
Abstract
Objectives
In the United States, rising rates of overdose deaths and recent outbreaks of hepatitis C virus and HIV infection are associated with injection drug use. We updated a 2014 review of systems-level opioid policy interventions by focusing on evidence published during 2014-2018 and new and expanded opioid policies.
Methods
We searched the MEDLINE database, consistent with the 2014 review. We included articles that provided original empirical evidence on the effects of systems-level interventions on opioid use, overdose, or death; were from the United States or Canada; had a clear comparison group; and were published from January 1, 2014, through July 19, 2018. Two raters screened articles and extracted full-text data for qualitative synthesis of consistent or contradictory findings across studies. Given the rapidly evolving field, the review was supplemented with a search of additional articles through November 17, 2019, to assess consistency of more recent findings.
Results
The keyword search yielded 535 studies, 66 of which met inclusion criteria. The most studied interventions were prescription drug monitoring programs (PDMPs) (59.1%), and the least studied interventions were clinical guideline changes (7.6%). The most common outcome was opioid use (77.3%). Few articles evaluated combination interventions (18.2%). Study findings included the following: PDMP effectiveness depends on policy design, with robust PDMPs needed for impact; health insurer and pharmacy benefit management strategies, pill-mill laws, pain clinic regulations, and patient/health care provider educational interventions reduced inappropriate prescribing; and marijuana laws led to a decrease in adverse opioid-related outcomes. Naloxone distribution programs were understudied, and evidence of their effectiveness was mixed. In the evidence published after our search’s 4-year window, findings on opioid guidelines and education were consistent and findings for other policies differed.
Conclusions
Although robust PDMPs and marijuana laws are promising, they do not target all outcomes, and multipronged interventions are needed. Future research should address marijuana laws, harm-reduction interventions, health insurer policies, patient/health care provider education, and the effects of simultaneous interventions on opioid-related outcomes.
The age-adjusted rate of opioid-related overdose deaths in theUnited States increased from 2.9 per 100 000 population in 1999 to 14.9 per 100 000 population in 2017. 1 Synthetic opioids (non-methadone) were involved in 59.8% of opioid-related overdose deaths in 2017. 1,2 The opioid epidemic and associated increases in injection drug use have increased hepatitis C virus (HCV) incidence, particularly in the West and Appalachia, and contributed to HIV outbreaks among persons who inject drugs. 3 -5
Systems-level policy interventions, defined as state- or health systems–level regulations, laws, and policies, are needed to combat drug-related harms, including overdoses, and increased morbidity, mortality, and economic consequences of HIV infection, HCV infection, and related conditions. Some interventions address prescribing behavior: (1) state-level prescription drug monitoring programs (PDMPs), which require pharmacies to submit prescribing information on controlled substances to health departments or pharmacy boards; (2) health insurer and pharmacy benefit management strategies (eg, lock-in programs that limit opioid access among beneficiaries with a potential for overuse to a single prescriber or pharmacy or prior authorization programs that allow reimbursement only with the health care providers’ confirmation of a patient’s need for medication); (3) clinical guidelines on appropriate prescribing (eg, dosing, duration, and type of medication); and (4) pain clinic regulations (also referred to as “pill-mill” laws) that regulate certification, ownership, and other procedures in pain clinics that prescribe opioids. Other interventions address harm reduction and education: (1) legalizing the medical or recreational use of marijuana as a potential alternative for pain control; (2) naloxone distribution to persons who use drugs, community members, and first responders; (3) Good Samaritan laws, which provide immunity from investigation about possession of drugs for persons who call 911 while having or witnessing an overdose; and (4) educational materials for patients and/or health care providers about opioid use, adverse effects, and abuse, as well as alternative options for pain treatment.
Despite rapidly expanding literature evaluating systems-level opioid policies, consensus is limited. Results are mixed on whether PDMPs and state-level prescribing policies encourage responsible prescribing. 6,7 Naloxone distribution programs and legalization of medical marijuana show positive results, but studies have substantial limitations. 8,9 A comprehensive review of systems-level policies conducted in 2014 concluded that the evidence about which policies are effective was weak; many studies used low-quality designs and examined intermediary outcomes (eg, knowledge or prescribing practices) rather than direct health outcomes (eg, opioid use or opioid-related overdose). 10
Many studies of systems-level policies have been published since the 2014 comprehensive review. 10 Recent literature reviews on opioid policies have focused on 1 or few interventions, 6 -9 making it difficult to summarize current knowledge across interventions. The opioid epidemic has evolved since 2014, and interventions have expanded accordingly. To our knowledge, no similar updated review had been published at the time of our analysis. Our review updates the 2014 review with recent evidence about the effectiveness of systems-level interventions on opioid use, overdose, and mortality to identify promising policy interventions and research priorities.
Methods
We conducted a rapid review of literature published during 2014-2018, using the search strategy from a 2014 systematic review on this topic. 10 Rapid reviews and systematic reviews use similar techniques for finding and synthesizing evidence, but rapid reviews emphasize timeliness rather than exhaustiveness. 11 Although systematic reviews are the gold standard, rapid reviews address decision makers’ needs for quick syntheses of broader scopes of knowledge. They expedite the review process by narrowing the search, restricting review of the title/abstract or limiting review of the full-text article, and limiting the amount of data extracted or the quality of data assessed. 12 We used a rapid review because studies on opioid policies are evolving quickly, and timely assessment of the current state of knowledge and evidence gaps of these studies is crucial to inform current policy and research. Because we conducted a rapid review, 13 we did not perform a systematic assessment of each study’s bias risk. However, we extracted the limitations of each study, which are in an appendix (available from the authors upon request). A summary of the themes of these limitations is provided (Box).
Summary of major study limitations a among studies that examined the effectiveness of systems-level policies and interventions on opioid use, overdose, and deaths, United States and Canada, 2014-2018
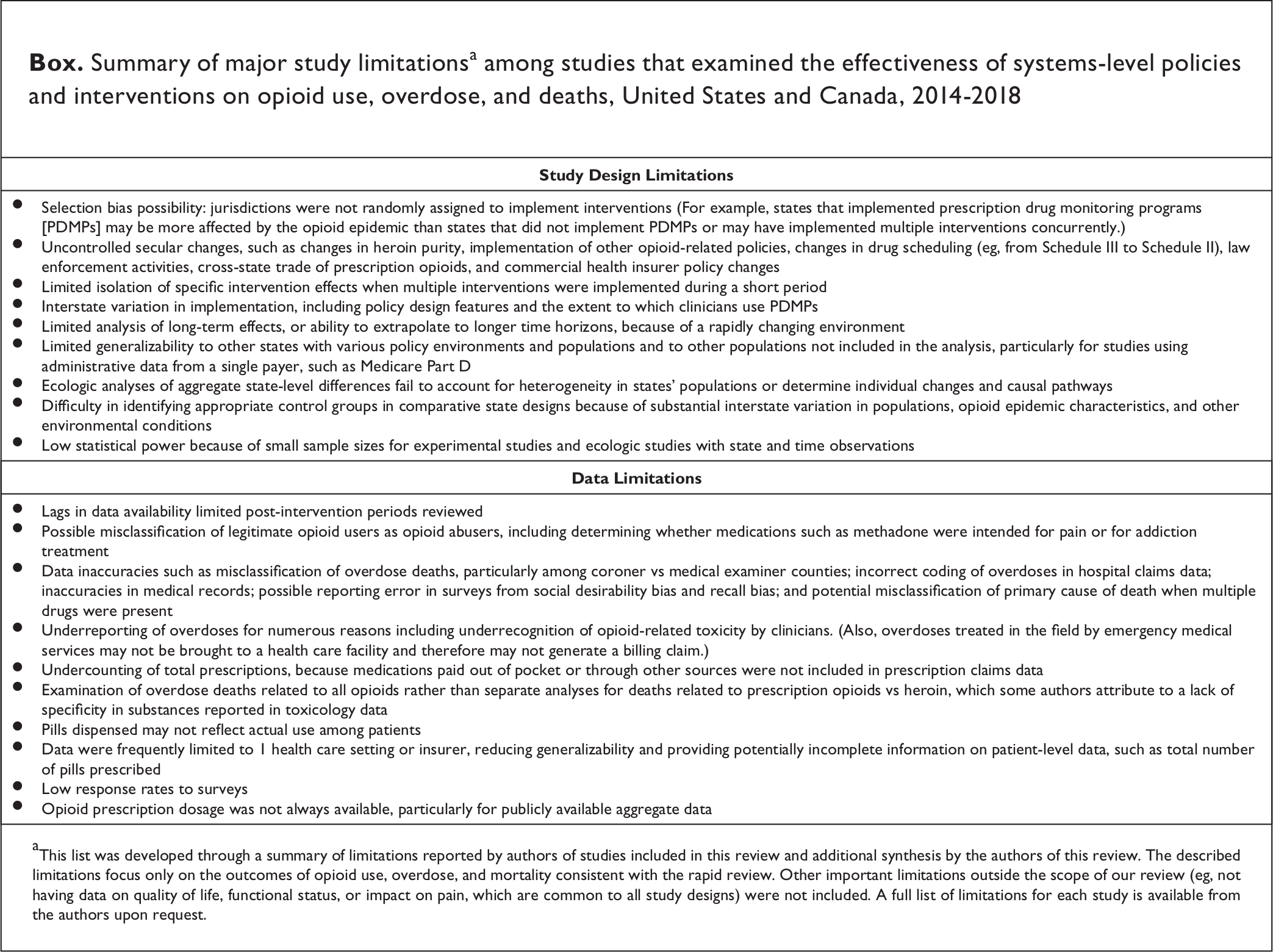
aThis list was developed through a summary of limitations reported by authors of studies included in this review and additional synthesis by the authors of this review. The described limitations focus only on the outcomes of opioid use, overdose, and mortality consistent with the rapid review. Other important limitations outside the scope of our review (eg, not having data on quality of life, functional status, or impact on pain, which are common to all study designs) were not included. A full list of limitations for each study is available from the authors upon request.
Search Strategy
We searched MEDLINE for articles published from January 1, 2014, through July 19, 2018. We selected the start date because the previous review went through 2013. The full list of search keywords is available in our study protocol, which is available from the authors upon request. A public health reference librarian reviewed our search strategy. We included all interventions from the 2014 review 10 : PDMPs, health insurer benefit management strategies, pain clinic regulations, clinical guidelines, harm-reduction interventions, patient and health care provider education, and safe storage and disposal of prescription drugs. We added marijuana laws. We excluded clinic-focused studies, such as studies of the effectiveness of naloxone in reversing overdose or marijuana in treating certain health conditions because we were interested in systems-level interventions. We supplemented our search procedure with a manual search of articles cited in references.
Review Process
Two coders (B.A., K.M.T.) reviewed titles and abstracts for eligibility and discussed discrepancies with other authors until they reached consensus. If inclusion criteria were unclear during title and abstract review, we assessed eligibility using full-text review. Study eligibility followed the population, intervention, comparator, outcomes, and timing (PICOT) approach from the Institute of Medicine guidance. 14 We limited the population to the United States and Canada. Our outcomes were opioid use, opioid-related overdose, and opioid-related overdose death. These population-level outcomes reflect the health experience of target populations receiving systems-level interventions, unlike individual-level outcomes from clinical studies such as the effects of medical marijuana on acute myocardial infarction, 15 oncology management, 16 and chronic neuropathic pain. 17 Opioid use outcomes included total number or volume of opioid prescriptions filled, per-capita or per-transaction morphine milligram equivalent (MME) dispensing, and number of opioid-abusing patients. Opioid-related overdose outcomes included overdose-related emergency department visits or inpatient admissions and self-reported surviving or witnessing an overdose. Opioid-related overdose death outcomes included age-adjusted opioid-related overdose death rates or death rates related to specific opioids, such as methadone or heroin. Included articles provided primary data analysis with an appropriate comparator for evaluating the policies using cross-sectional data, control groups, or pre–post designs.
Data Extraction and Synthesis
Two coders (B.A., K.M.T.) extracted study data, and other authors (E.S.R., E.G.M.) reviewed the data. We extracted data on location, data source, population covered, study design, treatment and control group characteristics, measures, key findings, and reported limitations. We categorized study locations into 4 US Census regions (Northeast, Midwest, South, and West), plus the New England Census division and Appalachia, which have high overdose rates. 1 Data sources were classified as survey data collected by investigators, administrative data (eg, PDMP and claims data), health surveillance systems (eg, vital statistics and national health monitoring surveys), and medical records.
We classified studies into 4 categories: (1) randomized experimental (investigators manipulated a treatment intervention, with randomized assignment of treatment and control conditions), (2) nonrandomized experimental (nonrandom assignment of treatment and control conditions), (3) quasi-experimental (longitudinal observational study of an intervention, with or without control groups), and (4) cross-sectional. Generally, evidence is strongest for randomized experimental studies, moderate for nonrandomized experimental or quasi-experimental designs, and weakest for cross-sectional studies. 18 Our qualitative synthesis focused on whether studies on a given intervention provided consistent or contradictory results for each outcome and the reasons for contradictory results (eg, intervention design features, data sources, outcomes, or other factors). Highly variable outcome definitions precluded a meta-analysis.
Results
Study Screening
The search yielded 535 unique articles, 465 of which were removed after screening titles and abstracts and 6 of which were subsequently removed after full-text review, leaving 66 studies for inclusion. The flow diagram of the study selection process is available from the authors upon request.
Overview of Study Designs, Outcomes Assessed, and Study Characteristics
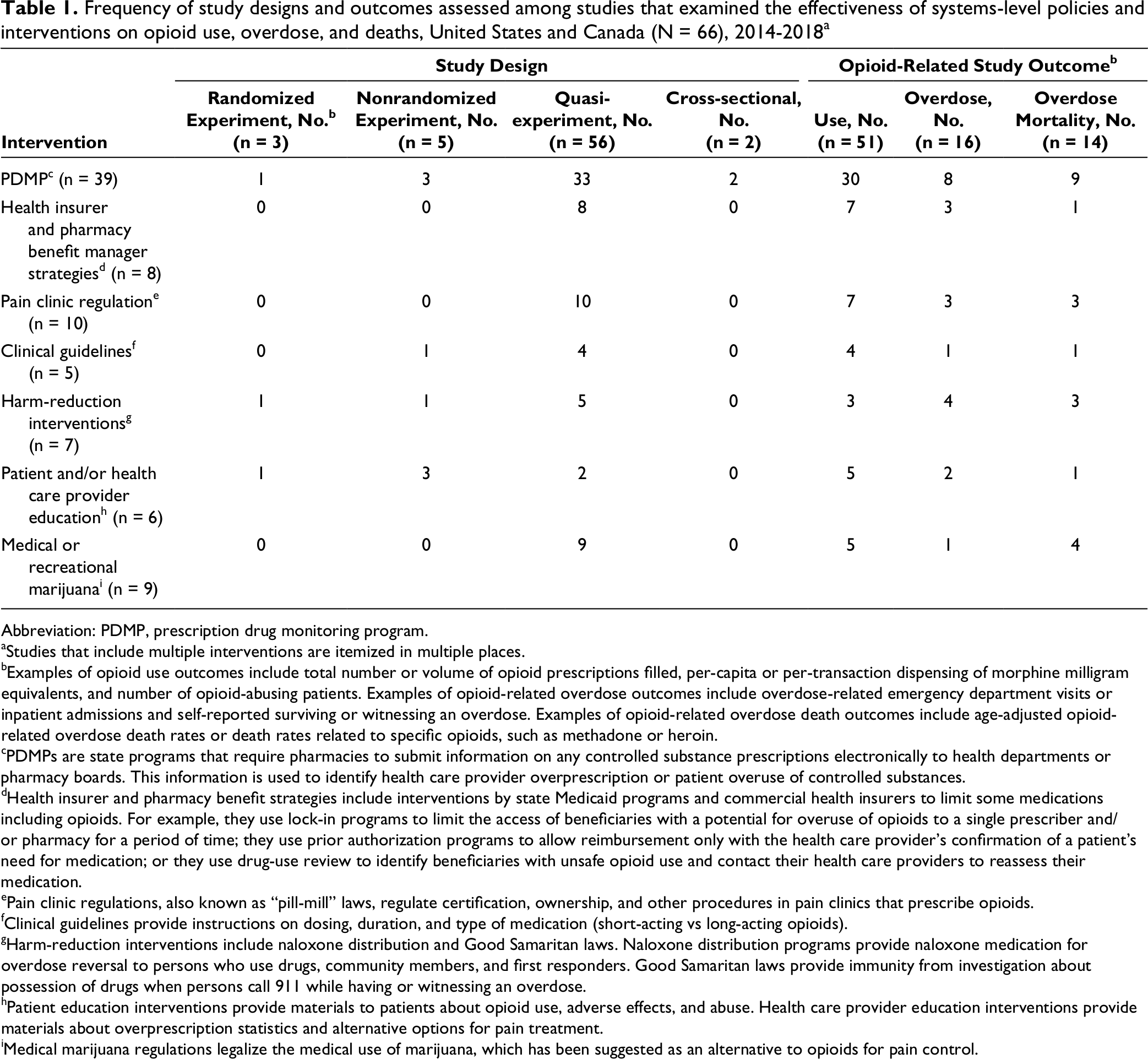
Quasi-experimental designs were most common overall (n = 56, 84.8% of all studies) and among all interventions except patient and/or health care provider education (Table 1). These studies leveraged states’ phased implementations to compare outcomes of intervention and control jurisdictions or evaluate interventions’ effectiveness by measuring changes in outcome trends before and after implementation. Experimental designs were used in 8 (12.1%) articles overall but were the most common design in studies evaluating educational interventions. Opioid use was the most common outcome assessed among all studies (n = 51, 77.3%), followed by opioid overdose (n = 16, 24.2%) and opioid-related overdose mortality (n = 14, 21.2%).
Frequency of study designs and outcomes assessed among studies that examined the effectiveness of systems-level policies and interventions on opioid use, overdose, and deaths, United States and Canada (N = 66), 2014-2018 a
Abbreviation: PDMP, prescription drug monitoring program.
aStudies that include multiple interventions are itemized in multiple places.
bExamples of opioid use outcomes include total number or volume of opioid prescriptions filled, per-capita or per-transaction dispensing of morphine milligram equivalents, and number of opioid-abusing patients. Examples of opioid-related overdose outcomes include overdose-related emergency department visits or inpatient admissions and self-reported surviving or witnessing an overdose. Examples of opioid-related overdose death outcomes include age-adjusted opioid-related overdose death rates or death rates related to specific opioids, such as methadone or heroin.
cPDMPs are state programs that require pharmacies to submit information on any controlled substance prescriptions electronically to health departments or pharmacy boards. This information is used to identify health care provider overprescription or patient overuse of controlled substances.
dHealth insurer and pharmacy benefit strategies include interventions by state Medicaid programs and commercial health insurers to limit some medications including opioids. For example, they use lock-in programs to limit the access of beneficiaries with a potential for overuse of opioids to a single prescriber and/or pharmacy for a period of time; they use prior authorization programs to allow reimbursement only with the health care provider’s confirmation of a patient’s need for medication; or they use drug-use review to identify beneficiaries with unsafe opioid use and contact their health care providers to reassess their medication.
ePain clinic regulations, also known as “pill-mill” laws, regulate certification, ownership, and other procedures in pain clinics that prescribe opioids.
fClinical guidelines provide instructions on dosing, duration, and type of medication (short-acting vs long-acting opioids).
gHarm-reduction interventions include naloxone distribution and Good Samaritan laws. Naloxone distribution programs provide naloxone medication for overdose reversal to persons who use drugs, community members, and first responders. Good Samaritan laws provide immunity from investigation about possession of drugs when persons call 911 while having or witnessing an overdose.
hPatient education interventions provide materials to patients about opioid use, adverse effects, and abuse. Health care provider education interventions provide materials about overprescription statistics and alternative options for pain treatment.
iMedical marijuana regulations legalize the medical use of marijuana, which has been suggested as an alternative to opioids for pain control.
All outcomes were evaluated in each region, although the Midwest was slightly underrepresented among studies that evaluated overdose, and the South and West had higher coverage than the Northeast and Midwest among studies that reported mortality (Table 2). Half (n = 35, 53.0%) of the studies included states in Appalachia and/or New England. The most commonly used data source was administrative data (n = 45, 68.2% of all studies), followed by surveillance data (n = 17, 25.8%), medical records (n = 6, 9.1%), and survey data (n = 5, 7.6%). Among 14 studies reporting opioid-related overdose mortality, 13 articles used mortality surveillance data. Overall, only 12 (18.2%) studies examined multiple policies.
Summary of geography, data source, and other characteristics of studies that examined the effectiveness of systems-level policies and interventions on opioid use (N = 66), United States and Canada, 2014-2018
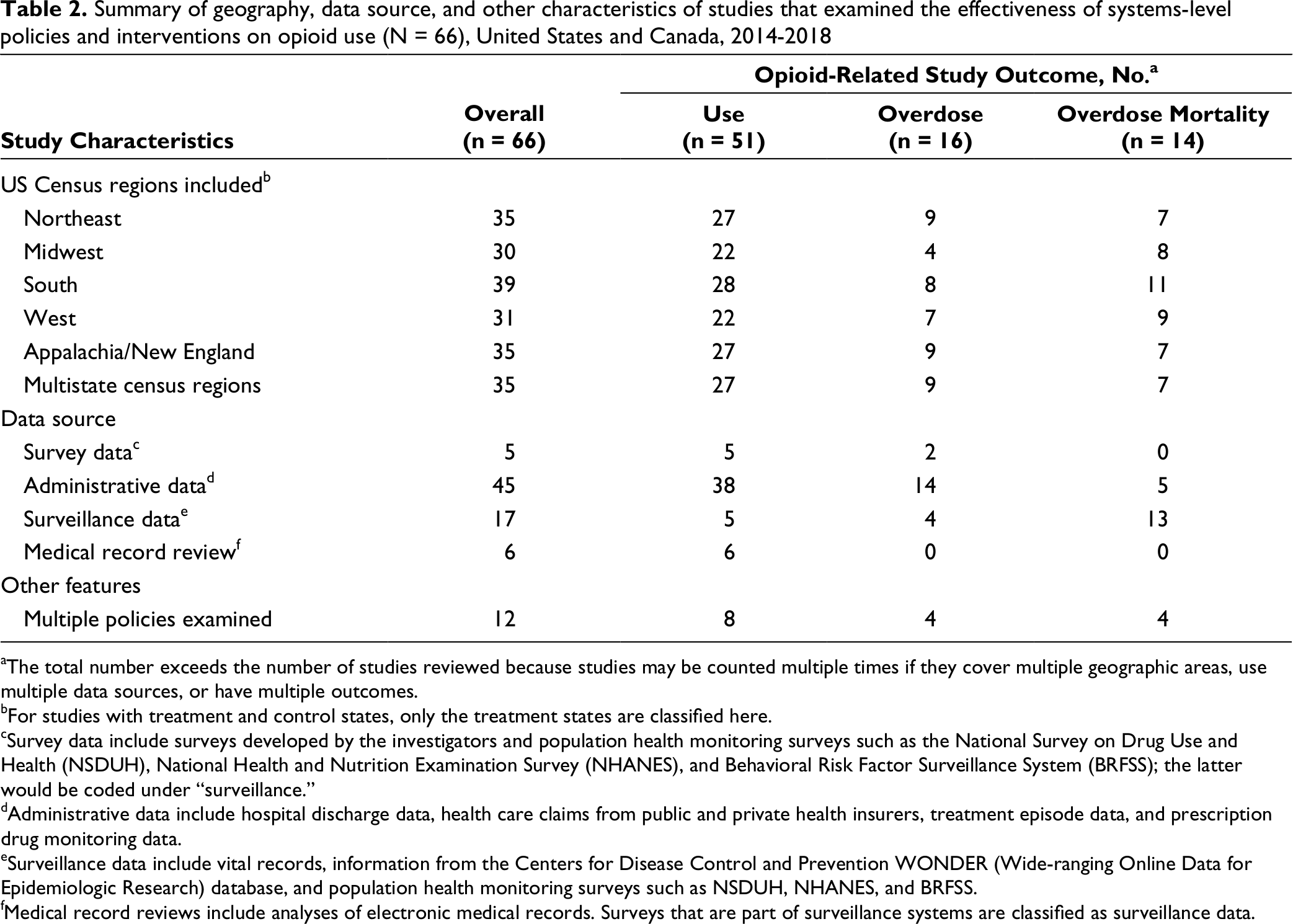
aThe total number exceeds the number of studies reviewed because studies may be counted multiple times if they cover multiple geographic areas, use multiple data sources, or have multiple outcomes.
bFor studies with treatment and control states, only the treatment states are classified here.
cSurvey data include surveys developed by the investigators and population health monitoring surveys such as the National Survey on Drug Use and Health (NSDUH), National Health and Nutrition Examination Survey (NHANES), and Behavioral Risk Factor Surveillance System (BRFSS); the latter would be coded under “surveillance.”
dAdministrative data include hospital discharge data, health care claims from public and private health insurers, treatment episode data, and prescription drug monitoring data.
eSurveillance data include vital records, information from the Centers for Disease Control and Prevention WONDER (Wide-ranging Online Data for Epidemiologic Research) database, and population health monitoring surveys such as NSDUH, NHANES, and BRFSS.
fMedical record reviews include analyses of electronic medical records. Surveys that are part of surveillance systems are classified as surveillance data.
Impact of Systems-Level Interventions on Opioid Use, Overdose, and Mortality
We report key findings from each study, by intervention type (Tables 3 -5). For each study, we report the population, type of data and data sources used, and key findings per outcome (ie, opioid use, overdose, and mortality outcomes).
Findings on the effect of prescribing interventions on opioid use, overdose, and mortality from studies examining the effectiveness of systems-level policies and interventions on opioid use (n = 41), United States and Canada, 2014-2018 a

aPolicy types are explained in detail in Table 1.
Findings on the effect of harm-reduction and educational interventions on opioid use, overdose, and mortality from studies examining the effectiveness of systems-level policies and interventions on opioid use (n = 13), United States and Canada, 2014-2018 a
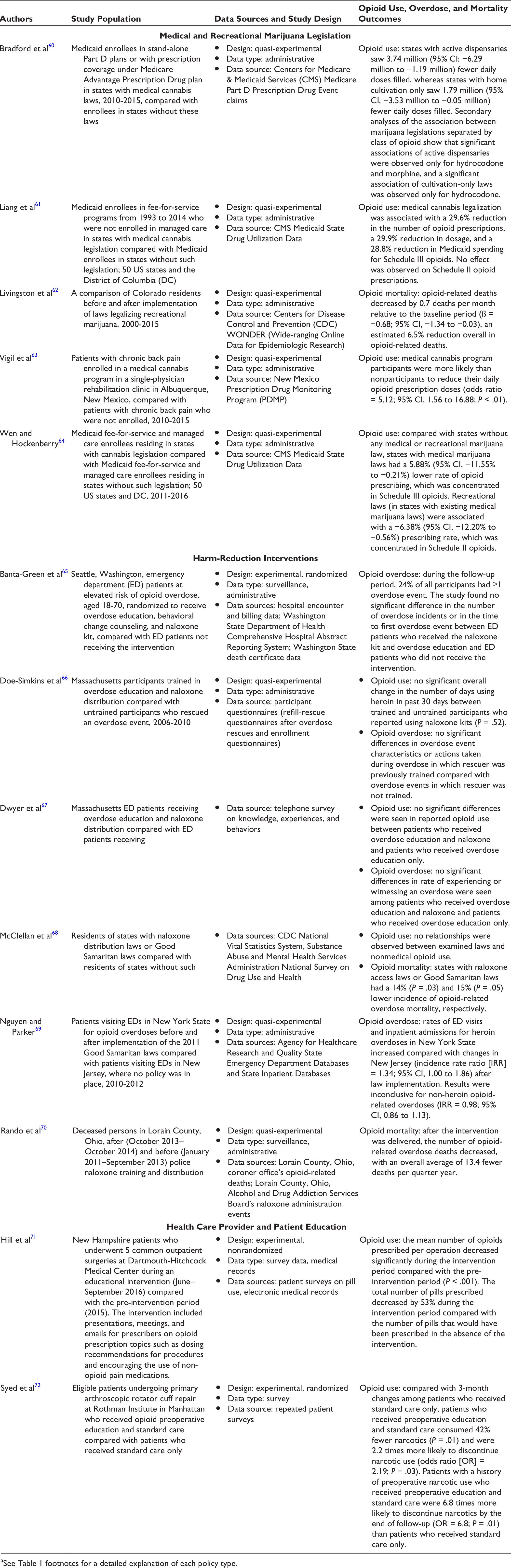
aSee Table 1 footnotes for a detailed explanation of each policy type.
Findings on the effect of implementing multiple concurrent interventions on opioid use, overdose, and mortality from studies that examined the effectiveness of systems-level policies and interventions on opioid use (n = 12), United States and Canada, 2014-2018 a
aSee Table 1 for detailed explanations of each policy type.
PDMPs
We found little consensus on the effectiveness of PDMPs. Although several studies found no effect on opioid prescribing and use after PDMP implementation 21,26,30–32,32 opioid prescription rates declined in Iowa 39 and pharmacists’ self-reported dispensing decreased in Indiana. 36 One study reported a 12.5% reduction in potentially inappropriate opioid prescriptions to Ontario residents with publicly funded drug insurance after implementation of a narcotic drug monitoring program. 27 Several multistate studies showed reductions in opioid prescriptions after PDMP implementation, including a 30% reduction in the self-reported rate of Schedule II prescriptions (opioids with high potential for abuse, such as hydromorphone) among patients reporting pain as a reason for visit 20 a limited decline in days’ supply of opioids prescribed among Medicare Part D enrollees, 45 and a reduction in the amount of opioid pills prescribed among persons with disabilities and older adult Medicare enrollees. 34
PDMP effects were stronger in regions where health care provider participation was mandatory, with varying effect sizes. Compared with pre-PDMP implementation, mandatory PDMP registration and use in Ohio were associated with fewer pills dispensed but not with reduced MME per prescription. 44 In Pittsburgh, Pennsylvania, mandatory PDMP access was associated with fewer patients prescribed opioids in the emergency department than pre-PDMP implementation 41 and mandatory PDMP access in New York State was associated with reduced prescription rates and quantity of pills prescribed by dentists. 40 States with mandatory PDMPs (vs states without mandatory PDMPs) reported reduced volume of opioid prescriptions filled among Medicaid enrollees 43 and reduced opioid misuse among Medicare Part D beneficiaries. 24
Unsolicited or automated reporting of PDMP data led to a significant reduction in the number of prescriptions and total MME prescribed in Massachusetts 46 yet it had no effect on the same measures in Nevada 33 or on the proportion of emergency department visits resulting in opioid prescriptions or prescribed MME in Washington State. 42 These differences may have been the result of state PDMP characteristics, such as different methods of automated reporting and/or analytic designs (eg, the study of unsolicited PDMP reporting in Nevada used propensity score matching 33 ). PDMP effectiveness may change over time: a 4-state study found an immediate decline in the percentage of persons filling opioid prescriptions after implementation of robust PDMPs that mandate access, monitor multiple drug schedules, and update data regularly, but only 1 state saw a sustained effect. 28
Some evidence suggests that PDMPs result in increased heroin use, presumably because opioid users will substitute heroin for opioids. Compared with residents of states without active PDMPs, residents of states with active PDMPs self-reported fewer days of nonmedical prescription pain medication use but more days of past-year heroin use. 19 Another study found higher treatment admissions for heroin and prescription opioids in 22 states after PDMP implementation (vs pre-PDMP implementation). 22
Findings on PDMPs’ influences on overdose and mortality rates were mixed. PDMPs were not associated with changes in nonfatal overdose rates among Medicare Part D enrollees nationwide, 24 but opioid- and heroin-related mortality in New York State increased after PDMP implementation. 23 In Florida, PDMP implementation was associated with decreased oxycodone-related overdose mortality 25 ; in Oregon, a higher number of overdoses occurred among patients of PDMP-registered physicians than among patients of clinicians who did not register for PDMPs. 26 Although 1 study found no effect of PDMPs on the rate of fatal drug overdoses in the US general population 35 PDMPs were associated with an increased risk of fatal overdose in 17 states. 29 Robust PDMP policies were associated with greater overdose mortality protection among states with PDMPs (vs states without PDMPs). 37,38
Health insurer benefit management strategies
State Medicaid programs and commercial health insurers commonly use preferred drug lists of certain brand-name and generic medications and require physician authorization for nonpreferred products. Compared with no policy, preferred drug lists and authorization policies were associated with fewer high-dose opioid prescription fills and a reduced likelihood of abusing opioid medication in several studies. 47,50 Rates of methadone overdose mortality were higher in Florida and North Carolina, which included methadone as a preferred drug, than in South Carolina, which did not include methadone as a preferred drug. 49 Health insurer–initiated drug-use review programs, which provide patients’ histories with controlled substances to health care providers, were associated with fewer controlled substance prescriptions filled compared with no drug-use review programs. 48 A drug-use review intervention in a Midwest Blue Cross Blue Shield plan led to a 28% decrease in the number of patients who received unsafe opioid combination prescriptions (eg, opioid and benzodiazepine). 52 Medicaid lock-in programs require patients to use a single designated prescriber and pharmacy. In North Carolina, the number of Medicaid-funded prescriptions and the average daily dose declined after implementation of lock-in programs 54 but this effect may have been offset by patients seeking non–Medicaid-reimbursed health care providers and prescriptions. 51 Similarly, a policy that limited the number of Medicaid-reimbursed short-acting opioids in Colorado was associated with a 3% decrease in the number of overall daily prescriptions reimbursed. 53
Clinical guidelines
Limited evidence exists on the effect of clinical guidelines for prescribing opioids 55,56 and no studies on clinical guidelines in our review examined overdose or mortality outcomes. A hospital system in Philadelphia found sustained decreases in the rate of opioid prescriptions after physician guidelines were distributed. 55 In Washington State, the median number of opioid prescription doses did not change among all users, but the median dose was reduced among patients who received high daily opioid doses. 56
Pain clinic regulations
Pill-mill laws in Texas were associated with reduced opioid use (number of prescriptions, average daily MME doses, and number of pills dispensed) 58 ; however, they were not associated with changes in the monthly percentage of Medicare beneficiaries who filled Schedule II or Schedule III prescriptions or with rates of opioid-related hospitalizations. 59 Pain clinic regulations and increased penalties for overprescribing were associated with fewer prescription opioid and heroin overdose deaths in Florida compared with North Carolina, which did not have pain clinic regulations. 57
Medical and recreational marijuana policy
One study with a small sample size found that patients with chronic pain who received medical cannabis had lower doses of opioid prescription than patients with chronic back pain who did not receive medical cannabis. 63 However, studies of Medicaid beneficiaries show that states with medical cannabis policies had fewer Schedule III opioid prescriptions, but not fewer Schedule II prescriptions, than states without medical cannabis policies. 61,64 States with medical cannabis laws with active dispensaries had fewer morphine and hydrocodone prescriptions among Medicaid Part D enrollees than states without these regulations. 60
We found limited but mixed results on recreational cannabis. One study found a decrease in the rate of opioid-related overdose deaths after Colorado legalized recreational marijuana. 62 Another study found no significant association between legalization of recreational marijuana and any opioid prescription (Schedule II or III) among Medicaid fee-for-service enrollees. 61 Yet another study found that, compared with states without any medical or recreational marijuana law, states with recreational cannabis laws had fewer Schedule II opioid prescriptions. 64
Harm-reduction interventions
Naloxone distribution programs were understudied in the articles we reviewed. In Lorain County, Ohio, the rate of overdose deaths decreased after a police naloxone training and distribution intervention. 70 The Good Samaritan law in New York State was associated with increased hospital admissions for heroin overdoses but not for non-heroin opioid-related overdoses. 69 Consistent with arguments that harm-reduction programs do not increase drug use 85 states with naloxone distribution and Good Samaritan laws had lower rates of opioid-related overdose mortality but no difference in opioid use compared with states that did not have such laws. 68 No benefits were observed in studies examining combined overdose education and naloxone distribution. A randomized controlled trial in Seattle, Washington, found that offering naloxone kits and education did not affect the time to first overdose event among patients at risk of opioid abuse. 65 Similarly, a study of overdose education and a naloxone distribution program in Massachusetts found no significant differences in opioid use, overdose occurrence, and actions taken during overdose among trainees who received a kit and education, trainees who received education only, and nonparticipants. 66,67 Of 6 studies on naloxone, deaths were evaluated in only 2 studies. 68,70
Patient and health care provider education
Several recent studies indicated that education interventions lead to a reduction in inappropriate prescribing and opioid use. A health care provider education intervention at a New Hampshire medical center was associated with fewer opioids prescribed than before the intervention 71 and a patient education intervention in a New York City institution led to lower opioid consumption, particularly among persons at high risk of opioid abuse or with past narcotic abuse, compared with persons who did not receive the intervention. 72
PDMP and pain clinic regulations
After Florida’s concurrent implementation of a PDMP and pill-mill laws, the number of opioid prescriptions, total opioid volume, and MME per transaction decreased among prescribers and patients with high rates of opioid prescriptions but not among prescribers and patients with low rates of opioid prescription. 73–75,75
Health care provider education and patient histories or clinical guidelines
Providing hand surgeons with prescription guidelines for various operations and an educational assistance tool reduced the amount of pain medication they prescribed. 77 However, an experimental study found that sending prescribers educational material and/or information about patients at risk for opioid abuse did not affect the number of opioid prescriptions. 76
Medical marijuana with PDMP and pain clinic regulations
After controlling for PDMP and pain clinic regulations, 2 studies reported negative associations between medical cannabis laws and opioid-related hospitalization and mortality. 78,81 A study of PDMP and medical marijuana policies found an interaction effect between the 2 policies: mortality was lowered when PDMPs and medical marijuana policies were implemented simultaneously. 80 A national study of PDMPs, pain clinic regulations, medical marijuana, and harm-reduction strategies found that only robust PDMPs and medical marijuana policies had significant effects on opioid-related mortality. 79
Other concurrently implemented interventions
One multi-intervention study (including prescribing and dispensing limits, health care provider education, and prescriber-specific performance feedback to health care providers) in a large health care system in Southern California reported 30% fewer high-dose prescriptions and 98% fewer prescriptions with ≥200 pills after implementation compared with before implementation. 83 A study of 7 interventions (diversion control, community education, health care provider education, naloxone policies, support for patients with pain, hospital emergency department policies, and addiction treatment) in North Carolina found little to no effect of each strategy on the rate of opioid-related hospital visits and death after controlling for the presence of other policies. 82 A national evaluation of 8 policies—PDMPs, pain clinic regulations, prescription limits, tamper-resistant prescriptions, patient identification, doctor-shopping (ie, visiting multiple physicians to obtain multiple prescriptions) restrictions, physician examinations, and pharmacist verification—found little effect on opioid use or overdose among Medicare beneficiaries. 84
Impact of Systems-Level Interventions on HIV, HCV, Tuberculosis, and Sexually Transmitted Infections
Only 1 study reported HIV/HCV outcomes. The study examined implementation of an automated PDMP among Medicaid members in Washington State and reported no change from pre- to post-implementation of the automated PDMP in the percentage of patients with a reported history of HIV/AIDS. 42
Study Limitations
We found common study limitations (eg, selection bias, secular changes, isolating intervention effects, implementation variability, short time horizons, generalizability, ecological studies, and appropriate control groups) and data limitations (eg, time lags, misclassification of abuse and deaths, undercounting overdoses and prescriptions, aggregate mortality measures, pills dispensed vs use of pills, and generalizability) among most studies we examined (Box). However, although selection bias and interstate variation in implementation were commonly stated in PDMP studies, they are broadly applicable to any state-level intervention.
Discussion
Considerable developments have taken place in opioid-related policies since the 2014 review, which concluded that the evidence base was weak overall. 10 Robust evidence in the current review supports the effectiveness of PDMPs that mandate physicians’ access to patients’ prescription history for controlled substances. Evidence was limited on new interventions, such as naloxone distribution and marijuana legalization. Furthermore, evidence on clinical guidelines, health insurer policies, and educational interventions continues to be limited. Future research should focus on these areas.
Interventions to lower the prevalence of opioid use disorder may improve downstream control of HIV/HCV infection. 86 Modeling evidence shows that these interventions increase the efficiency and cost effectiveness of HIV/HCV epidemic strategies, supplementing interventions focused on risk behaviors, such as syringe services programs. 87,88 Systems-level opioid use interventions will likely be a necessary part of achieving national goals of ending the HIV and HCV epidemics. 89,90
Naloxone distribution and Good Samaritan laws are understudied. These interventions are crucial for mitigating negative consequences of the opioid epidemic, and evidence suggests that they may reduce opioid-related overdose mortality. 68 A 2019 study (outside our review period) found that states with laws on naloxone access had fewer fatal overdoses but more nonfatal overdoses presenting to emergency departments than states without laws on naloxone access. 91 Further research is needed on potential unintended consequences. We focused on the effects of harm-reduction interventions on opioid use, overdose, and mortality outcomes. However, other interventions (eg, syringe services programs) may alleviate the incidence of infectious disease associated with injection drug use.
Medical cannabis laws are associated with reduced opioid-related hospitalizations and mortality. 78,79,81 Laws to legalize recreational marijuana are new, and few studies evaluated their effect on opioid-related outcomes. Because early adopters of medical marijuana legalization may differ, it is speculative to extrapolate from the limited evidence to determine how similar changes in law will affect population outcomes in other states. Further research using longer time horizons and individual-level data is needed.
PDMPs are the most studied and widely implemented opioid policy. Consistent with the previous review, 10 we found inconsistent results for the effect of PDMPs on opioid use, overdose, and deaths, which is partly attributable to heterogeneous policy designs. However, converging evidence suggests that mandatory PDMPs reduce inappropriate prescribing behavior. Our rapid review focused on opioid use, overdose, and mortality outcomes. However, a potential unintended consequence of systems-level policies such as PDMPs and changing health care providers’ prescribing behavior is that individual or population health might worsen if persons with addiction are pushed to illicit markets. This concern is supported by 3 studies we reviewed that found higher heroin poisoning rates among states that implemented PDMPs than among states that did not implement PDMPs. 19,22,23 Most studies of PDMPs use administrative PDMP or claims data on the number of pills or MME dispensed per capita. These studies may underreport total number of prescriptions because other sources, including the illicit market, are excluded and pills dispensed may not reflect actual use. More importantly, the administrative data include behaviors and not meaningful health outcomes such as addiction, quality-of-life indicators (eg, poor health days, self-rated health), and sequelae of heroin use (eg, HCV and HIV infection). Future research should prioritize long-term health consequences of these policies beyond opioid use, overdose, and mortality.
Since the 2014 review, 10 few studies have investigated the effects of clinical guidelines, health insurer policies, and patient or health care provider interventions on opioid mortality. We identified only 1 study that examined the effect of health insurer policies on opioid mortality. 49 This study was limited in scope and had no causal identification; yet, its positive results suggest that clinical guidelines are promising.
Heterogeneity in implementation, and the concurrent implementation of multiple interventions, precludes meta-analyses. Some studies examined concurrent interventions, using particular study designs to isolate the effects of individual interventions in combination studies. 82 -84 Only 12 included studies examined multiple interventions. Studying simultaneous interventions is a priority research area, because interventions are rarely implemented in isolation.
Given the rapid evolution of studies on opioid policies, additional literature has been published since our review: 23 studies published from July 19, 2018, through November 17, 2019, met our inclusion criteria. PDMPs are still the most commonly studied intervention, and recent research has focused on the program characteristics that improve the effect of PDMPs on opioid-related outcomes. Consistent with the findings from our rapid review, newer studies have mixed conclusions. Two studies investigated interstate PDMP data sharing (not investigated in the studies we reviewed) and found no effect on the number of opioid prescriptions. 92,93 Six studies found that mandatory use of PDMPs, including unsolicited and proactive reporting of patient prescription histories, improved opioid-related outcomes. 94 -99 These positive findings on strong PDMPs were not uniform: 1 study found no significant association between mandatory use requirements and the number of opioid prescriptions among patients undergoing general surgical procedures 100 and another study found that strong and weak PDMPs were associated with similar changes in opioid prescription rates, the number of cumulative doses, and prescription length (in days) among Medicare beneficiaries. 101
Studies published after our review period investigated Good Samaritan laws, pain clinic and marijuana regulations, prescribing guidelines, and educational interventions. Evidence in more recent studies refutes positive findings from the studies in our review. We reviewed a national study that found reduced mortality after implementation of Good Samaritan laws and naloxone distribution. 68 However, a more recent study on Good Samaritan laws found no significant effect on opioid-related overdose mortality. 102 Similarly, studies on pill-mill laws that we reviewed found an increase in the number of opioid prescriptions in Texas 58,59 and opioid-related mortality in Florida 57 ; however, a 2019 study found null effects of pill-mill laws on opioid prescriptions in Ohio and Tennessee, despite robust enforcement of these laws. 103 Two additional studies in 2019 on medical marijuana policies found lower rates of opioid use in areas with legalized medical marijuana policy than in areas without such policy, consistent with our results. 104,105 However, a replication of the article by Bachhuber et al 78 that used more recent data concluded that associations between opioid-related overdose mortality and cannabis laws may be “spurious”: the association between opioid-related overdose mortality and medical marijuana laws reversed direction, and mortality increased during the longer time horizon, but no association was found between recreational marijuana laws and the number of overdoses. 106
Studies of prescribing guidelines and educational interventions published after our review were consistent with studies we reviewed. The 5 newer studies on institutional, state, or national guidelines also found significant associations between guideline implementation and a decrease in the number of opioid prescriptions. 107 -111 The 3 recent studies on educational interventions found a decrease in opioid prescribing after implementation of an educational intervention for patients 112 and a combined guidelines/educational intervention for health care providers. 113,114
Public Health Implications
Tackling the opioid epidemic and its effect on HCV/HIV infection, morbidity, and mortality requires a comprehensive approach with multiple interventions. States that mandate PDMP access have seen declines in inappropriate prescribing practices 24,43 and states that have legalized medical or recreational marijuana have seen reductions in the number of opioid-related overdose deaths. 78,79,81 An integrated approach that combines multiple intervention strategies is needed, but scaling up complex policies to state or regional scales can be difficult to implement and monitor. 82 Future research should focus on the effects of these combined interventions.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors declared no financial support with respect to the research, authorship, and/or publication of this article.