
Abstract
Objectives
California is experiencing a syphilis and congenital syphilis epidemic, and many persons diagnosed with syphilis report a history of recent incarceration or sexual contact with a person who has recently been incarcerated. Fresno County’s local health department and jail collaborated to implement a routine syphilis screening policy for male adults aged 18-30 and female adults aged 18-35 booked into the facility. We evaluated syphilis screening, case finding, and treatment rates after implementation of the new policy.
Methods
We linked jail census and laboratory data to syphilis surveillance data to assess screening coverage, positivity, and treatment rates for age-eligible persons who were booked into Fresno County Jail from April 1, 2016, through December 31, 2017.
Results
Of 24 045 age-eligible persons who were booked into the jail during the study period, 5897 (24.5%) were female and 18 148 (75.5%) were male. Of 7144 (29.7%) persons who were screened for syphilis, 611 (8.6%) had a reactive rapid plasma reagin blood test result (16.4% [253 of 1546] of female adults; 6.4% [358 of 5598] of male adults) and 238 (3.3%) were newly diagnosed with syphilis, as confirmed by matching to the surveillance system (6.9% [106 of 1546] of female adults; 2.4% [132 of 5598] of male adults). Of persons identified with syphilis, 51.7% (n = 123 of 238) received adequate recommended treatment (59.4% [63 of 106] of female adults; 45.5% [60 of 132] of male adults).
Conclusions
The age-based syphilis screening policy adopted in this jail yielded high positivity, including newly identified syphilis infections among female adults of childbearing age. The targeted screening policy was formalized in the county-negotiated contract with the jail’s private correctional health care company in 2018—a strategy that can be replicated.
From 2012 to 2018, the total number of syphilis cases reported in the United States more than doubled, from 49 915 to 115 045. 1,2 Although the reasons for this increase are not fully understood, experts at the Centers for Disease Control and Prevention (CDC) hypothesize that contributing factors may include drug use, poverty, stigma, unstable housing, and cuts to sexually transmitted disease (STD) programs. 3 Untreated syphilis infection can lead to severe, long-term health problems, including brain and nerve damage. Syphilis can also be transmitted from mother to infant during pregnancy, known as congenital syphilis, at any stage of maternal disease and at any gestational age. 4 Syphilis infection during the prenatal period can cause adverse pregnancy outcomes, such as premature birth, and other negative fetal outcomes, such as low birth weight, stillbirth, and neonatal death. 5
Increases in syphilis morbidity in California mirror national trends, increasing 215.1% from 2012 (n = 8016) to 2018 (n = 25 256). 1,2 Most syphilis cases are reported among male adults, particularly among gay, bisexual, and other men who have sex with men. 6,7 Although the number of cases among female adolescents and adults is smaller than among male adolescents and adults, the greatest proportional increase in morbidity is among female adolescents and adults of childbearing age (15-44 years) and infants. 6,7 From 2012 to 2018, the number of cases of syphilis among female adolescents and adults of childbearing age increased 621.7% (from 608 to 4388; unpublished data, California Department of Public Health [CDPH], 2018), and the number of cases of congenital syphilis increased by nearly 900% (from 33 to 329). 7 National increases in the number of cases of congenital syphilis were driven by rising trends in states in the West and South. In 2018, approximately 25% of congenital syphilis cases in the United States were in California. 2 Resources for syphilis prevention, screening and treatment, outbreak response, and coordination of care for persons diagnosed with syphilis have not kept pace with increasing morbidity in California.
Nationally, jails admit more than 10 million persons each year. 8 Previous studies have found high rates of syphilis and other STDs among persons who are incarcerated. 9 -12 Factors that currently contribute to overall increases in STD incidence, such as drug use and unstable housing, are also commonly reported by persons who are incarcerated. 13,14 In addition, persons entering jails have lower rates of health care access and poorer health outcomes than their nonincarcerated peers. 15,16 These factors highlight the importance of directing public health efforts toward persons who are incarcerated. CDC, the National Commission on Correctional Health Care, and the US Preventive Services Task Force recommend syphilis screening in correctional facilities that are located in high morbidity areas. 17 -19 However, reviews have found that most jails do not implement routine, universal screening. 20,21
Given the aforementioned potentially severe consequences of untreated syphilis infection before pregnancy, focus has been placed on programmatic efforts to prevent, identify, and treat syphilis among nonpregnant female adolescents and adults of childbearing age in California. In 2018, 30.4% (479 of 1574) of interviewed female adolescents and adults of childbearing age diagnosed with syphilis in California (except San Francisco and Los Angeles) reported a history of incarceration or partner incarceration in the previous 12 months (unpublished data, CDPH, 2018). Although providing health care services in correctional settings requires unique structural and logistical considerations, STD screening in jails provides an opportunity to identify and treat infections that may otherwise go undetected to improve individual outcomes and interrupt ongoing community and fetal transmission.
Program Description
In 2018, Fresno County, located in California’s Central Valley, ranked fourth for the rate of congenital syphilis among all 58 California counties. 7 The incidence per 100 000 persons in Fresno County for all syphilis cases rose from approximately 3 cases in 2012 to 120 cases in 2018 (unpublished data, Fresno County Department of Public Health [FDPH], 2018). Given the increases in syphilis incidence among female adolescents and adults of childbearing age and congenital syphilis, FDPH issued a Health Alert (a message of high importance warranting immediate attention or action) in March 2015 designating Fresno County as an area with high syphilis morbidity. 22
In 2018, 21.8% (26 of 119) of interviewed female adolescents and adults of childbearing age diagnosed with syphilis in Fresno County reported a history of incarceration or partner incarceration in the previous 12 months, highlighting an opportunity to detect and treat infection (unpublished data, CDPH, 2018). The Fresno County Jail books more than 29 000 persons annually. 23
Counties may opt to outsource the provision of health care at correctional facilities by paying private, nongovernmental companies to provide care. From 2014 through 2018, the County of Fresno contracted with Corizon Health to provide health services at the jail. Given the ongoing syphilis epidemic and the overlap between persons diagnosed with syphilis and the local correctional system, FDPH and Corizon Health collaborated to develop a protocol for routine screening among persons entering the facility. Before the new protocol, the Fresno County Jail conducted symptom-based or patient-requested testing only. Symptom-based (diagnostic) testing occurred during the medical examination around day 10-14 after booking, and patients could request testing at any time during their incarceration.
In April 2016, the Fresno County Jail implemented the new policy to screen all booked male adults aged 18-30 and female adults aged 18-35 using a rapid plasma reagin (RPR) blood test as close to booking as feasible, with confirmatory treponemal testing occurring within 48 hours after the return of a reactive RPR result. Targeted age groups followed the model of CDC screening recommendations for chlamydia and gonorrhea in correctional settings. 17 The protocol instructed jail medical staff members to collect blood specimens after the person was released from the booking floor and moved to a housing unit. Collection occurred as close to booking as feasible, typically within 24-72 hours; however, at times it took longer. The jail began treatment for anyone still in custody after positive confirmatory results were returned. FDPH staff members conducted public health follow-up (eg, treatment verification) on persons with syphilis who were released before treatment completion, as determined by a prioritization algorithm. 24 For high-priority cases, such as pregnant persons, FDPH staff members reviewed electronic medical records, communicated with diagnosing and treating providers in the jail, conducted investigation and interview to confirm treatment, and, when possible, facilitated linkage to care for treatment. Corizon Health did not receive additional funding from the county to expand screening and treatment services beyond the amount stipulated by the existing contract.
The most recent published literature on routine syphilis screening in jails is limited to findings from efforts in New York in the early 1990s, which may not reflect the current epidemic. 25,26 We evaluated syphilis screening, case finding, and treatment rates from April 1, 2016, through December 31, 2017, after implementation of the new policy at the Fresno County Jail. Our evaluation provides current data that may be valuable to local health department STD programs that are looking for ways to collaborate with correctional partners, particularly jails, to provide routine STD screening for persons who are incarcerated.
Methods
Jail Census and Laboratory Data
We obtained a census database from the Fresno County Jail that included the name, jail identification number, date of birth, sex (male, female), date of booking, and date of release for each person incarcerated from January 1, 2016 (earliest data available), through December 31, 2017. A private laboratory processed specimens and transmitted the results back to the jail. Laboratory data included test date, RPR results, and titer values.
We linked the jail’s census data with its laboratory data based on a person’s jail identification number to determine screening coverage. We included specimen collection dates that fell within a person’s incarceration period. In the rare instance in which a person received >1 test during a single incarceration period, we retained the earliest positive result or the earliest result if all test results were negative. A person could have had >1 incarceration period included in the analysis if the person was arrested multiple times during the analysis period. All jail data were transferred to public health and stored securely.
Surveillance Data
Syphilis is a nationally notifiable disease and is required by law to be reported to governmental agencies. In California, laboratories and diagnosing and/or treating medical providers report notifiable disease data to the local health department, and data are collected and managed via an electronic surveillance system, the California Reportable Disease Information Exchange (CalREDIE). 27 To assess identification of new syphilis infection, treatment rates, and location of treatment administration (at the jail or otherwise), we linked jail census and laboratory data to CalREDIE data by using a probabilistic matching method based on name, date of birth, and sex. 28 We defined a newly identified case as a person who had evidence of a new diagnosis of syphilis with a reactive RPR and positive confirmatory test. To restrict results to identify only new cases and not follow up on existing cases in CalREDIE, we limited matches to those with a jail specimen collection date that preceded the CalREDIE record creation date.
Data Analysis
We calculated the screening rate among 24 045 age-eligible persons (male adults aged 18-30 and female adults aged 18-35) booked from April 1, 2016—after policy implementation—through December 31, 2017. We defined overall positivity as a reactive RPR and calculated the RPR reactivity rate among age-eligible persons booked who were screened for syphilis. We also calculated the proportion of newly identified cases among age-eligible persons who were screened for syphilis. Cases were classified in CalREDIE based on disease stage as defined by CDC (early: primary, secondary, or early nonprimary, nonsecondary; late or unknown duration). 29 We also calculated the testing rate and positivity among 3648 age-eligible persons booked from January 1 through March 31, 2016, before policy implementation.
We defined adequate treatment for nonpregnant persons as the recommended regimen of 1 dose of penicillin G or an alternative regimen of 14-day doxycycline administered for early syphilis and 3 doses of penicillin G administered 6-20 days apart or a 28-day doxycycline regimen for syphilis of late or unknown duration. Adequate treatment for pregnant persons was 1 dose of penicillin G for early syphilis or 3 doses of penicillin G, 6-8 days apart, for syphilis of late or unknown duration. 17 Inadequate treatment was any treatment documented in CalREDIE that did not meet the aforementioned criteria. We classified cases without treatment documentation in CalREDIE as unknown. We calculated treatment rates among persons newly identified with syphilis.
Using a combination of jail census, laboratory, and CalREDIE data, we calculated the median time from booking to release (length of stay) among persons newly identified with syphilis. We conducted all data management, matching, and data analyses using SAS version 9.4, 30 and we used the Pearson χ2 test to determine significant differences, with P < .05 considered significant. Because this study was an evaluation of an existing public health program, this analysis was considered exempt from institutional review board review.
Results
From January 1 through March 31, 2016, the Fresno County Jail tested 195 of 3648 (5.3%) age-eligible persons for syphilis.
From April 1, 2016, through December 31, 2017, 24 045 persons booked at the Fresno County Jail were eligible for syphilis screening, of whom 24.5% (n = 5897) were female and 75.5% (n = 18 148) were male. The distribution among age categories was nearly even for female adults and male adults (Table 1). The jail screened 7144 of 24 045 (29.7%) age-eligible persons for syphilis; the screening rate was significantly higher among male adults than among female adults (30.8% vs 26.2%; P < .001; Table 2).
Persons booked in the Fresno County Jail who were age-eligible for syphilis screening (n = 24 045), by age and sex, Fresno, California, April 1, 2016, through December 31, 2017 a
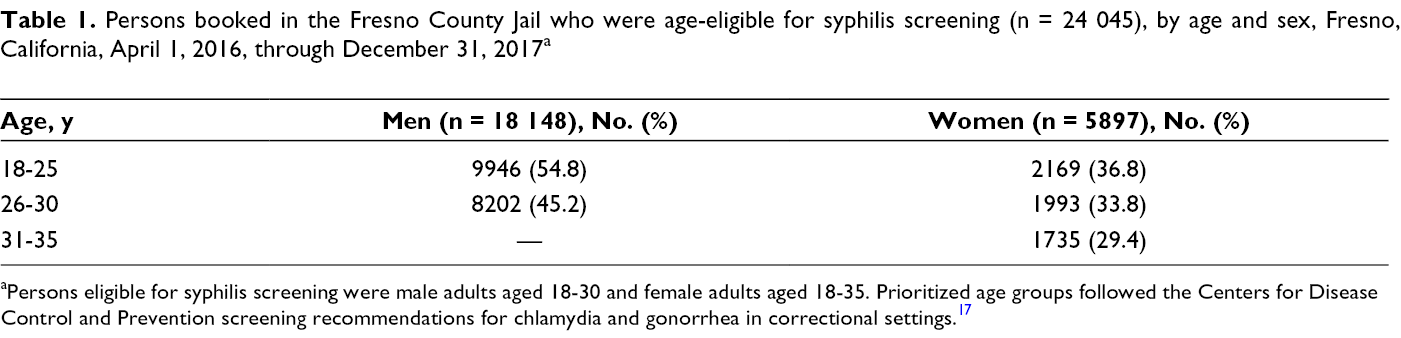
aPersons eligible for syphilis screening were male adults aged 18-30 and female adults aged 18-35. Prioritized age groups followed the Centers for Disease Control and Prevention screening recommendations for chlamydia and gonorrhea in correctional settings. 17
Syphilis screening results among age-eligible a persons incarcerated in the Fresno County Jail (n = 24 045), by sex, Fresno, California, April 1, 2016, through December 31, 2017
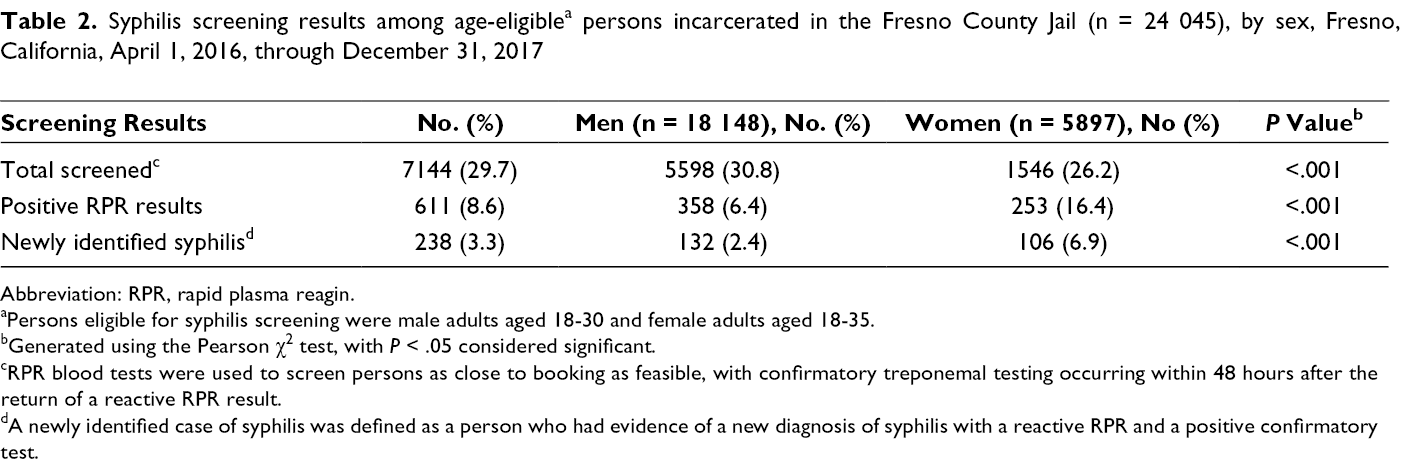
Abbreviation: RPR, rapid plasma reagin.
aPersons eligible for syphilis screening were male adults aged 18-30 and female adults aged 18-35.
bGenerated using the Pearson χ2 test, with P < .05 considered significant.
cRPR blood tests were used to screen persons as close to booking as feasible, with confirmatory treponemal testing occurring within 48 hours after the return of a reactive RPR result.
dA newly identified case of syphilis was defined as a person who had evidence of a new diagnosis of syphilis with a reactive RPR and a positive confirmatory test.
From January 1 through March 31, 2016, of 195 persons screened for syphilis, 40 (20.5%) had a reactive RPR and 23 (11.8%) were newly identified with syphilis (data not shown).
From April 1, 2016, through December 31, 2017, 611 of 7144 (8.6%) persons screened for syphilis had a reactive RPR (Table 2). RPR reactivity was significantly higher among female adults (16.4%; 253 of 1546) than among male adults (6.4%; 358 of 5598; P < .001). Three percent (238 of 7144) of persons screened were newly identified with syphilis, and the proportion of newly identified persons was significantly higher among female adults (6.9%) than among male adults (2.4%; P < .001; Table 2). Most (70.6%; 168 of 238) syphilis infections were staged as late syphilis or syphilis of unknown duration (Figure). The proportion of persons with late syphilis or syphilis of unknown duration was slightly but not significantly lower among female adults (67.9%; 72 of 106) than among male adults (72.7%; 96 of 132). The median length of stay for persons newly identified with syphilis was 34 days.
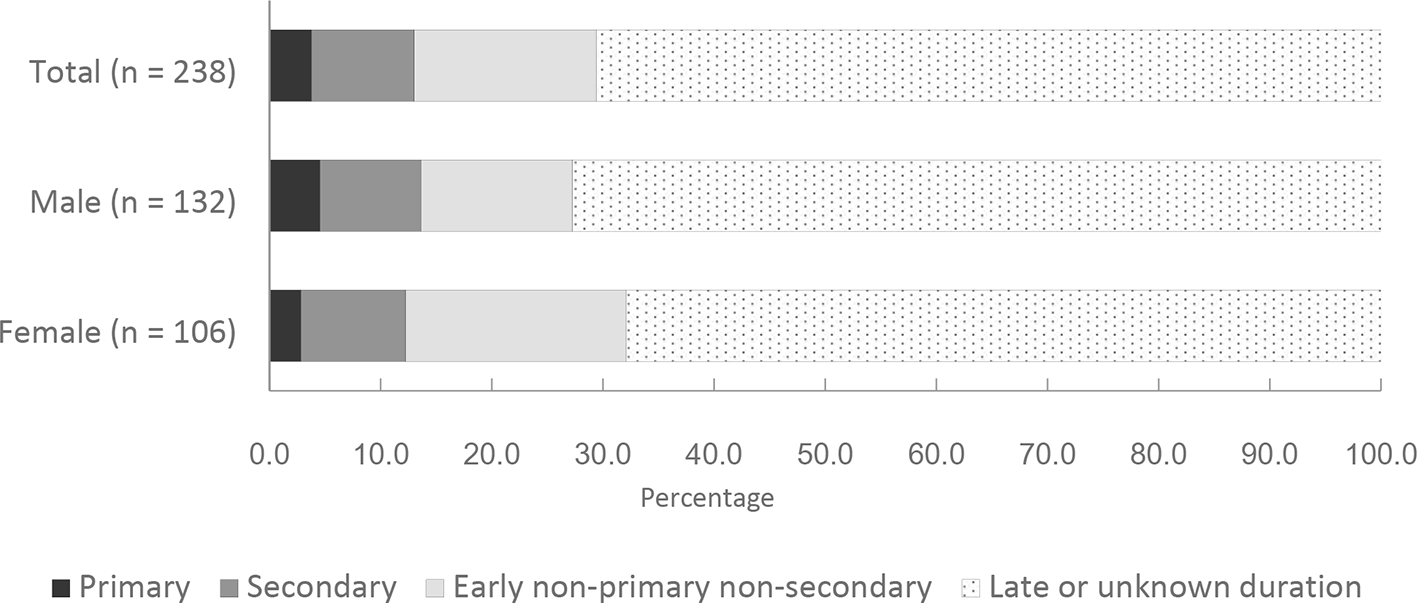
Stage of disease among male adults aged 18-30 and female adults aged 18-35 who were newly identified with syphilis (n = 238) at the Fresno County Jail, by sex, Fresno, California, April 1, 2016, through December 31, 2017. Primary, secondary, and early non-primary non-secondary syphilis are considered early syphilis.
Of 238 persons newly identified with syphilis, 162 (68.1%) received any treatment, 123 (75.9%) of whom were reported as adequately treated (Tables 3 and 4). Most persons who received any treatment received the first-line regimen (penicillin G; 79.0%; 128 of 162). The median length of stay was 58 days for persons who received adequate treatment and 36 days for persons who received inadequate treatment (data not shown).
Treatment results among male adults aged 18-30 and female adults aged 18-35 who were newly identified with syphilis at the Fresno County Jail (n = 238), by sex and stage of disease, Fresno, California, April 1, 2016, through December 31, 2017
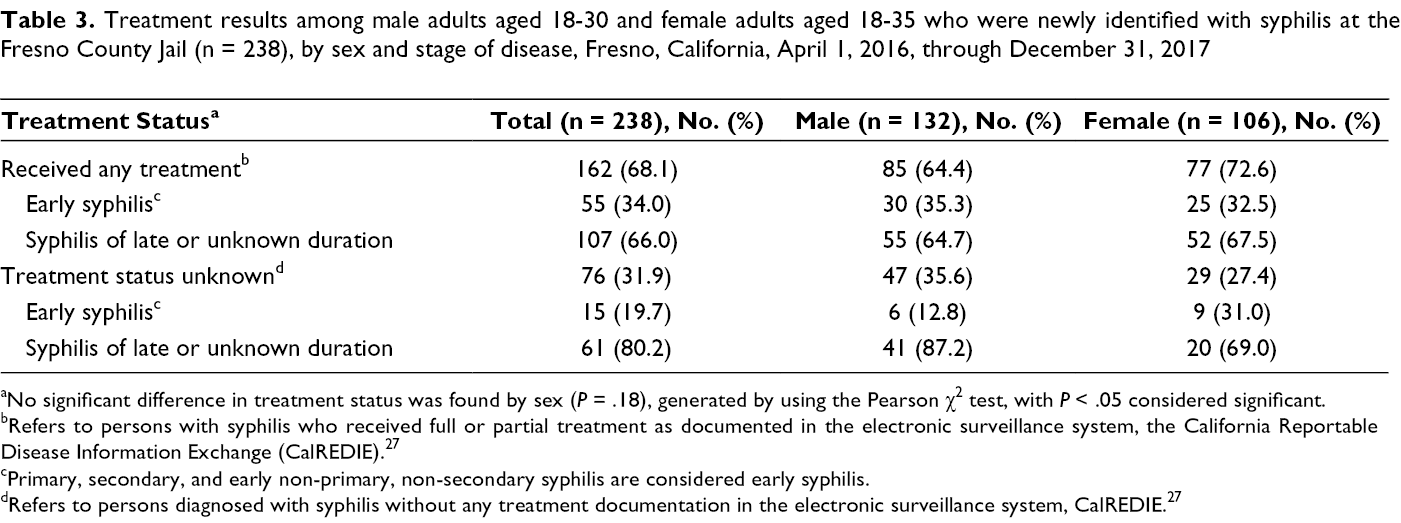
aNo significant difference in treatment status was found by sex (P = .18), generated by using the Pearson χ2 test, with P < .05 considered significant.
bRefers to persons with syphilis who received full or partial treatment as documented in the electronic surveillance system, the California Reportable Disease Information Exchange (CalREDIE).27
cPrimary, secondary, and early non-primary, non-secondary syphilis are considered early syphilis.
dRefers to persons diagnosed with syphilis without any treatment documentation in the electronic surveillance system, CalREDIE.27
Treatment adequacy among male adults aged 18-30 and female adults aged 18-35 who were newly diagnosed with syphilis at the Fresno County Jail (n = 238), by sex and stage of disease, Fresno, California, April 1, 2016, through December 31, 2017
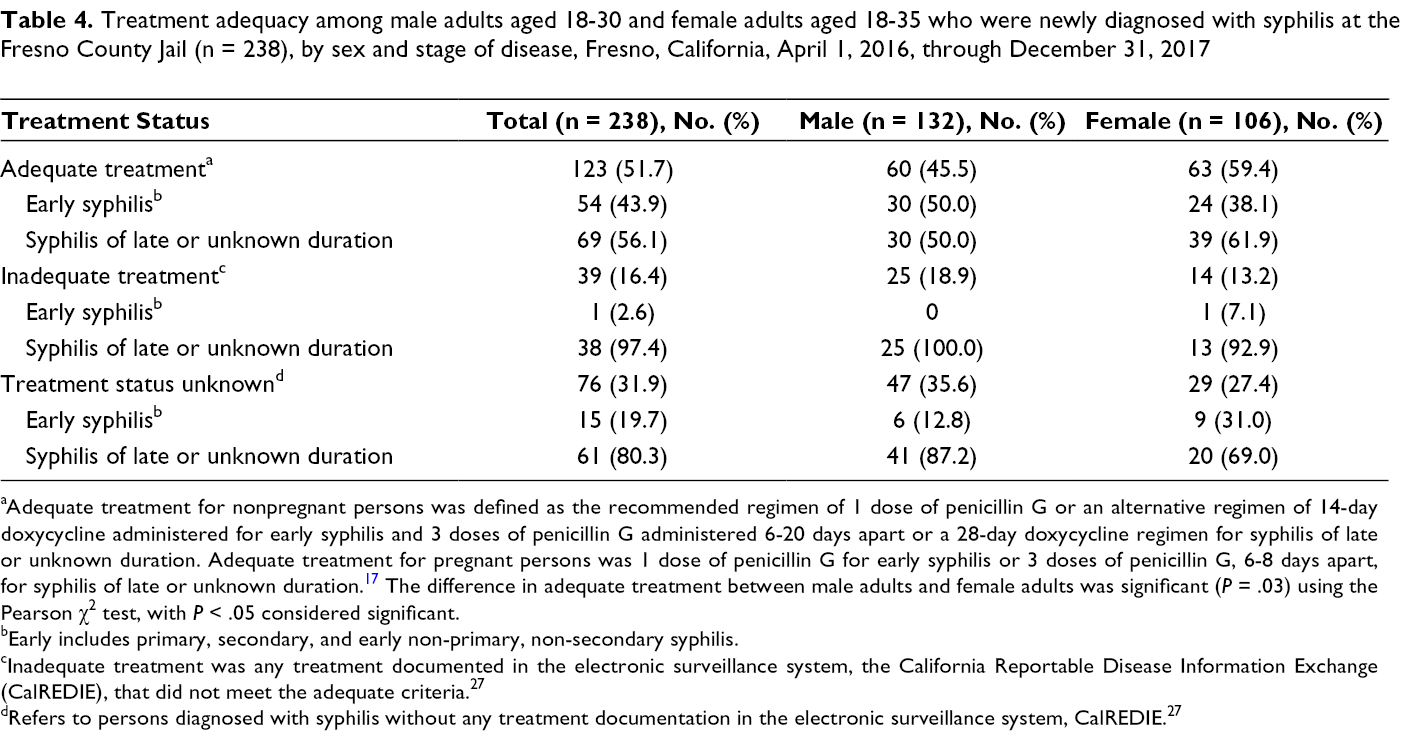
aAdequate treatment for nonpregnant persons was defined as the recommended regimen of 1 dose of penicillin G or an alternative regimen of 14-day doxycycline administered for early syphilis and 3 doses of penicillin G administered 6-20 days apart or a 28-day doxycycline regimen for syphilis of late or unknown duration. Adequate treatment for pregnant persons was 1 dose of penicillin G for early syphilis or 3 doses of penicillin G, 6-8 days apart, for syphilis of late or unknown duration. 17 The difference in adequate treatment between male adults and female adults was significant (P = .03) using the Pearson χ2 test, with P < .05 considered significant.
bEarly includes primary, secondary, and early non-primary, non-secondary syphilis.
cInadequate treatment was any treatment documented in the electronic surveillance system, the California Reportable Disease Information Exchange (CalREDIE), that did not meet the adequate criteria.27
dRefers to persons diagnosed with syphilis without any treatment documentation in the electronic surveillance system, CalREDIE.27
Of 123 persons who received adequate treatment, 103 (83.7%) received treatment from the jail during incarceration and 20 (16.3%) were treated after release (data not shown). A significantly higher percentage of female adults (59.4%; 63 of 106) than male adults (45.5%; 60 of 132) received adequate treatment (P = .03; Table 4). Most persons with early syphilis received adequate treatment (77.1%; 54 of 70), whereas a significantly lower percentage of persons with late syphilis or syphilis of unknown duration received adequate treatment (41.1%; 69 of 168; P < .001). Of 39 persons who received inadequate treatment, 34 (87.2%) had initiated treatment while incarcerated (data not shown).
Lessons Learned
Considerations for establishing a syphilis screening policy and implementing a screening program vary on the basis of factors such as jail operations and availability of resources (eg, staff members to conduct screening and deliver screening materials). Although no one-size-fits-all approach to implementing a syphilis screening program exists, our evaluation found that implementing a targeted, age-based routine syphilis screening policy in a local jail is feasible without additional funding. As with other corrections-based routine syphilis screening programs documented in the literature from the early 1990s, 25,26 the Fresno County Jail’s age-based screening policy led to the identification of many new syphilis infections (n = 238) that required treatment. These results suggest that even when universal screening (ie, screening all persons booked in the jail) is not possible because of resource constraints or other limitations, targeted methods (eg, screening on the basis of age) can be used to help detect syphilis in populations that are at high risk of syphilis, including incarcerated persons. Focusing on these populations can play an important role during epidemics to reduce the number of persons with syphilis and congenital syphilis. Although detection and treatment of syphilis among all persons have implications for congenital syphilis prevention, quickly identifying and treating female adolescents and adults of childbearing age diagnosed with syphilis is an important programmatic priority to prevent congenital syphilis. After the new screening policy was implemented, Fresno County Jail detected higher syphilis positivity among female adults than among male adults.
Although limited in scope, testing and positivity data from 3 months before implementation of the screening policy demonstrated the value of screening in this setting. We observed a greater proportion of syphilis cases among persons tested during the prepolicy period; however, this symptom-based testing method most often includes persons with clinical indications of syphilis. As such, a higher proportion of persons testing positive for syphilis prepolicy is not surprising. During high-incidence periods and particularly during congenital syphilis epidemics, the actual number of cases detected has greater importance, and more persons with syphilis on average per month were detected after the screening policy went into effect. STD programs that collaborate with jails to implement syphilis screening for priority populations should make efforts to acquire appropriate baseline data to evaluate the policy change, even if baseline data available are for diagnostic testing only.
Several important implementation considerations make a syphilis screening program in this setting challenging even when policies support the practice. Despite the policy, Fresno County Jail did not reach a high screening rate during the study period for several reasons. For one, it was not feasible for the jail to immediately screen persons at booking. Often, screening occurred several days after a person was booked; as a result, some persons were released from jail before screening could be conducted. In other cases, persons refused to be screened. Persons who are incarcerated often have competing health priorities or may have social and medical challenges that take precedence at the time of booking. Other possible challenges may include safety concerns for medical staff members that delay delivery of care, physical environment constraints such as lacking a proper place to draw a person’s blood at the booking station, and short turnaround time from when a person is booked and released. 31 These implementation considerations highlight that a formalized screening policy is a first step to authorizing and prioritizing screening in this setting, but the policy alone may not be sufficient.
Ensuring adequate treatment of syphilis is complex regardless of the setting, but it can be particularly complicated for persons who are incarcerated. For one, syphilis is most infectious and likely to be transmitted during the early stages, and most persons newly identified with early syphilis at the jail were reported to have received adequate treatment (54 of 70). For another, of those who were not adequately treated or whose treatment status was unknown, most had syphilis of late or unknown duration, which requires a longer treatment regimen than early syphilis. Using the jail census, laboratory, and surveillance data, we determined that one common reason why persons did not receive adequate treatment in the facility was because the jail received screening results with too little time to treat persons adequately before release. In addition, the percentage of persons who refused treatment is unknown. The jail initiated but did not complete treatment for 34 of 39 persons with newly identified syphilis. The New York City jail-based syphilis screening program achieved a >80% treatment rate by implementing rapid syphilis tests (STAT RPR) within 24 hours of booking for female patients. 25 Given that many persons who were diagnosed with syphilis at the Fresno County Jail were released before treatment could be initiated, FDPH and the jail plan to explore strategies to improve the treatment rate such as those used in New York City.
Accurately staging syphilis can be challenging, and syphilis of late or unknown duration may be more commonly staged than early syphilis because medical providers do not always have access to complete patient histories. In some instances, syphilis of late or unknown duration may in fact be an early syphilis infection, and partial treatment may be effective. Another treatment challenge is the cost of medication. The recommended treatment for syphilis, penicillin G, can be expensive, especially for correctional facilities that have barriers to accessing federal programs such as the 340B Drug Pricing Program, which reduces the cost of safety-net medications. 32 The cost of penicillin G could encourage facilities to use the alternative treatment regimen for nonpregnant persons, doxycycline, which is cheaper than penicillin G but takes longer to complete. However, treatment cost does not appear to have affected our analysis because, despite not participating in the 340B Drug Pricing Program, the Fresno County Jail stocked and administered penicillin G as the first line of treatment for syphilis during the analysis period. Persons who started but did not complete treatment were not discharged from jail with syphilis-related medications. Further research into the barriers to adequate treatment in jail populations and similar high-risk populations is needed.
Limitations
This analysis had several limitations. First, our analysis was limited by the data available from the jail’s census database, laboratory, and CalREDIE, which were the best sources available at the time. Data linking depended on record-matching methods that are inferential in nature and subject to false positives and false negatives. It is possible that some of the missing data were due to false results during the matching process. Second, surveillance data rely on accurate and comprehensive reporting of cases. Treatment rates may have been underestimated because of incomplete reporting of treatment data to public health surveillance or treatment having occurred outside the state. Regardless of the possibility of underreporting, it is promising that, at a minimum, 68.1% of persons newly diagnosed with syphilis received any treatment and that 51.7% of all persons newly identified with syphilis received adequate treatment.
In mid-2018, Corizon Health’s contract with Fresno County concluded, and a new private organization (Wellpath) began providing medical services in the jail. The same age-based routine screening policy was formally adopted into the new contract. To our knowledge, the County of Fresno’s contract with Wellpath represents the first time that syphilis screening has been explicitly incorporated into a county’s contract with a private jail medical services organization in California. Despite the many considerations of implementing such a screening policy, our evaluation demonstrates that a policy prioritizing syphilis screening can be a meaningful first step toward increasing the detection and treatment of persons with syphilis in a population at high risk for infection. FDPH and Wellpath plan to continue to evaluate the policy and identify strategies to increase screening coverage and overcome barriers to treatment.
Footnotes
Acknowledgments
The authors thank the staff members at the Fresno County Jail and Corizon for implementing the screening policy and providing the data needed to conduct the evaluation of this program. The authors also acknowledge colleagues at the California Department of Public Health (Ryan Murphy, PhD, MPH; Rosalyn Plotzker, MD, MPH; and Eric Tang, MD, MPH) and at the Fresno Department of Public Health (Joe Prado).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.