
Abstract

Keywords
Examination of complex public health policy issues can benefit from a mixed methods approach led by multidisciplinary teams. 1,2 Evolving problems confronted by law and public health inherently demand dynamic perspectives from diverse fields. However, in practice, professionals often succumb to established ways of approaching an issue within their own disciplines and areas of expertise. 3 The mixed methods approach uses quantitative and qualitative research methods to provide a more comprehensive understanding of a research question than any single method could provide. A key advantage of using a mixed methods approach is that the concurrent, coordinated design can offset the weaknesses of either individual approach. Although quantitative research may be inadequate to understand the context in which a phenomenon occurs, qualitative research alone may invoke subjectivity and may not yield generalizable findings. Therefore, the scientific study of the effects of public health law necessitates a multidisciplinary approach. 4 A multidisciplinary approach draws on the diverse subject matter expertise, training, and skills of partners from various fields.
Policy research often examines associations between policies and health outcomes. In some instances, noting the presence or absence of a policy and its direct effect on health may be straightforward. Implementation of laws that require all motorcyclists to wear helmets has been shown to decrease the number of injuries and deaths among motorcyclists and is a classic illustration of this principle in public health law curricula and literature. 5,6 However, many policies have a pervasive yet indirect relationship to health outcomes. Although assessments of laws, regulations, and other policies at the state and county level may provide contextual information to help develop or target interventions to address health disparities, this approach alone may be insufficient to assess complex associations between policy and public health outcomes, including social determinants of health (the “conditions in the environments in which people are born, live, learn, work, play, worship, and age that affect a wide range of health, functioning, and quality-of-life outcomes and risks”). 7 For example, high rates of incarceration can affect sexual mixing patterns (ie, how persons are connected in sexual networks) and contribute to increased STD rates in affected communities. 8 Furthermore, policies may foster conditions that influence health; therefore, policy often operates as a social determinant of health and can shape other social determinants of health. 9,10
Numerous studies document the influence of social determinants of health on STD morbidity, as discussed in a 2008 review. 11 Social determinants of health that can affect STD morbidity include racial/ethnic residential segregation, access to affordable and relevant health care, poverty, and discrimination. 11 A 2016 review of policy research on STDs identified policies that have the potential to either positively or negatively affect STD prevention by modifying social determinants (especially health care–focused policies) but urged additional research to identify policy interventions to address STDs. 12 A scan of CDC-authored articles on legal epidemiology, the scientific study of law as a factor in the cause, distribution, and prevention of disease (also known as public health law research, which includes policy surveillance research), identified few legally trained authors on teams conducting legal epidemiology research “despite the interdisciplinary quality of CDC’s staff members and work.” 13 The review did not identify any policy studies in STD prevention that used mixed methods.
To address these gaps in policy research aimed at STD prevention, we applied mixed methods approaches in 2 studies of policies that may affect 2 populations at high risk for STDs: (1) persons involved in the criminal justice system and (2) lesbian, gay, and bisexual (LGB) populations. 14 -16 Our multidisciplinary team comprised public health attorneys trained in established policy surveillance research methods 3,4 and public health scientists with broad subject matter expertise from the public (CDC Division of STD Prevention) and private (Research & Evaluation Group at Public Health Management Corporation, a nonprofit regional public health institute) sectors. As appropriate, we engaged content experts in related fields to study content to inform our research focus and enhance our analysis. To facilitate collaboration in our studies, we met biweekly via conference call and convened in person for intensive meetings to finalize the scope of each study after preliminary research and consultation with subject matter experts in related fields. We provide our reflections on 2 mixed methods studies conducted by our multidisciplinary, public–private sector team. We highlight lessons learned and implications for other stakeholders addressing complex concepts such as health equity.
Study 1: Criminal Justice–Involved Populations
Involvement with the criminal justice system and drug use are associated with health disparities, including an increased risk for STDs. 17,18 During 2015-2016, we examined justice-related policies in all states by using multidisciplinary, mixed methods research to conduct (1) a policy assessment of state laws related to justice-involved populations 19 and (2) a qualitative sub-study in 7 states of county jails’ STD policies to address STD prevention–related gaps. Jails are where persons charged with misdemeanor drug-related offenses are typically confined.
The purpose of the policy assessment, which we limited to state statutes and regulations, was to examine state policies associated with the possession of several drugs that have been associated with STDs. The assessment began with a review of relevant scholarly literature on the relationships among policy, social determinants of health, STD risk, and STD disparities. We used results of the literature review, in consultation with subject matter experts in related fields, to identify areas of policy hypothesized to relate to social determinants, STD risk, and STD disparities for criminal justice–involved populations. The attorneys on our team conducted preliminary statutory and regulatory research of policy areas in a subset of states, representing varied geography and population size, to hone research questions and identify variables. We focused on the following variables, in part because of their hypothesized relationship to increased likelihood of interaction with the criminal justice system and socioeconomic status: (1) drug possession sentences for persons convicted of possessing marijuana, crack cocaine, and methamphetamine and (2) consequences of drug-related convictions (eg, ineligibility for public programs and occupational licenses, employer inquiries about criminal history, implications for public housing eligibility). 19 We collaboratively developed a standardized protocol for collecting and coding policies. The attorneys, using policy surveillance methods, 3,4 applied the protocol to every state and the District of Columbia. Our policy assessment found substantial barriers for justice-involved persons accessing health-related public benefits after incarceration, including comprehensive prohibitions from select benefits programs based on criminal history. 19
We also conducted a qualitative sub-study to explore research questions in the context of STD prevention that could not be addressed within the scope of the policy assessment, because these topics are not normally found in statutes and regulations. Interview guides focused on how STD testing, linkage- and access-to-care policies in jails, and collateral consequences of conviction (eg, limitations for employment, housing, and public benefits) 20 for jail populations as they reenter their communities may affect STD risk among criminal justice–involved populations. 21 Persons who are incarcerated in jail receive health screenings and care, including STD testing, STD treatment, and linkage to care; however, evidence indicates that many county jails do not have or do not enforce routine testing or linkage-to-care protocols. 22 Our team collaborated on study design, scope, research questions, and methods. A public health researcher with qualitative research experience completed 13 interviews with jail staff members and service providers in jails in 7 counties across the United States with high STD morbidity during 2015-2016. 21 Interviewees were either currently working or had recently worked with the county correctional system in the areas of health services, infectious disease, behavioral health, or social services and were knowledgeable about STD-related health care services. Interviewees came from medical, nursing, social work, substance use, and public health backgrounds and were employed by the county correctional departments, commercial health systems that directly contracted with county correctional departments, city or county health departments, or public hospital systems responsible for providing health care to county residents in and out of correctional facilities. Qualitative findings highlighted that some incarcerated persons may be accessing health care, including health screenings and linkage to care, upon reentry, for possibly the first time. However, others may not have access to STD testing and treatment while incarcerated.
Study 2: LGB Populations
LGB persons have various health disparities, 14,16 and laws in a jurisdiction may serve as a proxy for the social environment in that jurisdiction. 23 We conducted a study of state- and county-level policies focusing on LGB populations in 2014. Using a multidisciplinary approach, we developed a policy data set to facilitate analysis of associations between policies focused on protections for LGB populations and health outcomes for LGB populations, particularly for STDs. 23 Using policy surveillance methods, 3,4 we identified and categorized protections for LGB populations across several legal domains: employment, same-sex relationship recognition (eg, marriage, civil unions), public accommodations, housing, and criminal justice. 23 Our policy assessment found substantial variability in state laws addressing formal protections for LGB persons among public and private employers, in housing practices, and for public accommodations by US census region; the largest percentage of states with protections was typically in the Northeast, followed by the West. 23 However, we found fewer local laws that focused on protections for LGB populations.
Using policy data from counties in the top 30 metropolitan statistical areas in the United States by population, 23 our team’s research scientists calculated quantitative indices, overall and for each legal domain, to develop proxy measures for the LGB-related social environment. We included numerous measures in our data set, because the development of composite measures may be more feasible to incorporate in data analyses. We assigned each domain a composite LGB protection score (out of 100) for each county based on (1) presence of legal protections in each domain, (2) state and/or county policy in each jurisdiction, and (3) weights based on empirical evidence of the association between each legal domain and study aims. For example, legal domains found in peer-reviewed literature to be most strongly linked to HIV and STD risk among LGB populations, including relationship recognition 24 -26 and employment, 26,27 were the most heavily weighted. Finally, we tested index reliability using Cronbach α. 28 Our composite scores had acceptable reliability (Cronbach α ranged from 0.68 to 0.80) and showed variation across counties. Of 100, the overall score for county-level LGB protections was a median of 21 (interquartile range = 4, 65) and a mean of 35.7 (standard deviation = 32.4). Through our use of weights, the index linked the legal findings to STD and HIV prevention, risk, and disparities that were previously identified in the scientific literature.
Lessons Learned
Our studies demonstrate how using multidisciplinary and/or mixed methods approaches can benefit projects and research questions related to social determinants of health in STD prevention, which can likely extend to related fields. Multidisciplinary, mixed methods research enhances policy research by providing important contextual information related to the implementation, perceptions, and experiences related to policies that may be indirectly associated with STDs in some populations that have health disparities, such as criminal justice–involved and LGB populations. Using policy surveillance methods to document misdemeanor drug-related sentencing laws in conjunction with qualitative data collection in Study 1 provided information on sentencing laws that can remove persons from their community (which can cause imbalanced sex ratios and enhanced STD transmission) and opportunities, or missed opportunities, for intervention and linkage to care in jails. These findings can be used to inform policy development and health outcomes–oriented enforcement. Using the results of the policy assessment of LGB protections across multiple domains to develop county-level indices in Study 2 provided an opportunity to analyze the relationship between comprehensive anti-discrimination policy and health outcomes, including STD risk. 29 The indices allowed us to condense numerous policies into variables useful for further analysis. Our partnership between the public and private sectors leveraged the unique expertise, networks, capacity, and resources of each entity to enhance the design, administration, and analysis of both studies.
Multidisciplinary teams provided a mix of unique skill sets that enriched each component of our studies (Table). Researchers involved with these studies had the expertise to develop new measures (indices) and conduct qualitative research, and attorneys helped scientists to recognize gaps in policies, understand the relationship between state and local policies, and identify qualitative interview participants. Content experts in related fields provided specialized expertise to hone research questions, instruments, and analysis (Table). Scientists are well versed in literature that is relevant to their research, and attorneys have the skills and understanding to find and interpret relevant policies; this combination improved each component of our studies. Using multidisciplinary and mixed methods approaches also helped us to address gaps in each of our study components and, in some instances, helped us to assess the potential effect of policies on rates of STDs and STD disparities more directly. For example, in Study 1, the policy assessment yielded a large amount of useful information about consequences of drug possession, including loss of eligibility for essential public services. The qualitative study filled in gaps about health care access and STD testing in jails, which is information that is not in statutes and regulations and is more directly tied to STD rates. In Study 2, our policy assessment provided us with a rich data set on state and local LGB policies, and the development of indices made the data more useful for others to directly examine the relationship between the policies and outcomes, such as STD rates.
Components of studies on the effect of policies on 2 populations at high risk for sexually transmitted diseases and corresponding activities conducted by multidisciplinary, public–private sector team members a
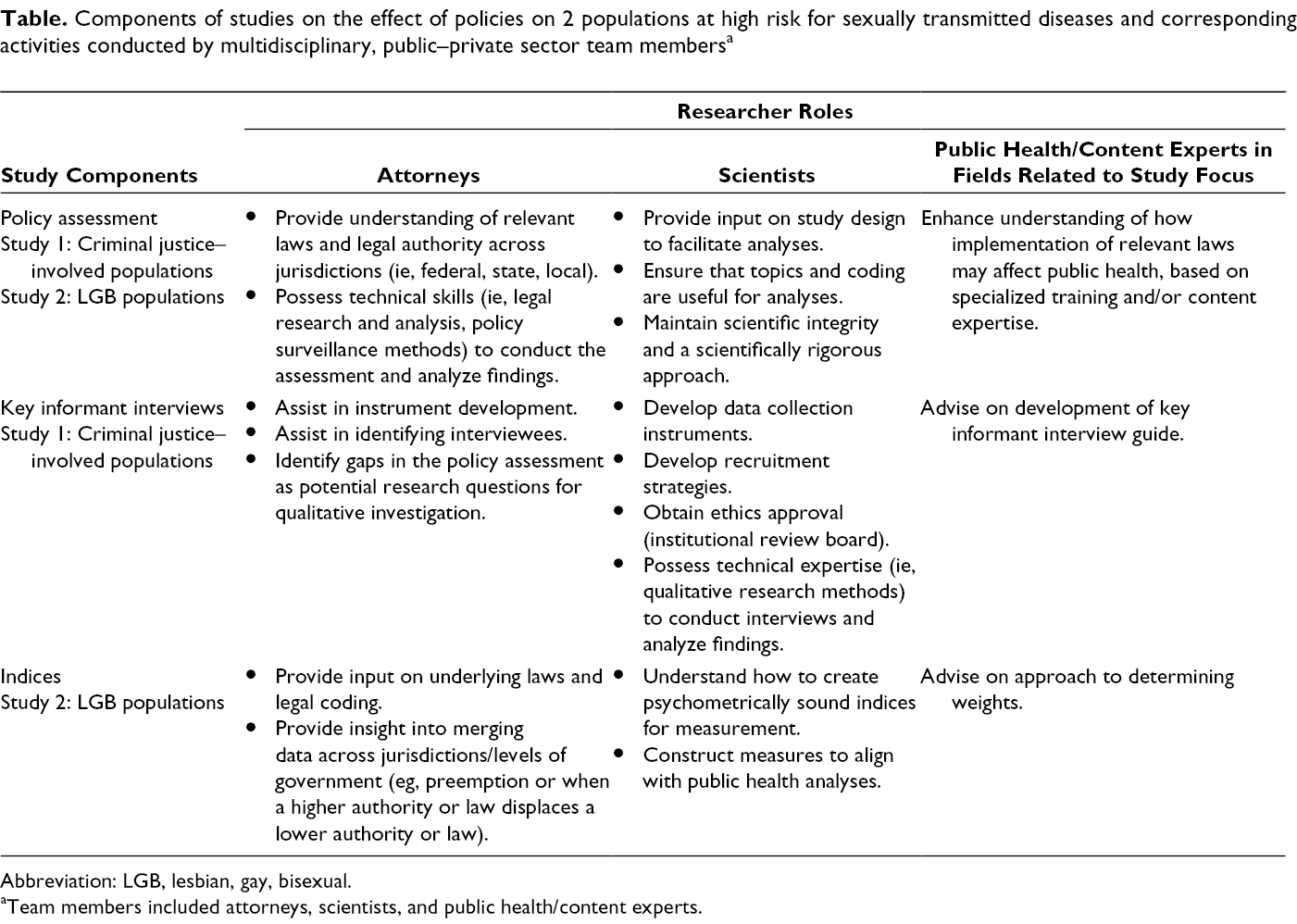
Abbreviation: LGB, lesbian, gay, bisexual.
aTeam members included attorneys, scientists, and public health/content experts.
Preliminary research in our studies, conducted by attorneys, confirmed the breadth and specificity of policies that influence known social determinants of health for populations at increased risk for STDs. Furthermore, the legal frameworks underlying public agency structures, such as public benefits administration, are often complicated and expansive. Our team leveraged our sexual health subject matter expertise, a strong grasp of broad public health principles, adept legal research and analysis, and diverse research methodologies to assess the complex relationships among relevant policies, social determinants of health, and STD prevention. The measures we collaboratively identified and coded in the policy assessments, and used to assign weights for our indices, functioned as proxies and offered a method for navigating some of the thousands of laws that affect vulnerable populations.
Although our policy assessments proved useful to evaluate policy landscapes by measuring variation in policies as written, using complementary methods to explore variation in policies as applied increased the usefulness of our results. For example, the policy assessment in Study 1 emphasized that state laws limit access to health-related public benefits programs, employment, and housing opportunities post-incarceration. Qualitative interviews found that persons may have increased opportunities to access health-related services, including STD screening and treatment, while incarcerated. This finding can inform policies that reduce barriers to benefits and services for persons reentering society, while continuing to invest resources into linkage-to-care services for incarcerated persons before reentry.
Our team continues to apply the benefits and lessons learned from our collaboration to engage in policy research studies that explore the relationship of STD disparities and social determinants of health in other populations that have health disparities. To build capacity for researchers and policy stakeholders who are interested in studying health disparities and improving policies with a public health lens, we have conducted trainings, presented at conferences and forums, published peer-reviewed articles, and made our data publicly available, when feasible. As research on the social determinants of health and health disparities evolves to leverage a multitude of methods and disciplines, we endeavor to accessibly and inclusively disseminate our work to engage a broader audience in policy solutions.
Evaluating the compound relationships of policies, social determinants of health, and STDs demands a multifaceted approach; however, including several disciplines and methods in a research study can be challenging. Because of variations among a multidisciplinary team in educational training, subject matter expertise, and skills, collaborators may not organically adopt a shared vocabulary and may be unfamiliar with each other’s research methods. Before conducting our studies, the attorneys on our research team were unfamiliar with developing protocols and instruments for human subjects research and the process of obtaining institutional review board approval, whereas the research scientists were not trained in using policy surveillance methods to study law and produce quantitative legal data. However, our experience demonstrated the usefulness of overcoming challenges in the use of multidisciplinary and mixed methods approaches and identified several areas for consideration when using these methods:
Consider applying mixed methods approaches to research studies related to STDs and social determinants of health and integrating team members from various disciplines with diverse research training and content expertise.
Establish a study foundation among multidisciplinary members. Identify the study scope collaboratively (and engage additional subject matter experts where appropriate), establish a shared vocabulary for methods and research questions, and facilitate regular and open communication.
Collaboratively engage in pilot or preliminary research to hone study objectives. Use iterative processes to align and refine methods, identify gaps in one method that the other can address, and clarify and define the scope before expanding the study population and jurisdictional focus.
Public Health Implications
We found that using mixed methods and multidisciplinary research strengthened our policy assessments for criminal justice–involved and LGB populations by improving our understanding of the scope of complex areas of policy that may indirectly influence STDs among vulnerable populations. Policy approaches in STD prevention have often focused on health care policies rather than broader policies that affect the social determinants of health. 12,30 Our research expanded such work to examine social determinants that may be less directly related to STD acquisition and prevention than health care policies. In addition, our results suggest that other research focusing on policy assessments of complex issues with substantial health disparities, such as HIV, viral hepatitis, and tuberculosis, may be enhanced by using a mixed methods approach and a diverse, multidisciplinary team.
Policies, and those who are affected by them, do not exist in a vacuum. Because public health is influenced by a variety of social, behavioral, biological, structural, and other factors, teams that include various disciplines and perspectives may be well equipped to explore solutions to improve public health. Using mixed methods and multidisciplinary approaches may leverage the strengths of each method to answer questions and find solutions for complex issues while addressing weaknesses of each method.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The projects described in this article were supported by cooperative agreements PS11-1112CONT14, CFDA# 93.978, and PS11-1112CONT13 from the Centers for Disease Control and Prevention.