
Abstract
Objectives
Sub-Saharan Africa faces a shortage of skilled epidemiologists to prevent, detect, and respond to health threats. Tanzania has implemented one of the first Centers for Disease Control and Prevention Field Epidemiology Training Program (FETP) Intermediate courses in Africa. This course aims to strengthen health workforce capacity in surveillance system assessment, outbreak investigation, and evaluation, prioritizing HIV control. We conducted an outcome evaluation of this new course.
Methods
We used a pre/post evaluation design using data from 4 cohorts of trainees who took the FETP Intermediate course from 2017 to 2020. We conducted knowledge assessments before and after each cohort and combined those results. Outcomes included knowledge and self-rated competency and trends in integrated disease surveillance and response (IDSR) data. We collected data through tests, field assignments, exit interviews, and data audits. We compared the mean change in pre-/posttest scores using linear regression and 95% CIs. We used content analysis to summarize exit interviews.
Results
Fifty-three FETP trainees from 10 regions enrolled in the FETP Intermediate course, and 52 (99.0%) completed the course. We found substantial increases in mean knowledge (44.0 to 68.0 points) and self-rated competency (4.14 to 4.43) scores before and after the course. Trainees evaluated 52 surveillance systems and 52 district HIV care programs, and 39 (75.0%) trainees participated in outbreak investigations. From before to after cohort 1, timeliness and completeness of IDSR reports increased from 4.2% to 52.1% and from 27.4% to 76.5%, respectively. Course strengths were quality of instruction, individualized mentoring, and practical skills gained. Challenges were mentor availability, limited time for data analysis practice, and balancing work and field assignments.
Conclusions
The Tanzania FETP Intermediate course substantially improved trainee knowledge and helped to improve local data quality and reporting. This course is a promising model to strengthen subnational capacity to prevent, detect, and respond to public health threats in Africa.
Sub-Saharan Africa faces a shortage of skilled epidemiologists to prevent, detect, and respond to public health threats and support global health security. 1 -3 Field epidemiologists have unique skills to collect and synthesize data from multiple sources and use data to inform decision making. Few countries have met the World Health Organization target of having at least 1 epidemiologist per 200 000 population to achieve the 2005 International Health Regulations requirements for public health preparedness. 4 Tanzania was the first country in Africa to conduct a Joint External Evaluation of its public health preparedness capacity in 2017, resulting in a 5-year national plan to address these gaps and meet all International Health Regulations targets. 5
Tanzania faces a substantial burden of preventable diseases including HIV, diarrhea, and malaria. 6 As a US President’s Emergency Plan for AIDS Relief priority country, Tanzania has an adult HIV prevalence of 4.9% and an estimated 81 000 new HIV infections among adults each year. 6 Greater field epidemiology capacity is critical to address gaps in HIV data quality and service delivery, to achieve testing and treatment targets.
Since 1980, the Centers for Disease Control and Prevention (CDC), in collaboration with ministries of health, has established Field Epidemiology Training Programs (FETPs) in more than 70 countries to strengthen public health response capacity. 2 This “pyramid” training model has 3 tiers, progressing from basic to advanced epidemiologic concepts. These competency-based field trainings include a 3-month short course (FETP Front-line), a new 6- to 9-month program (FETP Intermediate), and a 2-year field-based training program (FETP Advanced) that confer a master’s-level degree. Each tier targets health professionals at various levels of the public health sector. 7 FETP trainees apply skills to conduct evaluations of integrated disease surveillance and response (IDSR) systems, conduct outbreak investigations, and generate scientific publications. 2 Several African countries, including Tanzania, Kenya, and Nigeria, have established FETP Advanced and/or FETP Front-line programs, 8 -11 in which trainees have contributed to the President’s Emergency Plan for AIDS Relief targets, 12 STOP Polio, 8 and other health initiatives. 13 All FETP tiers cover similar core competencies at increasing depth to build capacity at all levels of a health system. 2 Graduates may advance up the pyramid and mentor trainees at lower tiers.
Despite the success of the Tanzania FETP Advanced course in producing skilled epidemiologists at the national level since launching in 2008, a need exists for skilled epidemiologists at the district and regional levels, to prevent, detect, and respond to disease threats where they originate. 2,14 To fill this gap, the Tanzanian Ministry of Health, Community Development, Gender, Elderly and Children (MoHCDGEC); the University of Washington International Training and Education Center for Health (UW I-TECH); and CDC collaboratively implemented the first standardized FETP Intermediate course in Africa for public health managers at the subnational level. We adapted this course, a Central American FETP curriculum, based on stakeholder input from MoHCDGEC, CDC, and local health officials. The course trained 4 cohorts, approximately 1 cohort per year, in 10 regions from July 2016 through September 2020. 15 Although FETP courses are well described, few have been evaluated. 9,15 -18 We evaluated this new course using data from 2017-2020 to assess improvements in trainees’ epidemiology knowledge, skills, and capacities at their workplaces.
Program
FETP Intermediate Course
The MoHCDGEC provided general oversight; UW I-TECH led course design, implementation, and logistics; and CDC content experts provided input on the curriculum. The 6-month competency-based training uses adult-learning principles that cover surveillance system evaluation, outbreak investigation, data analysis using Epi Info, health communication, and program evaluation (Figure 1). 7 Trainees received hard copies of course materials and could also access soft copies of course materials through their Gmail accounts. Approximately 20% of training time comprised 4 separate 2-week in-class modules combining morning lectures and afternoon group exercises; 80% of the training was field time, during which participants completed 3 worksite-based assignments during their regular work. 19 A team of course trainers and mentors were from Tanzania, all of whom had FETP Advanced training or an equivalent. Trainees received individualized mentorship during class and field assignments. The training was conducted in 4 cohorts of 11-15 trainees each in multiple regions, with each cohort completing the course approximately each year from 2017 through 2019. After cohort 1 completed the course in May 2017, field time was reduced so that the course could be completed in 6 calendar months and be eligible for local accreditation in Tanzania.
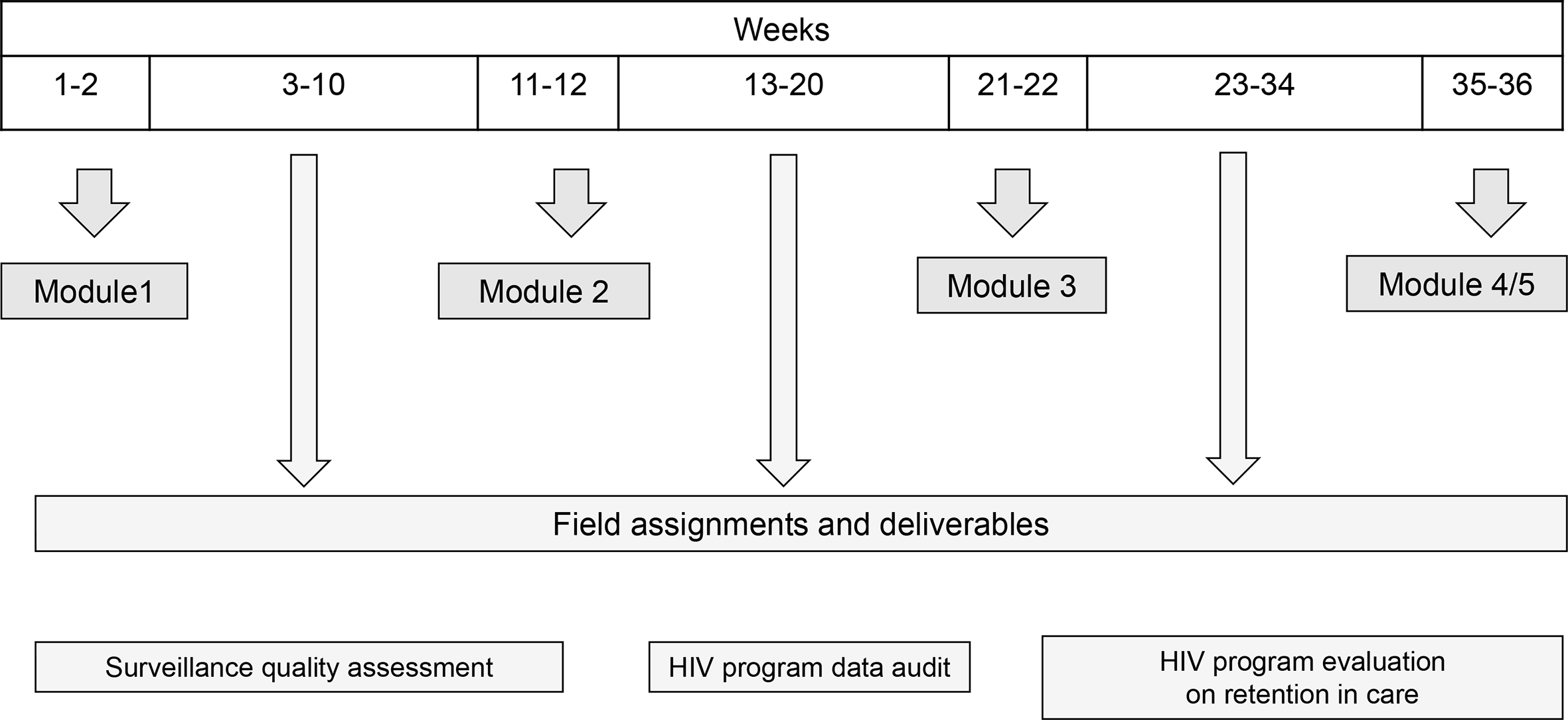
Tanzania Field Epidemiology Training Program Intermediate course structure showing alternating in-class sessions and field assignments, Tanzania, 2016-2020.
Field assignments enable trainees to apply skills learned and address local HIV-related health priorities. In the first assignment, trainees complete an assessment of timeliness, completeness, and accuracy of a district-level HIV surveillance system using IDSR data from the previous 12 months. We defined timeliness as the percentage of cases reported on time, using a random sample of 30 from the previous 12 months. We defined completeness as the percentage of critical variables (eg, age, test date) in the source data and in the surveillance data during a 30-day period. We defined accuracy as the percentage agreement between critical variables in the source and surveillance data in the previous 12 months. 20 In the second field assignment, each trainee conducted a data quality audit of HIV program registers in their districts. For the final field assignment, trainees completed HIV program evaluations using a case-control or cross-sectional study design to identify correlates of retention in care or clinical outcomes among adults aged ≥18 enrolled at district HIV care facilities.
The purpose of this evaluation was to assess the change in trainee knowledge and skills, including descriptive data on organizational impact, using a pre/post evaluation design without a comparison group. Outcome indicators included individual-level change in epidemiology knowledge and self-rated competency by the end of the course and percentage retained in the local health system after graduation. We assessed descriptive evidence of improvement in data reporting in the trainees’ workplaces, using available IDSR data and exit interviews. Process indicators included the number of field assignments completed as planned and qualitative experiences from trainees and staff members.
Methods
Population and Setting
Recruitment occurred in collaboration with the MoHCDGEC 1 month before each cohort during 2016-2019 in 10 regions of Tanzania and Zanzibar. Cohorts 1 through 4 competed the course sequentially in 2017, 2018 (cohorts 2 and 3), and 2019, respectively. Eligible applicants had FETP Front-line training or the equivalent, had at least 1 year of experience in surveillance and outbreak investigation, were employed full-time in a public-sector position at the district level, had computer access, and were fluent in English.
Data Collection
Data collection included trainee knowledge tests and competency surveys administered before and after course completion, individual module pre-/posttests, and program records (eg, completed assignments). The knowledge test included 10 closed-ended and short-answer responses that covered the course learning objectives. The self-rated competency survey asked trainees to rate themselves on a 5-item Likert scale (1 = not competent at all to 5 = very competent) for each learning objective. We conducted individual exit interviews using topic guides with trainees, staff members, and MoHCDGEC stakeholders to assess experiences, course quality, challenges, and recommendations, which informed both process and outcome indicators. We conducted exit interviews with trainees to determine potential improvements in organizational capacity. We reviewed available IDSR reports from 7 districts represented in cohort 1 to assess trends in timeliness (at least 80% of reports submitted on time) and completeness (at least 80% nonmissing data) of submitted reports before (November 2015–July 2016), during (August 2016–May 2017), and after (June 2017–February 2018) the course.
Analysis
We summarized data using means and proportions. We assessed changes in mean total scores on the epidemiology and self-rated competency surveys using linear regression with t tests of significance (P < .05 considered significant) and 95% CIs. We adjusted models for cohort and previous FETP Front-line training. We summarized data on improvements in data quality and reporting at trainees’ worksites and data trends in IDSR reports as proportions. We combined data from the HIV program evaluations to create data sets for each cohort and performed unadjusted regression analyses. We analyzed exit interview data using modified content analysis to identify course strengths, challenges, and recommendations. At the request of MoHCDGEC, we estimated the direct costs in US dollars to conduct a 6-month course for 12 trainees using program expense reports. Costs included travel, meals, and lodging for trainees and Ministry of Health staff members, course materials, and venue, excluding costs associated with UW I-TECH staff members. We entered and analyzed survey data in Epi Info 7 (CDC) and Stata version 14.0 (StataCorp LLC).
This evaluation was approved by the Tanzania National Institute for Medical Research, received a nonresearch determination from the UW Human Subjects Research Committee, and received a program determination from CDC. All participants provided written informed consent.
Results
Trainee Enrollment and Completion
Of 122 applicants, 53 (43.4%) were accepted, 52 (98.0%) of whom completed the course. Trainees represented 10 regions and 37 districts in Tanzania. Most trainees were male (n = 37, 71.2%); 14 (27.0%) were assistant health officers, 9 (17.0%) were environmental health officers, and 9 (17.0%) were nursing officers (Table 1). All trainees attended all sessions and completed all required assignments. By January 2020, 51 of 52 (98.0%) trainees who completed the course were employed at the district level, and 5 (9.6%) joined the FETP Advanced course.
Sociodemographic characteristics of Tanzania Field Epidemiology Training Program (FETP) Intermediate course trainees, by cohort, 2016-2020 (N = 52) a
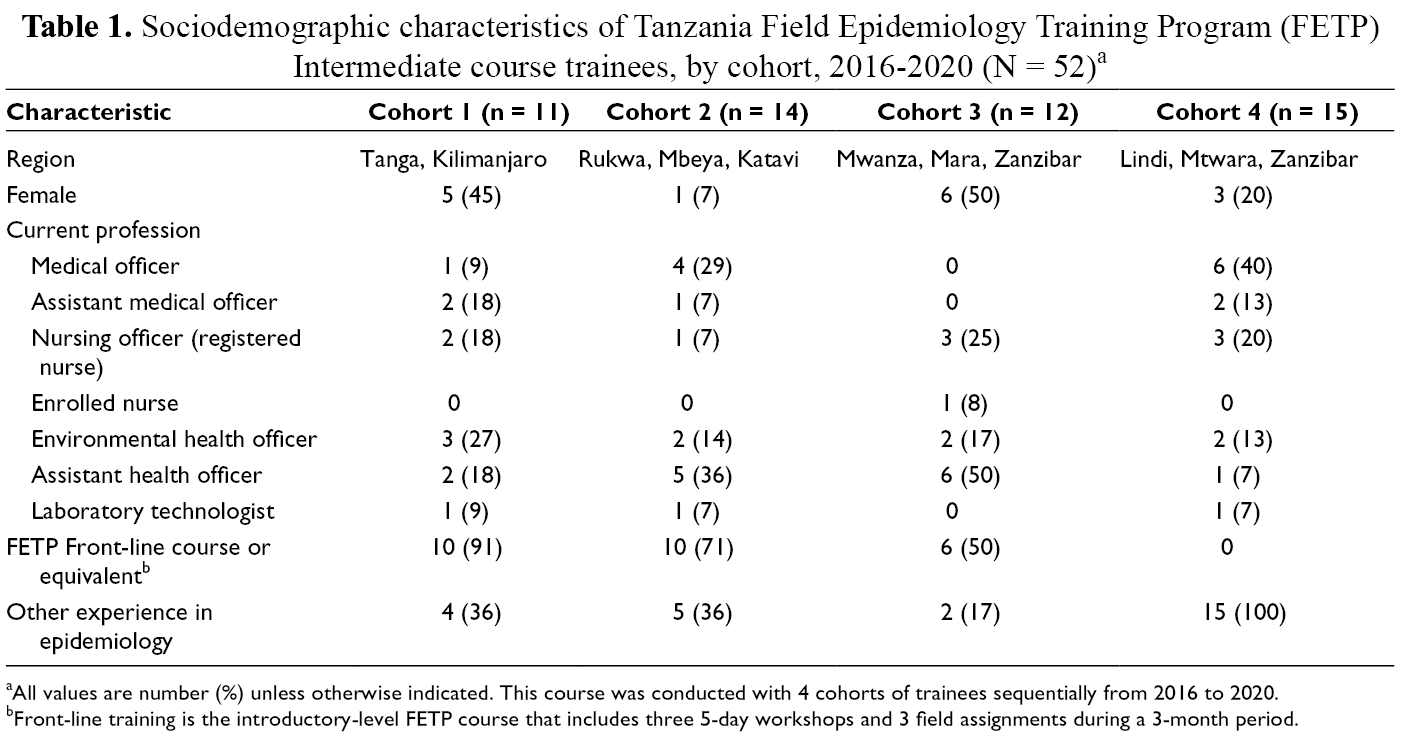
aAll values are number (%) unless otherwise indicated. This course was conducted with 4 cohorts of trainees sequentially from 2016 to 2020.
bFront-line training is the introductory-level FETP course that includes three 5-day workshops and 3 field assignments during a 3-month period.
Change in Knowledge and Self-Reported Competency
We found a significant increase in field epidemiology knowledge scores from before to after course completion (from 44.0% to 68.0%; mean percentage-point change, 24.0% [95% CI, 19.0%-29.0%]) after adjusting for cohort and previous FETP Front-line training (Table 2). Cohort 1 had substantially higher knowledge pretest scores than cohorts 2-4 and higher exposure to FETP Front-line training. However, FETP Front-line training was not associated with pretest scores (β = −0.01; 95% CI, −0.11 to 0.09). Trainees also improved on all individual module pre-/posttests, ranging from 10.0% to 30.0%. We also observed an improvement in self-rated competency scores (from 4.11 to 4.42 on a 5-point scale; 0.29 [95% CI, −0.02 to 0.61]).
Results from trainee pre and post knowledge and skills tests among Tanzania Field Epidemiology Training Program (FETP) Intermediate course trainees, by cohort, Tanzania, 2016-2020 (N = 52)
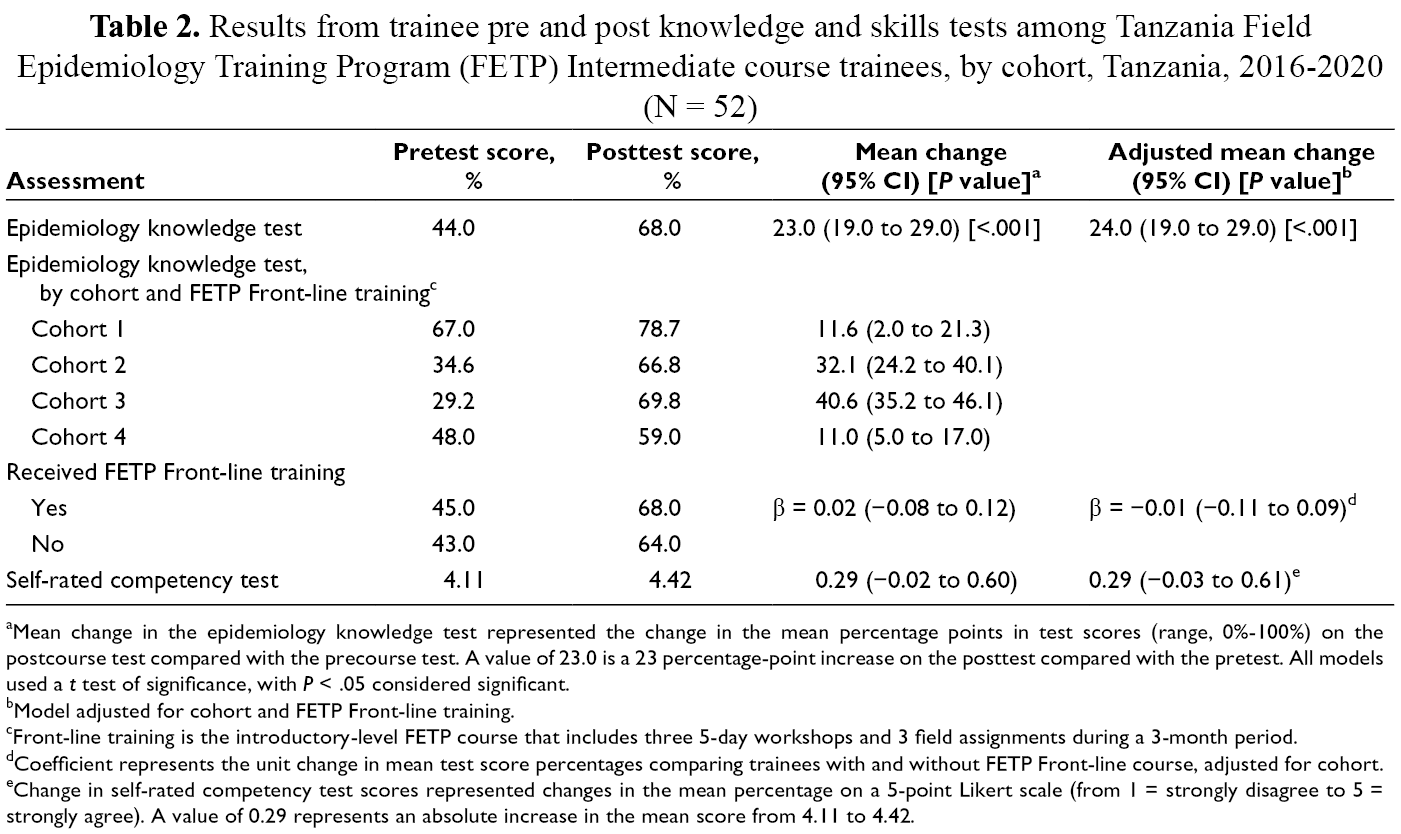
aMean change in the epidemiology knowledge test represented the change in the mean percentage points in test scores (range, 0%-100%) on the postcourse test compared with the precourse test. A value of 23.0 is a 23 percentage-point increase on the posttest compared with the pretest. All models used a t test of significance, with P < .05 considered significant.
bModel adjusted for cohort and FETP Front-line training.
cFront-line training is the introductory-level FETP course that includes three 5-day workshops and 3 field assignments during a 3-month period.
dCoefficient represents the unit change in mean test score percentages comparing trainees with and without FETP Front-line course, adjusted for cohort.
eChange in self-rated competency test scores represented changes in the mean percentage on a 5-point Likert scale (from 1 = strongly disagree to 5 = strongly agree). A value of 0.29 represents an absolute increase in the mean score from 4.11 to 4.42.
Surveillance System Assessment
All 52 trainees completed an assessment of a district-level surveillance system, including Early Infant Diagnosis of HIV and Prevention of Mother to Child Transmission, and generated reports with recommendations. We found substantial variation in the timeliness of surveillance data across districts. The mean percentage timeliness of monthly reports in the previous 12 months across these surveillance systems was 88% (range, 30%-100%). Completeness of critical variables (age, sex, sample dates) audited in a 1-month period was generally good across surveillance systems compared with source data (overall mean, 91%; range, 54%-100%), with differences among districts. Although this field assignment did not include a follow-up evaluation, at the end of the course, most trainees reported overall improvements in quality, timeliness, and completeness of surveillance data reported from their districts.
Case Example
One trainee evaluated the Early Infant Diagnosis of HIV surveillance system at her district hospital, comparing surveillance data with source records and conducting staff interviews. Sixty-one of 67 (91.0%) cases were reported. However, timeliness, measured by turnaround time from sample collection to return of laboratory results to facilities, exceeded targets by 1-14 days. The median turnaround time of results between the zonal laboratory and the facility was 27 days. Staff members reported reasons for poor timeliness including inadequate training in data entry, backlog in sample testing, and difficulty contacting clients. To address these problems, the trainee implemented a data verification procedure before filling out monthly reports, hung a checklist to verify dried blood spot sample shipment each day, and assigned home-based care staff members to encourage mothers to return for their dried blood spot results.
Outbreak Investigations
Overall, 39 (75.0%) trainees participated in real-time outbreak investigations and postoutbreak preparedness. One team working on an outbreak in Kilosa District (Morogoro Region) identified 163 cases of cholera. Through community interviews, sample collection, and use of epidemic curves and basic analyses, trainees identified a local river as the source of infection, implemented control measures, and submitted a report with recommendations to MoHCDGEC. Another team established a surveillance system to monitor infectious disease outbreaks after an earthquake in the Kagera region that destroyed the local latrine system.
HIV Program Evaluation
All 52 trainees completed a field assignment to evaluate the risk factors of poor retention in HIV care or viral suppression among adults at health facilities in their districts using surveys and medical record review. Cohort 1 conducted a case-control study of correlates of lost to follow-up from HIV care (>90 days since last scheduled visit) and found that perceived stigma after disclosure of HIV status and male sex were important risk factors for lost to follow-up. Cohort 2 trainees conducted cross-sectional studies on factors associated with missing clinic appointments and found that younger age (<30 years) and being married (vs single) were associated with a 2-fold greater likelihood of missing clinic appointments in the past 6 months. Trainees from cohorts 3 and 4 collected surveys and abstracted routine viral load data. For example, in cohort 3, using data from 372 clients, the proportion of adults taking antiretroviral therapy at least 6 months who had achieved viral suppression was high (83%). Lower cost of travel (<2000 Tanzanian shillings [~US $1]) to the clinic, less travel time (<1 hour), and female sex were associated with viral suppression. Trainees presented these results to course instructors, CDC, MoHCDEG, and local health management teams.
Exit Interviews
We conducted exit interviews with 52 trainees and 16 course stakeholders. Major strengths of the course included quality of instruction, individualized mentoring, and practical skills gained in data management, analysis, and presentation (Table 3). Most trainees described positive changes at their worksites. Specifically, they felt more competent to perform audits and create summaries of IDSR data, analyze data from surveys and outbreak investigations, and help their colleagues to conduct these activities. Several trainees reported improvements in timeliness and completeness of IDSR reports. Stakeholders remarked that the FETP Intermediate course had created a strong network of skilled epidemiologists that MoHCDEG can recruit for investigating future outbreaks and strengthening data systems.
Key themes and quotes from exit interviews with Tanzania Field Epidemiology Training Program (FETP) Intermediate course graduates, staff, and stakeholders, Tanzania, 2016-2020
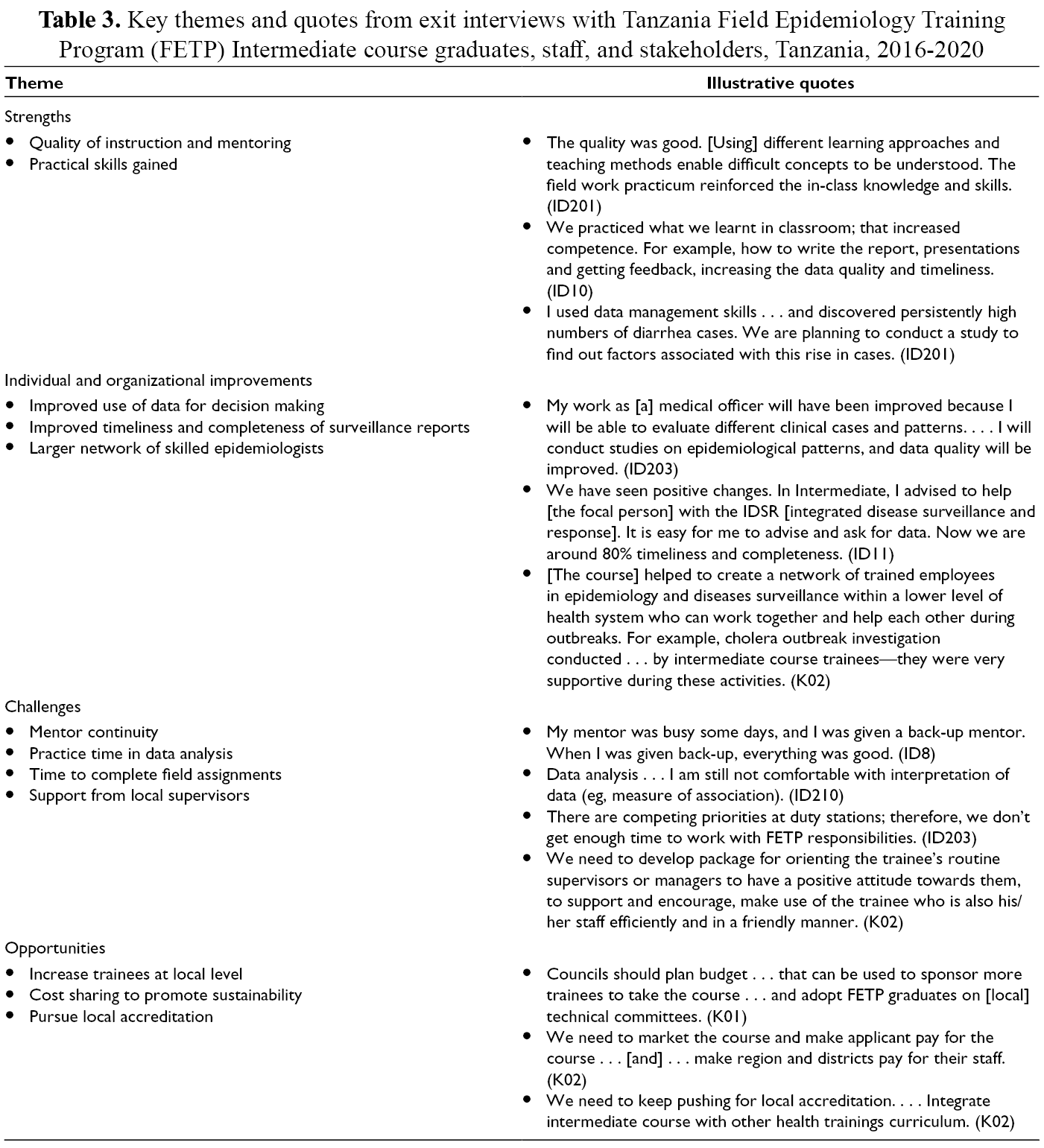
The main challenges identified were gaps in mentorship during field assignments, the need for more practice in data analysis, and difficulty balancing field assignments with work responsibilities. Suggestions for improvement included ensuring mentor availability for site visits, more instruction in data interpretation, and greater engagement of supervisors and district management officers to ensure successful completion of field assignments. All interviewees wanted this course to be expanded and suggested increasing the number of trainees per district and the number of trainees working in HIV control, which we targeted in cohort 4. Ministry stakeholders suggested ways to promote course sustainability, through local accreditation and cost sharing with applicants and districts.
Trends in IDSR Data and Cost
We found an overall increase in timeliness and completeness of IDSR reports at the end of cohort 1 compared with 9 months before the course (Figure 2). Before the course, the average timeliness and completeness in all districts were 4.2% and 27.4%, respectively, which increased to 52.1% and 76.5%, respectively. The estimated direct cost to conduct a 6-month course was $73 499, or $6200 per trainee.
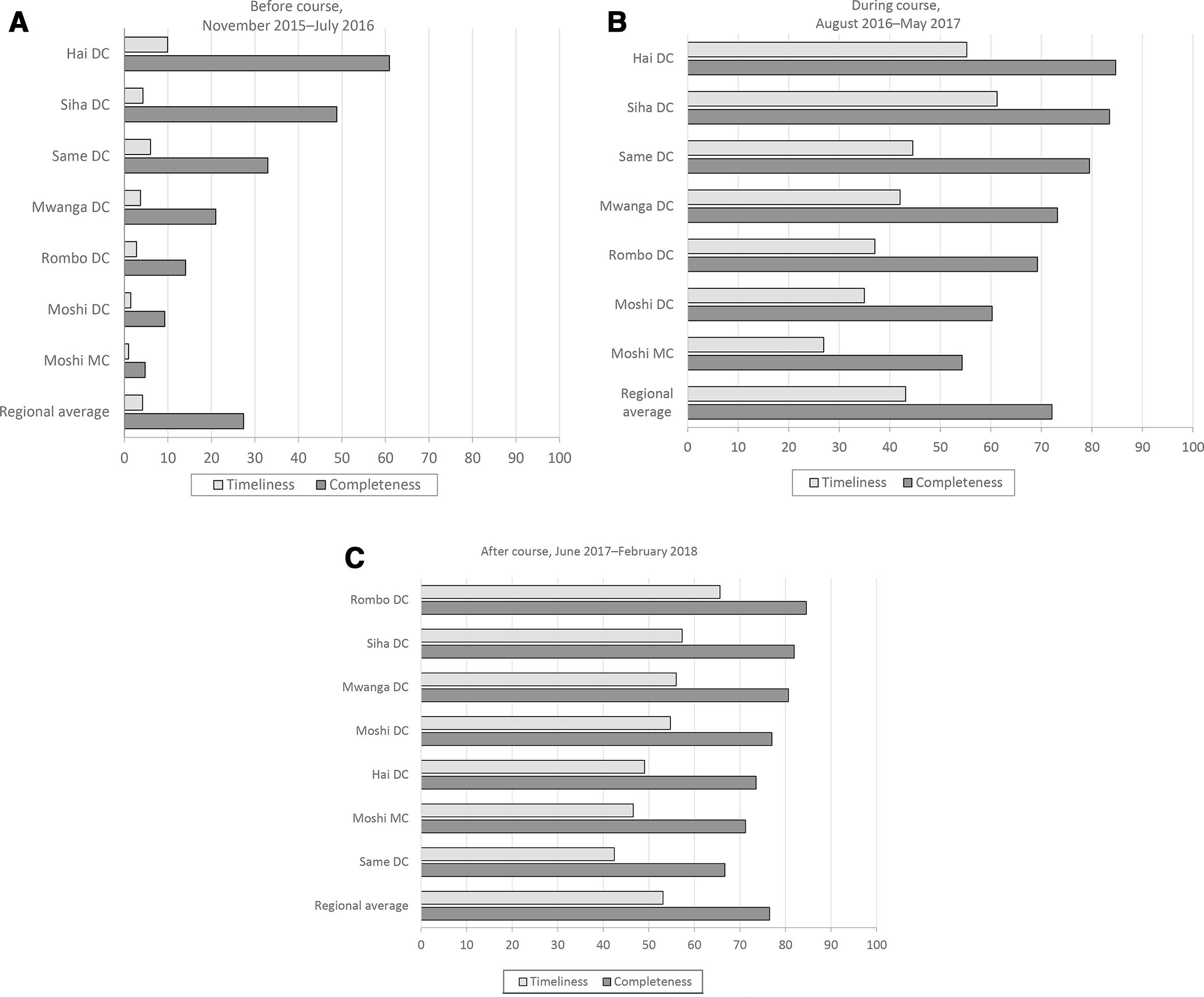
Timeliness and completeness of integrated disease surveillance and response (IDSR) monthly reports, by district, before (
Lessons Learned
The Tanzania FETP Intermediate course significantly improved trainee knowledge and self-rated competency in field epidemiology. Trainees also contributed to strengthening local public health capacity through increased numbers of surveillance systems assessed and HIV programs evaluated and improvements in outbreak investigations and reporting. Timeliness and completeness of IDSR reports increased during and after the course. Through these experiences, trainees filled local gaps in data quality and use of data for decision making while gaining core public health skills.
These findings are consistent with evaluations from FETP Advanced courses, 2,10,17,21,22 which showed that the 2-year training results in a greater number of trained field epidemiologists conducting core public health functions. Few studies assessed changes in individual knowledge and skills, although one evaluation of an FETP Advanced course in South Korea reported significant improvements in trainees’ knowledge and self-rated competency. 17 Our evaluation provides initial evidence that the FETP Intermediate course, which includes standard competencies and targets lower-level health managers, can achieve similar training outcomes. Previous training in FETP Front-line may not be required if trainees have other relevant skills and may enable enrolling trainees with different capacities and management responsibilities in their districts.
Exit interviews revealed how this training may strengthen both individual and organizational capacity. Trainees’ applied field assignments, where they could practice surveillance system evaluations and data audits, likely resulted in improvements in individual work performance. With more skills and confidence in field epidemiology, trainees also supported colleagues to improve data management and reporting. Most trainees played a role in compilation and reporting of local IDSR data. The combination of better individual performance and skill sharing may help to explain observed improvements in data quality and timeliness and completeness of IDSR reports.
A primary challenge of the course was achieving consistent mentoring, especially during field assignments. The lack of consistent monitoring was largely the result of mentors’ overlapping responsibilities with other FETP courses and differences in mentoring skills and styles. Strong mentoring is a core component of the FETP training model 16 and one of the most difficult to implement. 2 We addressed this challenge by strengthening mentor training and recruiting additional mentors from graduates of the FETP Advanced course. Some trainees reported challenges accessing routine data and survey participants for their field assignments because of limited flexibility in their work schedules and travel costs. To resolve these issues, course leadership engaged field supervisors and local health officials to ensure their buy-in and to support trainees’ local transportation costs. Plans for sustainability are under way, including pursuing local accreditation, charging tuition, and creating online content available through the Tanzanian government’s Center for Distance Education.
Strengths of this evaluation included the pre/post comparison, use of multiple data sources, and assessment of individual and program outcomes. One limitation was the potential social desirability bias of self-reported data, which we addressed by including objective knowledge assessments and program data. We could not attribute organizational improvements or IDSR reporting trends directly to trainees. Other factors may explain IDSR trends. However, FETPs should continue to explore ways to use routine data, including IDSR, for evaluations.
This first evaluation of a standardized FETP Intermediate course in Africa provides new evidence that a locally adapted training for mid-level health professionals can improve individual and organizational capacities in field epidemiology. Results will inform new FETP Intermediate courses in Africa and other regions. The FETP Intermediate course is a promising model for strengthening subnational disease prevention and response and improving global health security.
Footnotes
Acknowledgments
The authors acknowledge the Ministry of Health, Community Development, Gender, Elderly and Children for its engagement in design and implementation of this course and Innocent Semali of Muhimbili University of Health and Allied Sciences for his contribution in course oversight. The authors also recognize James Gibson, resident advisor of the Tanzania Field Epidemiology Training Program (FETP), for his active involvement in curriculum review, course implementation, and mentoring. The authors thank the course instructors and mentors, including Rogath Kishimba, Irene Masanja, Nsiande Lema, Ruth Jonathan, Sasita Shabani, Pius Tarimo, and Josephine Kapinga, as well as all trainees, for their active participation and feedback throughout the course. Finally, the authors acknowledge CDC/FETP Atlanta, especially Richard Dicker, Agusto Lopez, and Michele Evering-Watley, for their support with curriculum development and teaching; Oksana Bilukha for her support in securing accreditation; and Jose Aponte for his assistance in adapting training materials for Epi Info 7.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for this evaluation was provided by a cooperative agreement from the President’s Emergency Plan for AIDS Relief (PEPFAR)/CDC NU2GGH001304-03-00 (PI:Kohler).