
Abstract
Objectives
Assessment, Feedback, Incentives, and eXchange (AFIX) is a quality improvement model used to increase childhood and adolescent immunization rates in the United States. We evaluated implementation of a similar quality improvement model to boost adult immunization rates.
Methods
During November 2016 through May 2017, adult immunization outreach specialists conducted 124 in-person visits to clinics in Wisconsin that immunize adults, submit immunization information to the Wisconsin Immunization Registry (WIR), and agreed to participate in adult AFIX. Outreach specialists ran immunization assessment reports using the WIR and showed a paper copy of the report during the visit. Health care providers were encouraged to implement at least 1 of 18 strategies (eg, reminder-and-recall intervention, giving adult immunization resources to patients) to increase adult immunization rates. Outreach specialists conducted follow-up with health care providers at 3, 6, and 9-18 months after the initial visit to encourage strategy implementation. We compared AFIX sites with control clinics on practice type, geographic location, and clinic size.
Results
Clinics that participated in adult AFIX had a significantly larger increase in median adult immunization rates for completion of the human papillomavirus vaccine series at the 9- to 18-month follow-up than control clinics did (10.4% vs 7.7%; P = .02). The median immunization rate for 13-valent pneumococcal conjugate vaccine/23-valent pneumococcal polysaccharide vaccine completed in series was higher, but not significantly so, among adult AFIX clinics than among control clinics (12.6% vs 10.7%; P = .18).
Conclusions
Adult AFIX resulted in increased awareness about adult immunization recommendations and may be a useful tool for increasing adult immunization rates.
Vaccines are effective in preventing or mitigating disease across the life span. 1 Pediatric care providers have incorporated immunization into their daily practice, which, along with school-entry vaccination requirements, has resulted in relatively high childhood immunization rates. 2,3 In comparison, vaccination coverage rates among adults are moderate to low. 4 Among people with vaccination records in the Wisconsin Immunization Registry (WIR), the percentage of adults aged ≥19 who received an influenza vaccination in Wisconsin during the 2019-2020 influenza season was 42.5% (unpublished data, WIR). Furthermore, during 2016, only 30.6% of adults aged ≥60 received a dose of herpes zoster vaccine, and 24.7% of adults aged 19-26 completed the human papillomavirus (HPV) vaccine series. 5 Vaccination rates for tetanus, diphtheria, and acellular pertussis (Tdap) among adults aged 19-64 (62.0%), 23-valent pneumococcal polysaccharide vaccine (PPSV23) among adults aged ≥65 (51.5%), and 13-valent pneumococcal conjugate vaccine (PCV13) among adults aged ≥65 (49.8%) were slightly higher than the zoster and HPV vaccination rates during 2016 5 but still short of the Healthy People 2020 goals. 6
In 2014, the National Vaccine Advisory Committee revised the Standards for Adult Immunization Practice (hereinafter, Standards), which include strategies to improve adult vaccination rates. 7 The 4 key components of the Standards are (1) health care providers assessing which vaccines are needed for adult patients at each visit, (2) giving a strong recommendation for needed adult vaccines, (3) administering needed vaccines or referring the patient to a provider who can administer these vaccines, and (4) entering vaccine doses administered to adults into an immunization information system.
The Centers for Disease Control and Prevention’s (CDC’s) Assessment, Feedback, Incentives, and eXchange (AFIX) program is a quality improvement model used by state and city health departments to increase immunization coverage levels, reduce missed opportunities to vaccinate, and improve immunization practices at the provider level. The AFIX model includes an in-person consultation with health care providers and clinic staff members.
Assessment involves generating immunization coverage reports for a clinic and evaluating immunization practices of health care providers in the clinic.
Feedback provides an opportunity to share the immunization coverage reports, discuss practice procedures and barriers, and collaborate to develop customized, evidence-based quality improvement strategies.
Incentives recognize health care provider accomplishments, which can be a powerful motivator for increasing immunization rates.
eXchange is the periodic follow-up with health care providers to monitor immunization rates while offering support and encouragement to implement the quality improvement strategies selected.
AFIX has been successfully implemented in childhood and adolescent populations 8,9 ; however, to our knowledge, it has not been applied to adult populations. We describe how the Wisconsin Department of Health Services Immunization Program used this model to increase adult immunization rates among clinics that chose to participate in the program in Wisconsin.
Methods
Participants
Adult immunization outreach specialists (hereinafter, outreach specialists) selected prospective clinic sites based on WIR records indicating that vaccine doses were administered to adults. Established in 1999, WIR is a secure, web-based database that contains immunization information on children and adults. Information on doses administered, by a health care provider who uses WIR, is entered into WIR generally through a data exchange between the patient electronic health record and WIR or by manual entry of the information into WIR. During November 2016, outreach specialists sent an email invitation to 700 clinics to participate in adult AFIX. Of these, 124 (17.7%) agreed to participate in the program. AFIX is a quality improvement model routinely used to increase pediatric immunization rates without the need for institutional review board (IRB) review and approval. This same model was recently applied to adult immunization under the auspices of routine public health practice; therefore, we did not pursue IRB review and approval. All clinic immunization coverage rate data shared with clinics during site visits were aggregate.
Control Clinics
For each of the 124 clinics that received a site visit, outreach specialists selected a control clinic, which did not receive a site visit, for comparison. Outreach specialists matched the AFIX and control clinics by practice type, geographic location, and clinic size. Control clinics were clinics that had declined to participate in adult AFIX or did not respond to the invitation to participate. Practice type was determined by a review of the clinic’s web page, or often a clinic name was indicative of the clinic type, which we then confirmed by a review of the clinic’s web page.
Site Visits and Follow-up Visits
During November 2016 through May 2017, outreach specialists from the Wisconsin Department of Health Services conducted initial in-person visits to each adult AFIX site (baseline). Visits were typically 30 minutes to 1 hour long, and the purpose was to review the clinic’s current adult immunization rates, identify a quality improvement strategy that could be implemented, and discuss plans for follow-up.
Outreach specialists conducted follow-up by email at 3 months and 6 months after the initial in-person site visit. We calculated immunization coverage rates for control clinics using the same follow-up period used for the corresponding AFIX clinic. Outreach specialists offered an additional follow-up, by telephone, to all 124 clinics that participated in adult AFIX, which was scheduled for 9-18 months after the initial in-person site visit. Outreach specialists measured adult immunization coverage rates using WIR and reviewed them during each follow-up email or telephone call. The purpose of follow-up was to offer support and encouragement to initiate or to continue to fully implement the quality improvement strategies selected. Outreach specialists also discussed barriers to implementing the strategies selected during follow-up emails or telephone calls.
During November 2016 through May 2017, 124 clinics received an adult AFIX visit. Clinic types visited included 78 general medical practices (internal medicine or family practice), 25 family practices, 7 skilled nursing/rehabilitation facilities, 6 federally qualified health centers, 4 internal medicine clinics, 3 obstetrics–gynecology clinics, and 1 tribal health clinic. Health provider types participating in the visits included 22 physicians, 7 mid-level providers, 359 nurses/medical assistants, 152 clinic managers, 10 quality improvement personnel, and 19 others (eg, public service representatives, vaccine coordinators).
Assessment and Feedback
Outreach specialists assessed clinic-specific immunization rates for the following: Tdap (age 19-100), influenza (age 19-100), HPV series completion (age 19-26), zoster vaccine live (ZVL; age 60-100), and PPSV23/PCV13 completed in series (age 67-100). For each rate, we used as the numerator the number of adults in the clinic who received a vaccine indicated for their age. We used as the denominator the number of adults in the clinic whose age indicated they should receive the vaccine. We provided information to clinics on national immunization goals during the site visit, including Healthy People 2020 goals 6 for influenza (70%), ZVL (30%), and PPSV23/PCV13 immunization (90%), to orient the clinics to these goals. Clinics received an adult immunization toolkit of resources for clinic staff members (eg, Adult Immunization Standards, adult immunization schedules) to assist them with engaging patients on the topic of immunization.
Outreach specialists presented clinics with their adult influenza vaccination rates during the initial in-person site visit, although the vaccination rates were more relevant and timely if measured and shared during peak influenza disease activity (ie, late fall and winter) than during the summer. Because not all clinics received their site visit during peak influenza disease activity, we did not include influenza vaccination rates in our analysis.
Quality Improvement Strategy
Outreach specialists collected and reviewed baseline information on what the clinic was already doing to improve its adult immunization rates during the in-person site visit (during November 2016 through May 2017) to guide the selection of quality improvement strategies for new implementation. 7 In general, outreach specialists encouraged clinics to choose their own strategy. However, if the clinic requested assistance, the outreach specialists made recommendations based on each clinic’s needs or baseline immunization rates. The Centers for Disease Control and Prevention designed strategies for childhood AFIX that were adapted and applied to adult AFIX. These strategies were designed to improve the quality of immunization services, decrease missed opportunities to immunize, and improve completeness and accuracy of immunization information in WIR.
Data Analysis
We calculated the change in immunization coverage rates from baseline (the initial in-person visit) to the 6-month follow-up for each clinic that received an AFIX visit and for control clinics. We then calculated a median difference in immunization coverage rates among sites that received an AFIX visit and among control clinics. We then compared the overall median rate differences (clinics that received an AFIX visit vs control clinics). We used the exact Wilcoxon 2-sample test to determine the significance of differences, with P < .05 considered significant. We conducted all analyses using SAS version 9.4 (SAS Institute Inc).
Results
As of the baseline in-person site visit, all clinics were already implementing ≥1 quality improvement strategy to increase adult immunization coverage rates (Table 1). The most commonly selected strategies for new implementation were reminder-and-recall intervention (to improve the quality of immunization services, 49%), making adult immunization resources available to clinic staff members to address patient questions (to decrease missed opportunities, 70%), and inactivating patients no longer associated with the clinic (to improve completeness and accuracy of immunization information in WIR, 58%).
Strategies to increase demand for adult vaccines implemented among 124 clinics that received an AFIX quality improvement visit during 2016-2018, Wisconsina
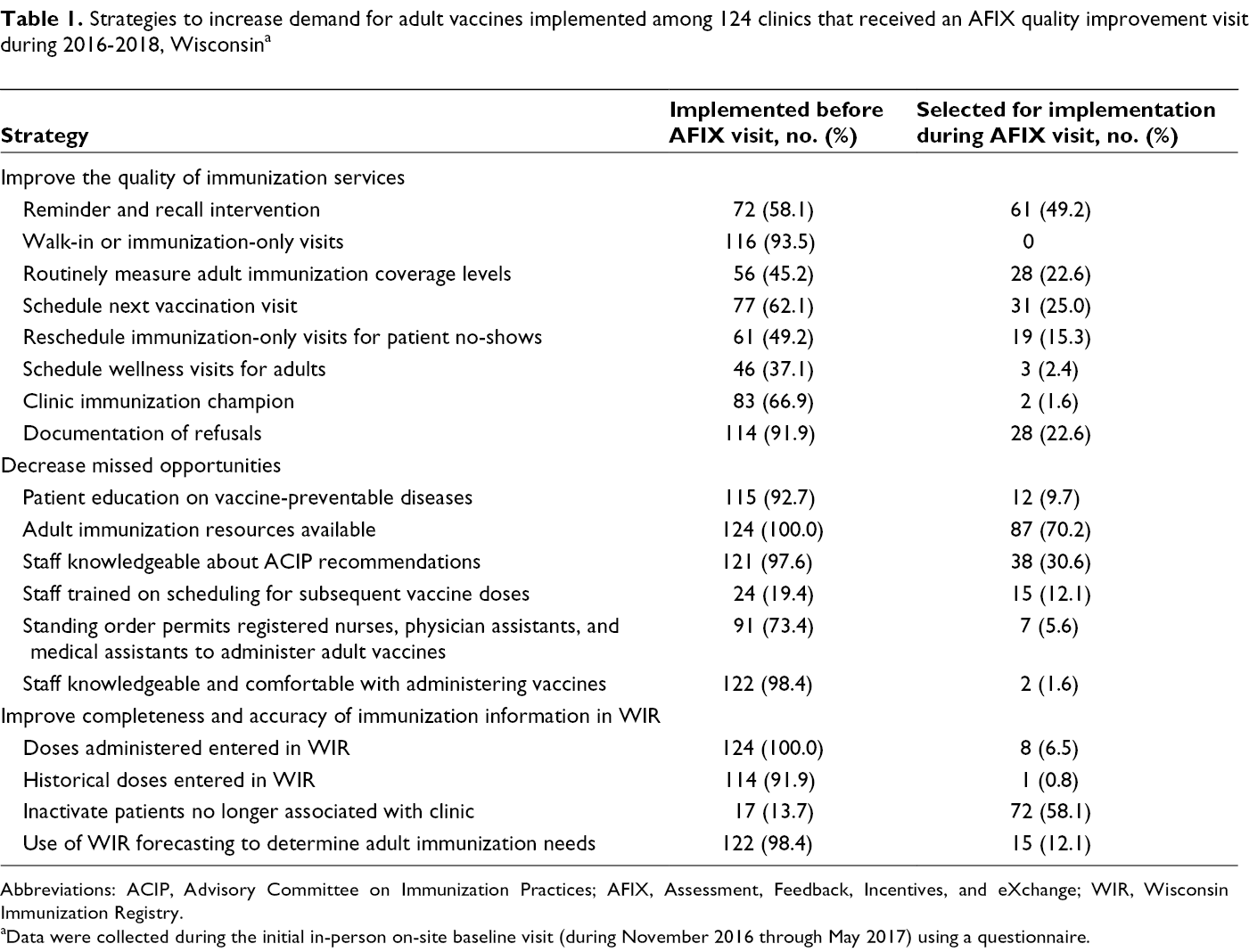
Abbreviations: ACIP, Advisory Committee on Immunization Practices; AFIX, Assessment, Feedback, Incentives, and eXchange; WIR, Wisconsin Immunization Registry.
aData were collected during the initial in-person on-site baseline visit (during November 2016 through May 2017) using a questionnaire.
Barriers discussed during follow-up emails and telephone calls often included the inability to stock all adult vaccines recommended by the Advisory Committee on Immunization Practices because of cost, difficulty with scheduling a subsequent immunization visit to complete a vaccine series, and clinic staff turnover.
All 124 clinics participated in the 6-month follow-up, and 25 clinics participated in the 9- to 18-month follow-up (Table 2). At the 9- to 18-month follow-up, the difference in median HPV series completion rate was significantly higher among clinics that received an AFIX site visit than among control clinics (10.4% vs 7.7%, P = .02; Table 3). Differences in median immunization rates for PCV13/PPSV23 (12.6% vs 10.7%) completed in series were higher among sites that received an adult AFIX visit than among control clinics, but not significantly so.
Adult immunization coverage rates among clinics that did and did not receive an AFIX quality improvement visit during 2016-2018, Wisconsina
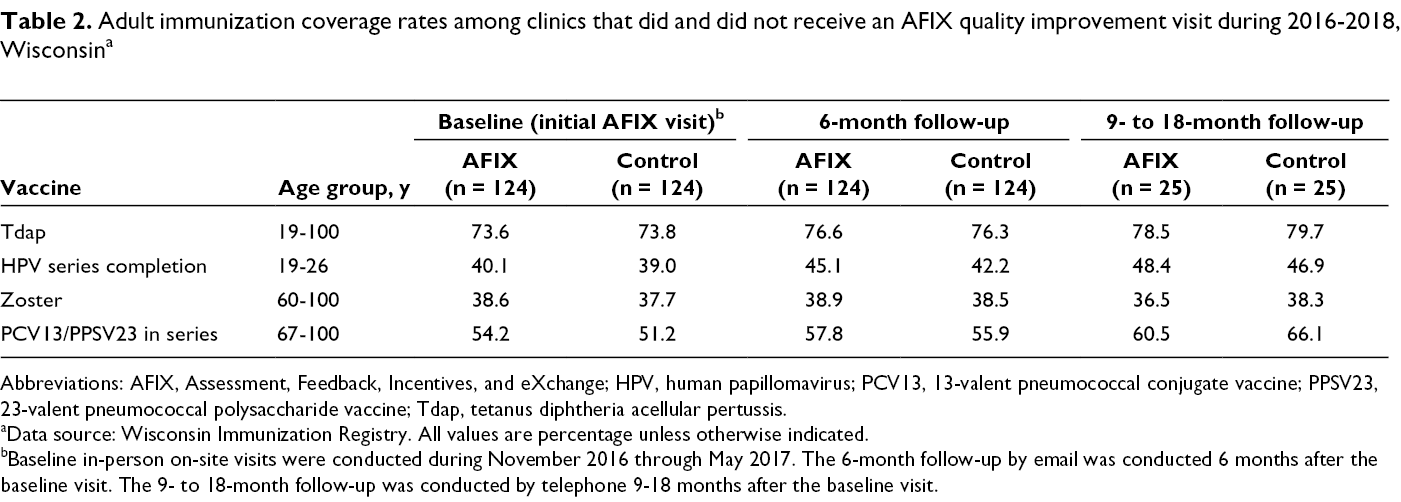
Abbreviations: AFIX, Assessment, Feedback, Incentives, and eXchange; HPV, human papillomavirus; PCV13, 13-valent pneumococcal conjugate vaccine; PPSV23, 23-valent pneumococcal polysaccharide vaccine; Tdap, tetanus diphtheria acellular pertussis.
aData source: Wisconsin Immunization Registry. All values are percentage unless otherwise indicated.
bBaseline in-person on-site visits were conducted during November 2016 through May 2017. The 6-month follow-up by email was conducted 6 months after the baseline visit. The 9- to 18-month follow-up was conducted by telephone 9-18 months after the baseline visit.
Median adult immunization rate differences between clinics that did and did not receive an AFIX quality improvement visit during 2016-2018, 6 and 9-18 months after the AFIX visit, Wisconsina
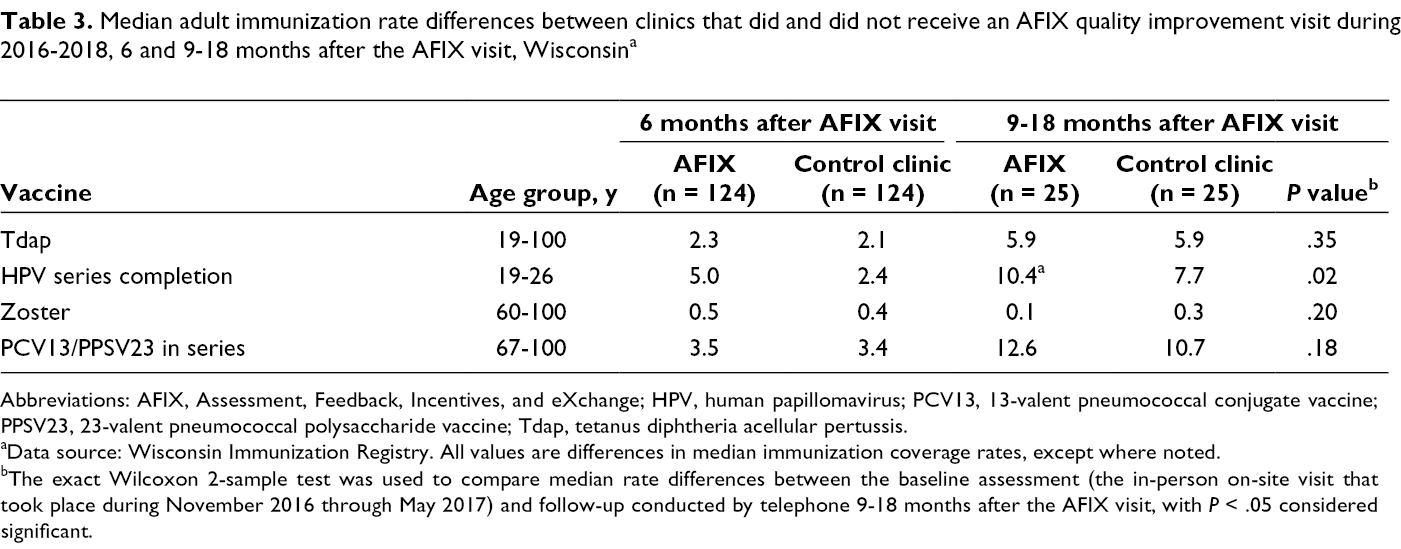
Abbreviations: AFIX, Assessment, Feedback, Incentives, and eXchange; HPV, human papillomavirus; PCV13, 13-valent pneumococcal conjugate vaccine; PPSV23, 23-valent pneumococcal polysaccharide vaccine; Tdap, tetanus diphtheria acellular pertussis.
aData source: Wisconsin Immunization Registry. All values are differences in median immunization coverage rates, except where noted.
bThe exact Wilcoxon 2-sample test was used to compare median rate differences between the baseline assessment (the in-person on-site visit that took place during November 2016 through May 2017) and follow-up conducted by telephone 9-18 months after the AFIX visit, with P < .05 considered significant.
Discussion
AFIX is a quality improvement model that has demonstrated measurable increases in childhood and adolescent immunization rates. 8,9 The logical next step was to apply this quality improvement model to adult immunization. Follow-up at 6 months after the initial AFIX visit is the typical end point for childhood and adolescent AFIX; however, health care providers immunizing adults were at a different starting point than their pediatric care counterparts. Because the adult AFIX program was the first time health care providers had been engaged in adult immunization, we suspected that more than 6 months of strategy implementation would be needed to detect a measurable increase in adult immunization rates. Therefore, immunization rates were measured and an additional follow-up was conducted (for 25 sites), by telephone, at 9-18 months after the initial AFIX visit to provide more time for strategy implementation.
The median rate for HPV series completion was higher among sites that received an adult AFIX visit than among control clinics. Baseline coverage rates for HPV vaccine were low; therefore, we suspect that the potential to increase rates of HPV vaccination was higher than for other vaccines. In addition, during December 2016, the HPV vaccine recommendations changed to a 2-dose series for children and adolescents initiating the series at age 9-14, which likely resulted in HPV vaccine series completion without receiving additional vaccine doses for some adults aged 19-26, as long as they had received their first HPV vaccine dose before age 15. 10
For ZVL, we found no change between sites that received an adult AFIX visit and control clinic sites, although the 9- to 18-month visits coincided with recombinant zoster vaccine (RZV) coming to market, which is preferentially recommended by the Advisory Committee on Immunization Practices. 11 Many clinics elected to wait for an adequate supply of RZV rather than continue to stock and administer ZVL. Outreach specialists calculated RZV coverage rates for the clinic using WIR and provided information about coverage rates during the 9- to 18-month visits. Median rate increases were not significantly higher for Tdap or PCV13/PPSV23 completed in series among sites that received an AFIX visit as compared with control clinics.
Further study is needed to determine the optimal timing between the initial in-person AFIX visit and follow-up visits for adult AFIX to be an effective method of increasing adult immunization rates. One potential step for improving adult AFIX would be to conduct the 3- and 6-month follow-up visits by telephone rather than by email, to offer support with strategy implementation, and to maintain accountability.
Although immunization rate increases were the primary outcome of AFIX, other beneficial but intangible outcomes resulted, including raising awareness about the adult immunization recommendations and teaching clinic staff members how to use WIR to measure immunization rates and to conduct reminder-and-recall intervention.
Limitations
This study had several limitations. First, health care providers invited to receive an AFIX visit were selected among health care providers who see adult patients and were providing vaccines and already providing immunization information to WIR rather than health care providers who care for adults. However, most health care providers who administer vaccines and who care for adults are likely providing immunization information to WIR given that all of the large health systems are doing so. Second, the sample size of clinics that participated in the 9- to 18-month follow-up visit was small because of clinic staff turnover, clinic mergers, and other reasons. Finally, results of this evaluation are not generalizable to all health care providers who see adult patients because not all health care providers report to WIR.
Conclusions
The Standards describe the role of health care providers in protecting adults from vaccine-preventable diseases. 1 Immunization providers are responsible for making a strong vaccine recommendation to their adult patients, and nonimmunization providers have a complementary role to discuss adult vaccine recommendations and refer their patients to an immunization provider for vaccine administration.
The AFIX quality improvement model was originally designed to increase childhood immunization rates, although we have demonstrated its potential among health care providers who immunize adults. Implementing strategies in the clinic setting to increase adult immunization rates may take more time, as we saw with our evaluation; however, the basic principles of AFIX are the same. Additional evaluations are warranted to further refine adult AFIX as a tool for increasing adult immunization rates.
Note
As of July 1, 2019, AFIX was replaced by IQIP (Immunization Quality Improvement for Providers), which is designed to promote and support the implementation of provider-level immunization quality improvement strategies to increase vaccine uptake among children and adolescents. 12 The 3 core strategies are scheduling the next immunization visit before the patient leaves the office, leveraging immunization information system functionality to support immunization, and giving a strong vaccine recommendation. Currently, IQIP is being used only as a tool to increase pediatric immunization rates.
Footnotes
Acknowledgments
The authors acknowledge Amy Parker Fiebelkorn and David Kim, MD, for their thoughtful review of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was funded in part by CDC-RFA-IP15-1502PPHF15. The views expressed do not necessarily reflect the official policies of the US Department of Health and Human Services.