medicaid expansion: a significant decline of 6.8 percentage points among respondents unable to see a doctor due to cost. The larger effect we found in Louisiana may have been driven by a population in Louisiana that was more economically disadvantaged than populations in states that expanded Medicaid programs before Louisiana’s expansion. The pre-expansion rate of unmet care needs was 35% in these other expansion states and 40% in Louisiana.
The findings of our study are consistent with the findings of a study that evaluated the effect of Medicaid expansion on the affordability of health care in Kentucky and Arkansas using Texas as a control. 12 Another study revealed declines in unmet medical needs due to cost among a low-income group in Kentucky after its Medicaid expansion. 9 Although the study in Kentucky used Missouri, Tennessee, and Virginia as controls in its DD model, we used all other nonexpansion states (before 2019) as controls in our DD model and found similar results. According to our dynamic estimates, we found a dip in the percentage of respondents unable to afford a doctor visit 2 years before Medicaid expansion, followed by an increase in the year before Medicaid expansion. Both changes were small relative to the declines we observed even 1 year after Louisiana’s Medicaid expansion and much smaller than subsequent declines. Our event study detected a decline in respondents unable to see a doctor due to cost in the year immediately after expansion, and this decline continued in the 3 years after expansion. In contrast to studies in other expansion states, we found no delay in effects of Medicaid expansion in Louisiana, possibly because of the use of an abbreviated enrollment process for a large number of qualified applicants. 32 Because of the imprecision of our estimates, we are unable to conclude whether Medicaid expansion had an early effect in 2015 on the affordability of prescribed medicine.
Limitations
Our study had several limitations. First, we used self-reported survey data, which may be subject to response, nonresponse, and recall biases, which could have affected the measurements of participants’ true barriers to medical care due to costs. People in Louisiana may feel better about the affordability of doctor visits and prescription medicine, but it is not clear how this perception affects their finances. Our results, using BRFSS data, subjectively measured the effect of Louisiana’s Medicaid expansion on affordability. Future studies could evaluate the effect of Medicaid expansion on actual out-of-pocket costs. Second, data on health insurance types were not always available from the BRFSS. Questions about types of health insurance were not added to surveys in 2011, 2012, 2013, or 2015. We could not investigate the effect of Louisiana’s Medicaid expansion among new enrollees because surveys lacked indicators for enrollment status in previous years. Third, surveys asked questions about affordability in the previous 12 months, which introduced measurement error in surveys conducted in the year immediately after expansion, because respondents may have placed more weight on financial experiences either before or after expansion. Fourth, the BRFSS does not ask about Medicaid eligibility directly. Instead, we had to impute data on eligibility from income data provided in a range. Our Medicaid eligibility imputation may have missed people potentially eligible and counted others as eligible when they were not. Therefore, findings in our study should be interpreted with caution.
Conclusion
Our study provides evidence that Louisiana’s Medicaid expansion lowered cost barriers to health care among low-income adults aged <65. These positive effects among residents of Louisiana may encourage the state to maintain expansion or prompt other states in the South to consider implementing expansion. Future research and practice are warranted in extrapolating these findings to other potential Medicaid expansion states.
Footnotes
Acknowledgments
The Louisiana Department of Health maintained no editorial control over this article or the research findings.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: A contract agreement with the Louisiana Department of Health provided financial support for this work.