
Abstract
Objectives
Human papillomavirus (HPV) vaccination coverage in the United States is far below coverage for other routine adolescent vaccines. We examined whether missed opportunities for HPV vaccination among adolescents differ by parental nativity (country of origin) in Minnesota.
Methods
We retrospectively analyzed birth record and immunization information data for adolescents in Minnesota born during 2004-2007 using data from January 1, 2015, through December 31, 2018. Using logistic regression, we assessed the association between parental nativity and missed opportunities for HPV vaccine initiation, or receipt of other vaccines without receipt of the HPV vaccine. We adjusted for parent/child demographic and vaccination characteristics. We defined nativity as the number of non–US-born parents and maternal region of birth.
Results
Adolescents with mothers born in Eastern Europe (adjusted odds ratio [aOR] = 2.33; 95% CI, 2.01-2.73) and Africa (aOR = 1.36; 95% CI, 1.28-1.43) had greater adjusted odds of missed opportunities for HPV vaccination than adolescents with US-born mothers. However, adolescents with mothers from Latin America and the Caribbean had lower odds of missed opportunities than adolescents with US-born mothers (aOR = 0.61; 95% CI, 0.58-0.65). Adolescents with 1 or 2 non–US-born parents had lower odds of missed opportunities for HPV vaccination than adolescents with 2 US-born parents (1 parent: aOR = 0.92; 95% CI, 0.88-0.96; 2 parents: aOR = 0.90; 95% CI, 0.87-0.94).
Conclusions
Future studies should evaluate outreach to groups with HPV vaccination disparities and identify other drivers of missed opportunities among adolescents with US-born parents, such as multiparity.
Human papillomavirus (HPV) is the most prevalent sexually transmitted infection in the United States and is a leading cause of cervical, oropharyngeal, and anal cancers. 1,2 Despite evidence of HPV vaccine safety and efficacy since it was first recommended for adolescent females in 2006 3 and males in 2011, 4 uptake is low compared with other adolescent vaccines. 5 According to the 2019 National Immunization Survey–Teen (NIS-Teen), only 71% of adolescents in the United States had received 1 or more HPV vaccines, and only 54.2% were up to date. 6 However, the 2019 NIS-Teen showed that 88.9% of adolescents had received 1 or more doses of the meningococcal vaccine, and 90.2% had received the tetanus, diphtheria, and acellular pertussis (Tdap) vaccine. 6
For several decades, non–US-born populations in the United States have been the fastest-growing demographic group, composing 4.7% of the total population in 1970 and 13.7% in 2019. 7,8 In Minnesota, immigrants constitute 9% of the population, and 13.4% of children in the United States have at least 1 non–US-born parent. 8,9 A 2018 analysis of disparities in HPV initiation and completion found substantially lower odds of HPV vaccination completion among non–US-born women than among US-born women, suggesting that nativity influences vaccination. 10 However, few studies have examined whether missed opportunities for vaccination, including HPV, differ by parental country of origin. 11 -13 We analyzed parental nativity for 2 reasons: (1) non–US-born populations in the United States may be less likely than US-born populations to initiate or complete the HPV vaccine series 14 and (2) parents play a critical role in vaccination decision making for adolescents. 15,16 We sought to determine whether (1) missed opportunities for HPV vaccination are more likely among adolescents with 1 or 2 non–US-born parents than among adolescents with 2 US-born parents and (2) the odds of missed opportunities for HPV vaccination among adolescents vary by maternal region of origin.
Methods
Data Sources
The Minnesota Immunization Information Connection (MIIC) is a statewide immunization information system (IIS) maintained by the Minnesota Department of Health since 2002. 17 As of July 2018, MIIC contained data on 93.1 million immunizations for 6.8 million people. About 91% of health care providers participating in the Minnesota Vaccines for Children program routinely submit vaccination data to MIIC. 18 For this study, MIIC generated a dataset of IIS entries from January 1, 2015, through December 31, 2018, for people born in Minnesota during 2004-2007. MIIC linked IIS data from adolescents to demographic information about parents at the time of the child’s birth from the Minnesota Department of Health Office of Vital Records in a de-identified dataset. MIIC matched 99.2% of data from the IIS to Office of Vital Records data by birth certificate number. This birth cohort included adolescents who were at least 11 years of age at the time of vaccination according to the HPV vaccination schedule (Figure 1). We obtained institutional review board waiver for data use from the University of Minnesota in agreement with the Minnesota Department of Health.
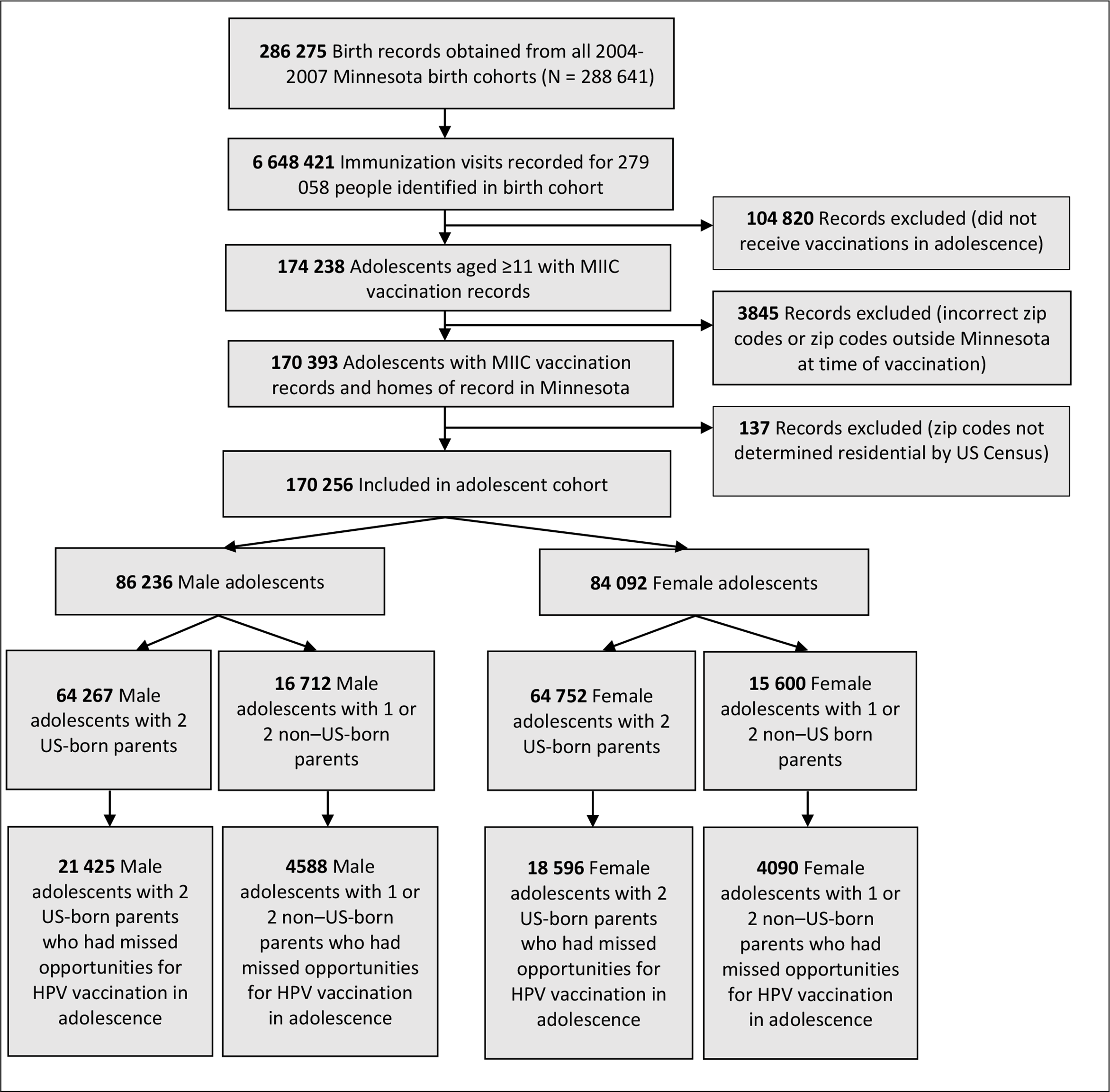
Flow chart of analysis dataset of human papillomavirus (HPV) vaccination among adolescents in Minnesota, January 2015–July 2018. A total of 5784 (6.1%) male adolescents and 5847 (7.0%) female adolescents were missing information on parental nativity for both parents. Data source: Minnesota Immunization Information Connection (MIIC) 17 and Minnesota Department of Health Office of Vital Records. All adolescents included in the study were born during 2004-2007.
Missed Opportunities
Our primary outcome was adolescents who had missed opportunities for HPV vaccination. We defined a missed opportunity as receipt of any vaccine between ages 11 and 14 without receipt of the HPV vaccine; vaccination encounters that could result in missed opportunities included routine adolescent vaccines such as meningococcal, Tdap, or other catchup or booster vaccines. We omitted the seasonal influenza vaccine because it may be administered in schools and pharmacies and would not represent a missed opportunity for HPV vaccination. We assessed this outcome among adolescents born during 2004-2007 who had at least 1 MIIC record as of 2018 and, therefore, had ever been vaccinated in Minnesota. We determined eligibility for the HPV vaccine by the adolescent’s age at the time of the visit and whether the adolescent had already completed the HPV vaccination series. We defined adolescence starting at age 11, corresponding to the recommended age for routine HPV vaccination. 19 Adolescents were aged 11-14 years given the available years of vaccination records for this birth cohort.
Parental Nativity
Parental country of birth was reported on the child’s birth certificate record. First, we categorized parental nativity as follows: (1) both parents born outside the United States (non–US-born), (2) both parents born in the United States (US-born), (3) 1 parent born outside the United States and 1 parent either born in the United States or missing data on nativity, and (4) data missing on nativity of both parents or missing for 1 parent and the other parent born in the United States. We chose this categorization to avoid inducing multicollinearity between maternal and paternal nativity (correlation coefficient = 0.66) and generating unstable parameter estimates.
Next, we assigned maternal region of origin according to the United Nations 5 Regional Groups: Africa, Asia-Pacific, Eastern Europe, Latin America and the Caribbean, and Western Europe and other. 20 We analyzed maternal region of origin because maternal nativity data were more complete than paternal nativity data. Modifications to these groups included counting the United States as a separate group, accounting for countries of birth listed in the birth record that no longer existed at the time of analysis, or zones/states that were unrecognized by the United Nations. We separated Western Europe and Canada from Oceania and other states. In some cases, we categorized countries by geographic area according to another analysis of timeliness of childhood vaccinations and parental nativity conducted by MIIC. 20,21
Vaccination Characteristics
Child vaccination characteristics for each vaccination visit included the following: vaccine administered, child’s age at vaccination, and type of health insurance (private, subsidized, or underinsured/uninsured) used to cover vaccination. 22 We selected the funding source most often used for vaccinations after the age of 11 when multiple funding sources were listed. Government-subsidized health insurance includes Minnesota’s public health insurance programs and federal programs designed to reach certain populations (eg, American Indian/Alaska Native people) and special vaccine insurance (Vaccines4Kids). Approximately 36.5% of people in Minnesota received a form of subsidized health insurance in 2017. 23,24 We included year of birth to account for differences in eligibility guidelines by year and age.
Demographic Characteristics
Demographic characteristics obtained from the birth record included parental education level at the time of birth, the child’s birth year, and the mother’s total previous number of births at the time of the child’s birth (multiparity). 25,26 We included categorical measures for maternal and paternal education level (≤high school, some college, ≥bachelor’s degree, missing). We did not use data on race/ethnicity because of inconsistencies in the self-reporting of race in the birth certificate; for example, 76% of mothers born in Africa were missing data on race.
We used median household income by zip code of residence at the time of vaccination from US Census data to adjust for confounding by socioeconomic status. 27 We also controlled for confounding by geographic area based on these zip codes using Rural–Urban Commuting Area Codes classified by the Minnesota State Demographic Center as urban core, small rural core, other urban, other small rural, other large rural, large rural core, and isolated rural. 28 -30 This classification is consistent with other published analyses using MIIC data and controls for distance from major population centers and small and large towns across the state. 25,31
Analysis
We used logistic regression to analyze the effect of parental nativity on 1 or more missed opportunities for HPV vaccination among adolescents. We compared missed opportunities for HPV vaccination among adolescents who had 2 non–US-born parents with adolescents who had 2 US-born parents, and then we compared adolescents who had 1 non–US-born parent with adolescents who had 2 US-born parents. Finally, we compared missed opportunities for HPV vaccination among adolescents by maternal region of origin.
We controlled for the following potential confounders: adolescent’s birth year (categorical), adolescent’s sex (male or female), maternal and paternal education levels (≤high school, some college, ≥bachelor’s degree, or missing), multiparity (1, 2, 3, 4, or ≥5 children), median annual household income by zip code of residence at the time of vaccination (<$35 000, $35 000-$39 999, $40 000-$49 999, ≥$50 000), geographic location by Rural–Urban Commuting Area Codes (grouped by urban core, other urban, large rural core, other large rural, small rural core, other small rural, or isolated rural), and type of health insurance used for vaccinations (private, other, or uninsured/underinsured).
We conducted crude and adjusted analyses of missed opportunities using logistic regression. We tested for a difference in the relationship between nativity and missed opportunities by sex in sensitivity analyses by including an interaction term. We conducted all analyses using StataIC version 15 (StataCorp). We used Pearson χ2 tests to determine significance of differences between groups in descriptive statistics, with P < .05 considered significant. We reported 95% CIs of model coefficients to indicate precision of estimates, and we used a significance level of P < .05 for coefficients to determine the significance of the interaction term in the model comparing effect size by biological sex.
The initial cohort comprised 279 058 members of the 2004-2007 Office of Vital Records birth cohort. After restricting the dataset to adolescents aged ≥11 years with IIS records (n = 174 238) and adolescents with residence zip codes in Minnesota, the final analysis cohort of linked birth and vaccination records included 170 256 adolescents (50.6% male).
Results
Missed Opportunities
Of 170 256 adolescents, 51 532 (30.3%) had missed opportunities for HPV vaccination (Table 1). Missed opportunities for HPV vaccination occurred among 27 488 of 86 164 (31.9%) male adolescents and 24 044 of 84 092 (28.6%) female adolescents. Adolescents with missed opportunities for HPV vaccination were similar in age to adolescents with no missed opportunities for vaccination (mean age = 12.4 years).
Characteristics of adolescents by missed opportunities or no missed opportunities for human papillomavirus vaccination, Minnesota, January 2015–July 2018 a
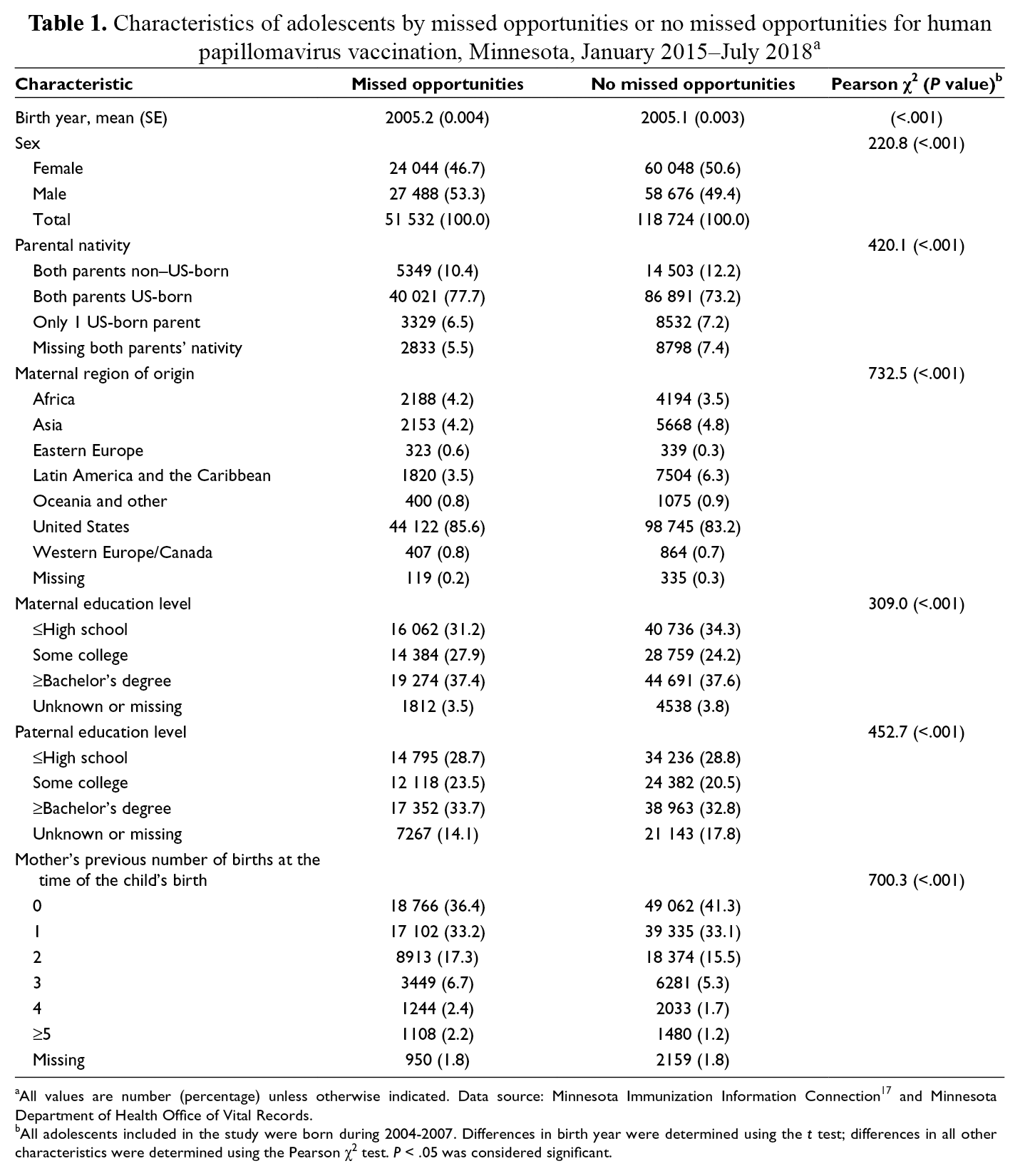
aAll values are number (percentage) unless otherwise indicated. Data source: Minnesota Immunization Information Connection 17 and Minnesota Department of Health Office of Vital Records.
bAll adolescents included in the study were born during 2004-2007. Differences in birth year were determined using the t test; differences in all other characteristics were determined using the Pearson χ2 test. P < .05 was considered significant.
Parental Nativity
A greater proportion of adolescents with missed opportunities (77.7%) than adolescents with no missed opportunities (73.2%) had 2 US-born parents (Table 1). Adolescents with 1 non–US-born parent comprised 6.5% of adolescents with missed opportunities and 7.2% of adolescents with no missed opportunities. A lower percentage of adolescents with 2 non–US-born parents had missed opportunities (10.4%) than no missed opportunities (12.2%). Because of the large sample size, all comparisons of differences between groups were significant (P < .001).
Among adolescents with US-born mothers, 85.6% had missed opportunities and 83.2% had no missed opportunities (Table 1). Similarly, among adolescents with mothers from Africa, 4.2% had missed opportunities and 3.5% had no missed opportunities, followed by adolescents with mothers from Eastern Europe (0.6% and 0.3%, respectively). Conversely, the proportion who had no missed opportunities was higher than the proportion who had missed opportunities among adolescents with mothers from Latin America and the Caribbean (6.3% vs 3.5%), followed by adolescents with mothers from Asia (4.8% vs 4.2%). The largest share of mothers from these regions originated in Russia (31.0% of Eastern European origin), Somalia (47.5% of African origin), Canada (42.6% of Western European and Canadian origin), Laos (25.5% of Asian origin), other countries (94.3% of Oceania and other origin), and Mexico (73.7% of Latin America and the Caribbean).
Vaccination Characteristics
Among adolescents with missed opportunities for HPV vaccination, 59.3% were privately insured, 19.4% were missing data on health insurance, 18.4% had subsidized health insurance, and 2.9% were uninsured or underinsured (Table 2). Among adolescents with no missed opportunities for HPV vaccination, 59.4% were privately insured, 20.9% had subsidized health insurance, 17.7% were missing data on health insurance, and 1.9% were uninsured or underinsured.
Geographic, income, and health insurance characteristics of adolescents, by missed opportunities or no missed opportunities for human papillomavirus vaccination, Minnesota, January 2015–July 2018 a
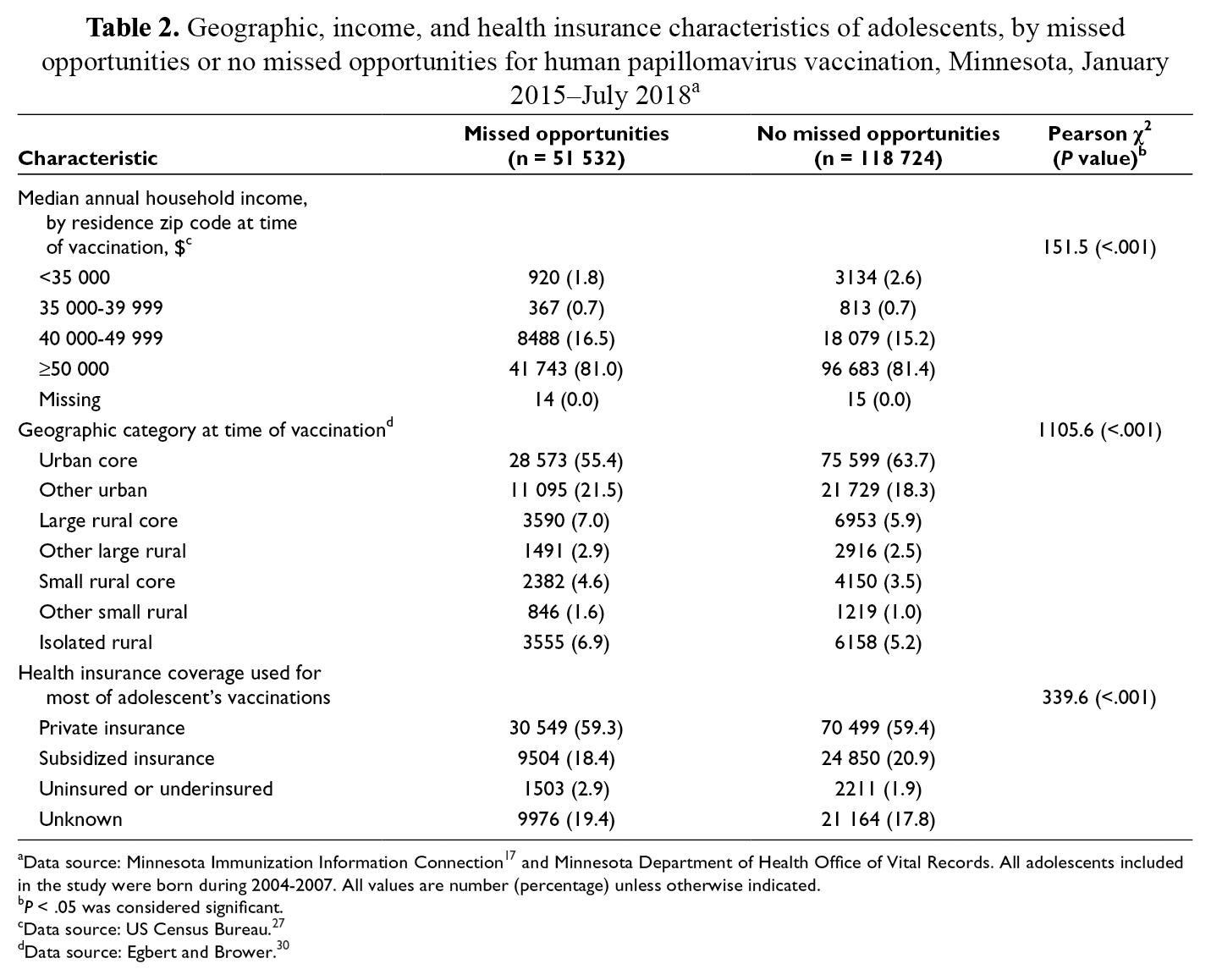
aData source: Minnesota Immunization Information Connection 17 and Minnesota Department of Health Office of Vital Records. All adolescents included in the study were born during 2004-2007. All values are number (percentage) unless otherwise indicated.
b P < .05 was considered significant.
cData source: US Census Bureau. 27
dData source: Egbert and Brower. 30
Other Demographic Characteristics
Among adolescents with mothers with ≤high school education, a smaller proportion of adolescents had missed opportunities than no missed opportunities (31.2% vs 34.3%) (Table 1). Adolescents whose mothers had some college education comprised 27.9% of adolescents with missed opportunities and 24.2% of adolescents with no missed opportunities, and patterns were similar for paternal education. Adolescents whose mothers had higher multiparity comprised a greater share of adolescents with missed opportunities than adolescents with no missed opportunities. For example, adolescents with no siblings at birth comprised 36.4% of adolescents with missed opportunities and 41.3% of adolescents with no missed opportunities. Adolescents with ≥5 siblings at birth comprised 2.2% of adolescents with missed opportunities and 1.2% of adolescents with no missed opportunities.
Among adolescents with missed opportunities for HPV vaccination, 81.0% resided in a zip code with a median annual household income of ≥$50 000 and 16.5% resided in a zip code with a median annual household income of $40 000-$49 999 (Table 2). Adolescents residing in the urban core comprised a smaller proportion of adolescents with missed opportunities (55.4%) than adolescents with no missed opportunities (63.7%). In urban areas, a higher proportion of adolescents had missed opportunities for HPV vaccination than no missed opportunities (21.5% vs 18.3%). A greater proportion of adolescents with missed opportunities than adolescents with no missed opportunities lived in isolated rural areas (6.9% vs 5.2%).
Odds of Missed Opportunities
Bivariate analyses estimated reduced odds of missed opportunities for HPV vaccination among adolescents with 1 non–US-born parent (odds ratio [OR] = 0.84; 95% CI, 0.81-0.88) or 2 non–US-born parents (OR = 0.80; 95% CI, 0.77-0.83) than among adolescents with 2 US-born parents (Table 3). These findings were consistent after adjusting for adolescents with 1 non–US-born parent (OR = 0.92; 95% CI, 0.88-0.96) and 2 non–US-born parents (OR = 0.90; 95% CI, 0.87-0.94).
Odds of missed opportunities for human papillomavirus vaccination among adolescents (n = 176 009), by parental nativity, Minnesota, January 2015–July 2018 a
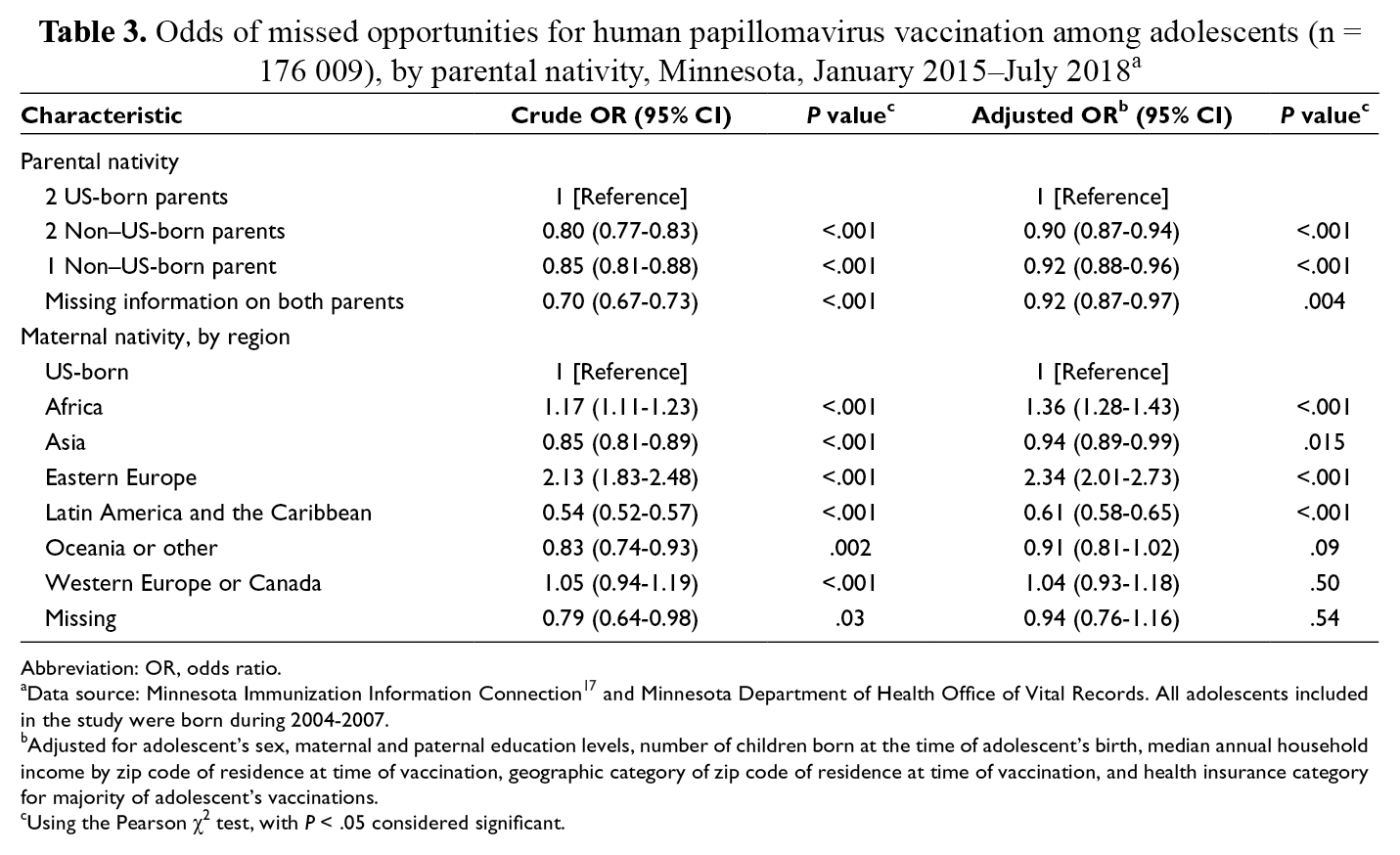
Abbreviation: OR, odds ratio.
aData source: Minnesota Immunization Information Connection 17 and Minnesota Department of Health Office of Vital Records. All adolescents included in the study were born during 2004-2007.
bAdjusted for adolescent’s sex, maternal and paternal education levels, number of children born at the time of adolescent’s birth, median annual household income by zip code of residence at time of vaccination, geographic category of zip code of residence at time of vaccination, and health insurance category for majority of adolescent’s vaccinations.
cUsing the Pearson χ2 test, with P < .05 considered significant.
Having a mother from Eastern Europe resulted in 2.34 (95% CI, 2.01-2.73) times the odds of a missed opportunity compared with having a US-born mother (Table 3). Adolescents whose mothers were born in Africa had the next highest odds of a missed opportunity for HPV vaccination compared with adolescents with US-born mothers (aOR = 1.36; 95% CI, 1.28-1.43). Compared with adolescents who had a US-born mother, adolescents with mothers from Latin America or the Caribbean had lower odds of a missed opportunity (aOR = 0.61; 95% CI, 0.58-0.65).
Biological Sex
We found no significant difference in the effect of parental nativity on missed opportunities by sex for all nativity groups (Figure 2). The interaction between sex and nativity was not significant (P = .21). When we used models restricted to only female adolescents or only male adolescents, our conclusions did not change substantially.
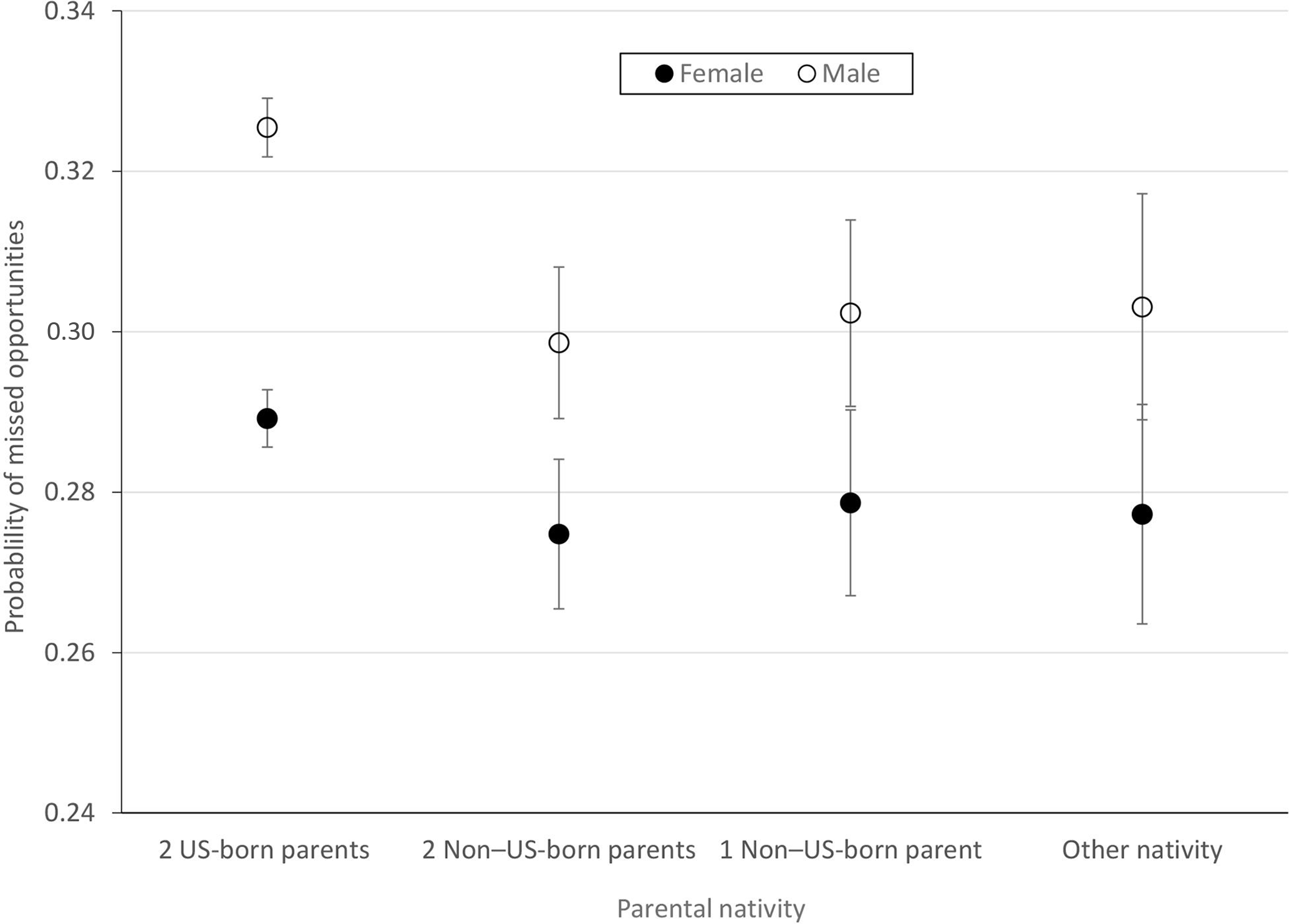
Probability of missed opportunities for human papillomavirus vaccination, by parental nativity and adolescent sex, Minnesota, January 2015–July 2018. Error bars indicate 95% CIs. Data source: Minnesota Immunization Information Connection 17 and Minnesota Department of Health Office of Vital Records. All adolescents included in the study were born during 2004-2007.
Discussion
This study is one of the first of its kind to use a statewide, population-based sample to examine missed opportunities for HPV vaccination by parental nativity. 11 It builds upon work by the Minnesota Department of Health that found that mothers from Somalia and Eastern Europe had children with the lowest rates of uptake for childhood vaccinations up to the age of 18 months. 21 Another study of Somali men in Olmsted County, Minnesota, found that most Somali fathers were unaware of the HPV vaccine and its role in preventing cervical cancer and other HPV-associated cancers in their children. 32 Therefore, identification of groups at increased risk for missed opportunities based on parental nativity may be useful in promoting the HPV vaccine.
Our finding that missed opportunities for HPV vaccination vary by maternal region of origin underscores the importance of considering region of origin rather than comparing HPV vaccination of adolescents with US-born parents with HPV vaccination of adolescents with non–US-born parents. If examined as a simple categorical measure, the greater odds of missed opportunities among adolescents with US-born mothers obscures disparities among adolescents whose mothers are from Africa and Eastern Europe. The Minnesota population is a useful population to study because of the large representation of refugees and parents from Africa, Asia, and Latin America. In our study, fewer adolescents with mothers from Asia and Latin America and the Caribbean compared with adolescents with US-born mothers had missed opportunities for HPV vaccination, indicating that these groups may be at lower risk of missed opportunities for HPV vaccination.
Vaccination practices in the country of origin may help explain differences in adolescent vaccination behavior. Adolescents whose mothers were born in Latin America and the Caribbean had the lowest odds of missed opportunities, and most Latin American and Caribbean mothers in our study came from Mexico (76%). HPV vaccination rates are high in Mexico, with an estimated 97% of coverage among adolescent girls for both the first and second dose of the HPV vaccine. 33 Although the mothers in our study would have immigrated before implementation of HPV vaccine rollout, they may still have a greater likelihood of vaccination acceptance than US-born parents. In another study conducted in California, Hispanic ethnicity was associated with a lower likelihood of vaccine hesitancy than non-Hispanic ethnicity. 34 Disparities in HPV vaccination by Hispanic ethnicity in the United States have been identified in other studies, but our study suggests that these disparities are not driven by vaccine hesitancy because of parental nativity. Other drivers may be more important, such as health care access. 35 -37
Adolescents whose parents were born in Eastern Europe are an overlooked group. HPV vaccine series completion in 2014 was estimated to be only 8% among females aged 10-19 years in Eastern Europe, compared with 46% and 69% among females aged 10-14 years and 15-19 years, respectively, in Western Europe. 38 As of 2016, the HPV vaccine was not fully integrated into the national immunization programs in 9 Eastern European nations. 39 In countries where HPV vaccination is provided, financial constraints and negative public perception are barriers to vaccination coverage. 40 Although HPV vaccination policies were enacted after parents in our study arrived in the United States, underlying lack of confidence in vaccination could continue to influence parents upon arrival in their destination country.
Our study found that adolescents with 2 US-born parents also had high odds of missed opportunities. Demographic and social factors including male sex, annual household income, number of children, and geographic area have been documented in other studies in Minnesota and nationally. 21,41 -50 For example, in the model comparing odds of missed opportunities among adolescents with US-born and non–US-born parents, we controlled for multiparity among other confounders, and adolescents in families of ≥5 children had approximately twice the odds of missed opportunities (OR = 2.15; 95% CI, 1.98-2.33) compared with adolescents without siblings at birth. More research may inform targeted approaches for HPV vaccination to parents of multiple children among other groups to mitigate these disparities.
Differences by nativity could reflect the social and demographic factors that influence missed opportunities for HPV vaccination. Although the HPV vaccine is provided free of charge by Medicaid and the Minnesota Vaccines for Children program, logistical barriers and opportunity costs of clinic visits may vary by nativity and may limit uptake.46 Our findings suggest that HPV vaccination guidelines should not merely increase targeting of HPV vaccine interventions to children of immigrants but, rather, rely on context-specific interventions appropriate to the needs of groups that have been overlooked. This increased targeting of interventions includes greater outreach among groups that have an increased risk of missed opportunities, such as adolescents who have African or Eastern European parents, and continued focus on adolescents with US-born parents.
Limitations
This study had several limitations. First, health care provider participation in MIIC and submission of health records are voluntary; as such, our study may have overestimated missed opportunities among adolescents who received vaccinations that were not recorded in the registry. However, we assumed missingness to be no different across exposure and outcome groups. Second, we focused on any HPV vaccination rather than completion of the HPV series because of the limited window of time for completing the HPV vaccine series for the years available in the MIIC registry. Third, although we controlled for income status by zip code, finer detail would have been preferable to account for income variability within zip codes. 31 However, most people are slow to relocate, so neighborhood-based measures of income likely reflect longer-term socioeconomic position. 51
Conclusion
Adolescents with 2 US-born parents had a greater risk of missed opportunities for HPV vaccination than adolescents with 1 or 2 non–US-born parents. Missed opportunities among adolescents differed by nativity by maternal region of birth, and the size and direction of the relationship varied by region. Our study may inform other state departments of health to tailor their outreach efforts in populations where nativity has either positive or negative effects on HPV vaccination behavior. Our study suggests that nativity may be a factor in driving missed opportunities for HPV vaccination among adolescents, particularly children of Eastern European and African-born parents in the United States.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a Healthcare Delivery Research Program grant supplement (principal investigator: S.K.) from the National Cancer Institute (NCI) Division of Cancer Control & Population Sciences (NCI 5P30CA077598-19). Additional funding support was provided by the University of Minnesota National Institutes of Health Clinical and Translational Science Award: TL1R002493 and UL1TR002494.