
Abstract
During the Russian influenza pandemic, which reached the United States in late 1889, US public health officials attempted to document the number of deaths associated with this disease outbreak. A historical perspective illuminates the complex categories used to classify deaths from influenza-associated diseases; substantial changes in weekly, monthly, and yearly death totals; and thoughtful efforts by health officials to measure the epidemic as it happened. The 1114 influenza deaths reported by the Connecticut State Board of Health in the 3 years after the January 1890 outbreak must be supplemented by the notable increases in the number of deaths from respiratory diseases, which elevates the likely toll to more than 7000 deaths during the epidemic. Whereas historians of public health have primarily examined efforts to control communicable diseases, this case study of mortality statistics reported by town officials and analyzed by the Connecticut State Board of Health demonstrates how officers of the local boards of health also responded to unexpected outbreaks of a familiar disease such as influenza. Understanding how organizations measured influenza-associated mortality illustrates an important stage in the development of American public health and also makes an important contribution to studying pandemics in history.
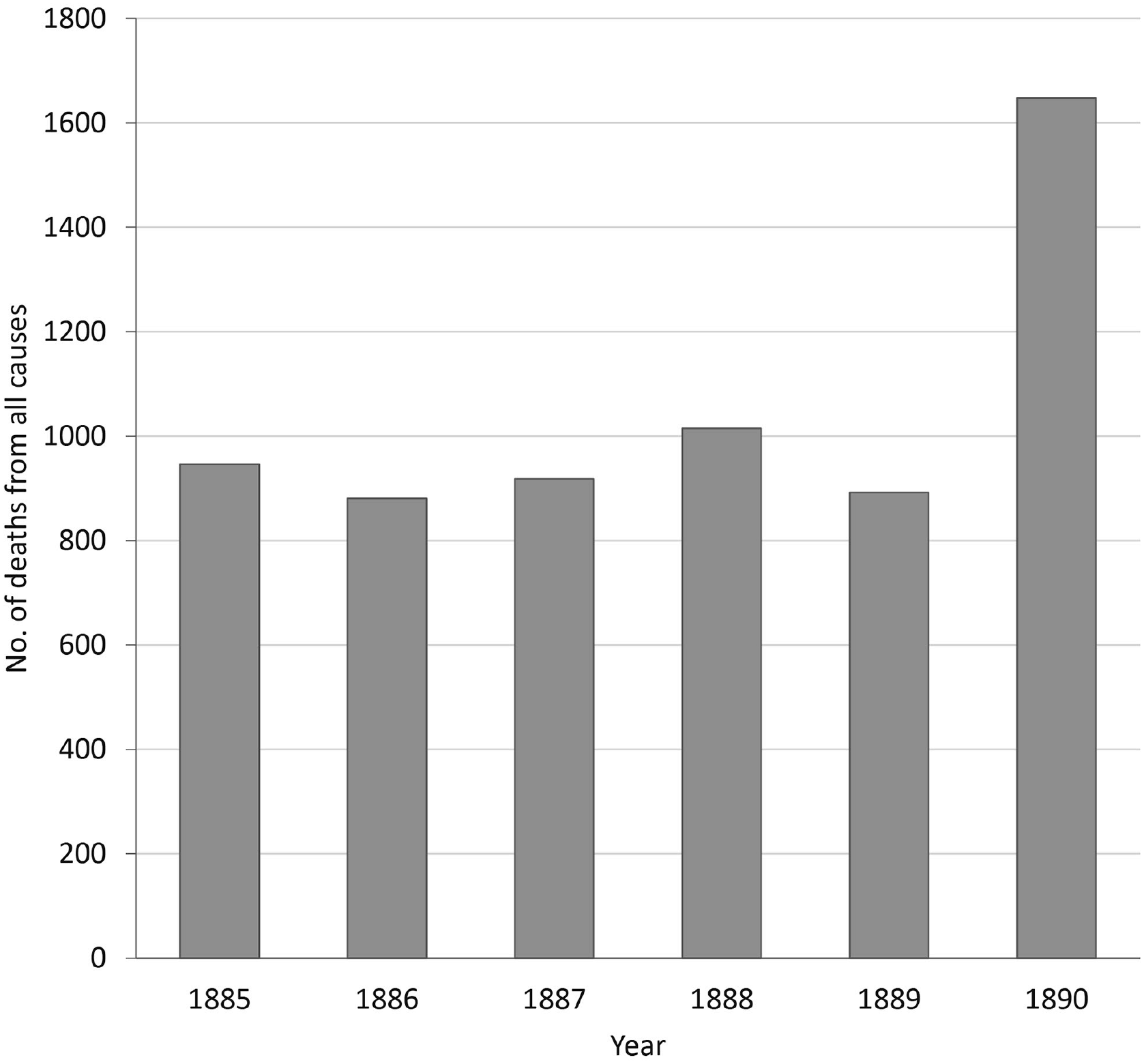
According to the January 1890 Monthly Bulletin from the Connecticut State Board of Health, epidemic influenza “has prevailed in every place in the state from which reports have been received.” 1 Despite the widespread evidence of the disease, Dr C.A. Lindsley, secretary of the Connecticut State Board of Health and superintendent of vital statistics, stated in the same report that influenza was “a mild epidemic; that is, of the whole numbers affected, only a few are seriously sick and the total deaths attributed to it have numbered only 38.” Yet, Lindsley also declared that the so-called “Russian influenza,” which first came to global attention in late 1889 after reports of widespread cases in St Petersburg, Russia, was “the most disastrous and fatal epidemic which has afflicted Connecticut in many years.” The quantitative evidence included the 1648 deaths from all causes recorded in January 1890, an 85% increase from the same month 1 year earlier, and a toll that “exceeded any previous experience in a single month in the history of the state.” 1
This tension between the declaration of a “disastrous and fatal epidemic” and that few (2%) deaths were attributed directly to Russian influenza illustrates the challenges of measuring the effect of any influenza epidemic but particularly in a context in which this disease was not regarded as a serious health danger. According to the Connecticut State Board of Health, 185 deaths from influenza in 1890 accounted for 1.3% of all deaths. 2 By contrast, nearly 8 times as many deaths were recorded for pneumonia (n = 1437). 2 These numbers indicate that Russian influenza had a substantial effect on public health and especially mortality, yet the scope and severity of this effect was complicated by the way diseases and deaths were classified, reported, and interpreted by local and state boards of health.
Purpose
This case study responds to recent calls for more research on historical pandemics, with particular attention to the range of sources that reliably recorded mortality at the individual, local, regional, and national level.3 -6 Scholars researching historical pandemics can learn from contemporary surveillance tools to distinguish between the low number of deaths attributed to influenza and the larger numbers attributed to influenza-associated diseases, particularly pneumonia. 7 By focusing on this question of how many people died from influenza-associated illnesses, this case study contributes to the existing literature on Russian influenza, which has primarily focused on questions of global spread, medical research, journalistic reporting, and public response.8 -13 Only a few studies have attempted a scholarly analysis of epidemiologic questions about mortality.14 -18
This case study examines public health responses to an influenza epidemic during an era when medical knowledge of the disease was limited, contested, and incomplete. Whereas scholars have documented (and debated) the effectiveness of public health measures implemented during the 1918 Spanish influenza pandemic, the absence of any such measures (or even discussion of such measures) during the Russian influenza pandemic prevents a similar analysis of public health responses in 1890.19 -21 Although inspired by research on public health measures implemented during the 1918 Spanish influenza pandemic,22,23 this case study focuses instead on a different but highly valued role for public health in the late 19th century: the documentation of vital statistics. 24 By examining the ways in which boards of health counted influenza-associated deaths, this case study contributes to a growing appreciation of the evolution of US public health.25 -27
Methods
Connecticut provides valuable perspectives for measuring mortality because of its geographic location, the commitment of public health officials at the local and state level to gathering and analyzing vital statistics, and the detailed recording of mortality totals for the 3 years after the 1890 influenza outbreak. Located on the eastern seaboard of the United States, Connecticut was among the first states with widespread outbreaks of disease associated with the Russian influenza pandemic, which meant health officials were measuring and recording the pandemic as it occurred. (Officials in states further south and west knew about the disease before its arrival.) In addition to geographic location, Connecticut was also distinguished by a broad commitment to collecting, preserving, and analyzing vital statistics. In 1878, the Connecticut State Board of Health was established with the “duty” to supervise the “system of registration of births, marriages, and deaths.” 28 The 1890 annual report from the Connecticut State Board of Health declared that vital statistics registration in Connecticut “in many respects is not excelled in any state in the Union at the present time.” 29
Public health officials in Connecticut documented the number of deaths in the annual reports and the Monthly Bulletins published by the Connecticut State Board of Health. In addition, lengthy extracts from the Connecticut State Board of Health reports were reprinted in the weekly Abstract of Sanitary Reports (which later became Public Health Reports).30 -32 Regional newspapers printed the monthly totals and cited evidence from the reports to evaluate the health of the community. The extensive circulation of these records reveals how broadly public health officials across the state attempted to count the number of deaths associated with Russian influenza.
Outcomes
Vital statistics published by the Connecticut State Board of Health demonstrated the notable spike in deaths in early 1890. The 1648 deaths recorded from all causes in January 1890 marked an increase of more than 700 deaths higher than the average of 930 deaths for January in the previous 4 years (Figure 1).2,29,33 -35 The Connecticut State Board of Health annual report acknowledged the change in mortality patterns at the start of the year. Whereas initially influenza “was not regarded as a disease of very formidable character, or one to which was attributed many fatal cases,” the developments during the year demonstrated that “in its consequences, both direct and indirect, it has proved to be one of the most destructive pestilences that has ever afflicted our people.” 29 The “pernicious effects” of the epidemic lasted beyond “the few weeks while it prevailed” in January 1890, because the mortality throughout the winter was higher than in any previous year. 29
From the perspective of physicians, the epidemic was marked by widespread illness, with few deaths directly attributed to influenza but increased mortality overall. In summarizing the physicians’ written responses, Superintendent Lindsley indicated the “most common sentiment” was that “the depressing effect upon the vitality of the patient was the chief factor in the disturbance, and that through this influence all acute diseases were prolonged,” with reference to heart disease and tuberculosis “causing a number of cases to terminate fatally which prior to the attack had been going well.”
29
This report called attention to “unusual mortality from pneumonia” in January 1890 “when the epidemic was at its height.” A summary of the physicians’ written responses by Superintendent Lindsley combined measurable statistics with subjective interpretations: In just what relation the two diseases were associated is not clearly proven, and we cannot perhaps at present do more than record the statements of those who have reported their observations, that in very many cases the pneumonia followed from a few days to a week after the primary attack of influenza, and was of an unusually severe type, the mortality [from pneumonia] for January, 1890, being 396, while for the same month in the preceding nine years it was as follows: 1889, 90; 1888, 133; 1887, 118; 1886, 74; 1885, 88; 1884; 69; 1883, 77; 1882, 92; 1881, 120.
29
By citing these numbers, Lindsley indicated how much the pattern of deaths from pneumonia in the current year diverged from patterns of previous years, patterns that accounted for seasonal variability, even as he remained cautious about reporting the total number of deaths caused by influenza. These numbers also suggest that the diagnosis of pneumonia as a cause of death did not increase substantially in the decade after researchers first identified the Streptococcus pneumoniae bacterium in 1881.37,38
The balance of perceived effects and measurable outcomes could also be seen in reports submitted by local health officials most directly involved in recording the number of decedents. The 1890 annual report published reports from nearly 150 towns throughout Connecticut. 29 Ninety towns, nearly two-thirds of those submitting reports, cited the prevalence of influenza, La Grippe, the “Grippe,” or the grip as an important health concern during the past year (Figure 2). 29 Many reports described the scope and severity of the epidemic: “quite a number of cases” in Monroe, “a few cases” in Avon, and “very numerous” in Putnam. 29 Several reports evaluated the severity of the illness: “some cases were a long time recovering” in Berlin; influenza cases were “very persistent, lasting anywhere from one to two months, confining the patient to bed a portion of the time in some instances” in East Windsor; “in a few cases severe, but with no complications” in Ridgefield; “very extensive, leaving patients in bad condition, with slow recovery” in Chester; and “hardly any escaped” the influenza in East Haddam. 29
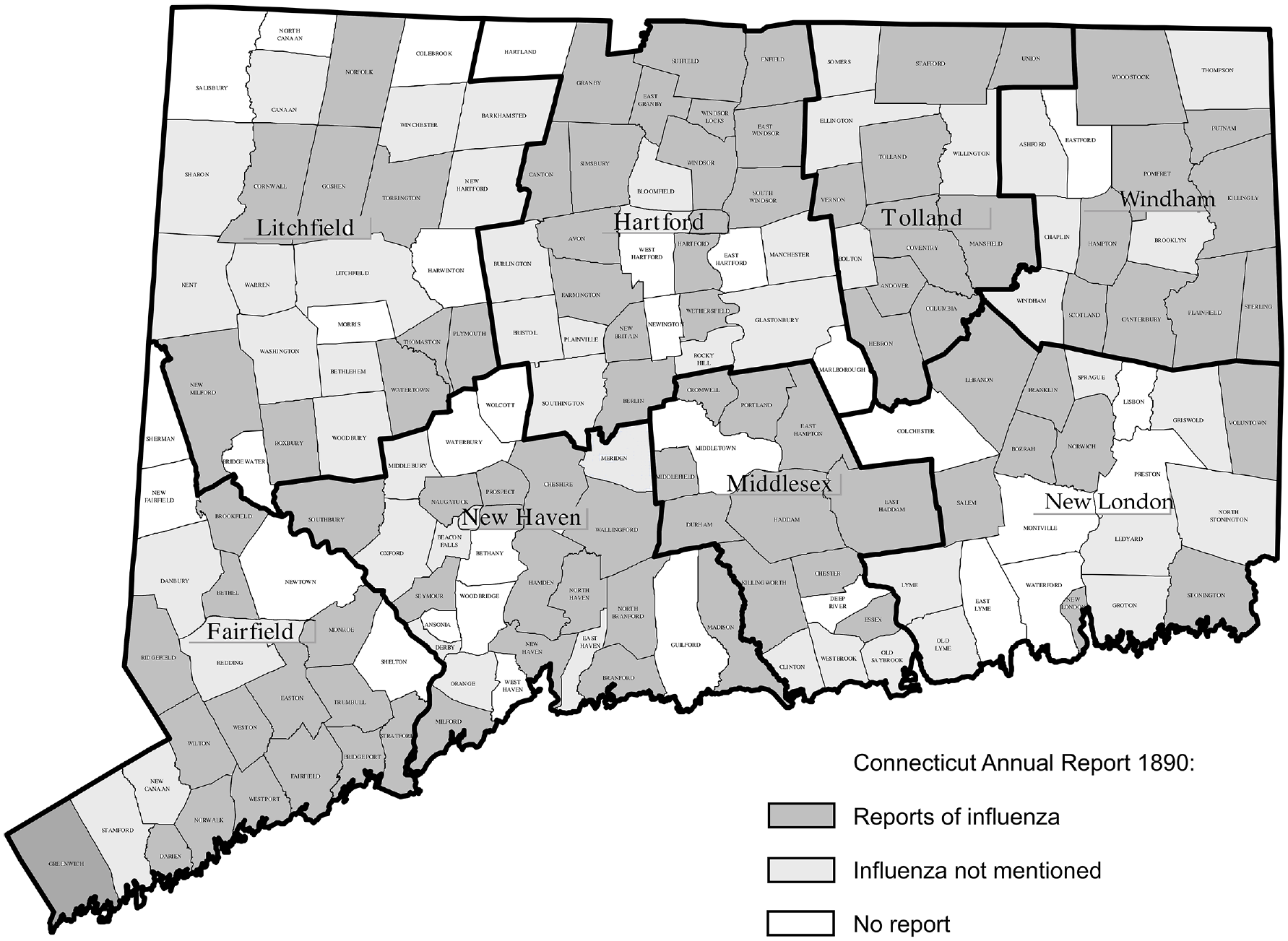
Reports of influenza, by town boards of health, Connecticut, 1890. Data source: Connecticut State Board of Health. 2
Several reports mentioned increased mortality associated with influenza. In New Britain, “fatal cases” usually took “the form of bronchitis, or pneumonia, with a tendency to chronic bronchitis or phthisis.” In Windsor Locks, “some mortality had attended the Grippe.” In North Haven, “La Grippe increased the mortality in all pulmonary diseases; but considering the number of cases treated, the mortality was comparatively light.” 29 In Bozrah, some cases of influenza “were quite severe with a few fatal, especially those running into pneumonia.” In New London, “Nearly half the people in town had the Grip,” but it was “of mild type” with “very light” fatality “except in a few instances from intercurrent diseases.” 29 In contrast, other reports underscored the mildness of the disease by claiming “no deaths” in Bridgeport and Norfolk; “few, if any, fatal cases” in Mansfield; “many severe cases; none fatal” in Farmington; and “whole households in some instances being sick at the same time” yet the disease “rarely proved fatal” in Coventry. 29
The sudden increase in the number of deaths from all causes in January clearly indicates that an unusual disease pattern was taking a toll on the population of Connecticut. Although the local board of health reports consistently described widespread illness, these same reports also suggested that mortality from this disease was perceived as generally low. 29 To return to the tension evident in the January 1890 Monthly Bulletin, Russian influenza was “disastrous and fatal” because it was so widespread that even with a low case fatality rate, the number of deaths increased because of the secondary effect of this disease, as illustrated by the spike in deaths from pneumonia, respiratory diseases, and all causes. 29
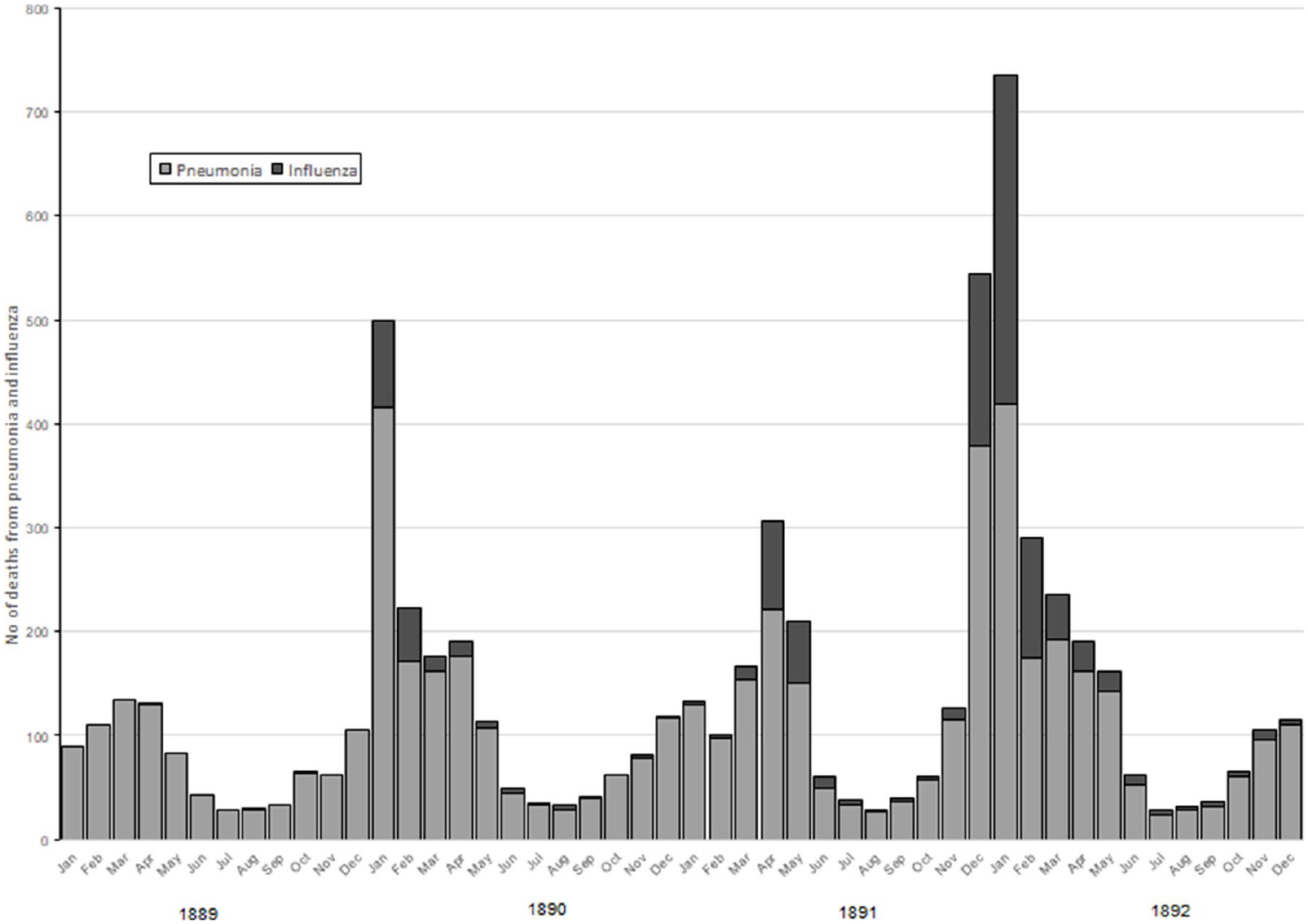
Although the sudden increase in deaths in early 1890 prompted considerable attention from local board of health officials, many more deaths from influenza and associated diseases were recorded in the next 2 years (Figure 3).39,40 The 499 deaths from influenza and pneumonia in January 1890, which prompted concern because the numbers were so much higher than during any month in 1889, were exceeded in December 1891 (544 deaths) and again in January 1892 (735 deaths).39,40 In fact, deaths from influenza recorded by the Connecticut State Board of Health in every year from 1891 to 1895 exceeded the total for 1890, the year of Russian influenza. The uncertainty about classification continued even as the number of deaths ascribed to influenza increased. The Connecticut State Board of Health attributed 376 deaths to influenza from December 1891 through February 1892 yet also conceded that these figures on influenza deaths “very imperfectly measure the work” of an epidemic. 40
A striking characteristic of Russian influenza was the extent to which death patterns by age and sex conformed to normal distributions. During the 3 years of heightened death totals, 1890-1892, the percentage of deaths from influenza, bronchitis, and pneumonia among adults aged 20-60 remained the same as in the year before the epidemic: 35.2% of deaths in 1889 compared with 33.4% of deaths in 1890-1892. The share of deaths among young people aged 1-20 years decreased from 17.4% in 1889 to 12.2% in 1890-1892, with a comparable increase in the share of deaths attributable to these causes among adults aged ≥60: 33.1% of deaths in 1889 versus 41.0% of deaths in 1890-1892.2,29,40,41 That the age distribution of deaths during the Russian influenza epidemic resembled earlier, “normal” years confirms that Russian influenza did not exhibit the remarkable pattern observed during the Spanish influenza pandemic of 1918, when 63% of all influenza-associated deaths were among adults aged 20-60, nearly twice the proportion recorded in 1890-1892. The distribution of deaths by sex during the Russian influenza epidemic also continued the distribution evident before the epidemic: during 1890-1892, females accounted for 49.3% of deaths associated with the epidemic, with higher rates (53.4%)—a proportion only slightly higher than the 48.1% of deaths recorded during the previous year.2,29,39,40
The 1114 deaths from influenza reported by the Connecticut State Board of Health from 1890 to 1892 can support a tentative estimate of epidemic-related deaths at a national level. Given the Connecticut population of 746 258, the annual death rate per 10 000 population for influenza was 2.48 in 1890, 4.90 in 1891, and 7.54 in 1892.2,29,39,40 Applying these death rates to the US population of 62 million suggests approximately 93 000 deaths from influenza during the 3 years that began in January 1890.
Estimating influenza-associated deaths for the United States using this same method is challenging because death rates for respiratory diseases in Connecticut were substantially higher than the national average. 41 Combining the 1114 deaths from influenza and 5931 deaths from respiratory diseases during the 3-year period produces a total of 7045 deaths and a death rate of 26.24 per 10 000 population in 1890, 26.02 in 1891, and 27.22 in 1892. Connecticut recorded the fourth-highest death rate from pneumonia in the 1890 census; as such, using this death rate to project a national total would produce an inflated figure. The death rate for pneumonia in Connecticut was 18.01 per 10 000 population, according to the 1890 census, whereas the death rate for pneumonia in the United States was 12.13 per 10 000 population. 41 Using the ratio that the US death rate was two-thirds of the Connecticut death rate, it is possible to estimate more than 300 000 deaths from influenza and respiratory diseases in the 3 years after the outbreak of Russian influenza in early 1890. This figure is consistent with estimates based on a case study using similar methods for Indiana. 42 This figure must remain tentative, however, until a more complete analysis is available for more states using a similar combination of individual death notices, local health reports, vital statistics compiled at the state level, and national data from the US Census.
Lessons Learned
In fall 1918, as public health officials in Connecticut and across the United States responded to unprecedented mortality because of Spanish influenza, they looked to vital statistics from the Russian influenza epidemic to make sense of the numbers. On October 9, 1918, a Bridgeport newspaper quoted Public Health Service statistics from the 1889 epidemic to predict that the “death rate” from influenza “usually” is “very low,” but also to warn that the new outbreak could produce “an increased number of deaths” due to complications. 43 Ten days later, a widely circulated bulletin from the Public Health Service referenced the history of the 1889 Russian influenza outbreak to warn that influenza cases could lead to complications associated with other diseases, especially pneumonia, and therefore people should take precautions to prevent the further spread of infection: while “the proportion of deaths in the present epidemic has generally been low, in some places the outbreak has been severe and deaths have been numerous.” 44 These predictions based on the historical experience of the Russian influenza epidemic vastly underestimated the mortality associated with the Spanish influenza pandemic, which caused more than 7000 deaths in Connecticut and more than 650 000 deaths nationally from influenza and influenza-associated diseases. 45 Yet when health statisticians attempted to make sense of the devastating effect of the 1918 Spanish influenza pandemic, they also recognized that the death rate had been nearly as high in 1892 as it was in 1918. 46 For public health officials in fall 1918, vital statistics from the Russian influenza epidemic shaped the ways in which they responded to the current epidemic and their efforts to place their immediate experiences in a broader historical context.
For public health scholars in the present and looking to the future, lessons learned from this case study are both obvious and complicated. The sudden implementation of public health measures in response to the coronavirus disease 2019 (COVID-19) pandemic in 2020 reinforces lessons learned from the Russian influenza epidemic: clearly explaining the nature of the infectious disease, finding consistent ways to count victims, and communicating the risks and effects. 47 Given the challenges that continue to face epidemiologists attempting to count influenza-related deaths, 7 this historical perspective demonstrates both the commitment made by state and local health boards to document mortality and the complexities of documenting influenza as a cause of death in the 1890s. Even as they recognized the importance of influenza as a secondary cause of death, Connecticut health officials offered different, and to some extent conflicting, explanations of how influenza deaths were recorded and reported. Similar patterns emerged in early 2020, as differences in how diseases are recorded, the inconsistent reporting on race and ethnicity, and the potential effects of related conditions have complicated both civic understanding of COVID-19 and the public health responses to this critical situation. This case study demonstrates how measuring mortality served as both an important function of public health and a meaningful contribution to understanding epidemics in history. Recognizing that defining and debating categories is part of the historical experience of health officials, physicians, and patients, this case study contributes to the evidentiary basis for understanding the history of US public health.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: National Endowment for the Humanities (grant HG22928315) and Yale Medical Historical Library Ferenc Gyorgyey Research Travel Grant, 2017-2018.