
Abstract
Objective
The hepatitis C virus (HCV) is the most common blood-borne infection in the United States. Although 2% to 3% of the global population is estimated to be infected with HCV, an estimated 18% of the US prison population may be infected. The objective of this study was to establish an epidemiologic profile of HCV infection in the largest urban jail system in the United States.
Methods
We retrospectively analyzed 20 years of data on demographic characteristics, risk factors, and HCV positivity among 80 681 individuals incarcerated at the Los Angeles County Jail who were tested for HCV infection from January 1, 2000, through December 31, 2019. We used multivariate logistic regression analysis to determine predictors of HCV positivity.
Results
Of the 80 681 individuals tested, 27 881 (34.6%) had positive test results for HCV infection. In the multivariate analysis, HCV positivity was most strongly associated with injection drug use (adjusted odds ratio [aOR] = 34.9; 95% CI, 24.6-49.5) and being born during 1946-1955 (aOR = 13.0; 95% CI, 11.9-14.2). Men were more likely than women to have HCV infection (aOR = 1.4; 95% CI, 1.3-1.5), and Hispanic (aOR = 4.2; 95% CI, 3.9-4.4) and non-Hispanic White (aOR = 3.8; 95% CI, 3.5-4.0) individuals were more likely than non-Hispanic African American individuals to have HCV infection. Noninjection drug use, homelessness, and mental health issues were also significantly associated with HCV positivity.
Conclusion
Even in the absence of resources for universal screening for HCV infection, the creation of a risk profile and its implementation into a screening program may be a beneficial first step toward improving HCV surveillance and establishing an accurate estimate of HCV infection in the incarcerated population.
The hepatitis C virus (HCV) is the most common blood-borne infection in the United States. 1 Approximately 75% to 85% of acute HCV infections become chronic infections, which can cause severe, continuous liver damage, leading to outcomes such as liver cancer and liver failure. 2 Hepatitis C infection and its complications impose a large burden on health care use and financial resources. 3,4 An estimated 2% to 3% of the global population is infected with HCV, 5 and the prevalence of HCV infection in the United States was estimated from the 2013 and 2016 National Health and Nutrition Examination Survey (NHANES) to be 1% 6 ; however, NHANES is inherently limited by its exclusion of high-risk populations, such as incarcerated and homeless people. The intersection of socioeconomic and racial/ethnic characteristics with indicators of poor health, likelihood of incarceration, high incarceration rates for drug-related offenses, and high recidivism rates contributes to the disproportionate burden of HCV infection in correctional populations. 7 -10 The estimated seroprevalence of HCV in 2015 among incarcerated individuals in US prisons was 18%. 11 Because of the high prevalence of several HCV risk factors among incarcerated individuals or individuals with a history of incarceration, including the use of injection and intranasal drugs and unregulated tattooing, both the Centers for Disease Control and Prevention and the US Preventive Services Task Force consider incarceration to be a risk factor for HCV infection. 2,12
Jails and prisons are, therefore, high-risk settings that warrant HCV universal opt-out screening programs. However, existing data demonstrate inconsistencies in HCV testing, education, and treatment practices across US correctional systems, and most incarcerated individuals with HCV infection are unaware of it. 13 -15 In addition, guidelines tailored to the jail setting are lacking, and much of the literature on HCV screening in correctional environments largely focuses on prisons, rather than jails. 16 Jails face 2 major health care delivery challenges: a largely transient population and a greater lack of funding and staffing than prisons for the coordination of comprehensive health services, including external care linkage. 17 Whereas the temporary nature of the jail population creates difficulties in establishing care, the lack of funding and staffing introduces competing issues of security and health, resulting in discontinuous care both during incarceration and upon release. Collectively, these factors challenge comprehensive universal HCV screening and treatment programs in jails, often leading to missed opportunities to accurately identify and quantify the true burden of communicable disease to improve surveillance, provide HCV education, and link eligible individuals to potential treatment options. 18 Nevertheless, even a short period of incarceration can present an ideal opportunity to provide some level of HCV screening and education, as it does for screening of HIV and sexually transmitted infections; HCV screening in jails may also have a substantial impact on community health and disease prevention because of the rapid return of individuals into communities. 16,18 -20
The objective of this study was to establish an epidemiologic profile of HCV infection in a large urban jail population by retrospectively examining medical record data during a 20-year period and to identify risk factors most closely associated with HCV infection. Characterizing the strength of association of these risk factors and identifying the key demographic trends during the 20-year period can help in establishing targeted programs for risk factor screening, testing, and education as harm-reduction measures to improve HCV surveillance, even in the absence of resources for universal screening.
Methods
Study Setting and Population
The Los Angeles County Jail (LACJ) is the largest jail system in the United States; it has approximately 115 000 bookings per year and an average daily population of approximately 17 500 individuals. It consists of 6 facilities: Men’s Central Jail, Inmate Reception Center, Twin Towers Correctional Facility, Century Regional Detention Facility, Pitchess Detention Center, and the Correctional Treatment Center (a skilled nursing facility). The Inmate Reception Center serves as the entry and processing point for all incarcerated males. Males are housed in Men’s Central Jail, Twin Towers Correctional Facility, and Pitchess Detention Center, and females are processed and housed at Century Regional Detention Facility. Health care is provided by Correctional Health Services, a dedicated department within the larger Los Angeles County Department of Health Services. The Los Angeles County Public Health, Ambulatory Care Network, and Health Services Administration Institutional Review Board approved this study.
Study Design
This study was a retrospective observational study focused on unique individuals incarcerated at LACJ who were tested for HCV infection from January 1, 2000, through December 31, 2019. We adapted covariates of interest (birth year, race, ethnicity, biological sex, mental health issues, injection drug use, noninjection drug use, HIV coinfection, and homelessness) described by Akiyama et al. 21 Because LACJ has never had an official policy on HCV screening, all testing resulted from the initiation of a health care provider or a patient request during assessment at intake or during any medical visit. To account for incomplete and inconsistent testing and to cast a wide net, we defined HCV positivity broadly as a positive result for an HCV antibody test, detectable HCV RNA, or a detectable HCV genotype. We did not examine reinfection. For individuals tested more than once during the study period, we included only the earliest positive or most recent negative test result. We obtained data on demographic characteristics such as race/ethnicity, sex, year of birth, and booking and release dates, as well as all laboratory results from the electronic health record. We extracted data on all other risk factors, including self-reported mental health issues, substance abuse, injection drug use, and homelessness, from intake questions in the electronic health record that are asked of all individuals upon entry into the Inmate Reception Center. We selected the beginning date of January 1, 2000, to capture the earliest electronically available data on the results of HCV tests, and the end date of December 31, 2019, to mark the end of the 20-year study period. We assessed trends in HCV positivity among individuals by race/ethnicity and age group.
We also examined data from a single day (December 31, 2019) to provide a representative snapshot of HCV positivity at LACJ on that date. We determined the number of individuals who had ever been tested for HCV by that day and examined data on HCV positivity, birth year, sex, race/ethnicity, the facility in which the individual was housed on that day, risk factors, and genotype.
An externally contracted laboratory performed all laboratory tests. Because rapid testing is currently not part of the standard testing algorithm for HIV or HCV at Correctional Health Services, the laboratories used standard assays (ie, a serological test to detect HCV antibodies, HIV enzyme immunoassay/Western blot with reflex before 2014, and HIV fourth-generation antigen/antibody after 2014). Genotype tests and HCV quantitative RNA testing (both separate and as a part of HCV reflex testing) first became accessible at LACJ in 2010 and 2011, respectively, and the results for both were collected beginning in those years.
We assessed the association between HCV positivity and risk factors using multivariate logistic regression analysis. We defined HCV positivity as a binary dependent variable (yes or no). Independent variables were birth year, sex, race/ethnicity, history of recidivism, self-reported drug use, HIV infection, homelessness, and mental health issues. We divided birth years into 6 categories (after 1985, 1976-1985, 1966-1975, 1956-1965, 1946-1955, and before 1946) and used them as indicator variables. We categorized race/ethnicity as non-Hispanic White, non-Hispanic African American, Hispanic, and “all others” (ie, Filipino, Chinese, Japanese, American Indian or Alaska Native, Native Hawaiian or Pacific Islander, and all others). We defined homelessness and mental health issues as ever being homeless (yes or no) and ever having mental health issues (yes or no), and we defined drug use as ever using any illicit substance by any route. We established the following categories for drug use: noninjection drug use, injection drug use, and no drug use. Noninjection drug use and injection drug use were not mutually exclusive. We defined a history of recidivism as having >1 incarceration during the study period.
We used a multivariate logistic regression model to estimate odds ratios (ORs) and 95% CIs for factors associated with HCV positivity. The model incorporated independent variables, with significance defined as P < .05. We adjusted the model for birth years in decades, sex, race/ethnicity, injection and noninjection drug use, history of recidivism, HIV status, homelessness, and mental health issues. We conducted all analyses using SAS version 9.4 (SAS Institute, Inc).
Results
During the 20-year study period, 80 681 unique individuals were tested for HCV infection while incarcerated (Table 1). The greatest proportion was born after 1985 (25.8%), male (75.0%), and Hispanic (41.6%); 68.3% had a history of recidivism; and 82.9% reported no drug use. Only 1.4% of individuals tested reported injection drug use. Among those who had a positive test result for HCV infection (34.6%), the greatest proportion was born during 1956-1965 (34.1%), male (81.7%), and Hispanic (41.5%), and they reported mental health issues (56.2%) and no drug use (56.5%). Of known genotypes, genotype 1A was the most common (7.5%); 88.6% of genotypes were unknown. Before 2011, most individuals with a positive test result for HCV infection were aged ≥35; after 2013, they were largely aged 18-34 (Figure 1). HCV positivity was consistently higher throughout the study period among Hispanic and non-Hispanic White individuals than among non-Hispanic African American individuals, and it was consistently the lowest among individuals in the “all others” racial/ethnic category (Figure 2).
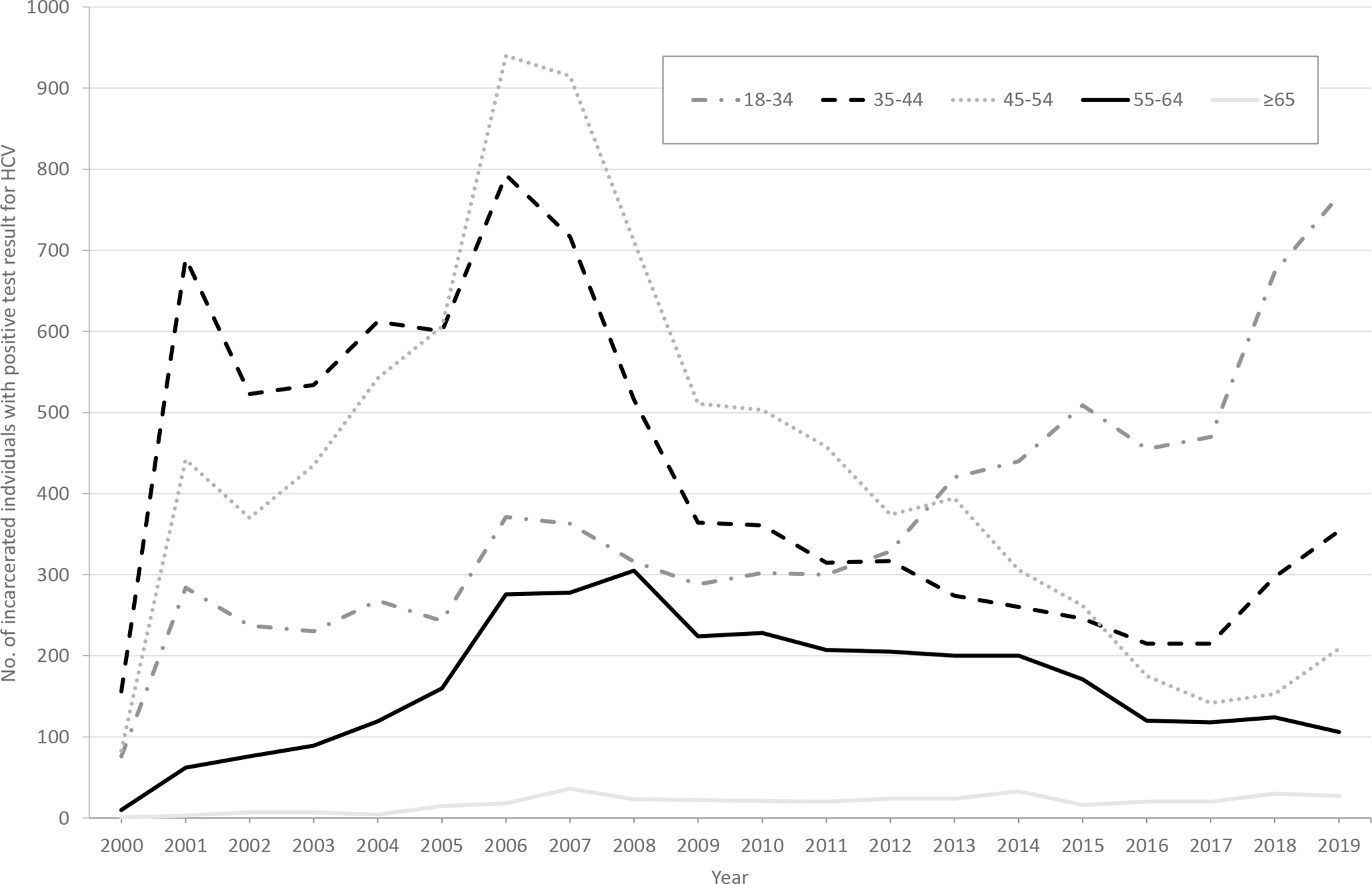
Number of unique individuals who had a positive test result for hepatitis C virus (HCV) infection, by age group, Los Angeles County Jail, January 1, 2000, through December 31, 2019. Positivity was defined as a positive result for an HCV antibody test, detectable HCV RNA, or detectable HCV genotype. Data were collected from the jail’s electronic health records.
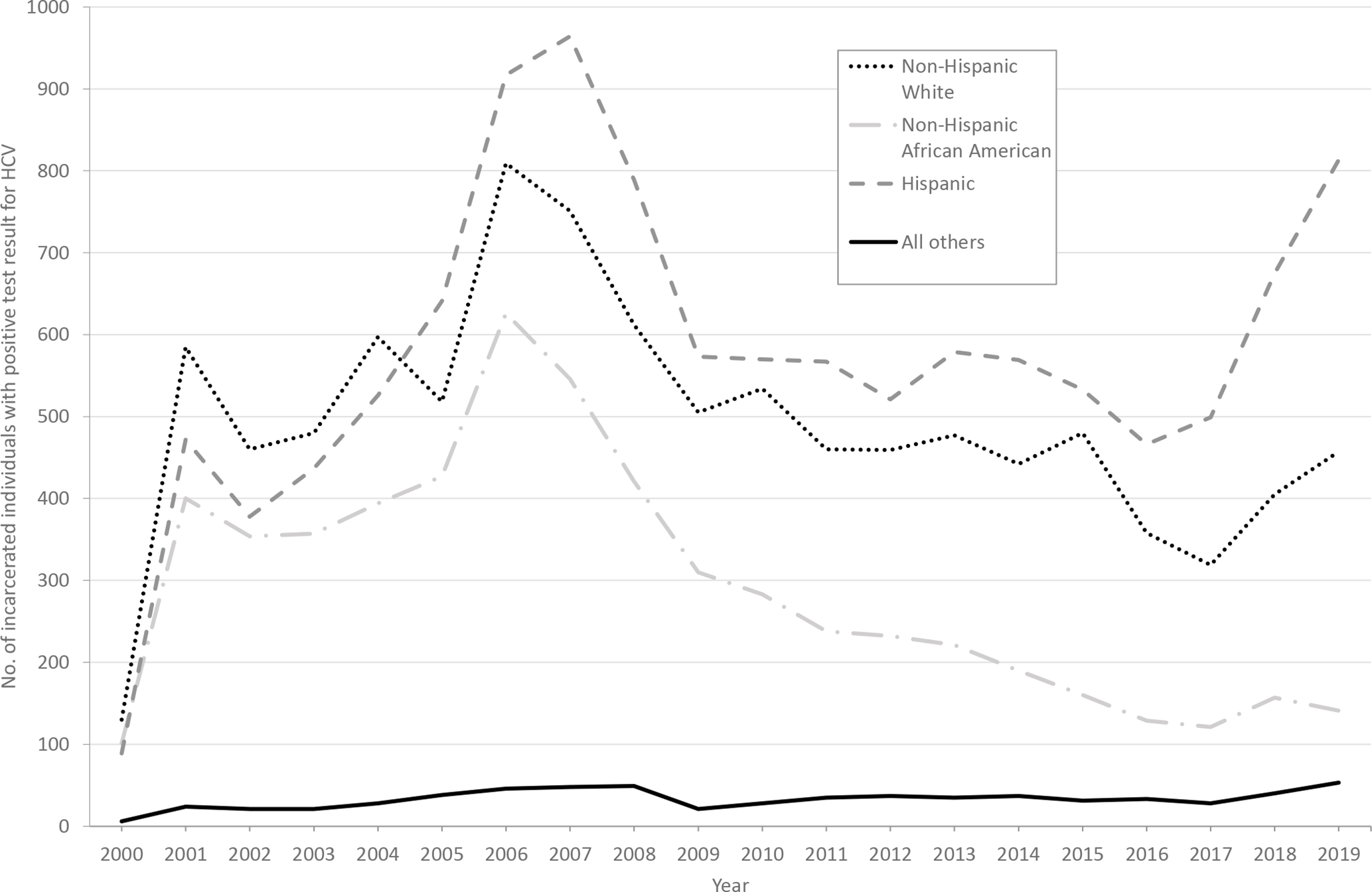
Number of unique individuals who had a positive test result for hepatitis C virus (HCV) infection, by race/ethnicity, Los Angeles County Jail, January 1, 2000, through December 31, 2019. Positivity was defined as a positive result for an HCV antibody test, detectable HCV RNA, or detectable HCV genotype. Data were collected from the jail’s electronic health records. “All others” category includes Filipino, Chinese, Japanese, American Indian or Alaska Native, Native Hawaiian or Pacific Islander, and all others.
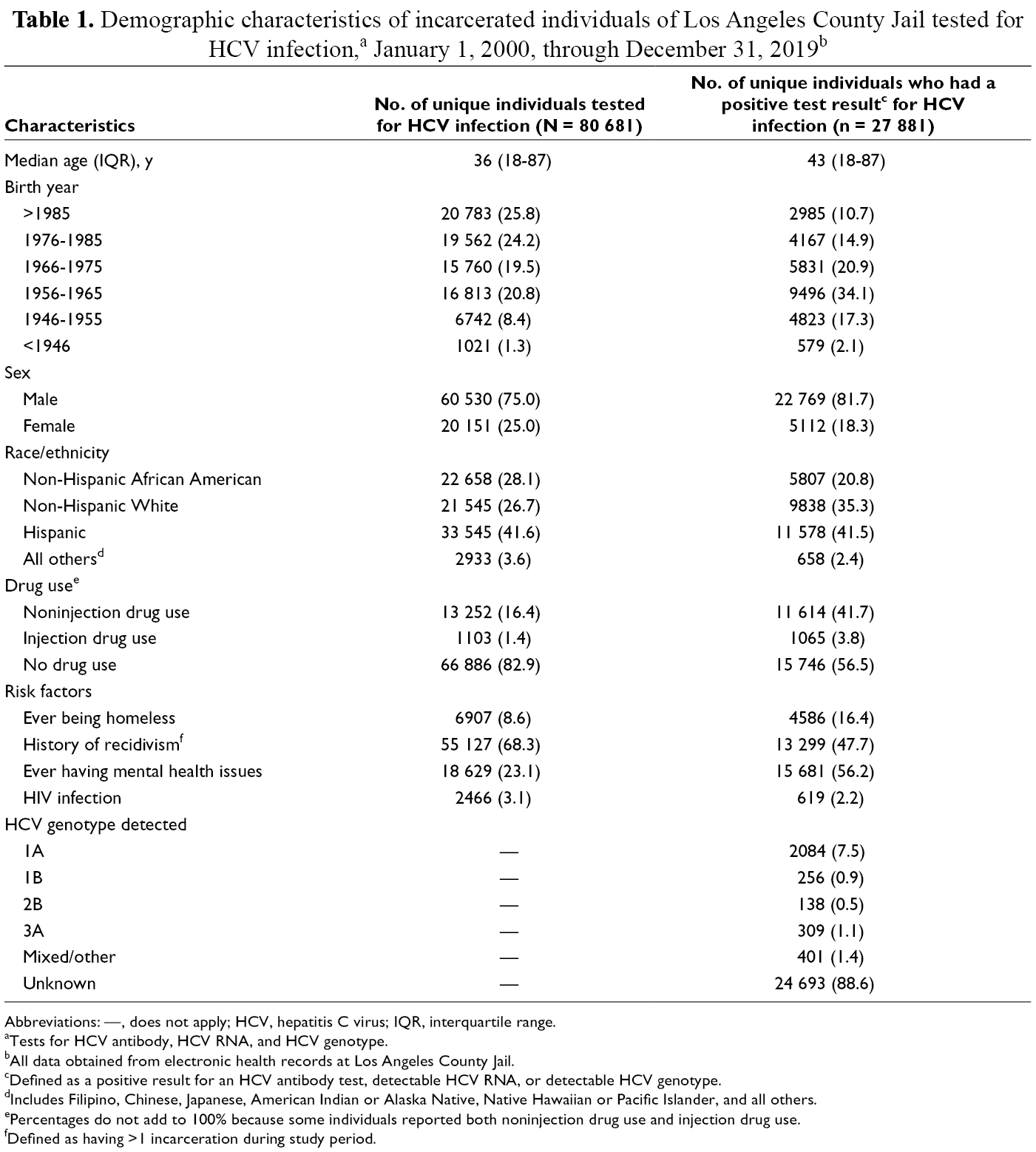
Abbreviations: —, does not apply; HCV, hepatitis C virus; IQR, interquartile range.
aTests for HCV antibody, HCV RNA, and HCV genotype.
bAll data obtained from electronic health records at Los Angeles County Jail.
cDefined as a positive result for an HCV antibody test, detectable HCV RNA, or detectable HCV genotype.
dIncludes Filipino, Chinese, Japanese, American Indian or Alaska Native, Native Hawaiian or Pacific Islander, and all others.
ePercentages do not add to 100% because some individuals reported both noninjection drug use and injection drug use.
fDefined as having >1 incarceration during study period.
The multivariate logistic regression model demonstrated that HCV positivity was significantly associated with being born before 1986 (with increasing ORs as decades became earlier, until before 1946), being male, being any race/ethnicity other than non-Hispanic African American, reporting homelessness, reporting mental health issues, and reporting both noninjection and injection drug use (P < .001) (Table 2).
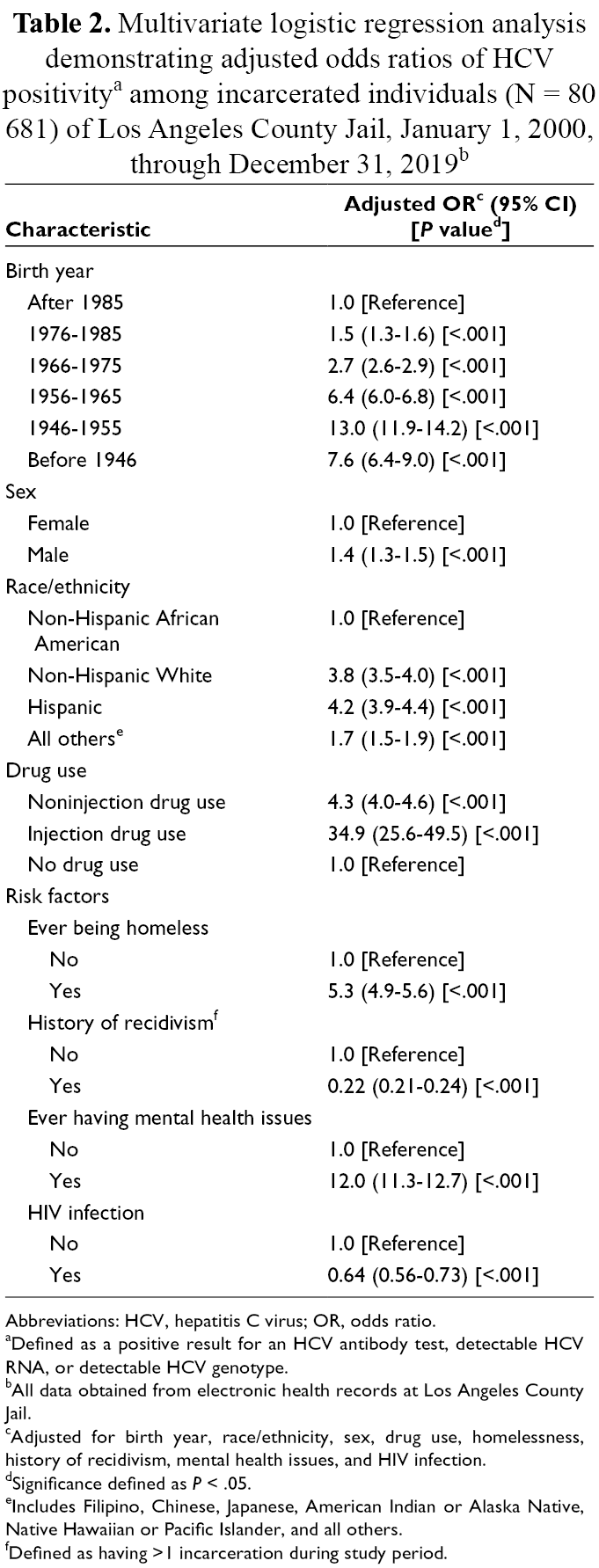
Abbreviations: HCV, hepatitis C virus; OR, odds ratio.
aDefined as a positive result for an HCV antibody test, detectable HCV RNA, or detectable HCV genotype.
bAll data obtained from electronic health records at Los Angeles County Jail.
cAdjusted for birth year, race/ethnicity, sex, drug use, homelessness, history of recidivism, mental health issues, and HIV infection.
dSignificance defined as P < .05.
eIncludes Filipino, Chinese, Japanese, American Indian or Alaska Native, Native Hawaiian or Pacific Islander, and all others.
fDefined as having >1 incarceration during study period.
Single-Day Snapshot of December 31, 2019
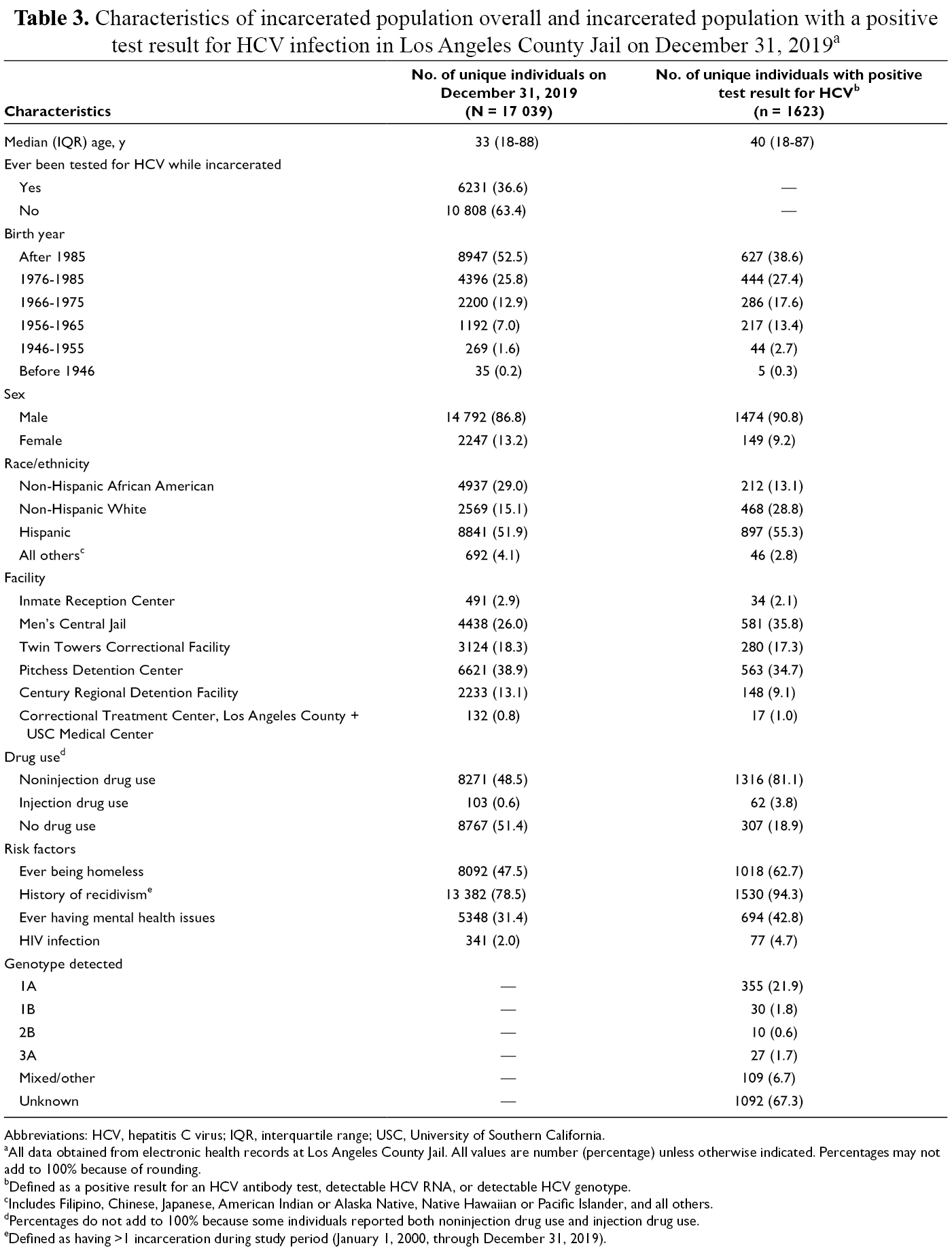
Of the 17 039 individuals who were part of the LACJ population on December 31, 2019, a total of 6231 (36.6%) individuals had ever been tested for HCV infection while incarcerated (Table 3). Among the LACJ population on that day, the greatest proportion was born after 1985 (52.5%), male (86.8%), and Hispanic (51.9%); housed at Pitchess Detention Center (38.9%); reported no injection drug use (51.4%); and had a history of recidivism (78.5%).
Characteristics of incarcerated population overall and incarcerated population with a positive test result for HCV infection in Los Angeles County Jail on December 31, 2019 a
Abbreviations: HCV, hepatitis C virus; IQR, interquartile range; USC, University of Southern California.
aAll data obtained from electronic health records at Los Angeles County Jail. All values are number (percentage) unless otherwise indicated. Percentages may not add to 100% because of rounding.
bDefined as a positive result for an HCV antibody test, detectable HCV RNA, or detectable HCV genotype.
cIncludes Filipino, Chinese, Japanese, American Indian or Alaska Native, Native Hawaiian or Pacific Islander, and all others.
dPercentages do not add to 100% because some individuals reported both noninjection drug use and injection drug use.
eDefined as having >1 incarceration during study period (January 1, 2000, through December 31, 2019).
Among the 1623 individuals with a positive test result for HCV infection (9.5% of the total population), the greatest proportion was born after 1985 (38.6%), male (90.8%), and Hispanic (55.3%); housed in Men’s Central Jail (35.8%); and reported noninjection drug use (81.1%). A small proportion (4.7%) had HIV coinfection. History of recidivism was high (94.3%) in this group, followed by ever being homeless (62.6%) and ever having mental health issues (42.8%). The most common genotype was Genotype 1A (21.9%).
Discussion
This analysis represents the first time that data have been examined and described on the prevalence of HCV infection and its risk factors in the largest jail system in the United States during a 20-year period. Although only 1.4% of individuals tested reported injection drug use, it was found to be the strongest predictor of HCV positivity. Noninjection drug use was significantly but less strongly associated with HCV positivity than injection drug use at the multivariate level. Although stigma may have led to the underreporting of injection drug use, previous studies noted that other noninjection drug routes can lead to HCV transmission, especially among vulnerable populations. 22 Associations between HCV infection and the sharing of noninjection drug paraphernalia such as snorting straws, in addition to having tattoos and body piercings and sharing personal care items, have been described among populations who report noninjection drug use. 23,24 Many individuals in our study reported both noninjection and injection drug use, which may have also contributed to the magnitude of the association of noninjection drug use and HCV positivity. We also observed an age-related increase in HCV positivity, which, as stated in Akiyama et al, 21 could be a function of cumulative risk resulting from increased exposure to injection drug use over time. The distribution of unique positive HCV test results by age for the 20-year study period, however, revealed that since 2013, individuals aged 18-34 have comprised the greatest proportion of positive test results. This observation may reflect a combination of 2 current US epidemiologic trends: a steady increase in HCV incidence primarily driven by injection drug use among young people as part of the opioid epidemic and increased incarceration for drug-related offenses. 25 -27 In addition, the single-day snapshot in 2019 revealed the greatest proportion of known HCV positivity among individuals born after 1985. Although the multivariate regression analysis demonstrated that being part of the 1945-1965 birth cohort (for which targeted screening is recommended) 2 is a strong indicator of HCV positivity, the snapshot data indicate that HCV prevalence in LACJ currently appears to be concentrated in a younger age group.
Mental health issues and homelessness were also found to be strong predictors of HCV positivity. Although the relationship among mental health, homelessness, recidivism, and HIV infection in relation to HCV infection has been well described, the multivariate analysis for our 20-year data set demonstrated that history of recidivism and HIV infection were negatively associated with HCV positivity. 2,28 For history of recidivism, the negative association could be due to the low prevalence of HCV screening during most of the study period. During the 20-year period, an estimated 3 million unique individuals were incarcerated in LACJ, but only 2.7% were ever tested for HCV. In contrast, the descriptive data from the single-day snapshot, in which 36.6% were ever tested for HCV, demonstrated that 94.3% of individuals with HCV positivity had a history of recidivism. The negative association observed in HIV infection could be attributed to the fact that all HIV-positive patients at LACJ, whose care is coordinated by a specialty care team, are offered enrollment into transitional case management programs during incarceration that offer housing and other services in addition to case management upon release. Such programs have been demonstrated to improve clinical outcomes in HIV-positive individuals by providing both medical and social support 29,30 ; although not demonstrated in the literature, these services may play a role in preventing and/or deterring HCV coinfection.
We observed the highest proportion of HCV positivity among Hispanic individuals (41.5%) and non-Hispanic White individuals (35.3%), and Hispanic individuals had the strongest association with HCV positivity in the multivariate regression analysis. This observation contrasts with NHANES findings from 2001-2010, which showed the highest prevalence of HCV infection among non-Hispanic Black people. 31,32 During our 20-year study period, HCV positivity was consistently higher among Hispanic and non-Hispanic White individuals than among non-Hispanic African American individuals, which appears to reflect community trends. In a cross-sectional analysis conducted on homeless parolees who were recruited from a residential drug treatment facility in Southern California, Nyamathi et al 33 noted lower odds of HCV infection among African American participants than among White participants. The authors commented that their findings perhaps reflected unique pockets of HCV-positive people living in urban settings, but 2011-2015 data from Los Angeles County collected by the California Department of Public Health noted that the percentage of newly reported chronic HCV cases was generally higher among White and/or Latino people than among African American people. 34 In addition, an older analysis conducted on people entering the California Correctional System in 1994 noted that the prevalence of HCV antibody positivity was highest among White people, 35 suggesting that the racial/ethnic trends in California observed by Nyamathi et al and in our analysis are perhaps neither an anomaly nor a new occurrence. We also observed a marked increase in HCV positivity among both Hispanic and non-Hispanic White individuals at LACJ from 2017 to 2019, independent of incarceration trends. This increase may reflect a combination of an increase in health care provider–initiated testing and an internally initiated HCV screening pilot that focused on individuals upon entry into LACJ during 2018-2019.
Limitations
This study had several inherent limitations. First, because HCV screening at LACJ has been largely inconsistent (initiated at the discretion of individual health care providers or through patient request rather than through an official policy of universal or targeted screening), providers were more likely to test individuals who reported risk factors; therefore, HCV positivity may be overestimated and concentrated mainly among individuals with reported risk factors, and the true prevalence of HCV infection may have been underestimated among those who did not report risk factors. Second, we could not estimate the prevalence of chronic HCV infection because HCV RNA results were not available for many individuals with positive HCV antibody test results during 2000-2010. Third, most information on risk factors was self-reported; its accuracy and completeness depended on both how agreeable individuals were about providing information at intake and whether the information was entered correctly into the electronic health record. It is not uncommon for individuals at LACJ to refuse intake screening or deny any medical issues to accelerate the jail housing process, and this refusal or denial can lead to incomplete, missing, or inaccurate information. Also, information such as duration of drug use or the presence or absence of tattoos was not easily ascertainable from the intake process and could not be used for our analysis. The intake questions themselves were modified many times during the 20-year study period. Lastly, although we presented data on distributions of unique positive HCV test results for the 20-year study period by age and race/ethnicity, we cannot regard these data as data on HCV incidence, because results that are new to our electronic health record may not be new to the individuals or the local health department. Confirmation of our results as true incident cases would require a detailed review of the medical record for each individual and/or verification with the local health department, neither of which could be done for our study because of the volume of observations.
Conclusion
This study helps characterize various demographic and risk factors of HCV infection and confirms current epidemiologic trends noted in the literature that had not been previously described among the LACJ population, especially the sizeable proportion of HCV infection among the non-Hispanic White population, the strength of association of risk factors such as homelessness and mental health, and the recent shift toward a greater proportion of HCV infections among individuals aged 18-34. This information has particularly important implications for the future direction of HCV screening, education, and care at LACJ. HCV infections, if chronic, can develop into HCV-associated liver disease (eg, cirrhosis, hepatocellular carcinoma, chronic liver disease), which will inevitably lead to an increase in hospitalizations and liver transplants. 36 -38 Given the current challenges at LACJ with securing resources and support for universal opt-out screening, the implementation of a targeted HCV testing and education program, which not only focuses on individuals with reported risk factors but also identifies individuals who have never been tested or are due for a retest, is likely the next essential step to identifying unknown infections and improving HCV surveillance. The implementation of such a program can ultimately guide future interventions for linkage to care and treatment coordination and create justification for the implementation of universal opt-out testing.
Footnotes
Acknowledgments
This work would not have been possible without the pioneering efforts of Mark Malek, MD, MPH, and Garrett Cox, MPH, whose invaluable work shaped the early stages of communicable disease surveillance at the Los Angeles County Jail.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.