
Abstract
Objectives
Hepatitis C virus (HCV) and HIV transmission in the United States may increase as a result of increasing rates of opioid use disorder (OUD) and associated injection drug use (IDU). Epidemiologic trends among American Indian/Alaska Native (AI/AN) persons are not well known.
Methods
We analyzed 2010-2014 Indian Health Service data on health care encounters to assess regional and temporal trends in IDU indicators among adults aged ≥18 years. IDU indicators included acute or chronic HCV infection (only among adults aged 18-35 years), arm cellulitis and abscess, OUD, and opioid-related overdose. We calculated rates per 10 000 AI/AN adults for each IDU indicator overall and stratified by sex, age group, and region and evaluated rate ratios and trends by using Poisson regression analysis.
Results
Rates of HCV infection among adults aged 18-35 increased 9.4% per year, and rates of OUD among all adults increased 13.3% per year from 2010 to 2014. The rate of HCV infection among young women was approximately 1.3 times that among young men. Rates of opioid-related overdose among adults aged <50 years were approximately 1.4 times the rates among adults aged ≥50 years. Among young adults with HCV infection, 25.6% had concurrent OUD. Among all adults with arm cellulitis and abscess, 5.6% had concurrent OUD.
Conclusions
Rates of HCV infection and OUD increased significantly in the AI/AN population. Strengthened public health efforts could ensure that AI/AN communities can address increasing needs for culturally appropriate interventions, including comprehensive syringe services programs, medication-assisted treatment, and opioid-related overdose prevention and can meet the growing need for treatment of HCV infection.
The risk for hepatitis C virus (HCV) and HIV infection in the United States has increased in parallel with increases in opioid use disorder (OUD) and injection drug use (IDU) in urban and rural areas. 1 -5 National hepatitis C surveillance data indicated a steeper increase in the number of acute cases of HCV infection among American Indian/Alaska Native (AI/AN) persons than among other racial/ethnic groups during 2001-2016 6 and that the number of opioid-related overdose deaths increased more among AI/AN persons than among other nonwhite groups. 7,8 However, compared with non-Hispanic white Appalachian communities with high numbers of cases of acute HCV infection and opioid-related overdose deaths, 3,9,10 AI/AN populations have received little public health attention. A landmark county-level vulnerability analysis of HIV and HCV infections among persons who inject drugs, conducted by Van Handel et al, showed vulnerability in 220 US counties, but few of these vulnerable counties had an AI/AN population of at least 3.0% (Figure 1). 9,11 An in-depth evaluation of IDU in AI/AN communities can inform infectious disease and opioid-related overdose prevention efforts and promote appropriate resource allocation to support interventions. 12
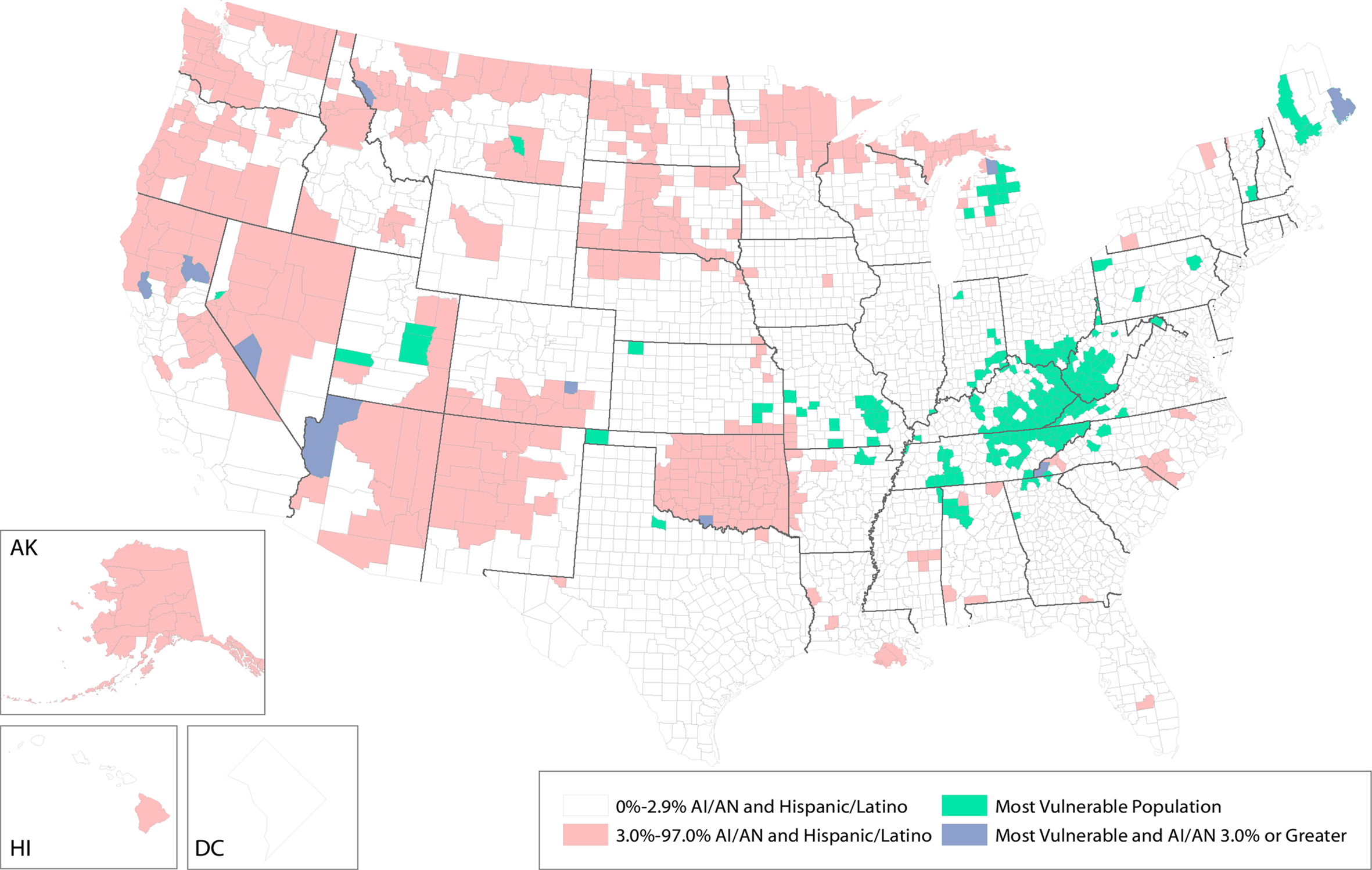
Representation of American Indian/Alaska Native (AI/AN) and Hispanic/Latino population, as a percentage of county population, by county, in 2010, and 220 counties deemed as most vulnerable to rapid dissemination of HIV or hepatitis C virus infection among persons who inject drugs in the United States, 2012-2013. Data on 220 most vulnerable counties from Van Handel et al. 9 Data on American Indian/Alaska Native population from the 2010 US Census. 11
No recognized International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) code for IDU exists. 13 Therefore, data on the risk of HCV and HIV transmission associated with IDU via administrative data must rely on proxy indicators, such as diagnoses known to be common among persons who inject drugs, from surveys, health care databases, and communities. 9 Collectively, high rates of these indicators in a geographic region may signal increased risk for IDU. We sought to assess temporal trends and regional differences in rates of HCV infection, arm cellulitis and abscess, OUD, and opioid-related overdose to help inform national or regional prevention programs for AI/AN persons at the highest risk for unsterile IDU-associated spread of blood-borne pathogens.
Methods
Data Source
We analyzed data from the Indian Health Service (IHS) administrative health care inpatient discharge and outpatient visit database. We accessed data through an existing Centers for Disease Control and Prevention–IHS data-use agreement, which permits geographic analyses of data at the regional and national level only. 5,14 The Indian health system supported by IHS serves IHS (federal), tribal, and urban (I/T/U) facilities and consists of 45 hospitals and more than 300 health centers in 37 US states, mainly primary care clinics in rural areas that are either federally or tribally operated 15 and contracted out-of-network health facilities, as needed. 15 Electronic health records at I/T/U facilities and some contracted care records are collected at the national level and maintained by the IHS National Patient Information Reporting System (NPIRS) using the National Data Warehouse. 16 NPIRS includes all inpatient discharge and outpatient visit records for services to patients eligible for IHS health care. We considered all AI/AN persons receiving care at I/T/U facilities or contracted care. NPIRS provides an annual denominator for the IHS user population, defined as the unduplicated count (by residence) of AI/AN registrants who have had an inpatient, ambulatory, or dental encounter with the Indian health system during the previous 3 years; these denominator data are provided only as aggregate counts by location, age, and sex.
Study Design
We analyzed NPIRS data from 2010 through 2014 and limited our analyses to data on adults aged ≥18 years. For study outcomes, we counted each diagnosis at its first documented instance during the 2010-2014 analysis period, to avoid overcounting diagnoses for chronic diseases, such as HCV infection, for which a diagnosis may have been recorded on multiple occasions. We defined HCV infection, arm cellulitis and abscess, OUD, and opioid-related overdose as indicators of IDU on the basis of the associations of these factors with IDU in previous studies. 3,10,17 -19 These indicators of IDU, the outcomes in our analyses, were defined by using ICD-9-CM codes and included the following: HCV infection (070.41, 070.44, 070.51, 070.54, 070.70, 070.71), OUD (304.00-304.03, 304.70-304.73, 305.50-305.53), opioid-related overdose (poisoning) (965.00-965.02, 965.09, 970.1, E850.0-E850.2), and arm cellulitis and abscess (682.3). 13
We limited analyses of HCV infection to adults aged 18-35 to exclude older persons whose chronic HCV infection might be unrelated to recent IDU. Analyses of OUD, arm cellulitis and abscess, and opioid-related overdose included all adults aged ≥18 years. OUD included opioid-type dependence, combinations of opioid-type drug with any other drug, and opioid use. Opioid-related overdose was defined as poisoning by opium, methadone, other opiates and related narcotics, heroin, or opiate antagonists. We also included accidental poisoning by heroin, methadone, and other opiates and related narcotics. Although drugs are injected at many anatomical locations, we chose the code for arm cellulitis and abscess because skin and soft-tissue infections of the arm are a common complication of unsterile injection, whereas skin and soft-tissue infections of the lower extremities are a common complication of diabetes and peripheral vascular disease. 14,20,21 We excluded adults with arm cellulitis and abscess from the numerator if they had an ICD-9-CM code indicating diabetes diagnosis (249, 250, 357.2, 362.0, 366.41, 648.0, 648.8, V45.85, V53.91, V65.46) in NPIRS on or before (since 2001) their first encounter for arm cellulitis or abscess. We considered several additional indicators of IDU, including endocarditis and osteomyelitis, but we eventually excluded them because of an insufficient number of these diagnoses to support analyses.
Statistical Analysis
For each IDU indicator, we counted the number of adults with that diagnosis during 2010-2014, overall and stratified by sex, age group, and region; NPIRS contains a unique patient registration identifier that allows the de-duplication of data on persons with >1 health care encounter with the same diagnoses, so that a person was counted only once in the numerator (first recorded diagnosis) during the study period. We calculated denominators by summing the NPIRS annual denominators during the study period. We determined sex, age group, and region from a person’s first visit during the study period for each IDU indicator. We also counted the number of persons with concurrent IDU indicators (ie, when a person met requirements for ≥2 IDU indicators during the study period). We categorized geographic regions as described elsewhere. 5,22 We calculated rates of each IDU indicator for 2010-2014 combined per 10 000 AI/AN adults to compare the burden between strata by using IDU indicator counts and the corresponding aggregation of NPIRS annual denominators; we used Poisson regression analysis to calculate rate ratios (RRs) and 95% confidence intervals (CIs).
We performed a trend analysis to examine changes over time in the number of adults with IDU indicators who used the IHS system. We calculated annual rates per 10 000 AI/AN adults by using the number of adults in each calendar year with a diagnosis for each IDU indicator as the numerator and the corresponding NPIRS annual denominators. We calculated unadjusted average annual percentage change and used Poisson regression analysis to evaluate trends over time. For all analyses, we used SAS version 9.4 23 and set significance at P < .05.
The project relied on preexisting de-identified data and was approved by the Centers for Disease Control and Prevention and IHS institutional review board processes and federal regulations for the protection of human subjects.
Results
Demographic and Regional Comparisons
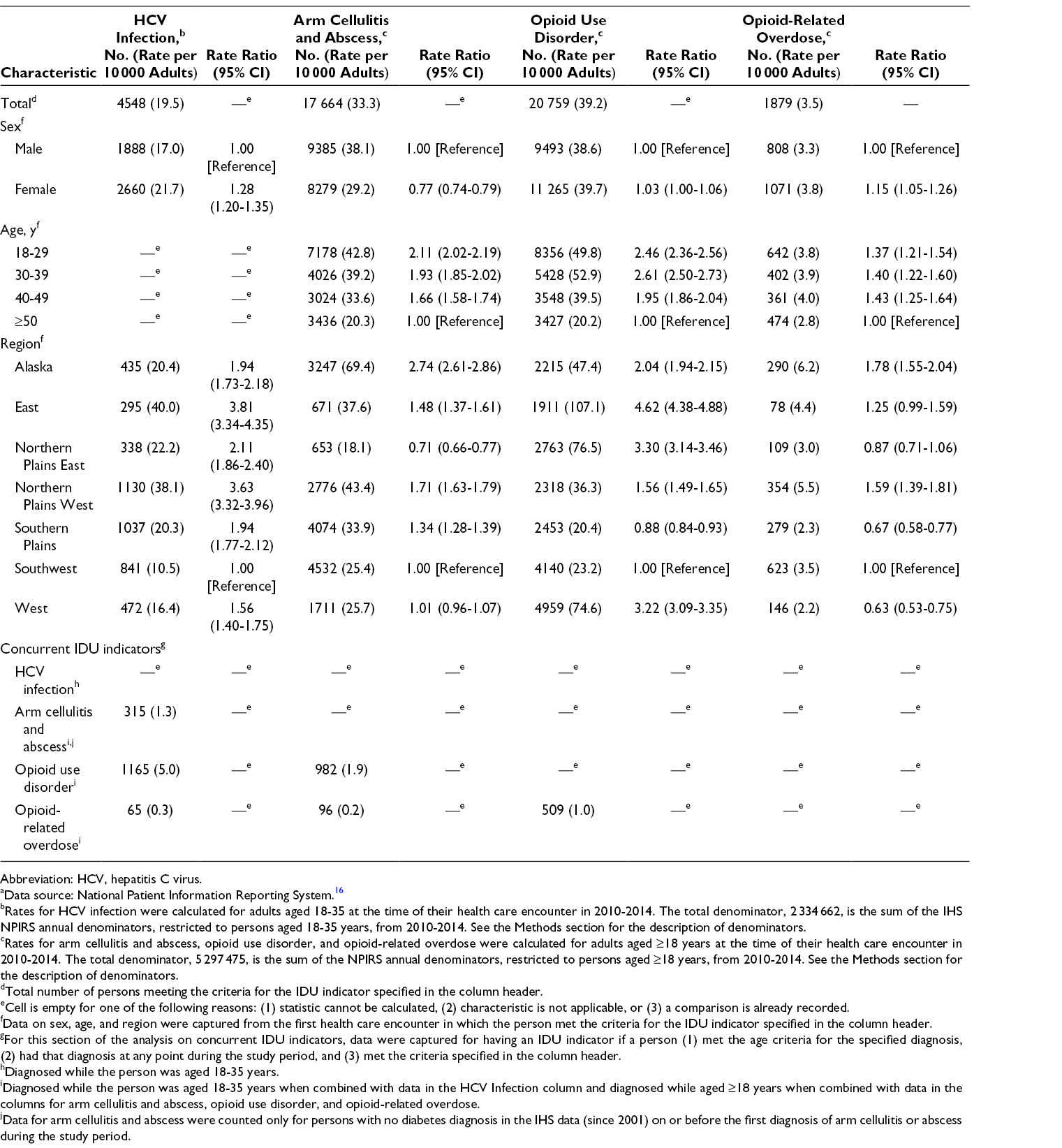
The rate of reported HCV infections across all regions was 19.5 per 10 000 AI/AN adults aged 18-35 (n = 4548; Table 1). Among AI/AN adults aged 18-35, the rate of HCV infection was higher among women than men (RR = 1.28). By region, the rate of HCV infection in the East was 3.81 times the rate in the Southwest, which had the lowest rate, and the rate of HCV infection in the Northern Plains West was 3.63 times the rate in the Southwest. The overall rate of OUD was 39.2 per 10 000 AI/AN adults aged ≥18 (n = 20 759). Compared with rates of OUD in the Southwest, rates of OUD were higher in the East (RR = 4.62), Northern Plains East (RR = 3.30), West (RR = 3.22), Alaska (RR = 2.04), and Northern Plains West (RR = 1.56) and lower in the Southern Plains (RR = 0.88). The overall rate of arm cellulitis and abscess was 33.3 per 10 000 AI/AN adults aged ≥18 (n = 17 664). The overall rate of opioid-related overdose was 3.5 per 10 000 AI/AN adults aged ≥18 (n = 1879). Opioid-related overdose was slightly more common among women than among men, and the relative rates of opioid-related overdose in all groups aged <50 were similarly higher, at approximately 1.4 times the rate in groups aged ≥50.
Number (rate per 10 000 adults) of American Indian/Alaska Native adults aged ≥18 years with a health care encounter who had an injection drug use (IDU) indicator diagnosis, National Patient Information Reporting System (NPIRS), Indian Health Service (IHS), 2010-2014 a
Abbreviation: HCV, hepatitis C virus.
aData source: National Patient Information Reporting System. 16
bRates for HCV infection were calculated for adults aged 18-35 at the time of their health care encounter in 2010-2014. The total denominator, 2 334 662, is the sum of the IHS NPIRS annual denominators, restricted to persons aged 18-35 years, from 2010-2014. See the Methods section for the description of denominators.
cRates for arm cellulitis and abscess, opioid use disorder, and opioid-related overdose were calculated for adults aged ≥18 years at the time of their health care encounter in 2010-2014. The total denominator, 5 297 475, is the sum of the NPIRS annual denominators, restricted to persons aged ≥18 years, from 2010-2014. See the Methods section for the description of denominators.
dTotal number of persons meeting the criteria for the IDU indicator specified in the column header.
eCell is empty for one of the following reasons: (1) statistic cannot be calculated, (2) characteristic is not applicable, or (3) a comparison is already recorded.
fData on sex, age, and region were captured from the first health care encounter in which the person met the criteria for the IDU indicator specified in the column header.
gFor this section of the analysis on concurrent IDU indicators, data were captured for having an IDU indicator if a person (1) met the age criteria for the specified diagnosis, (2) had that diagnosis at any point during the study period, and (3) met the criteria specified in the column header.
hDiagnosed while the person was aged 18-35 years.
iDiagnosed while the person was aged 18-35 years when combined with data in the HCV Infection column and diagnosed while aged ≥18 years when combined with data in the columns for arm cellulitis and abscess, opioid use disorder, and opioid-related overdose.
jData for arm cellulitis and abscess were counted only for persons with no diabetes diagnosis in the IHS data (since 2001) on or before the first diagnosis of arm cellulitis or abscess during the study period.
Concurrent Indicators
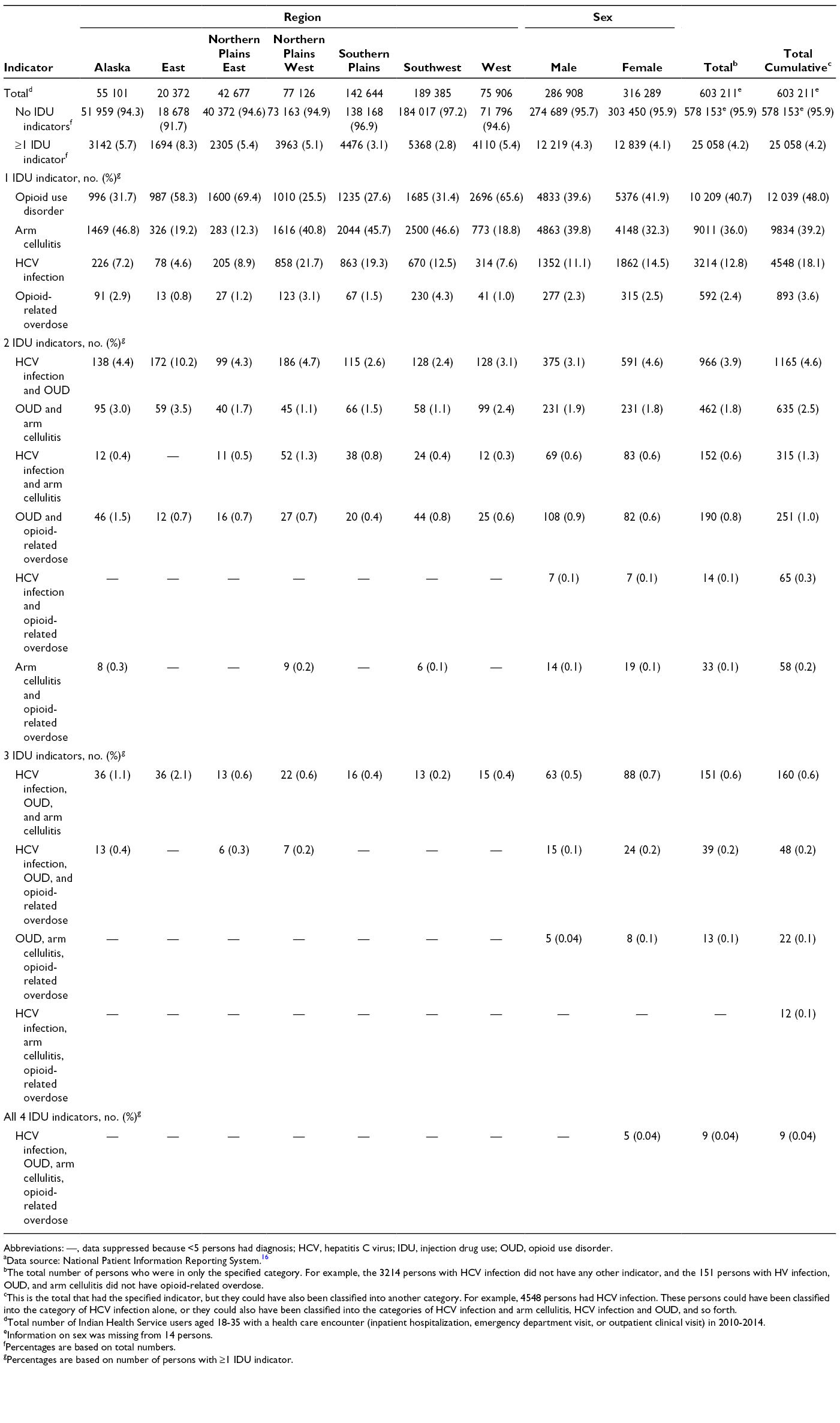
Among the 4548 AI/AN adults aged 18-35 with a diagnosis of HCV infection, 25.6% (n = 1165) had a concurrent diagnosis of OUD and 6.9% (n = 315) had a concurrent diagnosis of arm cellulitis and abscess (Table 1). Among the 17 664 AI/AN adults aged ≥18 with a diagnosis of arm cellulitis and abscess, 5.6% (n = 982) had a concurrent diagnosis of OUD. By region, the largest percentage of adults aged 18-35 with ≥1 IDU indicator was in the East (8.3%; 1694 of 20 372); a greater percentage of men (4.3%; 12 219 of 286 908) than women (4.1%; 12 839 of 316 289) had ≥1 IDU indicator (Table 2).
Percentage of American Indian/Alaska Native adults aged 18-35 years having each combination of injection drug use indicators, overall and by region and sex, Indian Health Service, 2010-2014 a
Abbreviations: —, data suppressed because <5 persons had diagnosis; HCV, hepatitis C virus; IDU, injection drug use; OUD, opioid use disorder.
aData source: National Patient Information Reporting System. 16
bThe total number of persons who were in only the specified category. For example, the 3214 persons with HCV infection did not have any other indicator, and the 151 persons with HV infection, OUD, and arm cellulitis did not have opioid-related overdose.
cThis is the total that had the specified indicator, but they could have also been classified into another category. For example, 4548 persons had HCV infection. These persons could have been classified into the category of HCV infection alone, or they could also have been classified into the categories of HCV infection and arm cellulitis, HCV infection and OUD, and so forth.
dTotal number of Indian Health Service users aged 18-35 with a health care encounter (inpatient hospitalization, emergency department visit, or outpatient clinical visit) in 2010-2014.
eInformation on sex was missing from 14 persons.
fPercentages are based on total numbers.
gPercentages are based on number of persons with ≥1 IDU indicator.
Trend Analysis
The annual rate of diagnoses of HCV infection per 10 000 AI/AN adults aged 18-35 increased significantly from 25.5 in 2010 to 35.1 in 2014, an average 9.4% increase per year (P < .001; Figure 2). The annual rate of OUD diagnoses per 10 000 AI/AN adults aged ≥18 increased significantly from 47.1 in 2010 to 72.2 in 2014; an average 13.3% increase per year (P < .001). The annual rate of arm cellulitis and abscess diagnosis per 10 000 AI/AN adults aged ≥18 decreased significantly from 38.4 in 2010 to 32.0 in 2014; an average 4.2% decrease per year (P < .001). We found no significant change in the annual rate of opioid-related overdose during the study period.
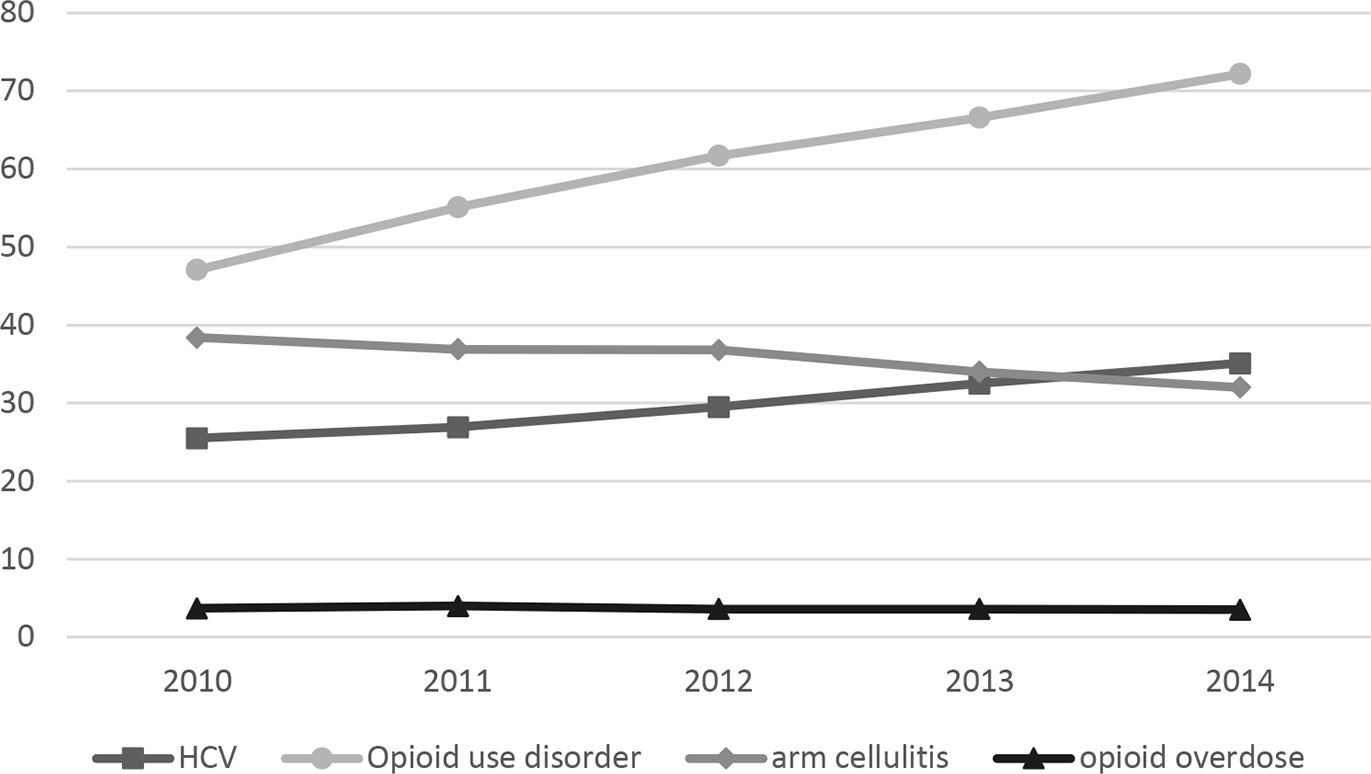
Overall national annual rates (per 10 000 adults) of diagnoses among American Indian/Alaska Native persons for hepatitis C virus (HCV) infection, opioid use disorder, arm cellulitis and abscess, and opioid-related overdose, Indian Health Service, 2010-2014. Rates of diagnoses represent 1 health care encounter per person per year. Data for HCV infections are for adults aged 18-35; all other data are for adults aged ≥18. Arm cellulitis was counted only among adults with no diabetes on or before the health care encounter for arm cellulitis visit (since 2001). Data source: National Patient Information Reporting System. 16
Discussion
In this analysis of a large database of outpatient and inpatient health care encounters among adult AI/AN patients at I/T/U facilities, the rates of HCV infection and OUD increased during 2010-2014. Our findings on HCV infection, based on ICD-9-CM codes, show a rate of 19.5 diagnoses per 10 000 adults for 2010-2014, in line with other studies reporting higher rates of HCV infection in the AI/AN population than in other racial/ethnic groups and an increase in rates of hospitalizations related to HCV infections among AI/AN persons over time. 6,22 Resources for treating and curing HCV infection in I/T/U facilities are inadequate 12 ; therefore, this vulnerable population is at an even higher risk than other racial/ethnic populations of further rapid HCV transmission and hepatitis C sequelae, including end-stage liver disease, cirrhosis, hepatic cancer, and death. 24 The rate of concurrent diagnoses of HCV infection and OUD in our study was 5.0 per 10 000 AI/AN adults, consistent with the documented correlation between HCV infection and IDU in the overall US population. 10 Finding novel methods for gauging IDU levels in AI/AN communities is particularly important to ensure sufficient access to culturally appropriate interventions, syringe services programs, medication-assisted treatment, and opioid-related overdose prevention (eg, access to naloxone). Syringe services programs and medication-assisted treatment are effective interventions to prevent HCV transmission, but access to these programs is limited for AI/AN persons. 25,26 Although some tribes have already implemented syringe services programs, our analysis provides impetus and a framework for additional tribes and others, such as tribal epidemiology centers and tribal serving organizations, to conduct their own data analysis and needs assessment, which may point to a need for establishing or expanding syringe services programs for AI/AN persons. 27
IHS has implemented opioid-prescribing guidelines 28 consistent with the CDC Guideline for Prescribing Opioids for Chronic Pain 29 and has expanded access to medication-assisted treatment and naloxone. 30 Our regional analyses can inform the geographic focus of resources, including access to medication-assisted treatment and naloxone. 16,28,30 Methamphetamine use, including injection, is common in many AI/AN communities 31 and might heighten the risk for introducing HIV into networks of persons who inject drugs if bridging or mixing occurs with the networks of men who have sex with men who use methamphetamines; methamphetamine is also increasingly combined with opioid injection. 32 -34 Finally, the increase over time in rates of HCV infection and OUD suggests a need to screen and provide treatment for injection-related blood-borne pathogens such as HCV and HIV. 12
Few studies have documented OUD among AI/AN persons; among 400 tribal members interviewed in 2009 on a rural Midwestern reservation, nearly 20% reported nonmedical use of OxyContin in the previous year. 35 Our study found that OUD was common, with increasing rates over time and substantial regional differences. However, trends in opioid-related overdose were stable, which was unexpected given that national data for AI/AN persons show increasing rates of opioid-related overdose. 36,37 Our discrepant findings may be due to inadequate capture of data on fatal overdose events in the health records database for persons outside health care settings and misclassification of OUD as other injury events in medical records. 38 In addition, synthetic opioids such as fentanyl are associated with the largest increase in opioid-related overdose deaths in the US general population. 39 The use of synthetic opioids is also affecting AI/AN persons, 40,41 but the availability of these drugs may have varied by community or region and been potentially lower in AI/AN communities than in the US general population during our study period.
Unlike rates of HCV infection and OUD, rates of arm cellulitis and abscess decreased during 2010-2014. Historical rates of hospitalization for skin and soft-tissue infection are higher among AI/AN persons than among other racial/ethnic groups, and the decrease in rates of arm cellulitis and abscess found in our study could be related to non-IDU factors, such as interventions that address the high rates of skin and soft-tissue infection. 42 Examining rates of arm cellulitis and abscess in the context of a concurrent IDU-related diagnosis of HCV infection or OUD is expected to increase the specificity of arm cellulitis and abscess as an indicator of IDU. Other studies relied on a single diagnosis, such as acute HCV infection or endocarditis, as a starting point for approximating county levels of IDU and then used multiple indicators. 9,43 Acute HCV infection is not a reliable measure for study in NPIRS because it is often asymptomatic and not recorded; other frequently used indicators, such as endocarditis, are not commonly managed in the IHS system.
Our assessment of the rates of HCV infection and OUD among AI/AN persons, whose tribal areas are not defined by US counties, suggests that the relatively high burden of these conditions among AI/AN persons, compared with other racial/ethnic populations, may not have been apparent in national county-level analyses that used acute HCV infection as an indicator across racial/ethnic populations. 9 The landmark county-level vulnerability study by Van Handel et al, which relied on acute HCV infection as an indicator, identified 220 US counties at risk for rapid spread of HIV and HCV infection via IDU and brought attention to areas that had few existing public health resources to spur mobilization of HIV and HCV infection prevention efforts. 9 Although the vulnerability analysis by Van Handel et al differed substantially from our study in objectives and methodology, some of the outcomes in our study are consistent with those in the vulnerability analysis, and we expected them. However, our study resulted in several unexpected outcomes; we identified regions not previously considered vulnerable, at least not for AI/AN populations. For example, the burden of HCV infection and OUD in the East in our study was consistent with the burden described by Van Handel et al. However, in our study, by region, Northern Plains West had the second highest rate of HCV infection and Northern Plains East had the second highest rate of OUD. On the basis of the vulnerability analysis, we did not expect either of these outcomes. Rates of OUD were also unexpectedly high in the West. Our findings add to the national data on IDU risk, illustrate the value of exploring a range of approaches and data sources, and provide evidence to support the need for broader distribution of opioid-related prevention and treatment resources beyond the most vulnerable counties previously identified. 9,44
The rise of HCV infection and OUD in AI/AN communities is deeply rooted in many social determinants of health that may manifest themselves in other substance use disorders, such as alcohol and methamphetamine use. Historical trauma is a well-documented factor associated with substance use disorders among many AI/AN persons who are raised in intergenerational traumas, such as forced removals like the Trail of Tears and mandatory boarding school attendance. 45 Resilience in the face of these traumas is an important strength in AI/AN communities and can help tribes identify culturally appropriate solutions unique to each tribe’s needs. For example, OUD treatments might need to be adapted to preserve unique cultural holistic and traditional healing practices. In exploring the cultural and logistic considerations for implementing medication-assisted treatment in tribal communities, Venner et al observed that using medication (eg, buprenorphine/naloxone) for treatment conflicted with some traditional healing practices that require a person not to take medications. This conflict has considerable implications for the delivery of medication-assisted treatment in AI/AN communities. 4
Limitations
Our study had several limitations. First, we did not include all infectious disease complications of IDU in our analysis. We did not consider hepatitis B or HIV infections because the prevalence of HCV infection is higher than the prevalence of hepatitis B or HIV infection in persons who inject drugs. 46 -48 We excluded adults aged >35 with HCV infection to limit the influence of chronic HCV infection among baby boomers (born 1945-1965) who are screened according to the Centers for Disease Control and Prevention recommendations. 49,50 Second, our data do not represent all AI/AN persons living in the United States, so our results cannot be generalized outside our study populations. Not all persons who identify as AI/AN use IHS-funded health care; 5.2 million adults and children in the United States self-identified as AI/AN in the 2010 US Census, 51 but only 1.2 million AI/AN adults were represented in our NPIRS analysis (which includes only members of the 573 federally recognized tribes who use IHS-provided care). Consequently, AI/AN adults who did not have a health encounter with the Indian health system in the past 3 years were not included in our analysis, and data on any health care encounter or diagnosis made outside Indian health I/T/U facilities or contracted care were not captured. Finally, restrictions on geographic analysis of IHS data required aggregating our analytic findings into large regions with sociodemographically and culturally diverse characteristics. Regional results must be interpreted cautiously to avoid generalizations about persons living in these large and diverse regions. Despite these limitations, our analysis adds important information about the relative burden of and increasing trends in HCV infection and OUD among the population of AI/AN persons served by I/T/U facilities and should be considered in public health planning and resource allocation.
Conclusion
Each tribal community in the United States has unique characteristics and will determine its own approach to addressing IDU among its members. Interested tribes could initiate exploration of tribe-specific data that are researched, analyzed, and disseminated internally, so that they can define their own data and program needs. However, our data offer compelling evidence for tribes already seeing anecdotal increases in IDU and, along with national data, could be used to support culturally appropriate interventions such as comprehensive syringe services programs, access to medication-assisted treatment, and opioid-related overdose prevention as well as to bolster treatment capacity for the rising number of IHS patients infected with HCV. Our analysis showed concerning trends in HCV infection and OUD among AI/AN persons and identified regional hotspots in which few counties were identified as vulnerable in a national vulnerability assessment. 9 These data reinforce the need for continued public health action to avert further IDU-related consequences and can help tribes allocate resources and plan policies to improve opioid-related overdose prevention and harm reduction in AI/AN communities.
Footnotes
Acknowledgments
We appreciate thoughtful insights from Vickie L. Bradley, Secretary, Public Health and Human Resources Eastern Band of Cherokee Indians, and Ginger Southard, Program Manager, Syringe Services Eastern Band of Cherokee Indians, who informed interpretations in this article. We also thank Melissa M. Smith, in the Geospatial Research, Analysis and Services Program at the Centers for Disease Control and Prevention, for assistance in preparation of the map.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors declared no financial support with respect to the research, authorship, and/or publication of this article.