
Abstract
Community resilience is a community’s ability to maintain functioning (ie, delivery of services) during and after a disaster event. The Composite of Post-Event Well-Being (COPEWELL) is a system dynamics model of community resilience that predicts a community’s disaster-specific functioning over time. We explored COPEWELL’s usefulness as a practice-based tool for understanding community resilience and to engage partners in identifying resilience-strengthening strategies. In 2014, along with academic partners, the New York City Department of Health and Mental Hygiene organized an interdisciplinary work group that used COPEWELL to advance cross-sector engagement, design approaches to understand and strengthen community resilience, and identify local data to explore COPEWELL implementation at neighborhood levels. The authors conducted participant interviews and collected shared experiences to capture information on lessons learned. The COPEWELL model led to an improved understanding of community resilience among agency members and community partners. Integration and enhanced alignment of efforts among preparedness, disaster resilience, and community development emerged. The work group identified strategies to strengthen resilience. Searches of neighborhood-level data sets and mapping helped prioritize communities that are vulnerable to disasters (eg, medically vulnerable, socially isolated, low income). These actions increased understanding of available data, identified data gaps, and generated ideas for future data collection. The COPEWELL model can be used to drive an understanding of resilience, identify key geographic areas at risk during and after a disaster, spur efforts to build on local metrics, and result in innovative interventions that integrate and align efforts among emergency preparedness, community development, and broader public health initiatives.
Keywords
Resilient communities are communities that are working to prepare for, withstand, respond to, and recover from disasters, yet few communities have resilience that functions at the highest levels. Varying models and methodologies to characterize and strengthen community resilience are being developed. 1 -5 Communities across the United States lack practical tools and resources to predict resilience or to support efforts that connect resilience-strengthening efforts with routine work in public health, community development, or emergency preparedness.
The Composite of Post-Event Well-Being (COPEWELL) is a system dynamics model that predicts community resilience, defined as a community’s ability to maintain functioning (delivery of services) during and after a disaster event. 6 Developed with funding from the Centers for Disease Control and Prevention, COPEWELL aims to support communities in strengthening their resilience to large-scale disasters. In the COPEWELL model, resilience uniquely consists of both a community’s resistance (against the initial drop in functioning brought on by a disaster) and its recovery (the trajectory back toward or even beyond its pre-event ability to deliver goods and services). COPEWELL combines a strong pictorial framework portraying the many factors influencing community resilience and how they interact (the conceptual model) with an underlying computational capability (the computational model) to predict how a given community’s functioning might play out over time in response to a disaster event. The computational model uses system dynamics modeling to generate a predicted time course of community functioning during and after a disaster (Figure). Information on the model and its development is available elsewhere. 6
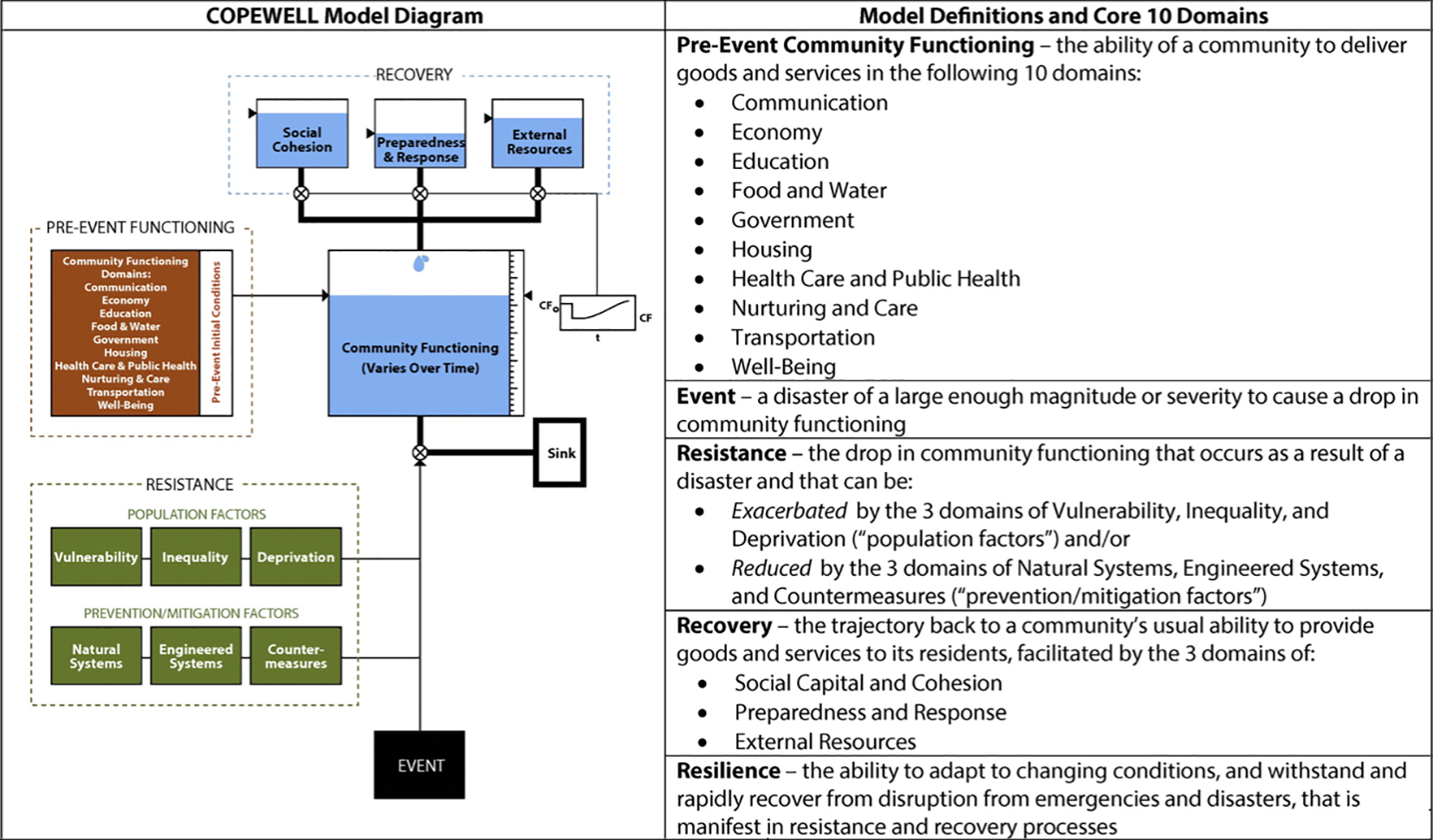
Composite of Post-Event Well-Being (COPEWELL) model of community resilience. The figure shows the conceptual model of community resilience, which guides users visually through the model cycle and describes the domains of pre-event community functioning, event, resistance, recovery, and resilience. Abbreviations: CF, community functioning; t, time. Modified from Links et al. 6
Purpose
In this case study, we explored how a public health agency in a large, densely populated, highly diverse urban setting (New York City) used COPEWELL to further elucidate community resilience and its influencers and to spark initiatives aimed at strengthening functioning and resilience. The work’s initial focus was on further development and use of the computational model (including a search for local indicators), as well as identifying what uses and benefits (both measurement and program related) might emerge in a field application of COPEWELL’s conceptual model.
Methods
At the invitation of academic partners developing the COPEWELL model at the Johns Hopkins University Center for Public Health Preparedness and the University of Delaware Disaster Research Center, the New York City Department of Health and Mental Hygiene (DOHMH) Office of Emergency Preparedness and Response formed an interagency work group, COPEWELL-NYC, to work with developers to explore the COPEWELL model, provide feedback on applied uses and value, discuss potential indicators of community functioning and resilience for use in the computational model, and design strategies to apply the model in locally relevant ways. This 9-member work group included staff representatives from the DOHMH Office of Emergency Preparedness and Response, Division of Environmental Health, Division of Mental Hygiene, Division of Prevention and Primary Care, and Center for Health Equity. Representatives from community-based organizations (CBOs) in New York City and community liaisons also participated. This effort aligned well with an existing key charge of DOHMH to enhance the resilience of New York City communities.
The work group used the COPEWELL model to guide internal and external discussions of community resilience, frame and prioritize additional data collection, and help identify and plan resilience-strengthening efforts. In addition to team meetings and project-lead telephone calls for coordination, the work group developed subcommittees that convened their own meetings between the work group’s monthly meetings: the Computational Modeling Work Group to identify and select locally available, routinely collected data at the subjurisdictional level for use in the computational model; the Survey/Focus Group Work Group to oversee the collection of potential new qualitative and quantitative data to advance cross-office understanding of resilience and generate ideas for candidate public health interventions; and the Candidate Intervention Work Group to evaluate the implementation potential of and further develop proposed intervention ideas. A fourth work group, Dissemination and Publication, was originally planned to organize community presentations on COPEWELL across New York City. However, agency staffing changes and additional emergency activations limited what could be done in this area.
Using this structure and the COPEWELL framework, the COPEWELL-NYC work group undertook multiple tasks.
Identification of Local Indicators
This effort identified indicators capable of generating outputs from the computational model at a subcounty geographic scale. The Computational Modeling Work Group initially identified several hundred potential local indicators. Many were excluded because they were not publicly available, did not reflect a geographic scale below the borough level, or were not collected regularly. Most remaining indicators originated from the US Census Bureau, DOHMH’s Community Health Survey, and city agencies and organizations such as the Metropolitan Transportation Authority and NYC Emergency Management (via NYC Open Data). The work group collected data at the zip-code level and at the level of the 42 United Hospital Fund neighborhoods. The United Hospital Fund is a nonprofit organization that, among other things, collects data in 42 contiguous geographic areas that cover New York City (https://uhfnyc.org).
CBO Focus Groups on Preparedness
In 2011, before Superstorm Sandy, DOHMH had worked with a consultant to conduct 6 focus group discussions to understand (1) the needs and challenges of CBOs in underserved New York City communities, (2) how they understood “community resilience,” and (3) how communities could improve preparedness for future disasters. Building on these discussions, in 2014, the Disaster Research Center and DOHMH work group organized 6 post–Superstorm Sandy focus group discussions among social services grantees in all 5 boroughs, to better understand their experiences during Superstorm Sandy and any subsequent preparedness and operational changes. Forty-three unique participants represented CBOs and faith-based organizations (FBOs) serving either communities affected by Superstorm Sandy or communities determined to be high in risk and vulnerable populations in a hazard vulnerability analysis conducted by the 2013 Office of Emergency Preparedness and Response. Informed by and using the COPEWELL conceptual model, the focus group discussions revolved around the roles and nature of CBO and FBO work during and after disasters; how CBOs and FBOs could deliver efficient, effective responses to such emergencies; and identifying needs related to organizational preparedness planning and partnerships.
Identification and Selection of Interventions to Strengthen Community Resilience
Informed by findings from the focus group discussions and indicator searches, as well as by COPEWELL concepts and computational outputs, the COPEWELL-NYC work group proposed several candidate interventions to strengthen community resilience to public health emergencies. The work group ultimately selected 2 interventions for further development in collaboration with community partners, based on a now-stronger understanding of factors influencing resilience, new recognition of related goals and existing alignments across agency programs, and awareness of how selected efforts could support broader citywide priorities.
Identifying Uses and Benefits of COPEWELL
COPEWELL team members from Johns Hopkins University and the University of Delaware collected information on COPEWELL’s designed and unanticipated utility through regular meetings with the DOHMH lead investigator and through a structured telephone interview with work group participants.
Outcomes
Field application of the COPEWELL model by the public health agency showed anticipated applications as well as unanticipated uses and benefits. These findings can—and now do—inform and guide new avenues for model implementation in communities.
Advance Agency and Partner Understanding of Community Resilience and Influencing Factors
COPEWELL helped DOHMH staff members and community partners better grasp the concept of community resilience and postevent functioning, helping them “get their minds around the[se] concept[s].” This shared understanding helped entities that had programmatically and operationally approached community-based efforts differently and in isolation to find areas of commonality and overlap. This understanding was especially true for the concept of social cohesion, which is shown to be associated with faster community recovery and better overall health. 7 COPEWELL enhanced an understanding of social cohesion and other factors that influence resilience, eventually informing the development of candidate interventions to enhance social cohesion.
Increase Awareness and Use of Available Local Data and Identify Gaps
The identification of local indicators to use in COPEWELL’s computational model raised awareness of locally available data, data limitations, and potential uses. The work group refined the initial set of potential indicators to 60 indicators aggregated at the level of United Hospital Fund areas. The Johns Hopkins University team generated New York City-specific maps of indicators, domain-level aggregates, and resilience, all with United Hospital Fund boundaries.
Recognition of data gaps generated novel ideas for identifying other proxy indicators for New York City communities. For example, data gaps in social cohesion led DOHMH staff members to advocate for new social cohesion–oriented questions in future New York City Community Health Surveys. Additional information was also necessary to account for structural differences, such as the geography, central function, proximity, and widespread use of the New York City transit system. Data gaps also generated interest in promoting sub-borough aggregation levels for use by all data collection sources.
Identify High-Risk or Target Areas for Intervention
Indicator- and domain-level COPEWELL maps helped identify communities at high risk during disasters in which candidate interventions had potential for the greatest effect (eg, communities with high rates of people with disabilities or older adults living alone, large immigrant populations, or low levels of social cohesion). For example, maps showed the South Bronx as an area with high rates of medically vulnerable, low-income, socially isolated residents. These vulnerabilities were coupled with environmental expertise recognizing that areas in the South Bronx are highly susceptible to heat-related health effects. Although most geographic areas have long been identified by DOHMH as vulnerable to a host of social, economic, and health-related disparities, the COPEWELL maps validated the need for more equitable preparation and more intensive response operations in locales with these disparities.
Spark Development of Resilience-Strengthening Interventions
The conceptual model not only helped stakeholders to visualize and understand connections between community functioning and resilience, but also to identify actions that could strengthen this functioning before, during, and after emergencies. Discussions helped identify, align, and leverage information and activities across programs in ways that could expand effectiveness of existing activities or reach new populations. For example, the COPEWELL model helped highlight the importance of and relationship between social cohesion and networks reflected in focus group findings. As a result, members of the interagency team helped further develop and implement an existing “Be a Buddy” proposal to link vulnerable people in the South Bronx with CBO staff members and peers before and during high-heat events. Indicator- and domain-level maps helped validate local observations and, given limited public health funding, guided support toward the identified geographic target areas.
Discussion about social cohesion as an influencer of community resilience and expanded partnerships across DOHMH offices and divisions also sparked plans for a second intervention, which leveraged public health experience with immigrant populations through work on Ebola, Legionnaires disease, and Zika with an existing Mental Health First Aid training initiative developed by the National Council for Behavioral Health. The initiative was offered through ThriveNYC, a mayoral initiative and interagency partnership led in large part by DOHMH’s Division of Mental Hygiene to promote mental health for all New Yorkers. COPEWELL-based discussions helped to link these interventions in the context of resilience and identified important immigrant populations that could benefit, specifically Liberian and Latino immigrants with limited access to mental health services.
Foster Integration and Alignment of Community-Based Efforts Among Partners
COPEWELL served as a strong engagement tool, enabling participants across DOHMH and in various New York City communities to conceptualize intersections between routine public health work and community resilience, leading to new partnerships and integrated interventions. COPEWELL fostered a partnership between the DOHMH Bureau of Environmental Surveillance and Policy and the Center for Health Equity’s Bronx Neighborhood Health Action Center on the aforementioned Be a Buddy initiative. Staff members reported that they expected this initiative to “foster greater community trust, provide a more detailed understanding of community conditions among CBOs and public health workers, and connect daily health functions with emergency response activities.”
Beyond agency and field partners, COPEWELL also helped communicate how the provision of Mental Health First Aid training aligned with and supported the broader goals of ThriveNYC. Framed in the broader context of resiliency, the Be a Buddy intervention received funding as part of New York City’s Cool Neighborhoods initiative, a comprehensive, multiagency effort to protect residents from current and future rising temperatures and reduce the effect of the urban heat island in vulnerable communities. 8
Lessons Learned
One of COPEWELL’s strongest practical uses derives from its conceptual model and the picture that represents that model (Figure). It evokes high explicit face validity during community- and agency-wide presentations that support various practical applications. These applications include providing a strong framework in which to discuss and understand community functioning and resilience, a partner engagement tool within and across organizations, a catalyst for generating ideas and relationships aimed at strengthening resilience, and (in conjunction with the computational model) a communications tool to help visualize the potential effects of proposed interventions. Of equal importance, COPEWELL helped DOHMH link efforts to advance community resilience with other priorities and citywide initiatives aimed at community development and preparedness. Such findings suggest the importance of fostering access to COPEWELL and its use by local communities.
This work also highlighted some of the challenges and uncovered opportunities in efforts to measure or predict resilience. Work to validate the computational model’s quantitative accuracy is needed for practitioners to use COPEWELL to computationally predict the resilience of jurisdictions and/or examine predicted quantitative effects of proposed interventions. At the time of this project, the computational model’s resilience output was primarily useful for demonstration purposes, showing the general effect of interventions on resilience. Even so, the indicator- and domain-level maps proved useful. The model provided a context and framework within which to identify, apply, and visualize locally available and relevant data and to identify gaps in data. In the context of the COPEWELL conceptual model’s strong capacity to spark cross-sector understanding and engagement of resilience, this case study triggered the concept of using the model for structured, rubric-based, community self-assessment where relevant data may not be available. 9 This work is currently underway and being explored in additional pilot communities.
Although this work represents a single case study, it identified multiple uses beyond the COPEWELL model’s initially envisioned one as a predictive tool by which to examine resilience. Its conceptual framework drove a deeper, more relevant understanding of resilience than had previously been the case within the public health agency and with partners. Additionally, use of the conceptual framework helped identify key geographic areas at risk, spurred efforts to build upon local metrics, and resulted in innovative interventions that integrated and aligned efforts among emergency preparedness, community development, and broader public health initiatives.
Footnotes
Acknowledgments
The authors thank Robert Burhans and Thomas Inglesby, MD, for their thoughtful comments on the article.
Authors’ note
Sarah Sisco’s present address is Office of Population Health, NYC Health + Hospitals, New York, NY, USA.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by funding from the Centers for Disease Control and Prevention (CDC; contract N-200-2014-60654, grant 5P01TP000288) and the Assistant Secretary for Preparedness and Response, US Department of Health and Human Services (HHS; grant HITEP 130007-01-00). The content of this article is solely the responsibility of the authors and does not necessarily represent the official views of CDC, HHS, the Office of the Assistant Secretary for Preparedness and Response, or the New York City Department of Health and Mental Hygiene.