
Abstract
Objectives
Having health insurance is associated with improvements in health care access and use, health behaviors, and outcomes. We examined changes in health insurance coverage for California women before, during, and after pregnancy after implementation of the Affordable Care Act (ACA).
Methods
We used data from the 2011-2017 California Maternal and Infant Health Assessment, an annual representative survey of women sampled from birth certificates (n = 47 487). We examined health insurance coverage at baseline before ACA implementation (2011-2013) and in each survey year from 2014 to 2017 for 3 periods (before, during, and after pregnancy). We calculated prevalence ratios to evaluate changes in health insurance coverage, adjusting for changes in demographic characteristics. Few women were uninsured during pregnancy before implementation of the ACA; therefore, analyses focused on health insurance before pregnancy and postpartum.
Results
Before ACA implementation, 24.4% of women reported being uninsured before pregnancy, which decreased to 10.1% in 2017. About 17% of women reported being uninsured postpartum before ACA implementation, and this percentage decreased to 7.5% in 2017. ACA implementation resulted in a >50% adjusted decline in the likelihood of being uninsured before pregnancy or postpartum, primarily because of substantial increases in Medicaid coverage.
Conclusions
ACA implementation resulted in a dramatic reduction in mothers in California who were uninsured before and after pregnancy. Medicaid expansion played a major role in this improvement.
Health care before, during, and after pregnancy is critical for the health of women and their children.1,2 Women who have a regular source of care before pregnancy are more likely than women who do not have a regular source of care to receive preventive services and have health conditions or behaviors identified that may lead to poor maternal and birth outcomes.3-5 Women who are insured before pregnancy are also more likely than women who are uninsured before pregnancy to have timely prenatal care, 6 which can reduce the risk of prematurity, stillbirth, and infant death. 2 Access to postpartum health coverage may help women manage pregnancy-related conditions, including pain and postpartum depression, which can harm maternal well-being and child development.7,8 Finally, having health insurance is associated with improvements in health care access and use, health behaviors, and outcomes.6,9-14
The purpose of the 2010 Patient Protection and Affordable Care Act (ACA) was to increase the number of people with access to affordable and quality health insurance coverage. 15 Starting in January 2014, states had the option to expand Medicaid eligibility to 138% of the federal poverty guidelines (FPG) for all adults, including parents and childless adults (who were previously ineligible). California took advantage of this opportunity by raising the income cutoff from 100% to 138% for adults with children and from 0% to 138% for childless adults. 16 Most counties in California began this expansion in July 2011 via the Low Income Health Plan, which expanded Medicaid eligibility for adults who would qualify for full Medicaid expansion in 2014. 16 In addition to Medicaid expansion, the ACA provided subsidies to purchase private health insurance to people with incomes between 138% and 400% FPG. The ACA eligibility threshold for pregnancy-only Medicaid in California increased slightly, from 200% to 213% FPG. 17
California’s early expansion program was associated with a slight increase in the percentage of low-income insured adults in the years before expansion, whereas implementation of the ACA more than doubled the number of adults receiving Medicaid from the beginning to the end of 2014.16,18 Among women of reproductive age (15-44) in California, the ACA was associated with a decrease in the percentage uninsured, from 22% in 2013 to 9% in 2018, which was similar to decreases in expansion states nationally. 19 The ACA also resulted in increases in Medicaid coverage before, during, and after pregnancy in expansion states compared with nonexpansion states, as well as reductions in “churn,” or disruptions in health insurance status, during the preconception to postpartum period.20-23
Because of wide differences among states in the percentage of women who were uninsured before, during, and after pregnancy,20,24 additional population-based studies are needed to examine the effect of the ACA on health insurance status around pregnancy at the state level. We examined trends in women’s health insurance status before, during, and after pregnancy from 2011 to 2017 in California, including among women who were more likely to be affected by the ACA, such as women who met the new income cutoff for Medi-Cal (California’s Medicaid program) and women who were childless before the index birth. We hypothesized that ACA implementation would result in declines in the percentage of uninsured women among women who gave birth in California during 2014-2017, particularly before pregnancy and postpartum, and among women more likely to be affected by changes in the law.
Methods
Data Source
This analysis used data from the California Maternal and Infant Health Assessment (MIHA) Survey from 2011 to 2017 (n = 47 487). MIHA is an annual stratified random sample survey of women in California who had a live birth during February through May, sampled from birth certificates. 25 Participants are women aged ≥15 years with a singleton, twin, or triplet birth. The survey is mailed in English or Spanish, with telephone follow-up of nonrespondents; a web option was added in 2017. Survey responses are linked to birth certificate data and weighted to represent all women in California with a live birth during each survey year. Response rates during 2011-2017 ranged from 64% to 70%; women could respond from 2 to 10 months postpartum; most women replied by 7 months postpartum. The MIHA study is conducted according to prevailing ethical principles and reviewed by 2 institutional review boards: the California Department of Health and Human Services and the University of California, San Francisco.
Health Insurance Status
Women reported their type of health insurance coverage and plan name at 3 time points: during the month before pregnancy, during pregnancy, and when they completed the survey after pregnancy. The questions were similar during the 7-year study period; starting in 2014, the private-purchased health insurance option added health insurance obtained through Covered California (the state’s health insurance exchange) or another health insurance marketplace.
Health insurance coverage was recoded into 5 mutually exclusive categories, hierarchically coded as:
Medi-Cal: includes Medi-Cal, a health plan paid for by Medi-Cal, emergency or pregnancy-only Medi-Cal, and both Medi-Cal and private health insurance
Private-purchased: coverage bought directly from a health insurance company or Covered California
Private-employer sponsored: coverage obtained through work (her employer, her partner’s employer, or a parent’s employer) and private health insurance with no indication of either purchased or employer-based health insurance
Other: another type of health insurance coverage, including military or county-based plans for low-income women
Uninsured: no health insurance coverage
Women who have pregnancy-related Medi-Cal can remain on Medi-Cal for approximately 60 days after delivery but may not qualify for Medi-Cal after that. We excluded from the analysis of postpartum health insurance 9 women who reported having Medi-Cal during pregnancy and responded during the postpartum grace period because we did not know if they would have continued to qualify. The following sample sizes were available: before pregnancy (n = 47 237), during pregnancy (n = 47 285), and after pregnancy (n = 47 060).
Covariates
Maternal characteristics used to adjust for sociodemographic and economic changes during the 7-year study period included maternal age (15-26, 27-34, ≥35; we used age 26 as a cutpoint because young adults could be on their parents’ health insurance until then); race/ethnicity/nativity (non-Latinx Asian/Pacific Islander, non-Latinx Black, non–US-born Latinx, US-born Latinx, non-Latinx White, or other); language spoken at home (English, Spanish, other); income as a percentage of the FPG (≤100%, 101%-138%, 139%-250%, >250%); education (<high school, high school graduate or general educational development, some college, ≥college graduate); marital status (married; living with a partner; or single, separated, widowed, or divorced); and number of live births (1, ≥2).
Women were asked to report their total family income before taxes during the calendar year before the birth. We used their self-reported family income and family size to assign each woman a percentage of the FPG. Family size was adjusted depending on the health insurance period; following Medi-Cal guidelines, for pregnancy and postpartum family income calculation, family size included the fetus/infant.
Statistical Analysis
To examine the effect of ACA implementation on women’s health insurance coverage over time, we created a 5-category variable for year, including a baseline category for the time before the law was fully implemented in California (2011-2013 [reference]) and categories for each year after the law went into full effect (2014, 2015, 2016, and 2017). Because health insurance coverage did not change significantly from 2011 to 2013, we combined the years. We first compared the characteristics of women during 2011-2013 with 2017 and calculated t tests to assess changes in maternal characteristics between baseline and 2017. We then examined the unadjusted prevalence of health insurance coverage during the study years for each of the 3 perinatal time points.
Based on MIHA’s design, all sampled women gave birth in the spring of the survey year; therefore, health insurance status in the month before pregnancy refers to health insurance coverage during the calendar year before the survey and the birth. Postpartum health insurance refers to coverage during the survey year after she gave birth, and prenatal health insurance coverage spans the years both before and during the survey. Thus, we expected to observe the effects of ACA implementation on prenatal and postpartum coverage starting in the 2014 survey and on pre-pregnancy coverage starting with MIHA 2015, because this was the first survey year in which pre-pregnancy health insurance referred to a period after ACA implementation.
To calculate the change in health insurance coverage associated with ACA implementation, we obtained adjusted prevalence ratios from the predicted marginals of logistic regression models. We ran 3 multilog regression models, 1 for each perinatal time point (before pregnancy, during pregnancy, and postpartum). The independent variable for each model was the 5-category year variable (2011-2013, 2014, 2015, 2016, or 2017), and the outcome for each model was the 5-category health insurance variable. All models excluded women with missing information on any of the covariates (complete case analysis).
Women born outside the United States may not be eligible for ACA coverage. Women with incomes from 101% to 138% FPG and women giving birth for the first time were likely previously ineligible for Medi-Cal; as such, they might be more likely to be affected by implementation of the ACA than women in other categories. To examine possible population differences in access and ability to enroll for health insurance through the ACA, we tested whether the association between year and health insurance differed by race/ethnicity/nativity, family income, and number of live births. We tested interactions between characteristics and ACA implementation periods using cross-product terms. We conducted all analyses by using SAS version 9.4 (SAS Institute Inc) and SAS-callable SUDAAN version 11.0.1 (Research Triangle Institute).
Results
From 2011-2013 (baseline) to 2017, the population of women giving birth in California shifted slightly toward an older, higher-income, more educated group (Table 1). Non–US-born Latinx women composed a smaller percentage of women giving birth in California in 2017 (19.5%) than at baseline (23.8%), and non-Latinx Asian/Pacific Islander women composed a larger percentage of women giving birth in 2017 (16.6%) than at baseline (14.3%).
Characteristics of women who gave birth in California from 2011-2013 (baseline) to 2017, Maternal and Infant Health Assessment (MIHA) Survey a
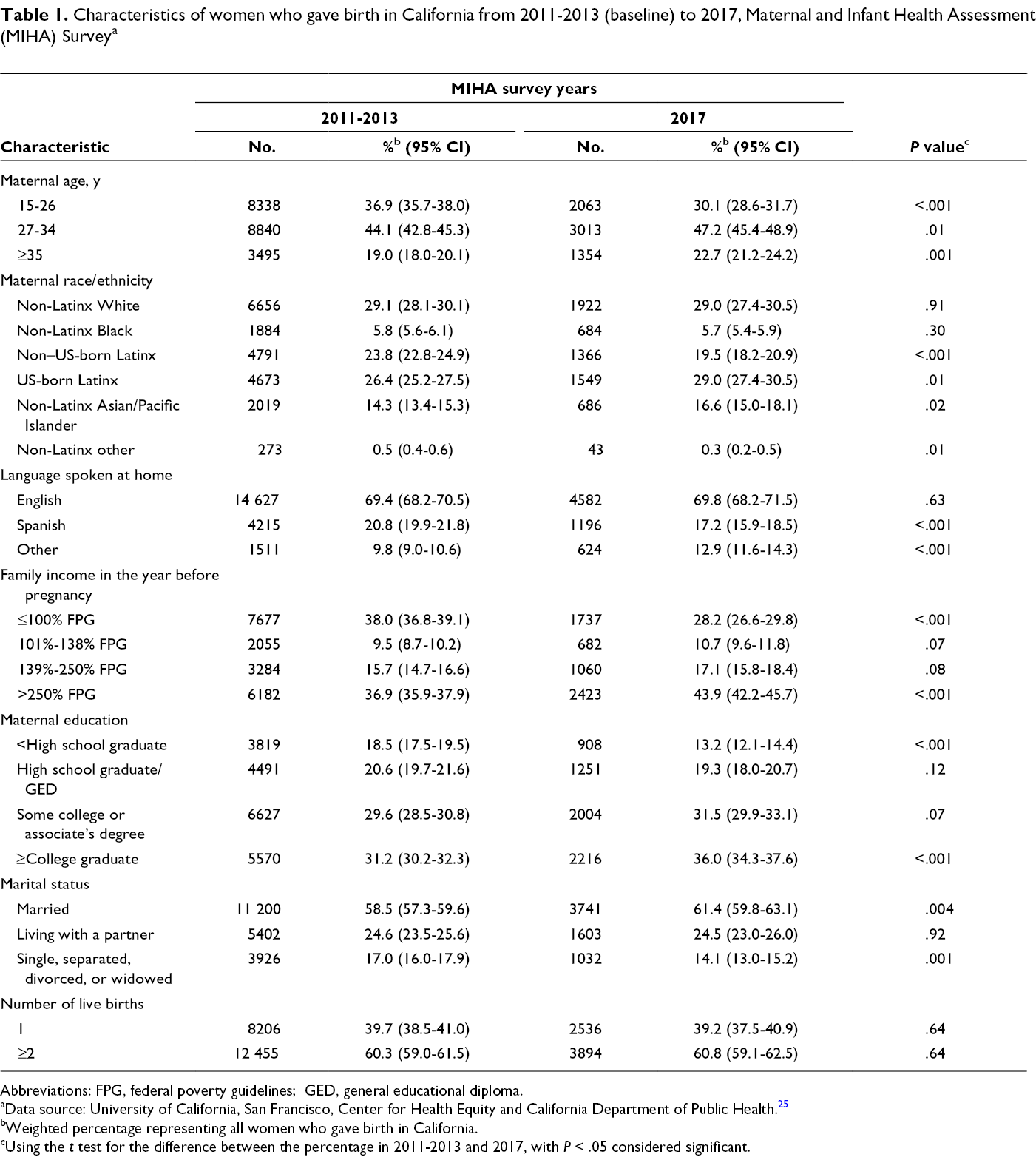
Abbreviations: FPG, federal poverty guidelines; GED, general educational diploma.
aData source: University of California, San Francisco, Center for Health Equity and California Department of Public Health. 25
bWeighted percentage representing all women who gave birth in California.
cUsing the t test for the difference between the percentage in 2011-2013 and 2017, with P < .05 considered significant.
The pre-pregnancy period consistently had the highest percentage of uninsured women, followed by postpartum and prenatal (Figure, Table 2). At baseline, 24.4% of women were uninsured before pregnancy. This percentage decreased to 16.6% in MIHA 2015 (corresponding to the first year after ACA implementation) and to 10.1% in MIHA 2017 (corresponding to 2016 pre-pregnancy coverage). The percentage of women uninsured prenatally was <2% (range, 1.1%-1.8%) each year and did not change significantly from baseline to 2017. The percentage of women uninsured postpartum was 17.4% at baseline and fell to 8.8% by 2015 and to 7.5% in 2017. Nearly 52 000 fewer postpartum women in California were uninsured in 2017 than in 2013.
Health insurance coverage among women who gave birth in California before, during, and after pregnancy, Maternal and Infant Health Assessment (MIHA) Survey, 2011-2017 a
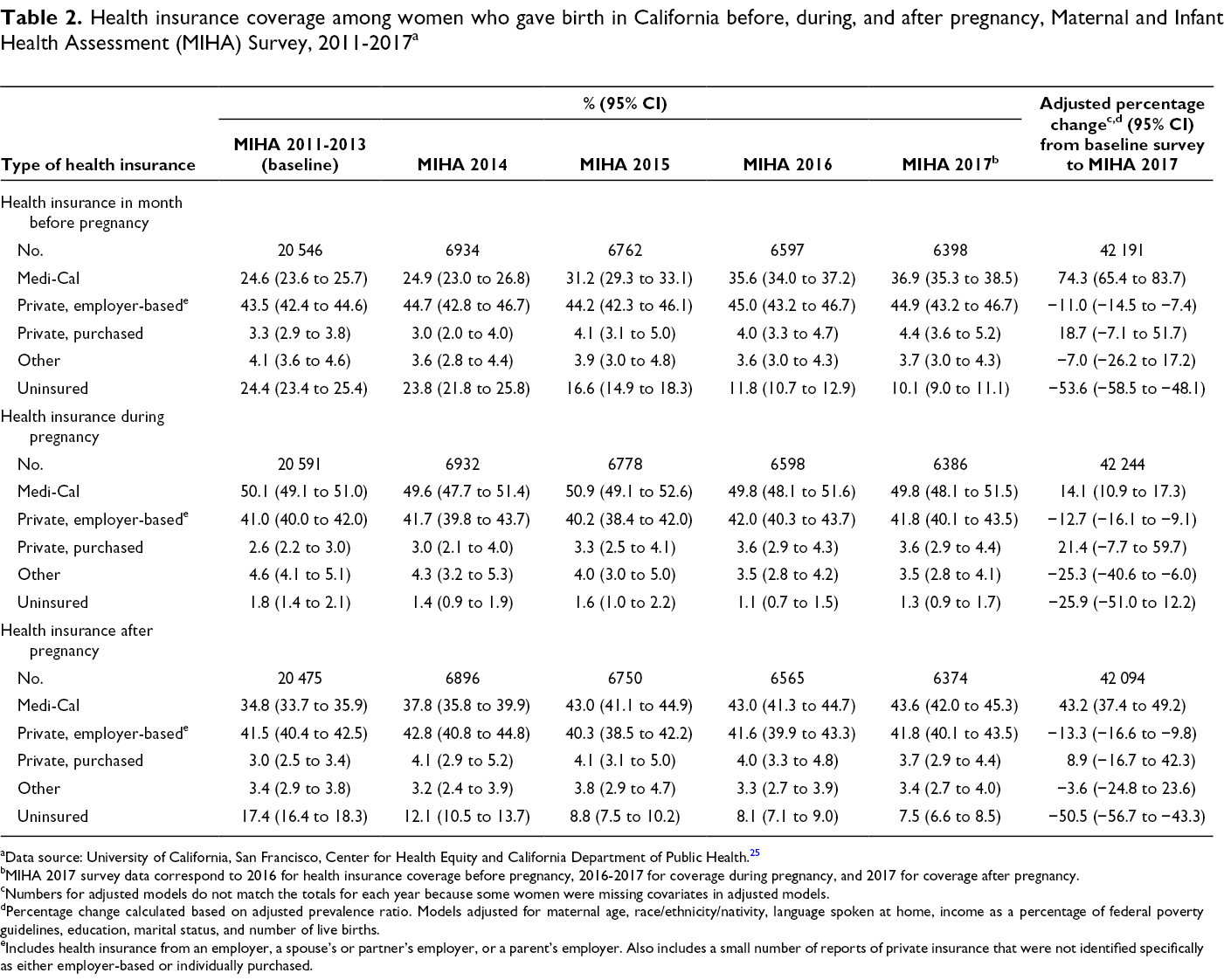
aData source: University of California, San Francisco, Center for Health Equity and California Department of Public Health. 25
bMIHA 2017 survey data correspond to 2016 for health insurance coverage before pregnancy, 2016-2017 for coverage during pregnancy, and 2017 for coverage after pregnancy.
cNumbers for adjusted models do not match the totals for each year because some women were missing covariates in adjusted models.
dPercentage change calculated based on adjusted prevalence ratio. Models adjusted for maternal age, race/ethnicity/nativity, language spoken at home, income as a percentage of federal poverty guidelines, education, marital status, and number of live births.
eIncludes health insurance from an employer, a spouse’s or partner’s employer, or a parent’s employer. Also includes a small number of reports of private insurance that were not identified specifically as either employer-based or individually purchased.
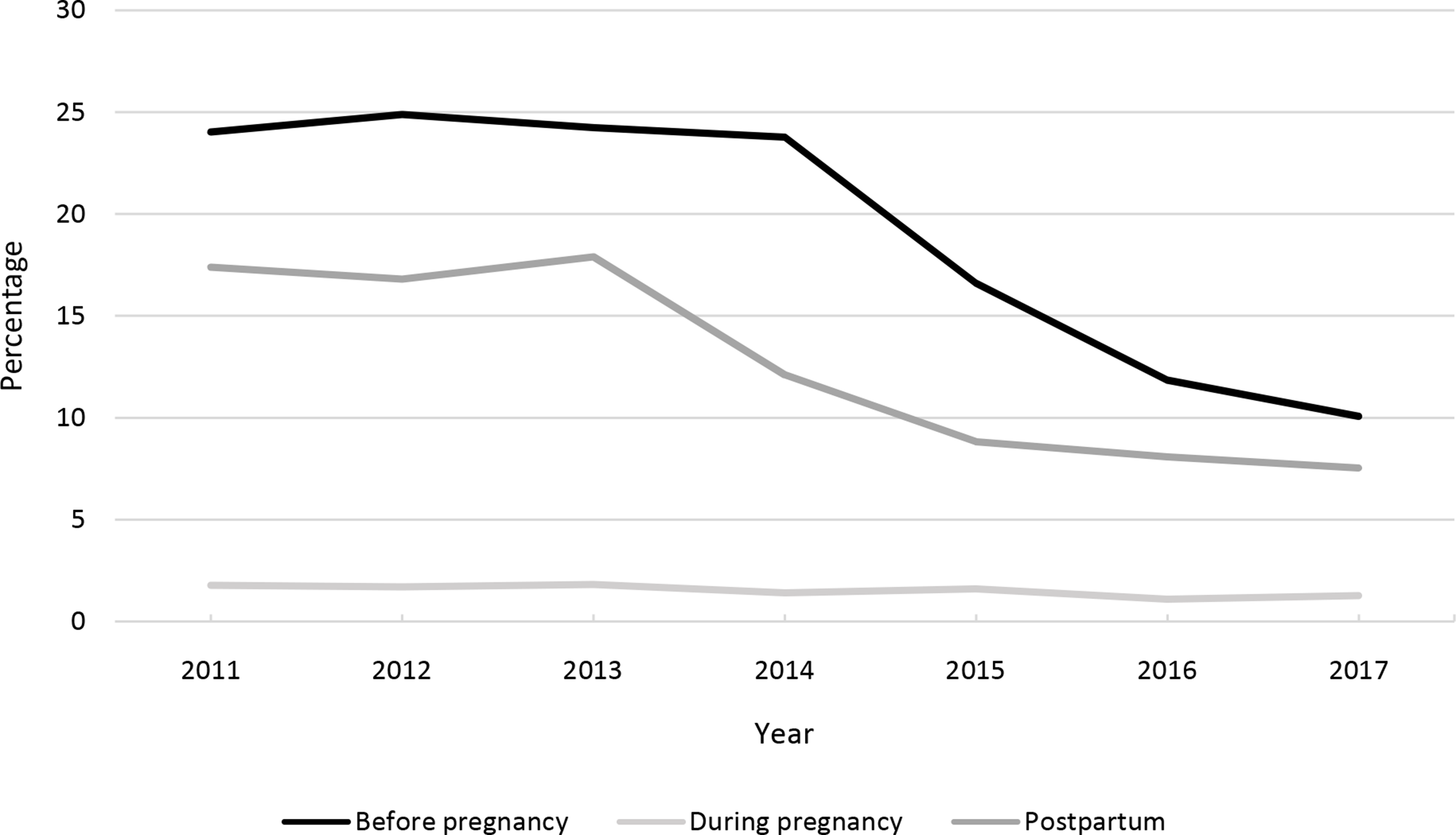
Percentage of women giving birth in California who were uninsured before, during, and after pregnancy, Maternal and Infant Health Assessment Survey 2011-2017. 25
Results adjusted for demographic changes showed similar patterns in the percentage of uninsured women before, during, and after pregnancy (Table 2). By the 2017 survey (2016 pre-pregnancy coverage), the percentage of women uninsured before pregnancy had significantly decreased by 53.6% compared with baseline, controlling for age, race/ethnicity/nativity, language, family income, education, marital status, and number of live births. The adjusted percentage of women with Medi-Cal before pregnancy was 74.3% higher by the 2017 survey than at baseline. Although the unadjusted percentage of women with private-employer sponsored health insurance slightly increased from baseline (43.5%) to 2017 (44.9%), private-employer sponsored health insurance decreased 11.0% after adjustment for population changes over time.
During pregnancy, few women were uninsured (Table 2), and changes from baseline to later years for women with other types of health insurance were small. We found a small increase in Medi-Cal coverage and private-purchased health insurance during pregnancy and a decline in employer-sponsored coverage.
We found substantial improvements in health insurance coverage during the postpartum period (Table 2). The percentage of women uninsured postpartum fell significantly, with a 50.5% decline from baseline to 2017, adjusting for covariates. Similar to the percentage of women with Medi-Cal pre-pregnancy, the percentage of women with Medi-Cal postpartum increased significantly by 43.2% from baseline to 2017, and the percentage of women with private-employer sponsored health insurance decreased significantly by 13.3% during this period.
The decline in the percentage of women who were uninsured postpartum from baseline to 2017 varied by population group (Table 3). All groups, except women with incomes >250% FPG, had a significant decline (≥36.0%) in the likelihood of being uninsured, but we found large differences among groups. Each race/ethnicity/nativity group had <5% of women who were uninsured postpartum during 2017 except for non–US-born Latinx women, 24.1% of whom were uninsured in 2017. Results from interaction terms indicated a significant difference in the association between year and uninsured status by race/ethnicity/nativity and language pre-pregnancy, using the P < .10 cutoff for significance (P = .01 for race/ethnicity/nativity; P = .06 for language) and postpartum (P = .10 for race/ethnicity/nativity; P = .003 for language). Women with family incomes ≤250% FPG were about 6 to 7 times more likely to be uninsured in 2017 than women with family incomes >250% FPG. However, we found no difference in the association between year and uninsured by parity or family income according to tests for interaction for either pre-pregnancy (P = .12 for parity; P = .13 for income) or postpartum (P = .10 for parity; P = .42 for family income).
Percentage of women who gave birth in California who were uninsured postpartum, stratified by maternal characteristics, comparing Maternal and Infant Health Assessment Survey (MIHA) data from 2011-2013 (baseline) and MIHA 2017 a
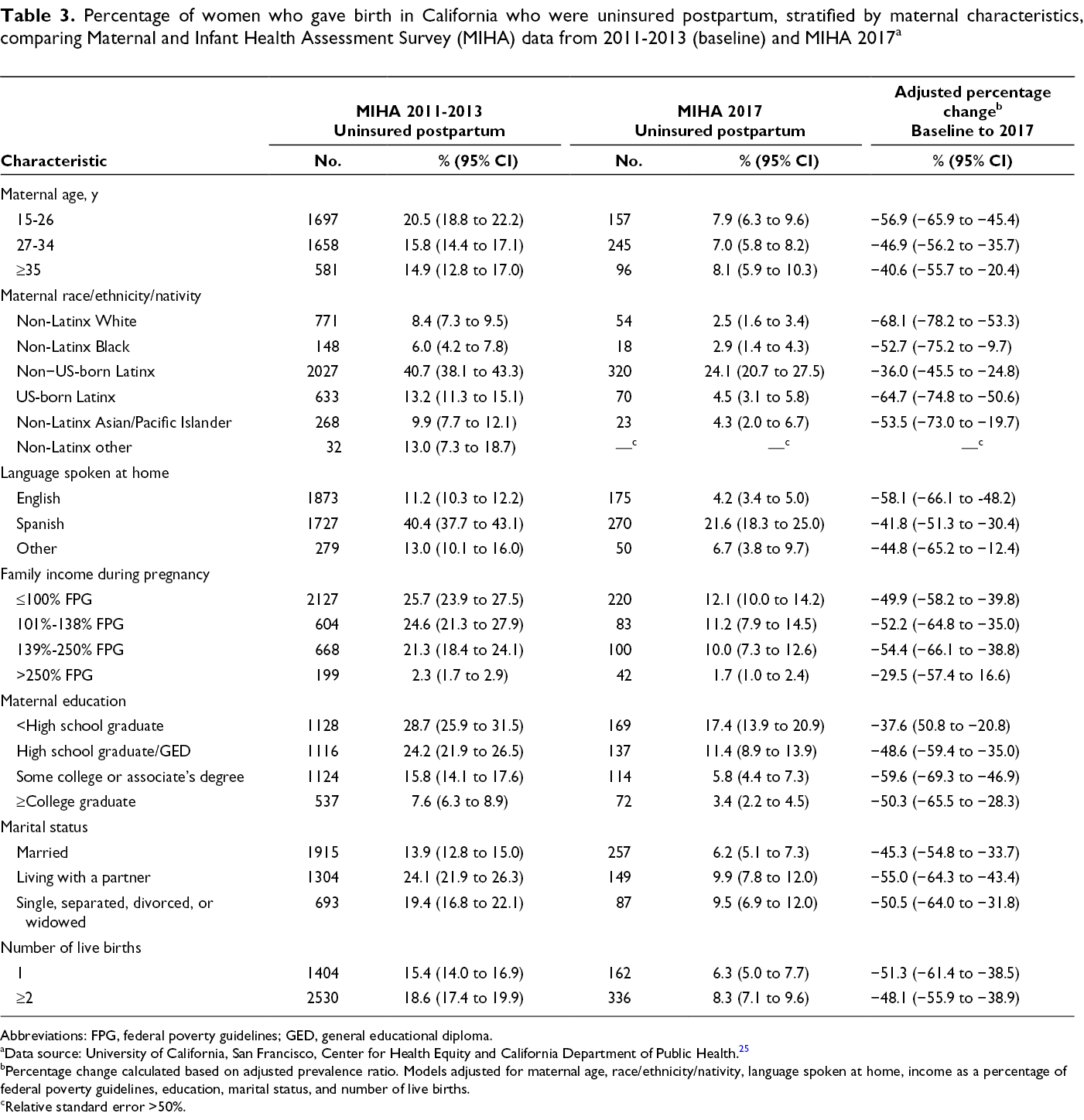
Abbreviations: FPG, federal poverty guidelines; GED, general educational diploma.
aData source: University of California, San Francisco, Center for Health Equity and California Department of Public Health. 25
bPercentage change calculated based on adjusted prevalence ratio. Models adjusted for maternal age, race/ethnicity/nativity, language spoken at home, income as a percentage of federal poverty guidelines, education, marital status, and number of live births.
cRelative standard error >50%.
Discussion
Implementation of the ACA was associated with a dramatic decrease in the percentage of uninsured California women shortly before and after pregnancy, even after adjustment for demographic changes. By 2017, the adjusted percentage of women uninsured postpartum had decreased by half. The large increase in the percentage of women covered by Medi-Cal during the pre-pregnancy and postpartum periods suggests that uninsured women predominantly transitioned into Medi-Cal. Our analysis did not include a comparison population (eg, another nonexpansion state), and our results cannot be considered causal; however, these patterns coincide with changes in Medi-Cal income eligibility cutoffs from 100% to 138% FPG and the expansion of benefits to childless adults. Our results were consistent with our hypothesis based on timing of the survey that the percentage uninsured pre-pregnancy would begin to decline by the 2015 MIHA survey and that the percentage uninsured postpartum would decrease starting in 2014. The timing of the changes points to the success of the ACA in improving health insurance coverage for women both pre-pregnancy and postpartum.
Although the percentage of women without health insurance coverage before pregnancy and postpartum decreased for all racial/ethnic, nativity, income, and parity groups after ACA implementation, the decreases were smaller among non–US-born Latinx women. Undocumented immigrants were not eligible for Covered California plans other than emergency or pregnancy-related Medi-Cal. Immigration status of women in the survey was unknown; it is reasonable to assume that some women were undocumented.
Results from this study of women with a recent live birth in California mirrored results of health insurance trends in other surveys of adults in California and the United States. The 50.5% drop in the percentage uninsured after pregnancy matched the approximately 50% reduction seen in the percentage of uninsured women of reproductive age in California and in Medicaid expansion states after implementation of the ACA. 19 Our results showing an increase in pre- and post-pregnancy Medicaid coverage after ACA implementation were also consistent with the results of other studies.21,25 Our results indicating only small changes in prenatal health insurance coverage were not consistent with previous research that showed a higher percentage of births covered by Medicaid post–ACA implementation in expansion states than in nonexpansion states 23 ; the reason for this difference may be that California has had a higher eligibility threshold (200% FPG) for pregnant women since 1990, and the percentage uninsured by the end of pregnancy was already low. 6
Despite improvements in health insurance coverage before, during, and after pregnancy, disruptions in health insurance from the preconception to postpartum periods may occur because of changes in eligibility. Our findings were consistent with these changes in that only 1.3% of pregnant women were uninsured in 2017 compared with 7.5%-10.1% of women shortly before and after pregnancy. To reduce these disruptions in health insurance status, the American College of Obstetricians and Gynecologists, the American Academy of Pediatrics, the American Medical Association, and other physician groups have made proposals to extend pregnancy-related Medicaid coverage from 60 days to 12 months postpartum. 26 In California, this extension has been proposed for pregnant or postpartum women diagnosed with a mental health condition, with a tentative start date of July 2020. 26 Extending postpartum health insurance coverage may be particularly critical for improving maternal morbidity and mortality.
Limitations
This study had several limitations. First, the study was limited by self-reporting of health insurance coverage. As with all self-reported variables, reports of health insurance coverage could be subject to error. However, self-reported family income and health insurance patterns were consistent with each other, and health insurance plan names provided generally coincided with the self-reported categories, suggesting that the measure was fairly robust. Women’s recall of health insurance plans would be unlikely to be affected by ACA implementation; as such, results would be biased toward the null. Second, the baseline period used in this analysis (2011-2013) may have included some women who enrolled in California’s early expansion Low-Income Health Plan program. However, enrollment in this early expansion program was associated with only a slight increase in the actual number of adults receiving Medicaid until 1 year after full ACA expansion; thus, we still expected to see changes after full Medicaid expansion.16,18
Conclusions
The percentage of women uninsured pre-pregnancy and postpartum dropped significantly after implementation of the ACA, even after we controlled for maternal characteristics. Similar to findings in other populations,9,15,19,21-23,27-31 results from this study of childbearing women in California show that the ACA had a positive effect on women’s health insurance coverage before, during, and after pregnancy. Expansions in pre-pregnancy and postpartum health insurance coverage, coupled with existing high rates of health insurance coverage during pregnancy, provided more women with health insurance coverage across the perinatal period, potentially greatly increasing access to maternal health care.
Despite significant decreases in the percentage of uninsured women before and after pregnancy, in the 2017 survey, 10.1% of women were uninsured before pregnancy and 7.5% of women were uninsured after pregnancy, suggesting that efforts could be made to provide additional health insurance coverage, such as extending postpartum Medi-Cal coverage beyond 60 days. Although the United States needs to address such health insurance–related issues as rising premiums and large deductibles, the passage of the ACA was an important step toward providing pregnant women in the United States with affordable health care.
Footnotes
Acknowledgments
The authors thank the leadership of the Maternal, Child, and Adolescent Health Division of the California Department of Public Health for their review of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Maternal, Child, and Adolescent Health Division of the California Department of Public Health using federal funds from the Title V Maternal and Child Health Block Grant and the Special Supplemental Nutrition Program for Women, Infants, and Children through an interagency agreement between the University of California, San Francisco, and the California Department of Public Health (grant number 16-10016).