
Abstract
Objectives
Studies describing linkage of ambulance trips and emergency department (ED) visits of patients with opioid-related overdose (ORO) are limited. We linked records of patients experiencing ORO from ambulance trip and ED visit records in Massachusetts during April 1–June 30, 2017.
Methods
We estimated the positive predictive value of ORO-capturing definitions by examining the narratives and triage notes of a sample of OROs from each data source. Because of a lack of common unique identifiers, we deterministically linked OROs to records in the counter data set on date of birth, incident date, facility, and sex. To validate the linkage strategy, we compared ambulance trip narratives with ED triage notes and chief complaints for a sample of pairs.
Results
Of 3203 ambulance trips for ORO and 3046 ED visits for ORO, 82% and 63%, respectively, matched a record in the counter data set on date of birth, incident date, facility, and sex. In 200 randomly selected linked pairs from a final linked data set of 3006 paired records, only 5 (3%) appeared to be false matches.
Practice Implications
This exercise demonstrated the feasibility of linking ORO records between 2 data sets without a unique identifier. Future analyses of the linked data could produce insights not available from analyzing either data set alone. Linkage using 2 rapidly available data sets can actively inform the state’s public health opioid overdose response and allow for de-duplicating counts of OROs treated by ambulance, in an ED, or both.
Researchers have linked records of people experiencing opioid-related overdose (ORO) from electronic health records, ambulance records, and other data sources. 1 -3 However, few studies have linked ORO records from rapidly available emergency department (ED) surveillance data. A linked data set including ED surveillance data and ambulance trip data can be produced in a more timely fashion than one that uses traditional ED discharge data alone. Linked surveillance data with a low false matching rate could be used by public health authorities to more accurately quantify OROs transported by ambulance and managed in the ED, with less of a lag in time between when an ORO occurs and when it can be included in analyses of trends. Given the dynamic nature of the opioid epidemic, this method supports public health responses that are informed by updated trends in ORO. In this study, we evaluated the feasibility of linking records of ORO events using both Massachusetts Ambulance Trip Record Information System (MATRIS) and Massachusetts Department of Public Health Syndromic Surveillance (MDPH SyS) from April 1 through June 30, 2017. We hypothesized that deterministic linkage could provide a data set with a low false match rate.
Materials and Methods
Population
Selection of ORO records for inclusion in the linkage
Emergency medical services personnel in the field generated reports that composed the ambulance trip records within MATRIS. Information available included incident date, time of arrival in the field, patient demographic characteristics (date of birth, sex), patient’s chief and secondary complaints, ambulance personnel’s primary and secondary impressions of the diagnosis, medications administered to the patient by ambulance personnel, name of facility to which the patient was transported, and a free-text narrative report written by ambulance personnel describing the patient’s condition, treatment, and transport. To identify ORO-related ambulance trips, we used an algorithm that searches for text indicators, such as “heroin” or “naloxone,” in the narrative report; chief and secondary complaints; medication administration; and primary impression fields. To flag an ambulance trip record as ORO, we selected those trips with a single indicator supporting ORO as the main reason for ambulance attendance in the chief or secondary complaint, or ≥2 indicators indicating ORO as the main reason for ambulance attendance in any of the other fields examined.
MDPH SyS compiles ED visit records from admit, discharge, and transfer messages sent from the electronic health record. Information available for each ED visit includes admission date and time; patient demographic characteristics (date of birth, age, or both [facilities can opt to send age in lieu of date of birth]); patient sex; chief complaint; diagnostic codes in International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) or International Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10-CM) format 4,5 ; and triage notes. To flag ORO, we searched for text elements in the chief complaint and triage note, and we searched the diagnostic fields in each ED visit record. We flagged records as ORO that had combinations of indicators in the chief complaint or triage note, or selected ICD-9-CM or ICD-10-CM codes consistent with opioid overdose. Both the MATRIS and MDPH SyS ORO algorithms incorporated inclusive definitions (a record documenting “heroin” or “overdose” was included as a case) and exclusive definitions (a record documenting “detoxification” in reference to requesting in-hospital detoxification treatment). The MDPH Internal Review Board waived institutional review board review for this study.
To quantify the accuracy of the ORO-capturing definitions, we examined randomly selected OROs from each data source to estimate the proportion that were true ORO events (positive predictive value [PPV]) by using a combination of clinical signs (respiratory compromise [decreased oxygen saturation], decreased [or absent] rate of respirations, or decreased level of consciousness) as the gold standard definition. 6 The overall PPV for ORO-flagged records among ambulance trip records was 85% (95% CI, 80%-89%) and for ED visit records was 76% (95% CI, 70%-81%). The most prevalent cause of a false-positive assignment was drug intoxication, without respiratory compromise or altered mental status to the degree that would threaten the airway. Less prevalent false-positive results were cases of intoxication with non-opioid substances, including alcohol, cocaine, crack, methamphetamines, or a combination of these substances.
Exclusion criteria
We restricted ORO cohorts from both data sources to incidents that occurred from April 1 through June 30, 2017. Only people aged ≥11 years were included because children are likely to accidentally ingest opioids, and we wanted a cohort that consisted of intentional opioid consumption. We excluded 31 facilities from the study because they did not submit data to MDPH SyS or did not provide the optional date of birth field needed for the linkage algorithm. We also excluded ambulance trip ORO records documenting that the patient was not transported to a medical facility, because these trips would not be expected to link to an ED visit. We included 39 facilities in the final linkage data set, representing approximately 60% of Massachusetts ED visits during the study period.
Linkage Approach
Because the data sources and the ORO definitions differ, we assumed that the 2 data sources captured overlapping but different ORO cohorts. Therefore, we executed a linkage strategy in which all flagged OROs from one data set (the “anchoring” data set) were matched against all records in the counter data set. We executed 2 merges in this way: one anchored on ORO-flagged ambulance trip records and the other anchored on ORO-flagged ED visit records. Using this strategy, an uncaptured ORO in either data set could be captured by pairing it with a flagged record in the anchoring data set. In theory, this linkage strategy captured data on a higher proportion of all OROs in Massachusetts during the study period than either ORO definition alone, thereby increasing capture of data on OROs treated in an ED or attended by ambulance in Massachusetts during the study period. We set together pairs from each of the 2 linkages, with duplicate pairs removed so that each observation in the linked data set was a unique ORO event.
Probabilistic linkage considers a combination of values in a pair of fields from 2 data sources and defines µ, the probability of observing the combination in a true match, and u, the probability of observing the combination in a false match. We chose deterministic linkage instead of probabilistic linkage to limit false matches, which may occur when probabilistic linkage deems a pair as matched because of a high overall match weight (an index that incorporates µ and u), even though the pair has discrepant values in ≥1 match field. 7 Because no common unique identifier was available in both data sources, we executed a deterministic linkage based on date of birth, incident date, facility, and sex. We used only records in the counter data set without missing values for any of these 4 fields. We standardized medical facility name between the 2 data sets, which included combining some facilities by health care system. We paired OROs from each anchoring data set with records in the counter data set that matched on date of birth, incident date (+1 day to allow for ambulance attendances occurring before midnight but arriving at the ED after midnight), facility, and sex. If a pair of records matched on all 4 fields, we considered that pair linked and it remained in the final linked data set. Some ORO records matched to >1 record in the counter data set. For the ambulance trip–anchored linkage, 191 ORO ambulance trips paired with >1 ED visit; for the ED visit–anchored linkage, 203 ORO ED visits paired with >1 ambulance trip. To select 1 record from among several records paired with a single ORO, we developed an algorithm designed to optimize selection of the true match. We removed records that were not flagged as ORO and sorted the remaining records by ED time of admission (ambulance trip–anchored linkage) or arrival time of the ambulance in the field (ED visit–anchored linkage). We selected the first of the former and the last of the latter to pair with the anchoring ORO.
Validation of the linkage approach
To validate the accuracy of the pairing produced by the linkage strategy, we randomly selected 100 pairs from both the ambulance trip–anchored linkage and ED visit–anchored linkage for review. Each batch included 50 pairs in which the anchoring ORO was paired with a record that was not flagged as ORO. In each randomly selected pair, we reviewed narrative reports from the ambulance trip record and compared that with information in the triage note and chief complaint of the ED visit record, to determine whether the pair appeared to be a true match or a false match. If unique details of the person-event’s history were reflected in the paired records’ text, we deemed the case-record pair a true match. Because of sparse triage notes and chief complaint fields in some ED visits, definitive validation was not possible in some cases. Often, however, a simple chief complaint of “overdose” would support that the ORO described in the matched ED visit record was a possible match to the ambulance trip.
Analyses on the final linked data set
For each cohort of ORO, we present the rate of matching on 2, 3, and 4 fields to a record in the counter data set. We present the linkage rate on 4 fields by month of the incident and by county (location of the incident for ambulance trips, location of the facility for ED visits) in Massachusetts. We used the χ2 test to compare linkage rates by month and county, with P < .05 considered significant. We determined age for each paired ORO by comparing the date of the incident and the date of birth and present the median (interquartile range [IQR]) age of the de-duplicated linked data set, along with the proportion of males and females. Using indicators based on text strings in the narrative, chief and secondary complaints, medication administration, and primary impression in the ambulance trip data, we estimated the proportion of the final linked data set that possibly used heroin during the ORO event, as well as the proportion that were administered naloxone by ambulance personnel. We used SAS Studio version 3.6 (SAS Institute, Inc) for all analyses.
Results
We identified 3203 ambulance trips for linkage with ED visits, and we identified 3046 ED visits for linkage with ambulance trips (Figure). Of 3203 ambulance trips for ORO, 2613 (82%) matched an ED visit on the 4 fields examined (Table 1). Of 3046 ED visits for ORO, 1907 (63%) matched an ambulance trip on the 4 fields examined. Of 2613 ambulance trips for ORO paired to ED visits, 1655 (63%) were paired to an ED visit that was also flagged as ORO. Of 1907 ED visits for ORO paired to ambulance trips, 1536 (81%) were paired to a trip that was also flagged as ORO. Because the data source–specific ORO-capturing algorithms (see the Methods section) and the linkage algorithm (match on date of birth, incident date, facility, and sex) differed, 47% of the ambulance trips and 19% of the ED visits paired with ED visits and ambulance trips, respectively, were not flagged as ORO.
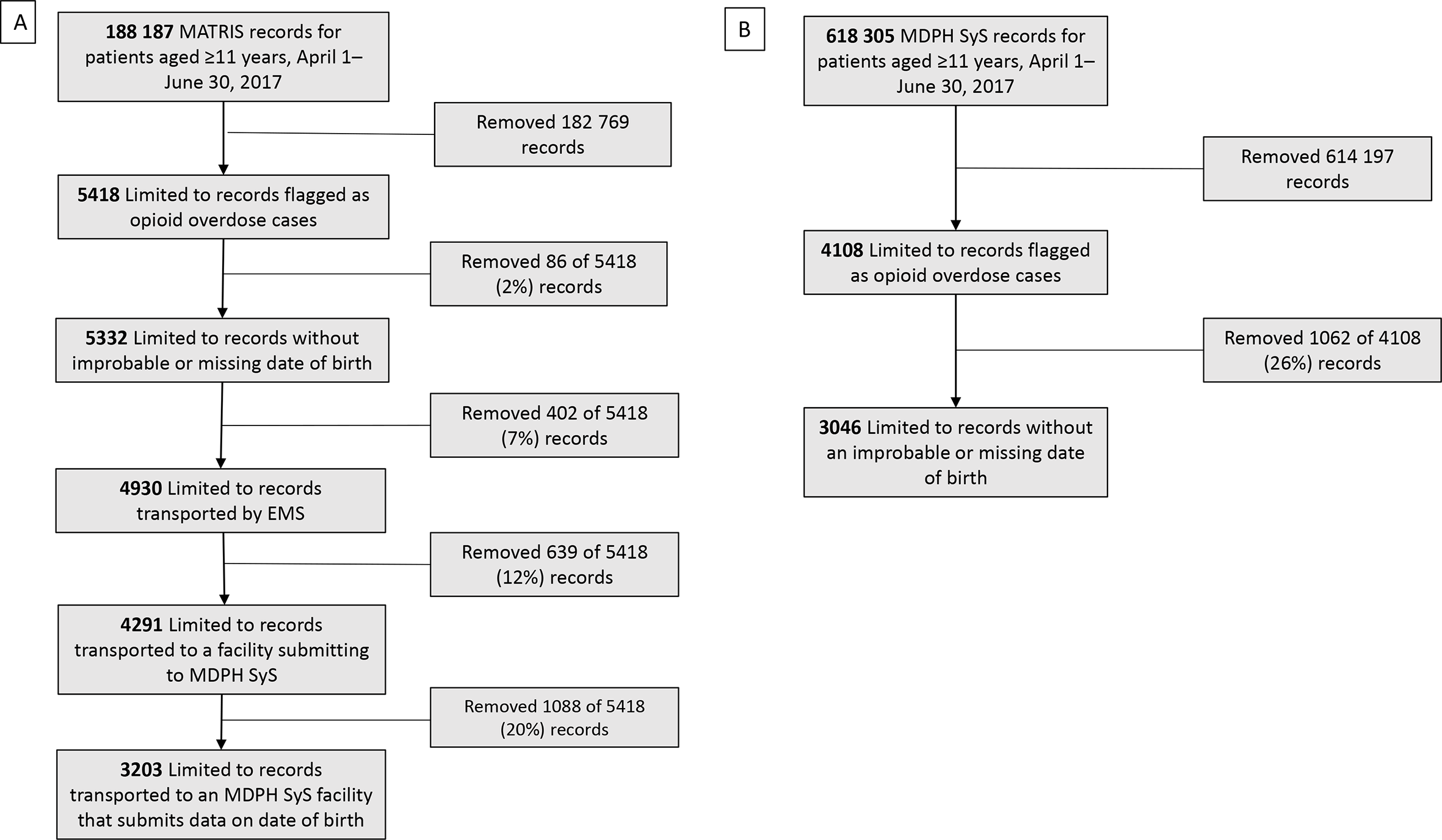
Selection of people experiencing opioid-related overdoses from (
Number of opioid-related overdose ambulance trip and emergency department (ED) visit records matching on 2, 3, and 4 fields, Massachusetts, April 1–June 30, 2017 a
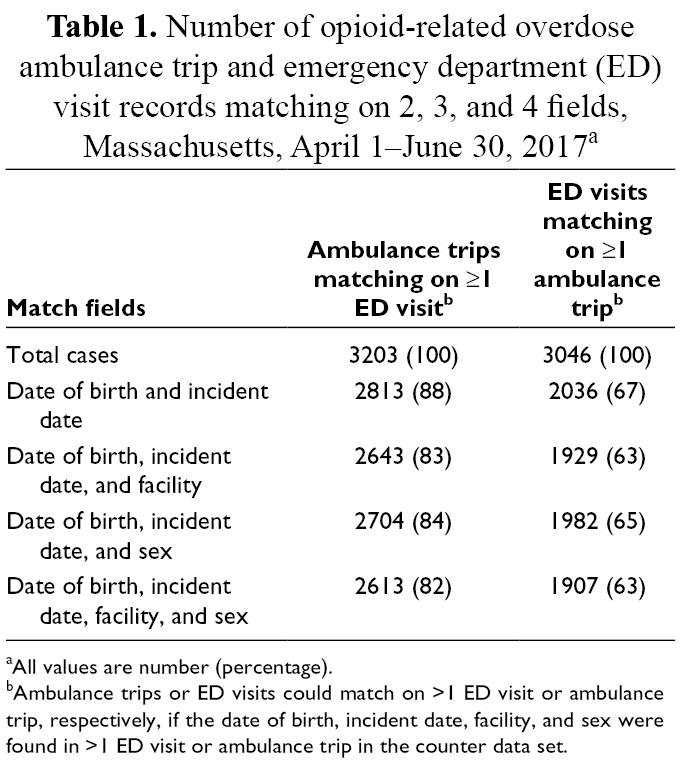
aAll values are number (percentage).
bAmbulance trips or ED visits could match on >1 ED visit or ambulance trip, respectively, if the date of birth, incident date, facility, and sex were found in >1 ED visit or ambulance trip in the counter data set.
Of all reviewed pairs, only 3% appeared to be false matches (estimated PPV for a true match, 97%) (Table 2). We adjudicated 148 (74%) to be true matches and 47 (24%) to be possible matches. Of 50 OROs matching to non-OROs, 35 (70%) ambulance trips and 41 (82%) ED visits appeared to be true matches. Of the 5 false matches identified, 4 were instances of ORO from 1 data source pairing with a non-ORO in the counter data set. The linkage produced 3006 unique pairs representing ORO attended by ambulance and treated in the ED. The median (IQR) age of people included in the linked data set was 36 (29-48) years, and two-thirds were male. We also found that most (53%) linked OROs in our study had indicators that suggested possible heroin use in the ambulance trip record, although toxicology results were not available in either data source. Sixty-three percent had indicators for naloxone administration by ambulance personnel.
Result of validation of linked pairs of ambulance trips and emergency department (ED) visits for opioid-related overdose (ORO), stratified by matching to flagged or unflagged records in the counter data sets, Massachusetts, April 1–June 30, 2017 a
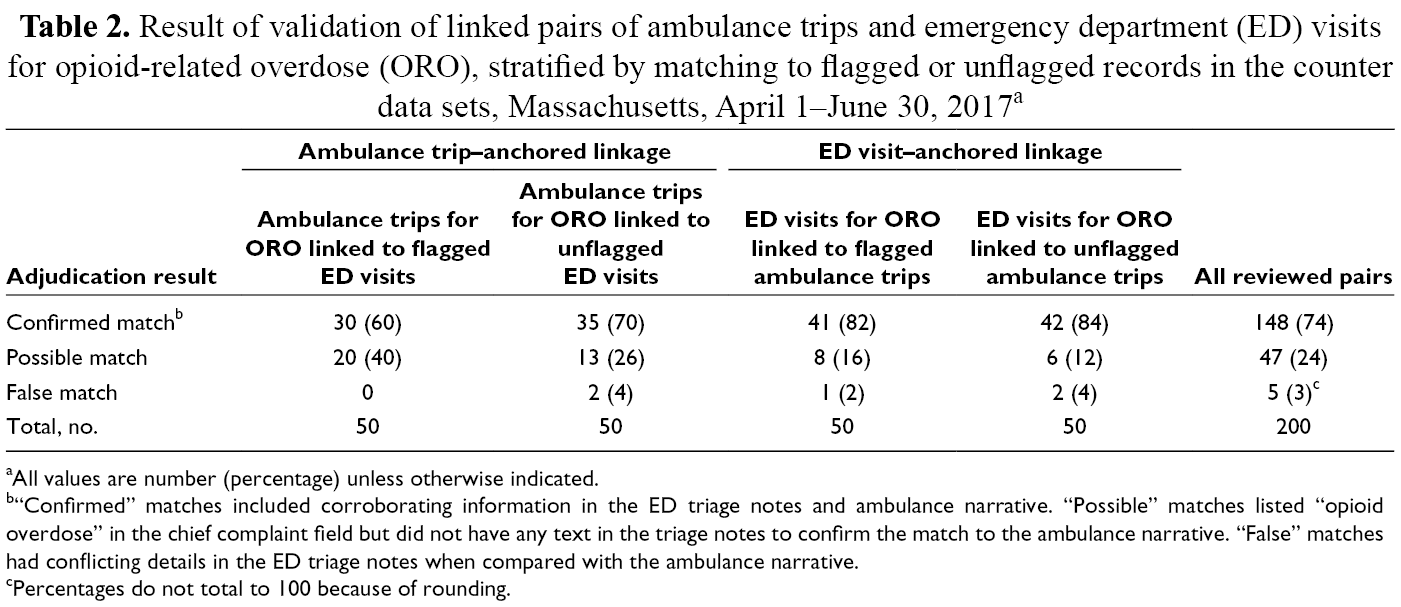
aAll values are number (percentage) unless otherwise indicated.
b“Confirmed” matches included corroborating information in the ED triage notes and ambulance narrative. “Possible” matches listed “opioid overdose” in the chief complaint field but did not have any text in the triage notes to confirm the match to the ambulance narrative. “False” matches had conflicting details in the ED triage notes when compared with the ambulance narrative.
cPercentages do not total to 100 because of rounding.
We found no significant difference in linkage rate by month for the ambulance trip–anchored linkage, but the linkage rate was significantly lower in April (59%) than in May (63%) or June (65%) in the ED visit–anchored linkage (P = .02) (Table 3). Although we found significant variability in linkage rates by county for both ambulance trips and ED visits for ORO (P < .001), linkage rates for most counties were close to the average linkage rate for the entire cohort. For Bristol, Middlesex, Norfolk, and Plymouth counties, 4-field match rates for both ambulance trips and ED visits were higher than the average rates for each of these linkages. For Essex County, a low ambulance trip linkage rate, relative to the average ambulance trip linkage rate of 82%, was coupled with a relatively high ED visit linkage rate. In Berkshire and Suffolk counties, high ambulance linkage rates were coupled with low ED visit linkage rates. Ambulance trips from Worcester County linked at a low rate compared with the average ambulance trip linkage rate, whereas ED visits in Worcester County linked at approximately the same rate as the average linkage rate for all ED visits.
Number of ambulance trips and emergency department (ED) visits for people experiencing opioid-related overdose, linked on 4 fields, by month and county, Massachusetts, April 1–June 30, 2017
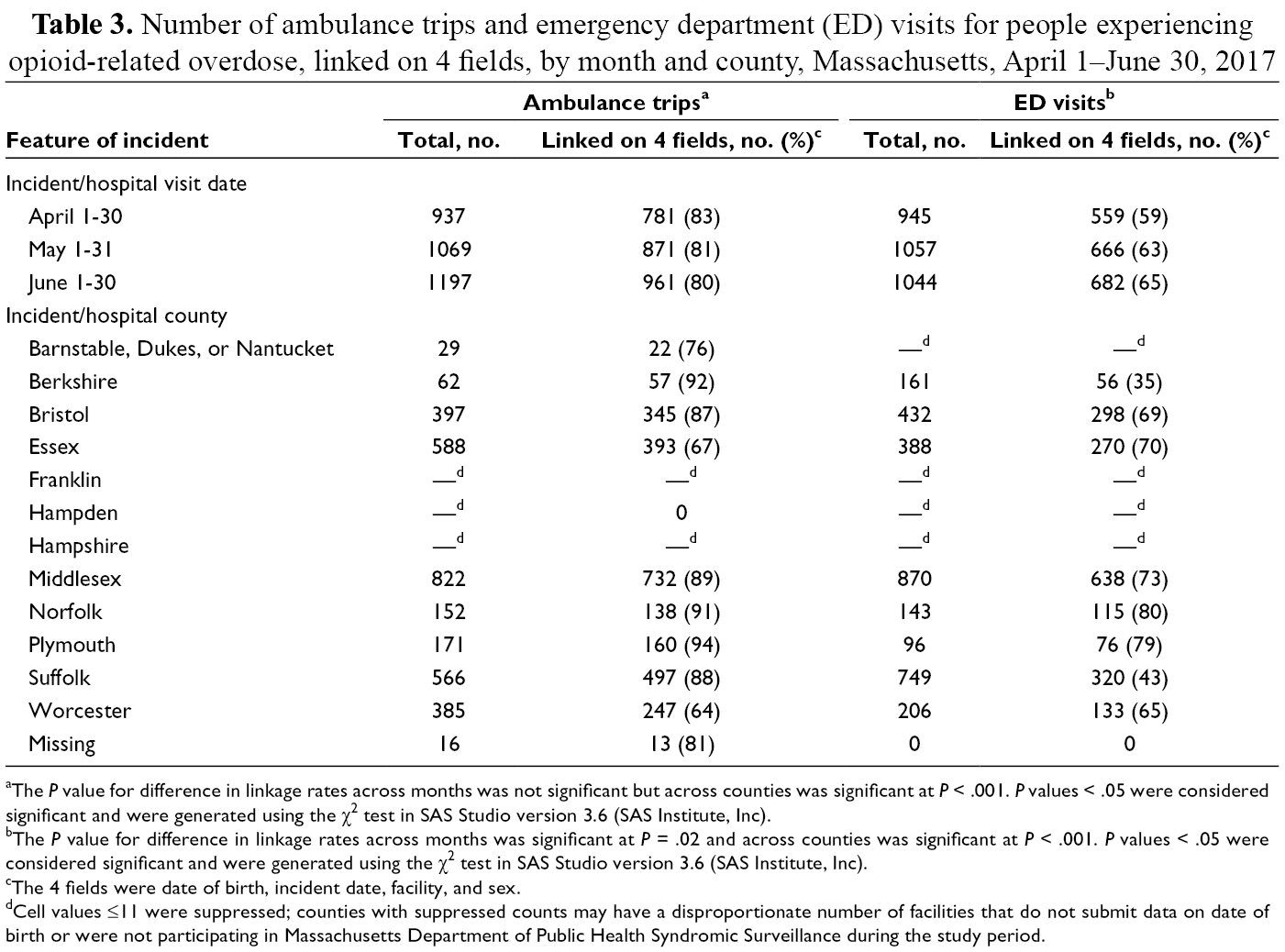
aThe P value for difference in linkage rates across months was not significant but across counties was significant at P < .001. P values < .05 were considered significant and were generated using the χ2 test in SAS Studio version 3.6 (SAS Institute, Inc).
bThe P value for difference in linkage rates across months was significant at P = .02 and across counties was significant at P < .001. P values < .05 were considered significant and were generated using the χ2 test in SAS Studio version 3.6 (SAS Institute, Inc).
cThe 4 fields were date of birth, incident date, facility, and sex.
dCell values ≤11 were suppressed; counties with suppressed counts may have a disproportionate number of facilities that do not submit data on date of birth or were not participating in Massachusetts Department of Public Health Syndromic Surveillance during the study period.
Discussion
Using a deterministic approach anchored on OROs identified from the 2 data sources, we linked 3006 ambulance trips with ED visits, with an estimated false match rate of 3%. To optimize capture of OROs attended by ambulance and treated in the ED, we used a 2-way strategy in which each ORO from 1 data source was compared with all records in the counter data set, including those not flagged as ORO. Our linked data set included a population that was similar to that reported in a previous study of ORO deaths in Massachusetts, in which 71% of linked events occurred among males, 81% occurred among people aged ≤44 years, and 66% involved heroin. 8 Unlike other studies that linked ambulance trips to traditional ED discharge records, we linked rapidly available ED surveillance data with ambulance trip data. 9 -13 Traditional ED discharge data include more comprehensive diagnostic fields that are standardized, resulting in less variability in diagnostic coding than in ED surveillance data. However, ED surveillance data are available more rapidly, allowing for more timely generation of linked data, and we found such data to be reliable enough to produce a linkage data set with few false matches. Studies have reported ambulance trip–anchored linkage rates ranging from 90% to 94% using matching algorithms incorporating date of birth, incident date, facility, and sex, among other fields. 7,8 Using algorithms similar to ours, studies reporting linkages anchored on ED visits reported rates ranging from 39% to 84%. 9 -11
Most states have ED surveillance and ambulance trip data collection systems through their participation in the National Syndromic Surveillance Program and a program for ambulance services to report trips to the National Emergency Medical Services Information System. 14,15 However, execution of a successful linkage at the state level requires complete and accurate reporting on date of birth, incident date, facility, and sex, at a minimum. Data quality and data completeness reported to ED and ambulance surveillance systems vary both between and within states. In Massachusetts during the study period, not all facilities reported to the ED surveillance system; therefore, OROs treated in these facilities are not represented in the final linked data set. In addition, many facilities that did submit to the ED surveillance system did not report date of birth. We estimate that the final linkage data set represents approximately 60% of Massachusetts ED visits during the study period. As an illustration of the effect of data quality variability in the state, we found variability in linkage rates by county, which we suspect is caused by variability in the quality of submitted data from hospitals and local ambulance services.
We examined why some OROs from each data source did not link. Of the 590 (18%) ambulance trips that did not link, we found that 11% transported the patient to an ED that allowed for documenting sex as “unknown.” ED documentation of sex as “unknown” might have resulted in non-linkage of some ambulance trips. We could not determine possible causes of non-linkage for the remainder of the 590 unlinked ambulance trips for ORO. For the ED visit–anchored linkage, some OROs that did not link may have arrived at the ED by means other than ambulance. No reliable field documented mode of arrival in MDPH SyS, and patients arriving via some other modality (eg, brought in by car by a family member) could not be identified and excluded from the ED visit denominator. We reviewed the triage notes of 100 randomly selected non-linking ED visits and found that 49% of these visits had “arrival by ambulance” documented in the triage note. Arrival by means other than ambulance may explain some but not all non-linked ED visits for ORO. Finally, other potential causes of non-linkage peculiar to this patient cohort may include inaccurate reporting of date of birth because of the patient’s decreased level of consciousness.
Practice Implications
The opioid epidemic is dynamic. As such, updated data reflecting changing trends are critical to implementing an effective public health response. In this pilot study, we demonstrated that the deterministic linkage of records of OROs captured in frequently updated ambulance trip and ED surveillance data can produce a reliable data set that is representative of OROs treated in both systems, with few false matches. The linkage allows for more accurate counting of OROs, because events captured in both data sources can be identified and removed from the count. Because each data source contains fields the other does not, characteristics of OROs can be examined in the linked data set that cannot be examined using either data source alone. This linkage strategy could be used as part of a comprehensive statewide surveillance of OROs attended by ambulance and treated in an ED.
Supplemental Material
Online supplementary file 1 - Supplemental material for Linking Ambulance Trip and Emergency Department Surveillance Data on Opioid-Related Overdose, Massachusetts, 2017
Supplemental material, Online supplementary file 1, for Linking Ambulance Trip and Emergency Department Surveillance Data on Opioid-Related Overdose, Massachusetts, 2017 by Catherine Rahilly-Tierney, Arman Altincatal, Anna Agan, Stefanie Albert, Rosa Ergas, Lauren Larochelle and Jeffrey Yu in Public Health Reports
Footnotes
Acknowledgments
The authors acknowledge Dana Bernson, Amy Bettano, Catherine Brown, Ridgely Ficks, Katherine Fillo, Gillian Haney, Katarina Jones, Monina Klevens, Sita Smith, Sarah Ruiz, and Sanouri Ursprung, who provided feedback on draft versions of the article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by the Centers for Disease Control and Prevention grant number 6NU17CE924877.
Supplemental Material
Supplemental material for this article is available online.