
Abstract
Objectives
Retention in care is a critical component of effective HIV treatment, and adolescents and young adults are at higher risk of inadequate retention than older adults. The objective of our study was to examine the patterns of retention in care among adolescents and young adults with HIV infection by analyzing Medicaid and commercial health insurance claims data.
Methods
We evaluated retention in care for HIV-diagnosed adolescents and young adults aged 13-24 using the 2010-2014 MarketScan Medicaid and MarketScan Commercial Claims health insurance databases. The study period extended 36 months from the date of the first claim with a code for HIV or AIDS. We determined the unweighted proportion retained in care for the Medicaid and Commercial Claims cohorts for months 0-24 and 25-36. We assessed associations between demographic characteristics and retention in care using logistic regression.
Results
A total of 378 adolescents and young adults were in the Medicaid cohort and 1028 in the Commercial Claims cohort. In the Medicaid and Commercial Claims cohorts, respectively, 186 (49%) and 591 (57%) adolescents and young adults were retained in care during months 0-24. In the Medicaid cohort, 113 (73%) people retained in care and 69 (45%) people not retained in care during months 0-24 were retained in care during months 25-36. In the Commercial Claims cohort, 313 (77%) and 94 (31%) retained and not retained people, respectively, were found to be in care during months 25-36.
Conclusions
Notable proportions of HIV-diagnosed adolescents and young adults are not adequately retained in care; public health interventions tailored to this population are needed.
With effective treatment, people with HIV infection can have near-normal life expectancies. 1 -3 Long-term survival with HIV infection depends on controlling the virus through antiretroviral therapy. 4 -6 Consistent medical care allows for provision of antiretroviral therapy, monitoring response to therapy, screening for comorbidities, managing adverse effects of treatment, and other critical aspects of medical care. 7 Poor retention in medical care is associated with reduced odds of survival for people with HIV infection. 8
Adolescents and young adults are particularly at risk of inadequate retention in care. 9,10 Compared with older adults with HIV infection, adolescents with HIV infection have lower rates of medication adherence, viral suppression, and retention in medical care. 11 -13 Increasing retention in care among adolescents and young adults with HIV infection may help improve outcomes for this population, because retention in care is associated with improved rates of viral suppression. 14
Greater understanding of the patterns of retention among adolescents and young adults with HIV may provide insights into possible barriers to retention. Health insurance claims databases contain information about medical encounters over time and are used to examine retention in care for HIV-diagnosed adults aged ≥18. 15,16 We used health insurance claims data to evaluate retention in medical care for insured, HIV-diagnosed adolescents and young adults in the United States.
Methods
Data sources for these analyses were the 2010-2014 MarketScan Multi-State Medicaid and MarketScan Commercial Claims and Encounters databases. MarketScan databases contain de-identified, patient-level health data, including inpatient, outpatient, and pharmaceutical services claims. In each database, individuals are tracked across various data types and during multiple years by a unique enrollee identifier. 17 The MarketScan Multi-State Medicaid databases include pooled Medicaid data from 6-12 unidentified states 15,17 ; the MarketScan Commercial Claims and Encounters databases contain medical data from employees, their spouses, and dependents covered by employer-sponsored private health insurance in the United States. 16
We defined separate Medicaid and commercial health insurance study cohorts using the following eligibility criteria: (1) an International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) diagnostic billing code for HIV or AIDS in 2010, (2) age 13-24 in 2010, (3) enrollment in Medicaid or commercial health insurance ≥10 months of each 12-month period during months 0-24, and (4) ≥1 outpatient visit with a physician, nurse practitioner, or physician’s assistant in the first 6 months of the study period. 18 We defined HIV infection by the presence of 1 of the following ICD-9-CM diagnostic codes: 042 (HIV disease), V08 (asymptomatic HIV infection), 079.53 (HIV, type 2), or 795.71 (nonspecific serologic evidence of HIV). To minimize the risk of including individuals with a diagnostic code assigned only for rule-out testing or with an HIV-specific diagnostic code assigned in error, we excluded adolescents and young adults with an ICD-9-CM code for HIV or AIDS on only 1 date. The study period extended 36 months from the date of the first claim containing an ICD-9-CM code for HIV or AIDS.
We used the Health Resources & Services Administration’s (HRSA’s) medical visit frequency performance measure to define care status. We defined retention in care as ≥1 outpatient visit with a physician, nurse practitioner, or physician’s assistant every 6 months, at least 60 days apart, for study period months 0-24. 19 We defined in care as ≥1 visit every 6 months, at least 60 days apart, for study period months 25-36. We defined an outpatient visit using Current Procedural Terminology (CPT) and MarketScan provider type codes. 17,20 We included the following outpatient visit CPT codes in the analysis: 99201, 99202, 99203, 99204, 99205, 99212, 99213, 99214, 99215, G0463, and T1015. We included CPT codes 99241, 99242, 99243, 99244, and 99275 if associated with a provider-type code indicating a visit with an infectious disease specialist.
We describe the demographic characteristics of adolescents and young adults in both cohorts. We determined the unweighted proportion of adolescents and young adults in each cohort who were retained in care during months 0-24. We then divided each cohort into retained and not retained subgroups, depending on whether they were classified as retained during months 0-24. Before performing the next step in the analysis, we excluded all adolescents and young adults who were not enrolled in the relevant health insurance program for ≥10 months during months 25-36. We then determined the unweighted proportions of retained and not retained adolescents and young adults who met the in-care definition during months 25-36.
To assess associations between available demographic characteristics and retention in care during months 0-24, we conducted bivariate logistic regression analyses, with P < .05 considered significant. Regression reference groups for the Medicaid cohort were male sex, White race (compared with Black, Hispanic/Latino, and “other” race [American Indian/Alaska Native, Native Hawaiian/Other Pacific Islander, ≥2 races, or other]), age 18-24 (compared with age 13-17), and basis of Medicaid eligibility of child (compared with person with blindness/disability, child in foster care, adult, and eligibility status unknown). Reference groups for the commercial cohort were male sex, age 18-24, and relationship to primary beneficiary of child/other (compared with self and spouse). Data on race/ethnicity were not available in the commercial database.
The HRSA medical visit frequency performance measure defines the denominator as the number of patients with a diagnosis of HIV infection with ≥1 medical visit in the first 6 months of the 24-month measurement period. 19 Our main analyses used the same criterion. We conducted a secondary analysis to assess possible differences in outpatient visit attendance among adolescents and young adults with no outpatient visit in the first 6 months of the 24-month measurement period but who otherwise met inclusion criteria. This project was determined to be research on nonhuman subjects. We conducted all analyses using SAS version 9.4 (SAS Institute, Inc).
Results
The Medicaid cohort included 378 adolescents and young adults, and the commercial insurance cohort included 1028 adolescents and young adults (Figure 1). The Medicaid cohort was predominantly female (n = 240, 63%), Black (n = 258, 68%), and aged 18-24 (n = 241, 64%) (Table 1). The commercial insurance cohort was predominantly male (n = 750, 73%) and dominated by young adults aged 18-24 (n = 883, 86%). The most common basis of Medicaid eligibility in the cohort was person with blindness/disability (n = 194, 51%). For the commercial insurance cohort, the most common relationship to primary beneficiary category was child/other (n = 618, 60%).
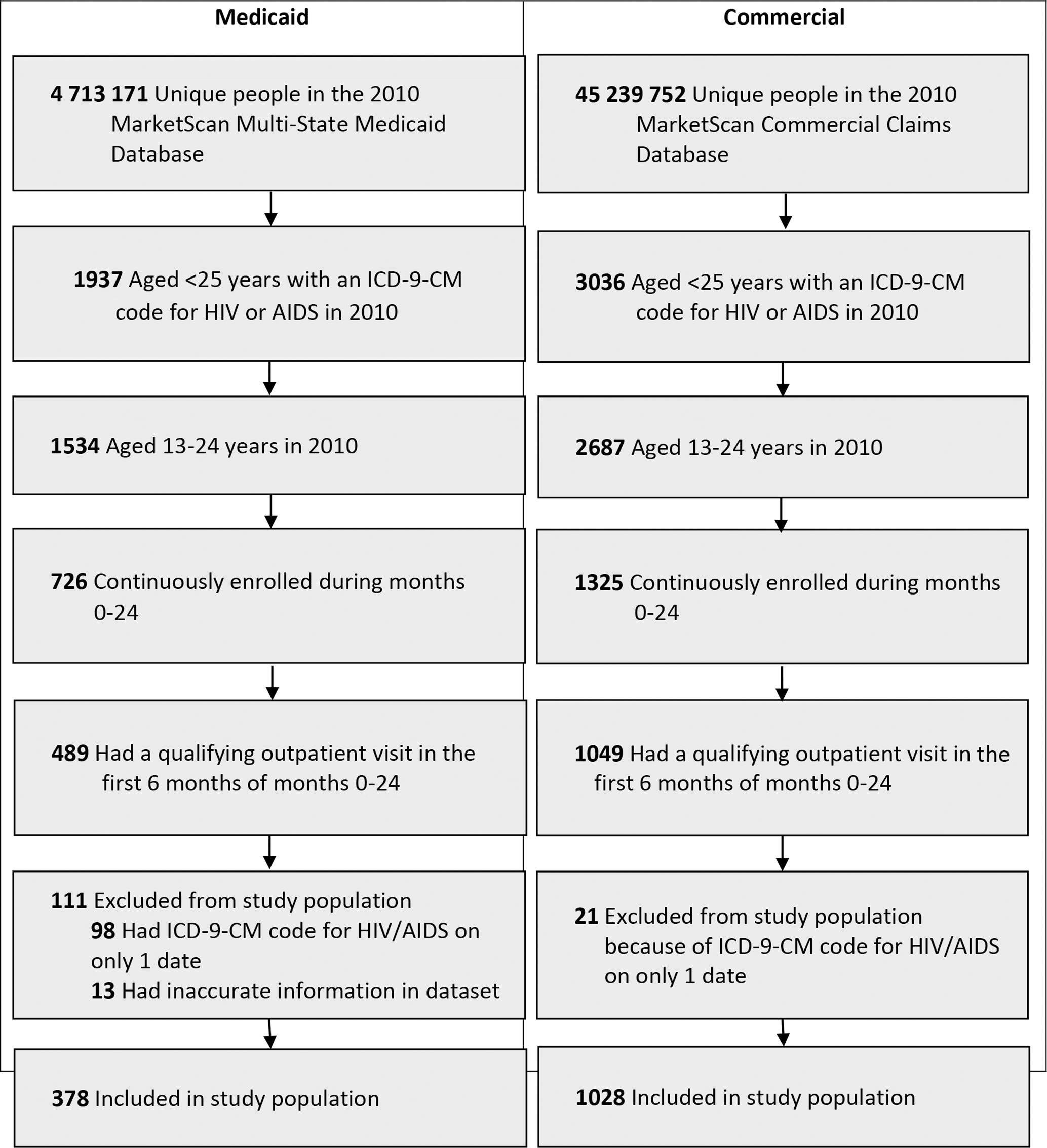
Selection criteria for study cohorts of Medicaid and commercially insured HIV-diagnosed adolescents and young adults aged 13-24, MarketScan Multi-State Medicaid and Commercial Claims and Encounters databases, 2010. Abbreviation: ICD-9-CM, International Classification of Diseases, Ninth Revision, Clinical Modification. Data source: Centers for Disease Control and Prevention. 18
Characteristics of Medicaid and commercially insured adolescents and young adults aged 13-24 with diagnosed HIV, MarketScan Multi-State Medicaid and Commercial Claims and Encounters databases, United States, 2010 a
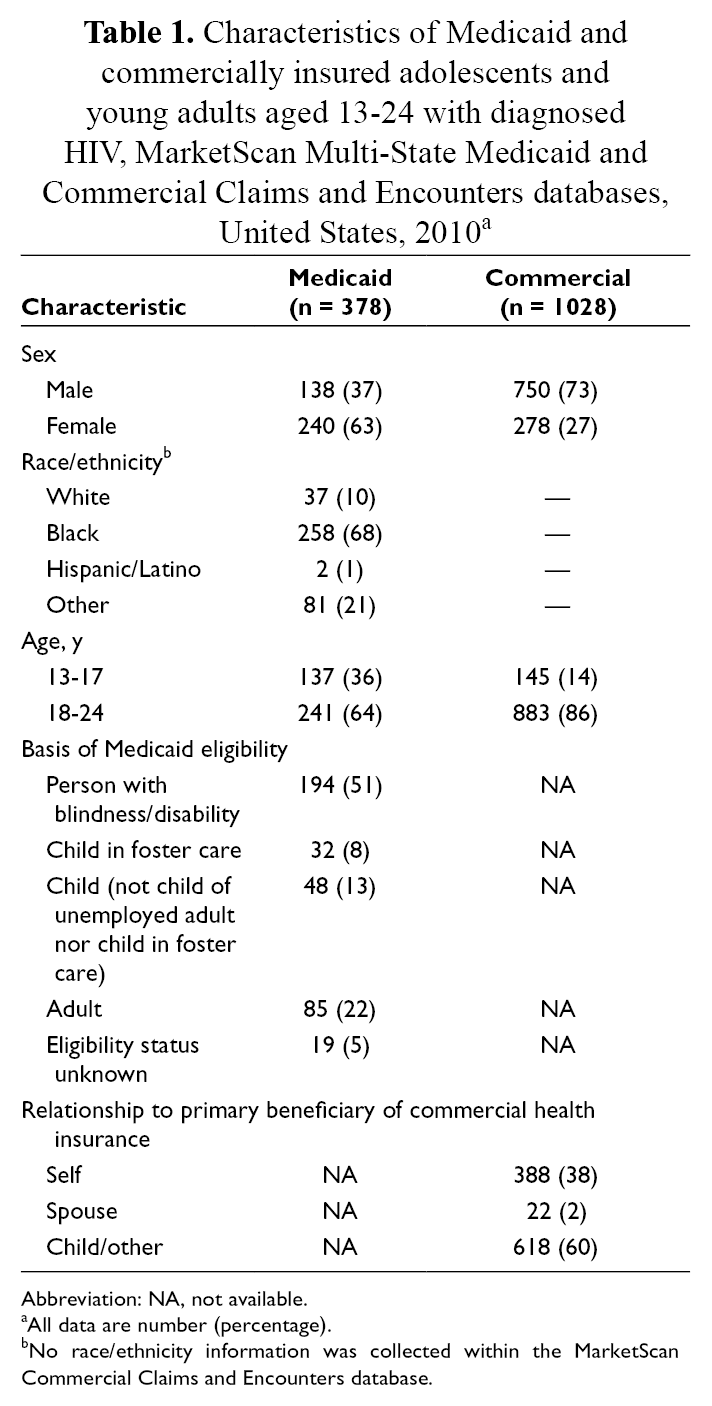
Abbreviation: NA, not available.
aAll data are number (percentage).
bNo race/ethnicity information was collected within the MarketScan Commercial Claims and Encounters database.
Retention in Care and In-Care Status Among Adolescents and Young Adults Enrolled in Medicaid
In the Medicaid cohort, 186 (49%) adolescents and young adults were retained in care during months 0-24 (Figure 2). In the retained-in-care subgroup, 31 (17%) adolescents and young adults were not enrolled for ≥10 months during months 25-36 and were excluded before the next stage of analysis; in the not-retained-in-care during months 0-24 subgroup, 38 (20%) adolescents and young adults were excluded from analysis. Of the remaining adolescents and young adults in the retained-in-care subgroup, 113 (73%) met the in-care during months 25-36 definition. Of the remaining adolescents and young adults in the not-retained-in-care during months 0-24 subgroup, 69 (45%) met the in-care definition during months 25-36.
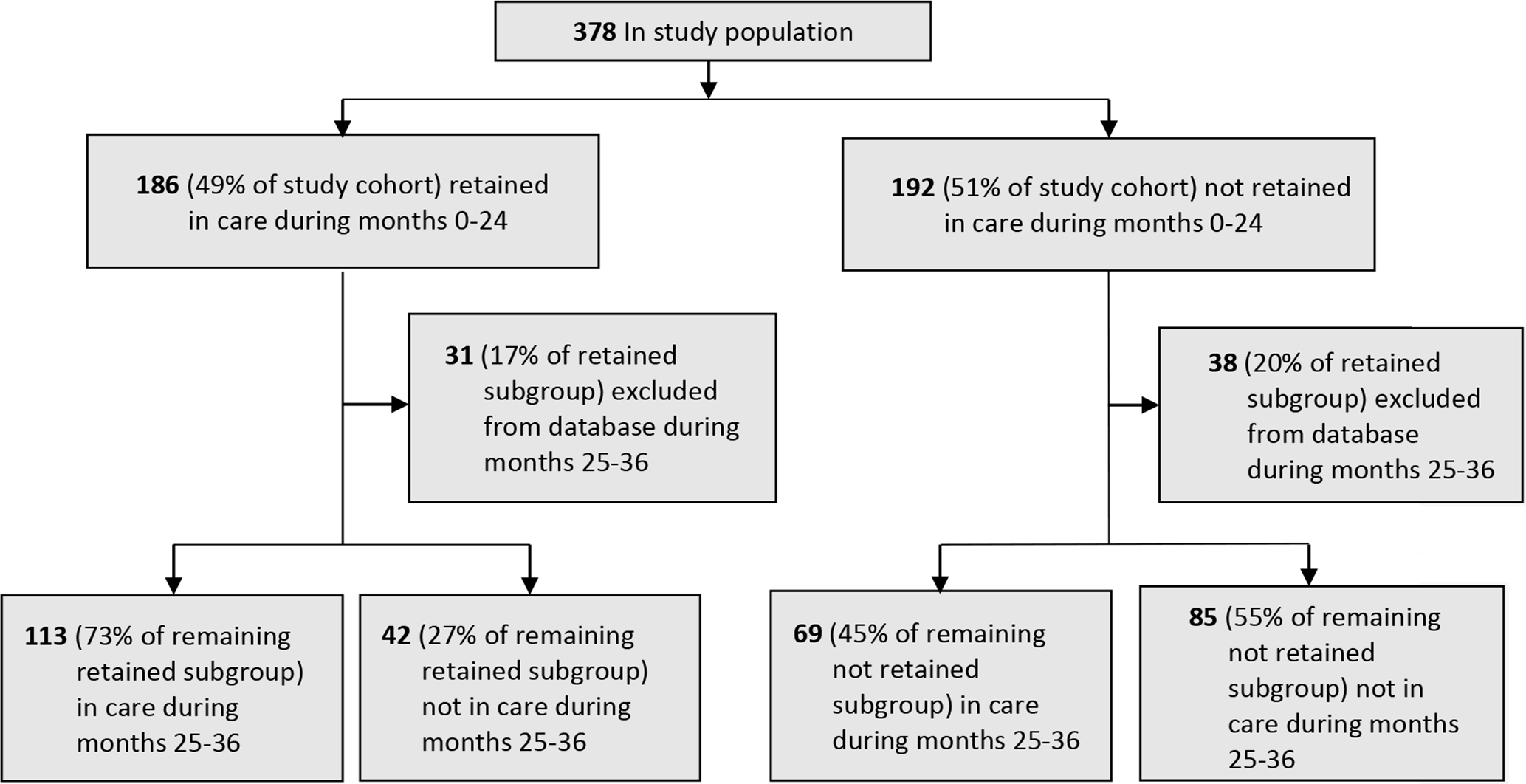
Retention in care and in-care status among Medicaid-insured adolescents and young adults aged 13-24 with diagnosed HIV infection, MarketScan Medicaid Multi-State databases, United States, 2010-2014.
Retention in Care and In-Care Status Among Commercially Insured Adolescents and Young Adults
In the commercial insurance cohort, 591 (57%) adolescents and young adults were retained in care during months 0-24 (Figure 3). In the retained-in-care during months 0-24 subgroup, 187 (32%) adolescents and young adults were not enrolled for ≥10 months during months 25-36 and were excluded before the next stage of analysis; in the not-retained-in-care during months 0-24 subgroup, 137 (31%) adolescents and young adults were excluded from analysis. Of the remaining adolescents and young adults in the retained-in-care during months 0-24 subgroup, 313 (77%) met the in-care definition during months 25-36. Of the remaining adolescents and young adults in the not-retained-in-care during months 0-24 subgroup, 94 (31%) met the in-care definition during months 25-36.
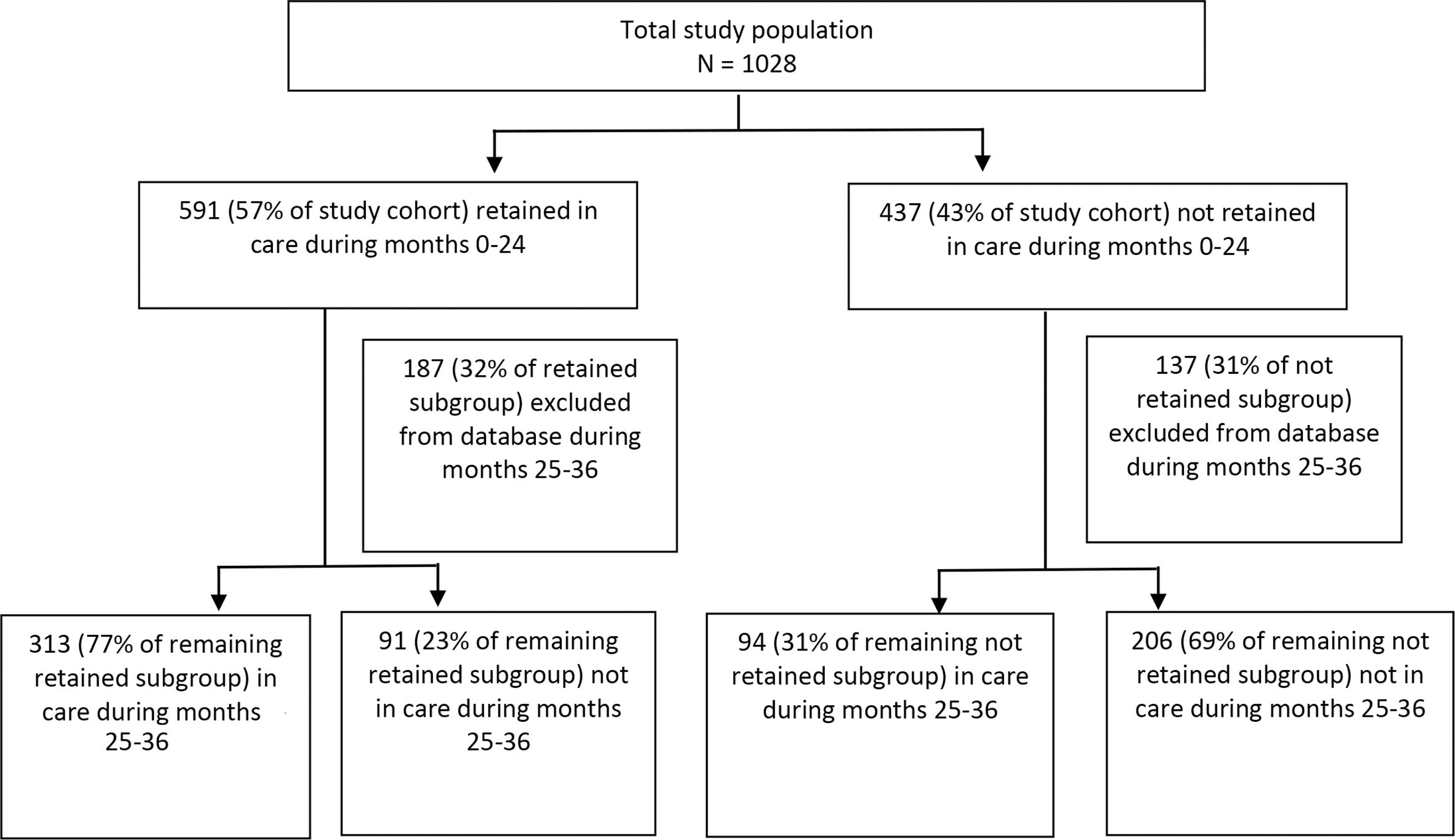
Retention in care and in-care status among commercially insured adolescents and young adults aged 13-24 with diagnosed HIV infection, MarketScan Commercial Claims and Encounters databases, United States, 2010-2014.
Factors Associated With Retention in Care
In the Medicaid cohort, we found no significant associations between retention in care during months 0-24 and any of the variables evaluated (Table 2). In the commercial insurance cohort, the relationship to primary beneficiary status of self and of spouse was significantly associated with a decreased odds of retention in care as compared with the status of child/other (odds ratio [OR] = 0.64; 95% CI, 0.49-0.83; and OR = 0.33; 95% CI, 0.12-0.91, respectively).
Bivariate logistic regression evaluating retention in care during 24 months of Medicaid and commercially insured HIV-diagnosed adolescents and young adults aged 13-24, MarketScan Multi-State Medicaid and Commercial Claims and Encounters databases, United States, 2010
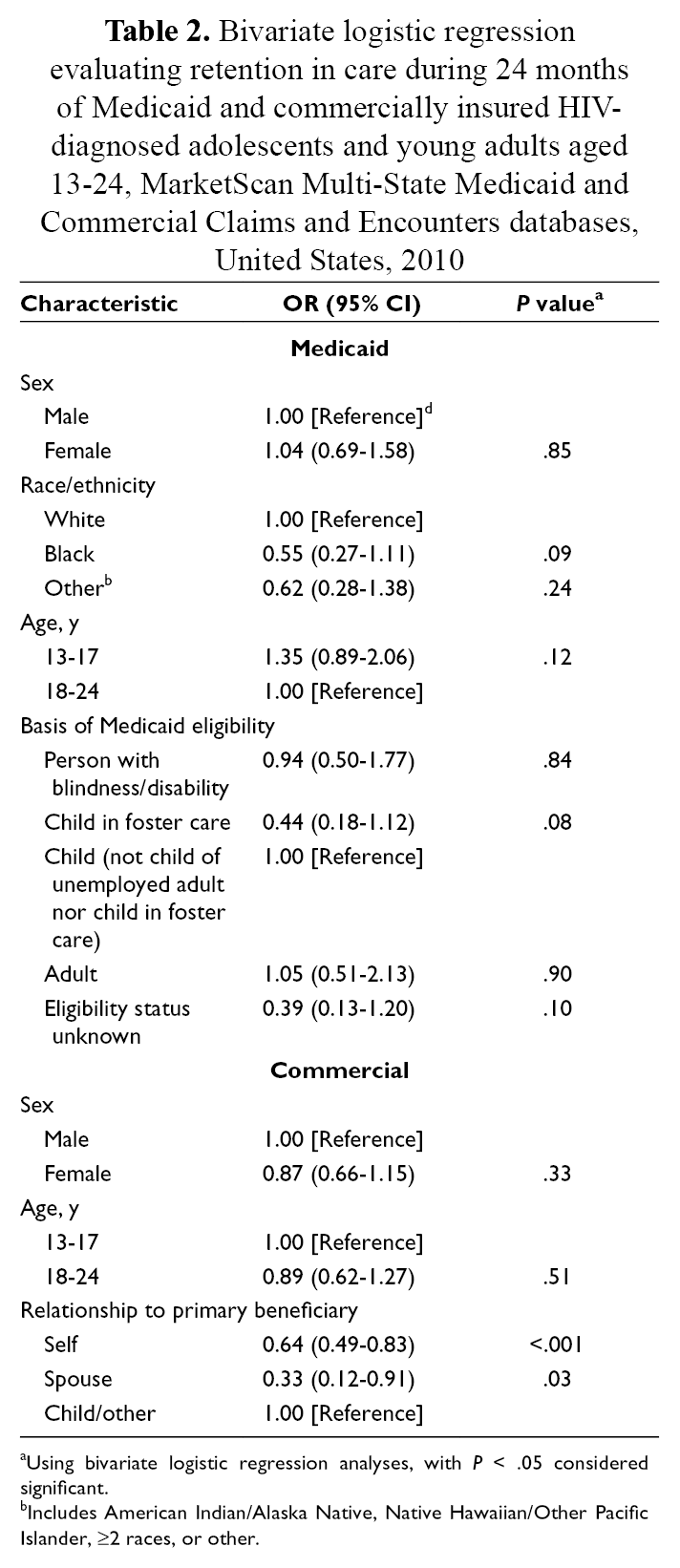
aUsing bivariate logistic regression analyses, with P < .05 considered significant.
bIncludes American Indian/Alaska Native, Native Hawaiian/Other Pacific Islander, ≥2 races, or other.
Outpatient Visit Attendance Among Adolescents and Young Adults With No Outpatient Visit in the First 6 Months of the 24-Month Measurement Period
From the Medicaid and commercial cohorts, respectively, 237 and 276 adolescents and young adults were excluded from the main analyses because they had no qualifying outpatient visit in the first 6 months of the study period. Among these adolescents and young adults, 51 (22%) in the Medicaid cohort and 126 (45%) in the commercial cohort had a qualifying outpatient visit in the second 6 months of the study period (months 7-12). In the Medicaid and commercial cohorts, respectively, 31 (13%) and 84 (30%) excluded adolescents and young adults met the in-care definition for months 13-24.
Discussion
Using a clinic-based definition of retention in care, we found that 49% and 57% of Medicaid and commercially insured adolescents and young adults, respectively, were retained in care during the study period; most remained in care through month 36. Our estimates of retention in care were lower than retention-in-care rates observed for HIV-diagnosed adults (aged ≥18) in similar analyses conducted with MarketScan claims data. 15,16 In those analyses, retention-in-care estimates for months 0-24 of the study periods were 61% for Medicaid-insured adults and 77% for commercially insured adults. 15,16 Our results, however, are similar to those reported in the National HIV Surveillance System report, of 55% for adolescents and young adults aged 13-24 diagnosed with HIV infection by year-end 2012 and alive by year-end 2013. 21 The National HIV Surveillance System uses HIV-specific laboratory tests to monitor retention in care at the national level.
Failure to retain adolescents and young adults with HIV infection in medical care may have a detrimental effect on their health. 8,22 Potential health consequences of suboptimally managed HIV infection during adolescence and young adulthood, such as development of antiretroviral drug resistance, opportunistic infections, or comorbidities, may continue to affect the health and medical care of young people into adulthood. Optimal management of HIV infection in adolescence and young adulthood improves the likelihood of achieving viral suppression, 14 which minimizes the risk of negative health outcomes from HIV, reduces the risk of transmission, and may reduce costs to the medical system. 23 In light of the importance of retention in medical care for adolescents and young adults with HIV infection, our findings of suboptimal retention in care among this population are particularly concerning. An intervention tailored to young people may successfully identify young people who are HIV infected, link them to care, and achieve high rates of retention in care. 24 Our findings indicate the need for more such interventions, with approaches tailored to the unique needs and characteristics of adolescents and young adults.
Adolescence is a unique neurodevelopmental stage associated with traits that may put young people at increased risk of nonretention. 25,26 For example, adolescence is characterized by an emphasis on peer relations, which may make adolescents particularly likely to attempt to conceal their HIV status by avoiding treatment. 27 Compared with adults, adolescents often have a greater propensity for taking risks and may be more likely to underestimate harm in the future because of choices made in the present. 25,28
Socioeconomic factors are associated with underuse of general medical services and poor HIV care outcomes for adolescents and young adults. 29 -31 Many young people are financially dependent on their families, or if they are independent, they may struggle to compete with adults in the employment market. 32,33 Overall, multiple levels of potential barriers to retention in care exist, from macro-level structural barriers to micro-level neurodevelopmental factors. 33
In general, a lack of health insurance is a possible barrier to retention in care, and adolescents and young adults without Medicaid or health insurance may have difficulties maintaining adequate medical visit frequency. 30 It is notable that in this study, we found suboptimal rates of retention in care among adolescents and young adults with Medicaid or private health insurance. These results are consistent with another study that found 29% of adolescents did not remain in care despite receiving services in an HIV clinic offering free medical care. 34 Ensuring access to care is a critical step to retaining patients in medical care. However, our findings further illustrate that adolescents and young adults may experience barriers to retention that extend beyond access to care. Adolescents and young adults with perinatally acquired HIV infection may have different barriers and facilitators to retention in care than people with nonperinatally acquired HIV infection. 35
In the Medicaid cohort, we found that more than half of adolescents and young adults categorized as not retained in care during months 0-24 were retained in care during months 25-36. This finding illustrates that adolescents and young adults may experience gaps in medical care without being lost to follow-up. However, gaps in care may be clinically important because they are associated with increased risks of viral rebound, decreased CD4 cell counts, and mortality. 22,36,37 Gaps in care may provide a red flag for health care providers to screen patients for factors associated with inadequate rates of retention in care among adolescents and young adults, including mental health concerns, substance abuse, and socioeconomic challenges. 30,38,39
Our finding, in the commercial insurance cohort, that the relationship to primary beneficiary status of self or spouse was associated with reduced odds of retention in care might be related to the fact that a relationship to the primary beneficiary status of child/other likely indicates that an adolescent or young adult is covered by his or her parents’ or guardians’ health insurance. Insurance under a parent’s policy may indicate a greater degree of familial support compared with adolescents categorized as the commercial insurance policy’s primary beneficiary or the primary beneficiary’s spouse. Social support is associated with improved attendance at outpatient clinic appointments. 40,41
We used the HRSA medical visit frequency performance measure to evaluate retention in care in this analysis. This measure includes as a denominator the number of patients with a diagnosis of HIV infection with ≥1 medical visit in the first 6 months of the 24-month measurement period. 19 When we evaluated adolescents and young adults who were excluded from the cohorts because of no qualifying outpatient visit in the first 6 months, we found that low proportions of these adolescents and young adults were in care during months 13-24. By excluding people with no medical visit in the first 6 months of the measurement period, the HRSA medical visit frequency criterion preferentially excludes adolescents and young adults with suboptimal visit consistency. An approach to assessing retention in care that included these individuals may have shown even more concerning retention-in-care proportions. Consideration of a subpopulation of adolescents and young adults excluded from our main analysis continues to support the conclusion that many adolescents and young adults with HIV infection in the United States do not have the recommended frequency of medical visits.
Limitations
Our study had several limitations. First, data on HIV transmission category were not available; as such, we were not able to evaluate differences in adolescents and young adults living with perinatally versus nonperinatally acquired HIV infection. Second, the counted outpatient visits may have been for non–HIV-related medical issues, as the data did not allow for specific identification of HIV primary care visits. Third, the health care provider type variable, in the MarketScan databases, consists of codes that indicate the type of medical professional (eg, physician, nurse practitioner) associated with a claim; however, it also contains codes that indicate the facility associated with a claim (eg, acute care hospital). Because we were unable to ascertain the characteristics of claims associated only with facility codes, those claims were not counted as outpatient visits in our study, which could have resulted in an underestimation of retention. Claims associated only with facility codes were more common in the Medicaid database than in the commercial insurance database. Fourth, results from the Medicaid and commercial cohorts could not be directly compared because of underlying differences in the databases and the inability to exclude overlap between database populations. Fifth, the states included in the Medicaid database are not identified, so we were unable to assess geographic distribution. Sixth, retention in care and HIV viral suppression are separate metrics; retained versus not retained in care may or may not correlate with viral suppression. In general, adequate frequency of HIV care visits is an important component of attaining viral suppression for people with HIV infection; as such, retention in care is a useful metric in assessing the adequacy of HIV medical care. Lastly, we calculated the unweighted proportions of retention in care; as such, our findings are not generalizable to the total population of HIV-diagnosed adolescents and young adults in the United States.
Conclusion
Our findings indicate that, even among adolescents and young adults with Medicaid or private health insurance, many adolescents and young adults with HIV infection in the United States have suboptimal retention in medical care. It is imperative to address these findings because poor retention in care puts adolescents and young adults at increased risk of poor HIV-related health outcomes. Our findings support the need for initiatives to increase retention in HIV care among this vulnerable population.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.