
Abstract
Objectives
Research examining the effect of changes in Medicaid dental benefits on emergency department (ED) use for dental conditions has had mixed results. We examined the effect of changes in Medicaid dental benefits on ED use for nontraumatic dental conditions (NTDCs) among adults in Massachusetts before and after Medicaid dental benefits for adults were eliminated (July 2010) and partially restored (January 2013).
Methods
We used 2009-2013 data from the Massachusetts All-Payer Claims Database. The study population included Medicaid enrollees aged ≥21 who made a visit to the ED for an NTDC that was paid for by Medicaid during the study period. We used an interrupted time-series study design and segmented regression model to assess the effect of the policy changes on ED use for NTDCs. We also conducted a subanalysis by patient age, sex, and geographic location.
Results
During the study period, 21 731 Medicaid enrollees aged ≥21 made 35 660 NTDC ED visits. Eliminating comprehensive dental benefits led to a significant increase in the use of EDs for NTDCs. This increase occurred over time (11% increase at 15 months after elimination of comprehensive dental benefits; estimate, 0.64 [95% CI, 0.07-1.21]; P = .03) rather than immediately after the policy change took effect. The partial restoration of certain dental benefits led to a significant decrease in the rate of ED visits for NTDCs over time (15.7% decrease at 5 months after partial restoration of certain dental benefits; estimate, –0.97 [95% CI, –1.83 to –0.11]; P = .03).
Conclusion
Strengthening dental coverage policies for adult Medicaid enrollees could decrease their reliance on EDs for NTDCs.
Medicaid is the primary provider of dental insurance coverage for low-income adults in the United States. Dental coverage for adults is an optional benefit under the federal Medicaid program, and individual states can determine dental coverage and the type of dental benefits that are offered to adult Medicaid enrollees. Thus, uptake varies by state and maintenance of dental benefits is uncertain 1 ; fewer than half of the states provided comprehensive dental benefits to their adult Medicaid enrollees as of 2016. 2
Recent research outlines the disparities in access to dental care and oral health outcomes among Medicaid enrollees. 3 -5 Apart from the well-documented barriers Medicaid enrollees have in accessing dental care (eg, oral health literacy, transportation, dental provider participation in Medicaid), researchers have hypothesized that inconsistent dental coverage provided by Medicaid is a key factor for impeding access to routine dental care in this population. 6,7 Inadequate access to routine care can result in patients deferring care or turning to more expensive and inappropriate care settings, such as emergency departments (EDs). 8,9
The number of visits to EDs for nontraumatic dental conditions (NTDCs) 10 -12 is on the rise, and most of these visits are made by adult Medicaid enrollees. From 2001 to 2008, national estimates for total ED visits for all conditions increased approximately 13% and for ED dental visit increased more than 41%. 5,11 Several studies examined how changes in Medicaid dental benefits for adults affected ED use for dental conditions in this population. Cohen et al 13 reported a 12% increase in the rate of nonurgent ED dental visits in Maryland after Medicaid dental benefits for adults were eliminated in 1993. Wallace et al 14 reported that after Oregon limited dental benefits for adult Medicaid patients in 2003, ED use for non-urgent dental conditions increased by 102%. A seminal study in California reported an immediate significant increase of about 1800 additional ED visits for dental conditions among adults after comprehensive Medicaid dental benefits were eliminated in 2010. 15 A more recent study in Kentucky that examined data from 2010-2014 found that adding dental benefits for adults under Medicaid expansion increased the rate of nonurgent ED dental visits. 16 A study examining data from 2010 in 29 states found that providing Medicaid dental benefits did not reduce the rate of ED dental visits. 17 Thus, current evidence on the effect of changes in Medicaid dental benefits on ED use for dental conditions is mixed, and these findings cannot be generalized to other states that have faced similar cuts. Therefore, continued assessment is needed to provide evidence on how changes in Medicaid dental benefits affect ED use for NTDCs.
In Massachusetts, Medicaid dental benefits for adults have been cut and restored multiple times during the past decade. However, no state-level study has examined the effect of these policy changes on ED use for dental conditions in Massachusetts. The objective of our study was to examine the effect of eliminating comprehensive dental benefits for adult Medicaid enrollees in Massachusetts, which took effect in July 2010, on ED use for NTDCs. In addition, we examined the effect of partial restoration of certain dental benefits on ED visits for NTDCs, which took effect in January 2013. To our knowledge, our study is the first to examine the effect of both dental benefits elimination and dental benefits restoration on ED visits for NTDCs in a single study. The examination of this bidirectional change in Medicaid adult dental benefits in a single study population will provide evidence of the effect of Medicaid dental coverage on ED visits and provide insight into the feasibility of reversing the effect of eliminating benefits.
Methods
Data Source
We used 2009-2013 data from the Massachusetts All-Payer Claims Database (unpublished data, Massachusetts Center for Health Information and Analysis, 2013). The study population included adult Medicaid enrollees aged ≥21 who made a visit to the ED for an NTDC that was paid for by Medicaid during the study period.
Study Design
We used an interrupted time-series study design, a strong quasi-experimental design that primarily consists of equally spaced observations interrupted by an intervention at a known point in time, thus creating ≥2 time periods. The design is robust despite the lack of randomization, because it allows assessment of the intervention’s effect by applying regression methods to multiple pre–post-intervention observations. 18 This study design offers several advantages. For one, it allows detection of and accounting for time trends that are unrelated to the intervention. 18 It also controls for secular trends (important in examining dental ED visits that are increasing nationally, even in the absence of any intervention), avoids individual confounders when data are analyzed at the aggregate level, and enables one to distinguish between immediate and longer-term effects of the intervention(s). 18,19 To minimize threats to internal validity because of history and maturation, we included 3 other outcome measures for ambulatory care–sensitive conditions. These outcomes are related but different from the main outcome of interest and would not be expected to change after the intervention of interest within the same group of participants.
Variables
The main outcome variable was the monthly rate of ED visits for NTDCs per 100 000 Medicaid enrollees. We calculated the monthly rate of NTDC ED visits by dividing the number of NTDC ED visits for each month of the study period by the number of enrollees for each month. The primary independent variables of interest were the 2 policy changes: (1) elimination of comprehensive Medicaid adult dental benefits on July 1, 2010 (during the 19th month of the study), and (2) partial restoration of dental benefits on January 1, 2013 (during the 49th month of the study). Similarly, we calculated the monthly rate of ED visits per 100 000 Medicaid enrollees for 3 other outcomes: the ambulatory care–sensitive conditions asthma, diabetes, and backache. Our rationale for selecting the 3 ambulatory care–sensitive conditions in the intervention group was that patients need not use EDs for these conditions; timely and effective outpatient care can prevent or minimize the need for an ED visit for these conditions, similar to NTDCs. Second, by using these conditions, we can compare our results with the results of the study conducted in California, which used a similar methodology. 15
We used the following International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) codes to identify NTDCs: 521-521.9 (disease of hard tissues of teeth), 522-522.9 (disease of pulp and periapical tissues), 523-523.9 (gingival and periodontal disease), 525-525.9 (other diseases and conditions of the teeth and supporting structures), and 528-528.9 (diseases of the oral soft tissues excluding lesions specific for gingiva and tongue). 20 The ICD-9-CM diagnostic codes used to identify the 3 ambulatory care–sensitive conditions were 493-493.9 (asthma), 7245 (backache), and 250-250.9 (diabetes).
Statistical Analysis
We used a segmented linear regression model to examine the effect of the policy interventions in adult Medicaid dental benefits on NTDC ED visits and on ED visits for asthma, diabetes, and backache. A change in intercept would indicate an immediate effect, and a change in slope after the new policy took effect would indicate an effect over time. We quantified these effects by using the following equation:

Yt = monthly rate of NTDC ED visits at time t
We examined the overall effect of the policy on NTDC ED visits and any differential effects for subgroups of the Medicaid population by patient’s age, sex, and geographic location. Analyzing the effect of the policy change across subgroups of the population can identify groups at high risk of making NTDC ED visits, thereby enabling decision makers to implement targeted policies and interventions. We excluded people aged ≥65 living in micropolitan or rural non-core areas from the subgroup analysis because they composed <5% of the patient population that had ED visits for NTDCs. We tested models for the presence of autocorrelation by using the Durbin–Watson statistic, seasonality, and structural break, and we adjusted the models accordingly. In addition, based on distribution of the data, we removed 2 anomalous observations, likely representing incomplete data collection, from the final models. We performed sensitivity analyses to test the robustness of our study findings. (Details about modeling adjustments and the results of these analyses can be accessed at https://drive.google.com/file/d/1O9BJrez8SrbunVJmJc9kuwputPHCyRA3/view.)
We conducted all statistical analyses using SAS version 9.4. 21 We determined significance at the .05 level. The Northeastern University Institutional Review Board, an internal Data Privacy Committee, and an external Data Release Committee at the Center for Health Information and Analysis approved the study protocol.
Results
During the 5-year study period, 21 731 adult Medicaid enrollees made 35 660 NTDC ED visits in Massachusetts, with an average of 46.7 NTDC ED visits per 100 000 adult Medicaid enrollees per month (Table 1). Most NTDC ED visits were made by adults aged 21-35 (55.9%) and by people living in large metropolitan areas (60.1%).
Characteristics of adult Medicaid enrollees who visited the emergency department for nontraumatic dental conditions, before and after a policy change eliminating comprehensive dental benefits, Massachusetts, 2009-2013 a
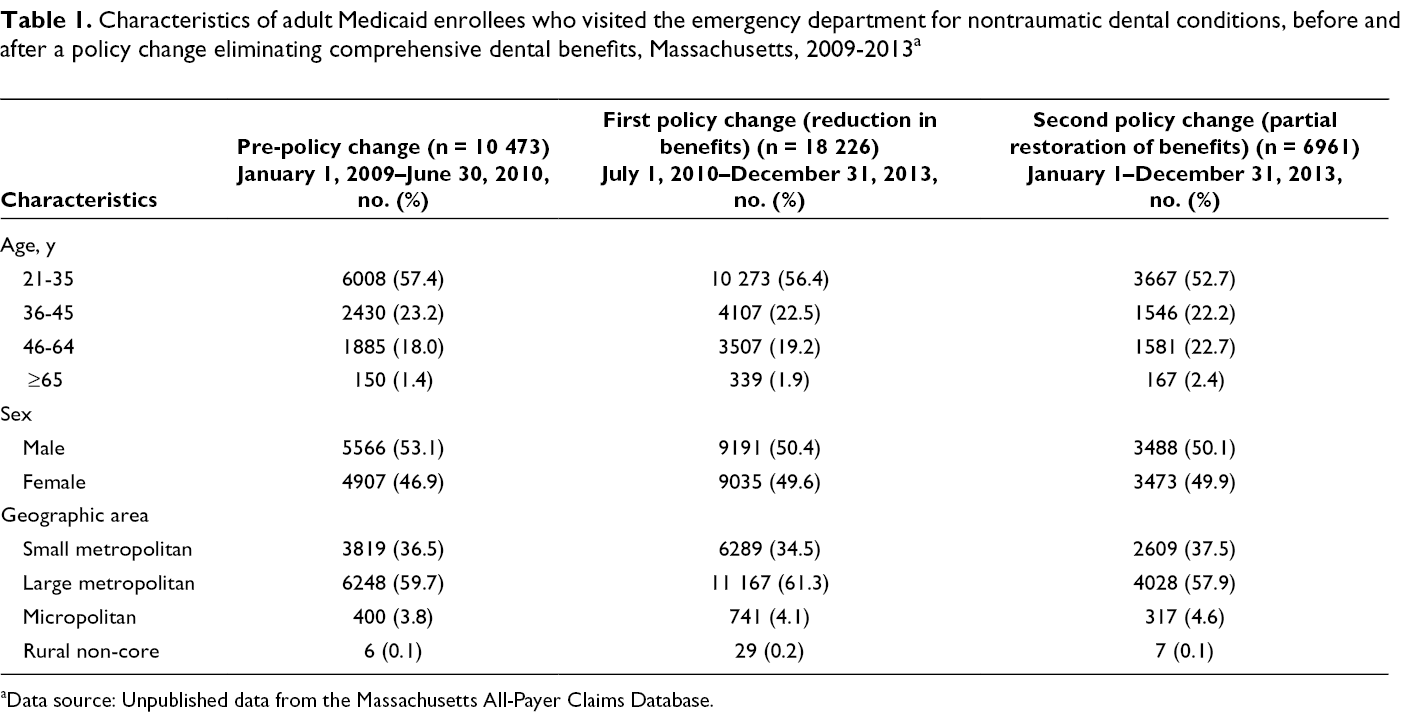
aData source: Unpublished data from the Massachusetts All-Payer Claims Database.
The elimination of comprehensive dental benefits led to an increase in the rate of NTDC ED visits over time and not immediately after the policy change took effect. This increase can be interpreted as a relative increase of 11% in the rate of NTDC ED visits at 15 months after the policy change took effect (estimate, 0.64 [95% CI, 0.07-1.21]; P = .03) (Table 2). The partial restoration of certain dental benefits was followed by a significant decrease in the rate of NTDC ED visits over time. This decrease can be interpreted as a 15.7% relative decrease in the rate of NTDC ED visits at 5 months after the partial restoration of dental benefits (estimate, –0.97 [95% CI, –1.83 to –0.11]; P = .03).
Segmented linear regression results for emergency department (ED) visits for nontraumatic dental conditions among adult Medicaid enrollees, Massachusetts, 2009-2013 a
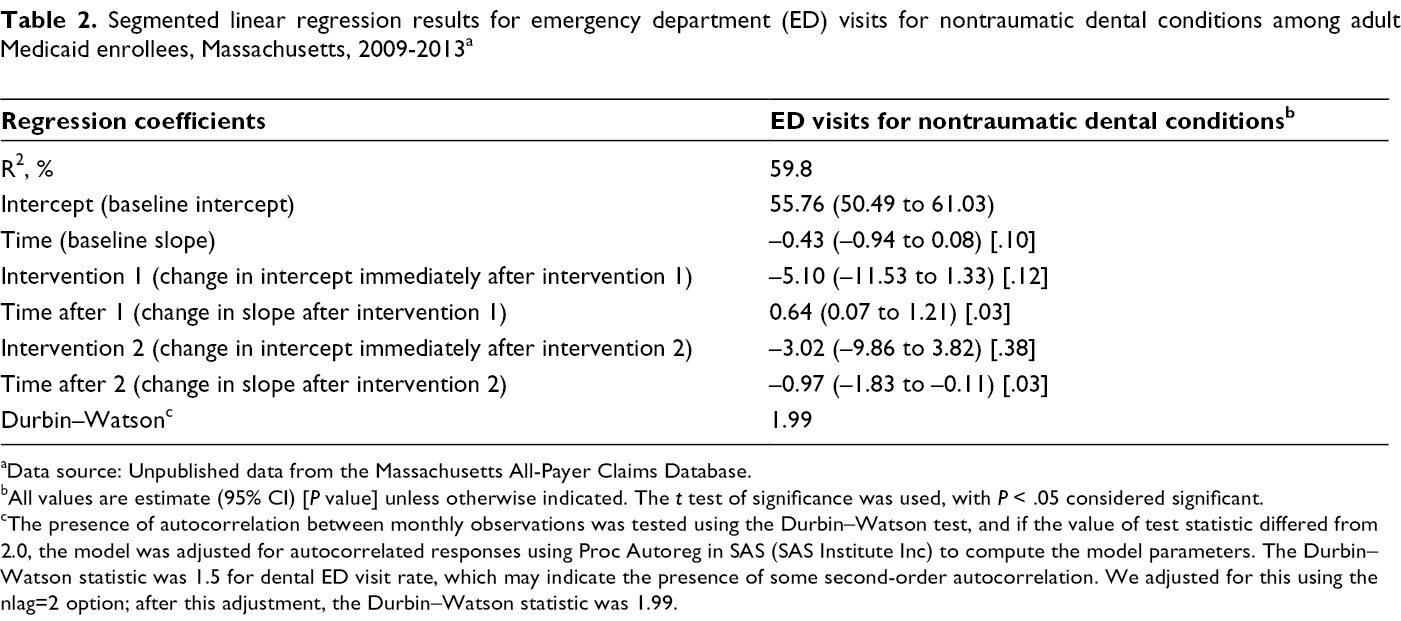
aData source: Unpublished data from the Massachusetts All-Payer Claims Database.
bAll values are estimate (95% CI) [P value] unless otherwise indicated. The t test of significance was used, with P < .05 considered significant.
cThe presence of autocorrelation between monthly observations was tested using the Durbin–Watson test, and if the value of test statistic differed from 2.0, the model was adjusted for autocorrelated responses using Proc Autoreg in SAS (SAS Institute Inc) to compute the model parameters. The Durbin–Watson statistic was 1.5 for dental ED visit rate, which may indicate the presence of some second-order autocorrelation. We adjusted for this using the nlag=2 option; after this adjustment, the Durbin–Watson statistic was 1.99.
The rate of NTDC ED visits per 100 000 Medicaid enrollees before the elimination of dental benefits showed a decreasing trend (Figure). The rate of NTDC ED visits dropped immediately after the policy change took effect, followed by an upward trend until the partial restoration of certain dental benefits took effect. After the partial restoration of dental benefits, the rate of NTDC ED visits decreased immediately and over time.
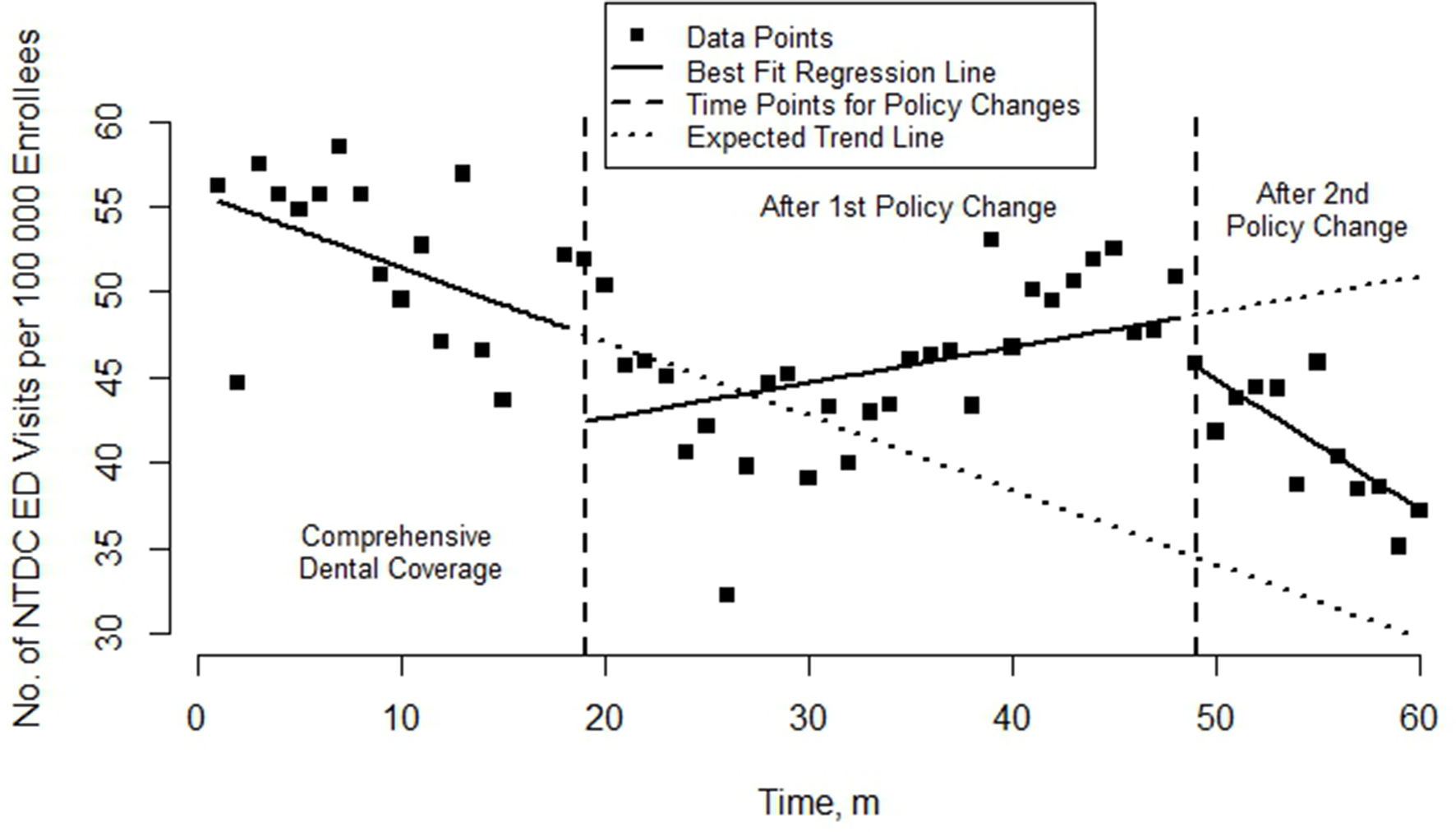
Rate of emergency department (ED) visits for nontraumatic dental conditions (NTDCs) per 100 000 Medicaid enrollees per month, Massachusetts, 2009-2013. Medicaid dental benefits for adults were eliminated in July 2010 and partially restored in January 2013. Data source: Unpublished data from the Massachusetts All-Payer Claims Database.
None of the 3 ambulatory care–sensitive conditions showed any significant change in the rate of ED visits over time after the policy changes. (Data available at https://drive.google.com/file/d/1O9BJrez8SrbunVJmJc9kuwputPHCyRA3/view.) Our subanalysis showed that women and enrollees living in large metropolitan areas had an increase in the rate of NTDC ED visits over time after the elimination of comprehensive dental benefits. Men and people aged 46-64 had a significant and immediate decrease in the rate of NTDC ED visits after the elimination of dental benefits. (Data available at https://drive.google.com/file/d/1O9BJrez8SrbunVJmJc9kuwputPHCyRA3/view.)
Discussion
Our study found that elimination of comprehensive Medicaid dental benefits for adults was associated with an increase in the use of EDs for NTDCs in Massachusetts over time but not immediately after the policy change took effect. One possible explanation for the increase in NTDC ED visits could be that patients deferred routine dental care in the absence of comprehensive dental benefit coverage. 15 As a result of not receiving timely care, they had acute symptoms that could not be managed at home and turned to EDs for dental care as a last resort. 15 Thus, the increase in NTDC ED visits over time may have been the result of a pent-up demand for dental services.
Our findings indicate that the reduction in adult Medicaid dental benefits had a differential effect across patient subgroups. Adults aged 21-35 accounted for most NTDC ED visits during the study period. This finding aligns with analyses of national data that revealed that young adults were at highest risk for visiting an ED for dental problems. 5 Nationally, the number of dentist visits among this age group has declined, and young adults may be replacing dentist visits with ED visits. 22 It is unclear why women and people residing in large metropolitan areas would have a greater increase in the rate of NTDC ED visits than other groups; however, other studies have found that both groups have been increasingly using EDs for all other causes. 23 Future research should aim to identify the barriers that are independent of dental insurance coverage experienced by Medicaid subgroups to better serve their needs. In addition, future research should assess a possible relationship between proximity to an ED and proximity to a dental provider and examine community resources to understand why patients in a certain geographic location have an increased likelihood of using EDs for NTDCs.
We examined the elimination and restoration of dental benefits for Medicaid enrollees in the same study population, which distinguishes our study from previous studies. As a result, our findings showed that partial restoration of dental benefits reversed the increasing trend in NTDC ED visits seen before the policy change. A dose–response relationship between the type of dental benefits offered to adult Medicaid enrollees and NTDC ED visits is possible. It is also possible that the type of dental benefits covered may influence the dental care–seeking behavior in this population. Thus, future research should examine the differential effects of coverage on ED use for NTDCs. This research may assist policy makers in making cost-effective decisions that align with the dental needs of this population.
Based on previous research, 13 -15 we did not expect to see a decrease in the rate of NTDC ED visits immediately after the elimination of comprehensive dental benefits. Although the decrease in the rate of NTDC ED visits in our study was not significant, except among older enrollees (aged 46-64) and men, we can attribute this finding to a number of factors. Cohen et al 24 reported that a lack of understanding of the changes in dental benefits and the resulting confusion for enrollees could have an effect on how patients choose to access dental care. This lack of understanding could have been true for our study as well, because it does not appear that MassHealth (the Massachusetts Medicaid program) had any substantial outreach efforts in place at the time to help Medicaid enrollees understand the changes in dental benefit coverage. Evidence for this rationale comes from a study conducted to assess the effect of this policy change on dental service use at community health centers in Massachusetts. That study stated that several dental directors reported that patients thought they had lost all dental benefits based on the communication received from MassHealth and had to be educated on which services they could receive and which services were not covered. 25 They also reported that private dentists were confused about the changes in dental benefit coverage; as a result, some patient services could not be completed within the timeline provided by MassHealth, 25 thereby potentially prompting patients to seek other sources of care. Second, 96% of the community health centers offering dental services in Massachusetts had a 20%-100% increase in volume of Medicaid patients seeking dental care and a 90% increase in patient emergencies and walk-ins for dental conditions at these centers within 6 months of the policy change. 25 This finding suggests that some Medicaid enrollees may have opted to receive dental care at other sources of care (eg, community health centers) before turning to EDs for dental care. A combination of pent-up demand, lack of understanding of the changes in dental service coverage, and reliance on other sources of care (eg, community health centers) could have led to the initial decrease followed by the increase in ED use for dental conditions over time.
As the current discussion on the expansion of eligibility for Medicaid under the Affordable Care Act continues and several states contemplate changing their Medicaid adult dental coverage policy under the expansion efforts, these findings are of importance for policy makers. Policy makers should consider our findings for Massachusetts and the implications for whether Medicaid enrollees access dental care in appropriate settings (dental offices) and rely less on EDs for nontraumatic dental care.
In addition, our study findings should be interpreted with the understanding that Medicaid enrollees are known to have several other barriers in accessing dental care that are independent of dental insurance coverage. Some well-documented barriers include lack of availability of dental providers that accept Medicaid, competing health priorities, and limited oral health literacy. 26 As of 2014, only 44% of dentists in Massachusetts accepted Medicaid insurance, citing burdensome administrative requirements, lengthy payment wait times, missed appointments, and low reimbursement rates as barriers to participation. 27 Limited oral health literacy can result in a lack of familiarity with appropriate treatment options and can lead to inappropriate use of EDs. 16,28 As reported by Fingar et al, 17 in the presence of these other barriers, expanded Medicaid coverage does not guarantee increased access to dental care nor does it decrease ED use for dental conditions. Therefore, along with strengthening coverage policies, it is important that policy makers put into place the enabling conditions to ensure that the Medicaid population can access care. Evidence strongly shows that these conditions include expanded outreach to Medicaid beneficiaries and dental care providers 29 ; improved health care provider incentive structures, including streamlined administrative structures and adjusted fees 30 -32 ; and innovative practice models. 33,34
Limitations
In terms of study caveats, apart from the inherent limitations of claims data, we were not able to assess the cost associated with NTDC ED use, although previous studies have shown that the cost of providing comprehensive dental benefits exceeds the cost of NTDC ED visits. But it is important to note that the cost of providing dental care in the absence of comprehensive dental benefits may be shifted to other sources of care. Therefore, further study of the financial impact of eliminating comprehensive dental benefits for Medicaid enrollees on ED visits and other sources of care is needed.
Conclusions
Our findings contribute to the current debate about the effect of Medicaid dental benefits for adults on ED use for dental conditions. To our knowledge, our study is the first state-level study conducted in Massachusetts to examine (1) the effect of eliminating comprehensive dental benefits for adult Medicaid enrollees on NTDC ED visits and (2) both elimination and partial restoration of dental benefits. Overall, our findings indicate that reliance on EDs for NTDCs in Massachusetts increased as a result of eliminating comprehensive dental benefits for adult Medicaid enrollees. Our findings indicate a shift in dental care–seeking behavior among Medicaid enrollees. NTDC ED visits are one way in which unmet dental needs manifest, and future research should examine other aspects of the dental care delivery system to fully understand the effect that changes in Medicaid dental benefits have on access to dental care in this population.
Footnotes
Authors’ Note
Partial findings from this article were presented as a poster at the AcademyHealth Annual Research Meeting in June 2019.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Northeastern University Tier-1 grant funds were used to gain access to the All-Payer Claims Database.