
Abstract
In 2014, New York State became the first jurisdiction to launch a statewide initiative to end AIDS by reducing the number of persons living with HIV for the first time since effective HIV treatment became available. The Ending the Epidemic (ETE) initiative encompasses (1) identifying and linking undiagnosed persons with HIV to care, (2) retaining persons with HIV in care, and (3) facilitating access to preexposure prophylaxis for persons at risk for acquiring HIV. We used a framework for public health program implementation to describe key characteristics of the ETE initiative, present progress toward 13 ETE target metrics, and identify areas in need of increased programming. We provide evidence suggesting that New York State is on track to end AIDS as an epidemic by the end of 2020. As of 2017, 76% of progress toward our primary ETE target had been achieved. Substantial progress on several additional metrics critical to decreasing HIV prevalence and to improving the health of persons living with HIV had also been achieved. Lessons learned included the following: (1) ETE-based programming should be tailored to each jurisdiction’s unique political and social climate, HIV epidemiology, fiscal resources, and network of HIV service providers; (2) key stakeholders should be involved in developing ETE metrics and setting targets; (3) performance-based measurement and timely communication to key stakeholders in real time are essential; and (4) examining trends in HIV prevention and care metrics is important for developing realistic ETE timelines.
For decades, New York State was the epicenter of the HIV epidemic in the United States, and the state still has more persons living with HIV (PLWH) than any other state. 1 Nationally, trends in the number of new HIV diagnoses vary by region; the largest decreases are in the Northeast, and little change has occurred in the South. From 2012 to 2017, the number of new HIV diagnoses decreased 20% in the Northeast (from 7509 to 6011), 8% in the Midwest (from 5489 to 5032), 7% in the West (from 7815 to 7270), and 2% in the South (from 20 367 to 19 968). 1 At the height of New York State’s HIV epidemic in the early 1990s, more than 14 000 persons were newly diagnosed with HIV annually. Noticeable and consistent annual decreases in new HIV diagnoses began immediately after the introduction of effective antiretroviral therapy in 1996. By the end of 2017, New York State ranked fourth in the number of new HIV diagnoses (2769) and ninth in the rate of new HIV diagnoses per 100 000 population (13.7). In 2017, 78% of PLWH and 73% of newly diagnosed persons in New York State lived in New York City. 2
The rate of decline in new HIV diagnoses had been increasing in the years leading up to 2014, when the New York State Ending the Epidemic (ETE) initiative launched: the number of new HIV diagnoses decreased 16% from 2002 to 2007 (from 5342 to 4477) and 25% from 2008 to 2013 (from 4545 to 3394), suggesting improved HIV prevention and care programming. 2 In addition, the estimated number of new HIV infections occurring annually (HIV incidence) decreased 40% in 7 years, from 4069 in 2006 to 2430 in 2013 (unpublished data, AIDS Institute Bureau of HIV/AIDS Epidemiology, 2019). Mother-to-child transmission of HIV in New York State decreased from an estimated 450 cases in 1989 to 2 cases in 2013, and injection drug use as a risk factor in new HIV diagnoses decreased from more than 40% in the early 1990s to less than 5% in 2013. 3
These epidemiologic conditions, coupled with the advent of new HIV prevention options including preexposure prophylaxis (PrEP), sparked discussions about the possibility of ending AIDS in New York State. New York State defines “ending AIDS” as a reduction in the estimated number of new HIV infections to levels below the number of observed HIV deaths among PLWH. When this reduction occurs, HIV prevalence, or the number of PLWH in New York State, will have decreased for the first time since effective HIV treatment became available in 1996. Importantly, the New York State definition of ETE does not require the absolute elimination of HIV/AIDS, which would require a cure for PLWH and a vaccine to prevent future transmission.
In June 2014, New York State became the first US jurisdiction to formally announce a plan (the ETE initiative) to end AIDS by the end of 2020. 4 Achieving this goal will require the annual decline in estimated new HIV infections to double relative to the pre-ETE rate of decline of 6 percentage points per year. The ETE initiative has 3 core components: (1) identifying persons with HIV who are undiagnosed and linking them to care, (2) retaining PLWH in care to maximize viral suppression, promote health, and prevent further transmission, and (3) facilitating access to PrEP and nonoccupational postexposure prophylaxis (nPEP) for persons at high risk of acquiring HIV to prevent acquisition of HIV. These 3 components are core activities to ending AIDS because up to 80% of new HIV infections are transmitted by persons who either are unaware of their HIV status or are aware of their HIV status but not receiving treatment 5 ; persons with undetectable viral load cannot transmit the virus sexually, 6,7 and PrEP reduces the risk of acquiring HIV through sexual contact by more than 90%. 8 -10
This article describes the key characteristics of the ETE initiative, provides an update on New York State’s progress toward ending AIDS at ETE’s halfway point (2017), and discusses considerations for replicability elsewhere.
Methods
We used a framework for effective public health program implementation to describe the key characteristics of New York State’s ETE initiative. The framework identifies 6 key areas for successful public health programming: (1) innovation to develop an evidence base on which to act, (2) a finite number of evidence-based interventions to effect change, (3) real-time performance-based measurement and evaluation, (4) effective public and private partnerships, (5) timely and effective communication to stakeholders, and (6) political commitment to secure resources and support. 11 We gathered evidence from policy documents developed through participatory processes, including New York State’s ETE Blueprint, 4 and the authors’ experiences as executives, researchers, epidemiologists, and academic partners involved in various phases of policy development and implementation. We also found evidence through surveillance 1,2 and other data available from New York State’s ETE Dashboard 12 and from New York State–specific literature. 13,14 New York State’s progress toward ending AIDS is described through core ETE metrics created by a specially formed metrics committee of New York State and New York City health department staff members, service providers, researchers, and community members.
Outcomes
The ETE Timeline
We identified key events leading up to, including, and following the announcement of New York State’s ETE initiative (Table 1).
New York State Ending the Epidemic (ETE) initiative timeline, 2013-2020 a
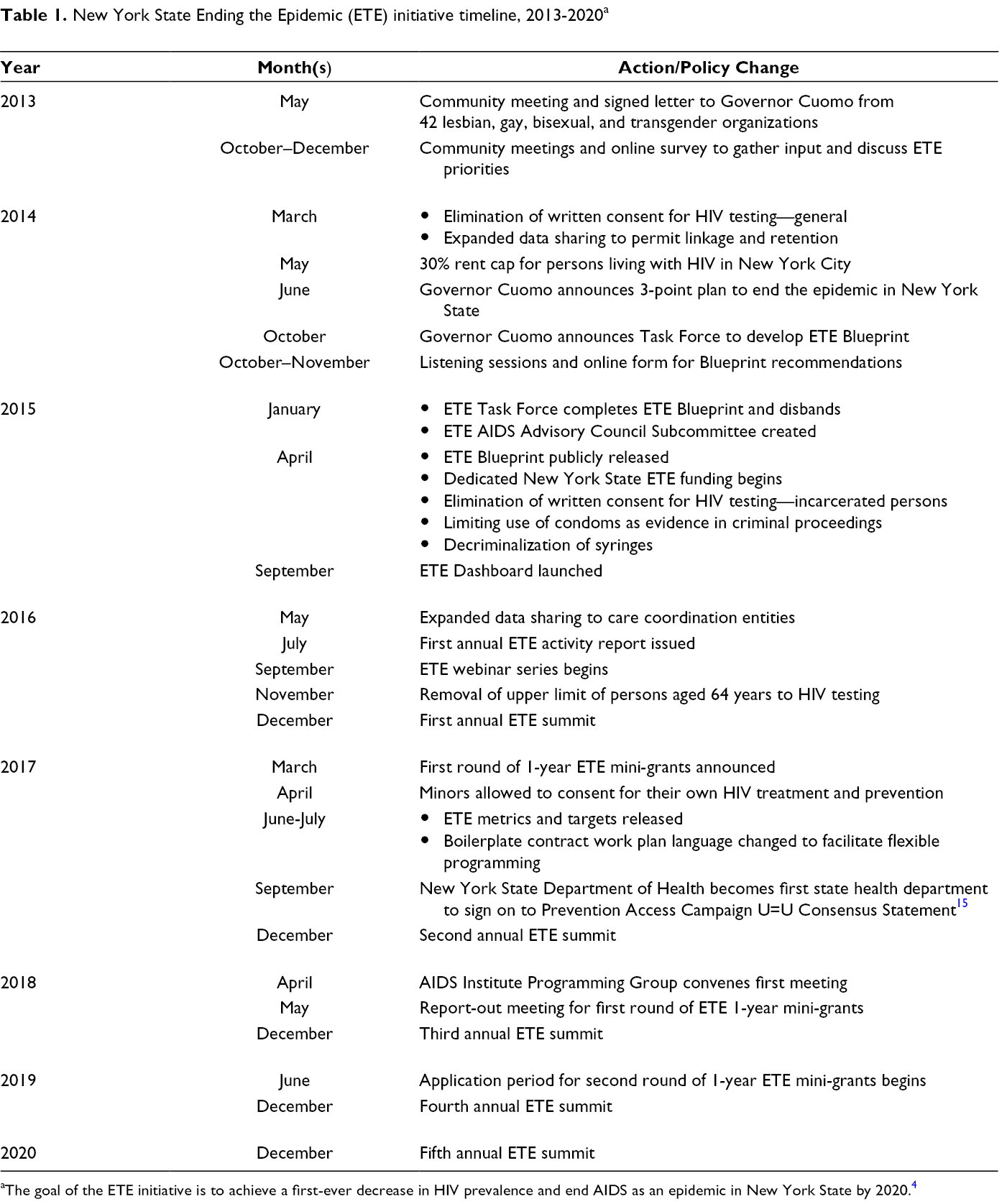
aThe goal of the ETE initiative is to achieve a first-ever decrease in HIV prevalence and end AIDS as an epidemic in New York State by 2020. 4
Effective Partnerships
The New York State ETE discussion began in the community. In May 2013, New York–based advocacy organizations convened community leaders, advocates, health care and social service providers, researchers, and government representatives to review the status of the HIV response in New York State and to discuss actions toward ending the AIDS epidemic in the state. 4 The meeting resulted in a letter to Governor Andrew M. Cuomo that catalyzed the ETE initiative in New York State. 4 The New York State Department of Health (NYSDOH) AIDS Institute then partnered with community leaders and the New York City Department of Health and Mental Hygiene to convene a meeting of more than 300 key stakeholders to gather input on defining what it means to “end AIDS” and what the key strategies for achieving an end of AIDS should look like for New York State. NYSDOH also gathered community input through an online survey that was administered during fall 2013 and targeted HIV service providers, the advocacy community, partnering agencies, and the general New York State population. NYSDOH received nearly 300 recommendations. A task force comprising 64 members from community, government, academia, and advocacy held 5 public meetings during 3 months beginning in October 2014 to process and synthesize this information and to produce the ETE Blueprint, which was officially accepted by Governor Cuomo and released in April 2015. 4 The ETE Blueprint serves as a roadmap for implementing the ETE initiative. Leveraging effective partnerships also plays a pivotal role in the implementation and evaluation of New York State’s ETE efforts. These partnerships are detailed later.
Innovation
Although the ETE initiative helped attract additional resources, ETE-specific funding composed a small percentage of New York State’s overall fiscal support for HIV prevention and care programming. Because prevention and care programming is managed by several divisions at NYSDOH, a centralized AIDS Institute Programming Workgroup was created to align New York State’s core programming with recommendations in the ETE Blueprint. The ability to target resources and permit programmatic direction changes mid-contract cycle in real time was accomplished through a modification of work plans for already funded HIV service providers. The centralized workgroup and efficient contracting enabled New York State to quickly redirect its resources to new and expanded programming to facilitate HIV testing, viral load suppression, and PrEP access.
Another area of innovation was the implementation of quick-strike mini-grants, for which a streamlined application process is used to fund 1-year, $30 000 projects designed to address ETE-related knowledge gaps and more closely align the research and HIV prevention and health care provider communities. The first cycle of mini-grants was completed in May 2018. Six of the 7 projects funded during this cycle focused on better understanding barriers to and facilitators of PrEP uptake in New York State. A second round of mini-grants, beginning in March 2020, focuses on reducing disparities in PrEP access and informing efforts to reduce late HIV diagnoses.
Evidence-Based Technical Package
Most successful public health programs are built on a set of interrelated and straightforward evidence-based interventions. 11 New York State’s ETE efforts leveraged evidence-based interventions in 3 areas: (1) HIV testing to identify undiagnosed persons, (2) improving viral suppression through quality-of-care and data-to-care approaches, and (3) facilitating access to PrEP and nPEP for persons who engage in high-risk behaviors, to prevent HIV acquisition. The approaches supported were those determined by the task force to be the most effective, feasible, sustainable, and scalable. 13,14 For example, NYSDOH expanded its data-to-care programming under ETE. Data to care uses surveillance data to identify and engage PLWH in care after initial HIV diagnoses or after they have fallen out of care. NYSDOH expanded its data-to-care capacity by deputizing staff members from community-based organizations to permit access to surveillance data and to grant deputized staff members the authority to engage HIV-positive persons in care. NYSDOH also created a rapid-response team to track new diagnoses in real time. The rapid-response team intervenes with medical providers and newly diagnosed persons, as necessary, to ensure linkage to HIV medical care within 7 days of diagnosis and to ensure viral suppression within 90 days of diagnosis. A detailed accounting of New York State’s ETE programming is available through its public-facing ETE dashboard. 12
Real-Time Performance-Based Measurement and Evaluation
Although tracking HIV prevalence—the main epidemiologic marker for ending AIDS—was already conducted annually, New York State’s ETE initiative outlines the need for expanded, enhanced, and transparent use of data to track and report progress. An ETE Metrics Committee comprising New York State and New York City health department staff members, researchers, service providers, consumers with lived experience, and advocates developed a set of core, population-level metrics along with ambitious targets for each metric. Where comparable National HIV/AIDS Strategy 16 metrics existed, the ETE Metrics Committee chose more ambitious targets, with progress prominently displayed on a public-facing online dashboard. 12
New York State also implemented research and evaluation efforts related to the ETE initiative. In addition to the ETE mini-grants, New York State contracted with academic partners to develop a computer simulation model to assess the extent to which New York State was on track to end AIDS and to inform program and policy implementation. 17 Results were used to inform program design and resource allocation.
Communication With Stakeholders
Timely and regular communication of ETE activities to stakeholders has been crucial to retain enthusiasm, momentum, and transparency throughout the ETE initiative; generate buy-in among stakeholders to support local implementation of ETE Blueprint recommendations; ensure locally appropriate ETE programming; and help focus programming in near–real time. External communication occurs through diverse channels, including the public-facing dashboard, public meetings of the New York State AIDS Advisory Council ETE Subcommittee and regional ETE committees, an ETE webinar series, and an annual ETE Summit. Communication has also occurred through recommendations from several population-specific subcommittees, the primary focus of which is to ensure that ETE Blueprint recommendations are tailored to the needs of priority population–specific groups (eg, women, black men who have sex with men, Native American persons, Latino gay and bisexual men, non–English-speaking migrants, seasonal farm workers and new immigrants, injection drug users, young and older adults living with HIV, and transgender and gender nonconforming persons). 13 Internal communication occurs through ETE-focused projects and meetings, through the NYSDOH AIDS Institute Programming Workgroup, and through an annual director’s update meeting.
Political Commitment
Strong political commitment has helped bring about legal and policy changes critical to New York State’s ETE efforts. Governor Cuomo convened the initial ETE Task Force, delivered its charge, and officially accepted the ETE Blueprint in a ceremony and press event held in New York City in April 2015. The governor’s early and direct involvement in the process has proven instrumental in securing buy-in and fostering partnerships across state and local governmental agencies, and his work with the advocacy community added legitimacy to ETE processes and initiatives.
Political commitment has also produced ETE-specific funding allocations, important for jumpstarting activities in key areas. The governor’s initiative added $20 million in ETE-specific funding to the state’s HIV prevention and care infrastructure (Figure).
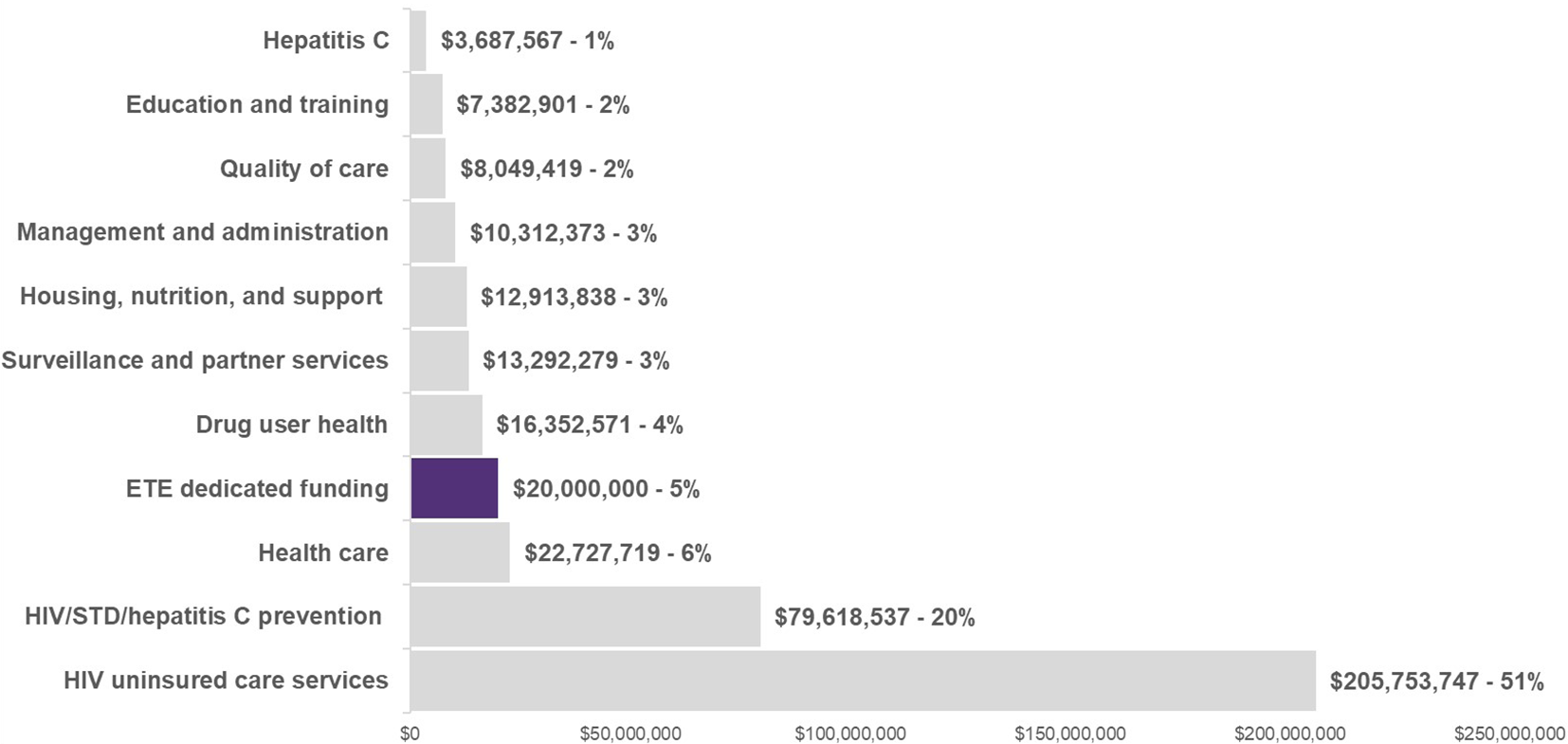
HIV funding by service category, New York State, 2017 (total funding: $400 090 951). Includes New York State and federal funding. New York State funding ($173 208 091) represents 43% of total funding but excludes $2.2 billion in Medicaid spending annually for HIV care and treatment. Excludes New York City Department of Health and Mental Hygiene funding for HIV care and treatment. Data source: Unpublished data from the Office of Contract Administration, New York State Department of Health AIDS Institute, 2018. Abbreviations: ETE, Ending the Epidemic; STD, sexually transmitted disease.
Political commitment and political will have been essential in accomplishing several legal and policy changes important to New York State’s ETE efforts, including eliminating the need for written consent for HIV testing for the general public (2014) 18 and incarcerated persons (2015) 19 ; requiring HIV testing to be offered in primary care to persons aged ≥65 (2016) (expanding the previous requirement of offering HIV testing to persons aged 13-64) 20 ; allowing minors to consent for their own HIV treatment and prevention (2017) 21 ; expanding data sharing to facilitate programming for linkage to and retention in care (2010, 22 2014, 23 and 2016 24 ); implementing a 30% rent cap for PLWH in New York City (2014) 25 ; limiting the use of condoms as evidence of prostitution in criminal proceedings (2015) 26 ; and reconciling criminal and public health law relative to syringes obtained through legal programming (2015). 27 These legal and policy changes have substantially affected the breadth, intensity, and timing of New York State’s evidence-based technical package for ETE. For example, New York State’s expanded data-sharing laws permit HIV surveillance information (identifiable data on thousands of PLWH who were not virally suppressed) to be shared with Medicaid managed care plans. New York State contracted with Medicaid managed care plans to improve rates of viral suppression; as a result, more than 40% of identified members achieved viral suppression within a brief follow-up period (unpublished data, AIDS Institute Office of Medicaid Policy and Health Care Financing, 2016). Many other legal and regulatory changes have been similarly effective and have served to substantially increase the effectiveness of HIV prevention and care programming in New York State. More information on each ETE-related legal or policy change is available from the Policy Tracker page on the New York State ETE dashboard. 12
New York State Progress on Ending AIDS
We measured progress toward ETE objectives in New York State with 13 metrics (Table 2). We describe results at pre-ETE baseline (2014) and at the halfway point (2017) and how those results compared with 2020 targets as of 2017 (Table 3). Statewide rather than citywide data are shown because ETE is a statewide initiative and because progress on the core ETE metrics is comparable between New York City and New York State.
Key metrics in the Ending the Epidemic initiative, a New York State, 2017
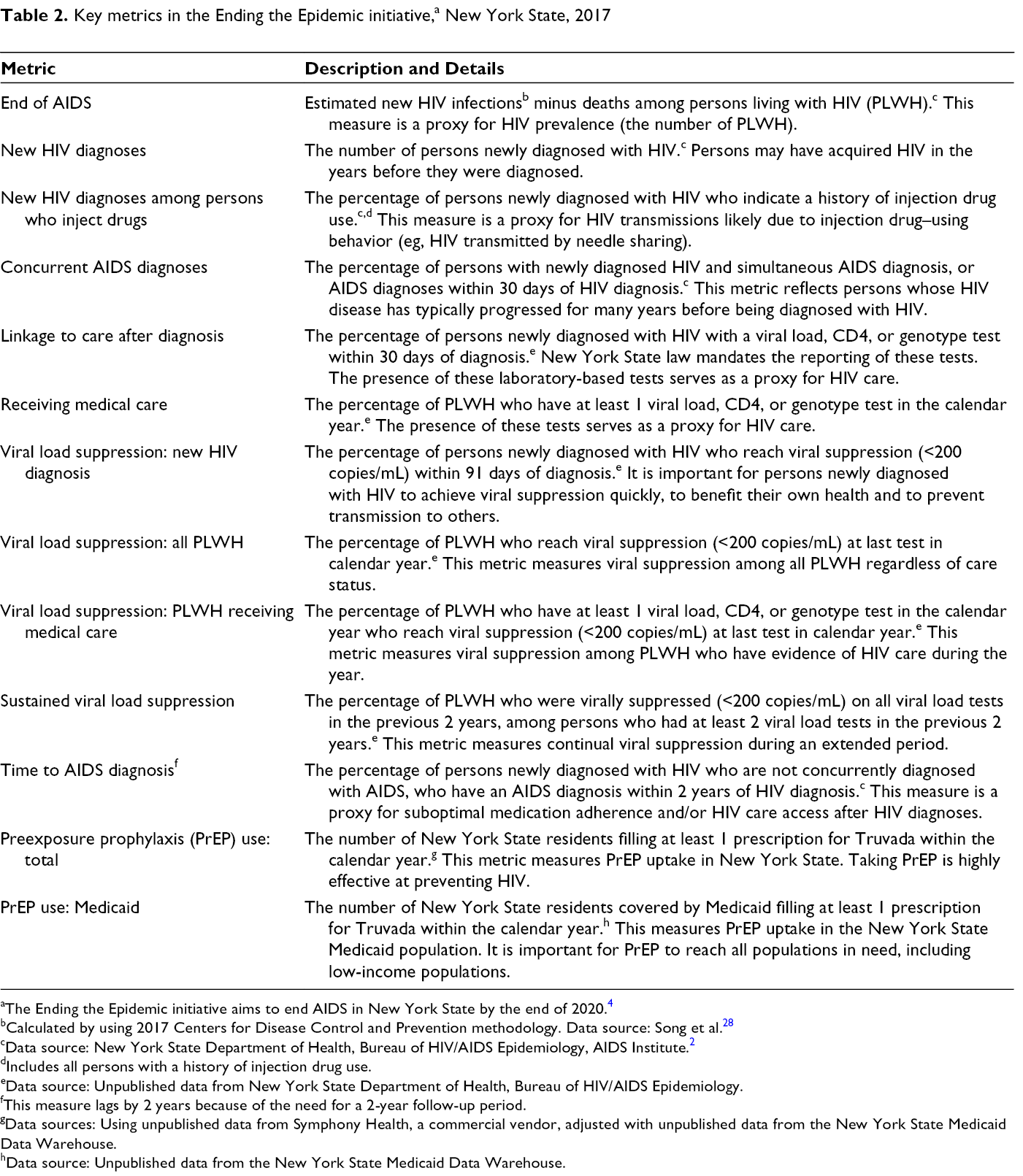
aThe Ending the Epidemic initiative aims to end AIDS in New York State by the end of 2020. 4
bCalculated by using 2017 Centers for Disease Control and Prevention methodology. Data source: Song et al. 28
cData source: New York State Department of Health, Bureau of HIV/AIDS Epidemiology, AIDS Institute. 2
dIncludes all persons with a history of injection drug use.
eData source: Unpublished data from New York State Department of Health, Bureau of HIV/AIDS Epidemiology.
fThis measure lags by 2 years because of the need for a 2-year follow-up period.
gData sources: Using unpublished data from Symphony Health, a commercial vendor, adjusted with unpublished data from the New York State Medicaid Data Warehouse.
hData source: Unpublished data from the New York State Medicaid Data Warehouse.
Target and actual results of key metrics in the Ending the Epidemic (ETE) initiative, a by year, New York State, 2014-2020
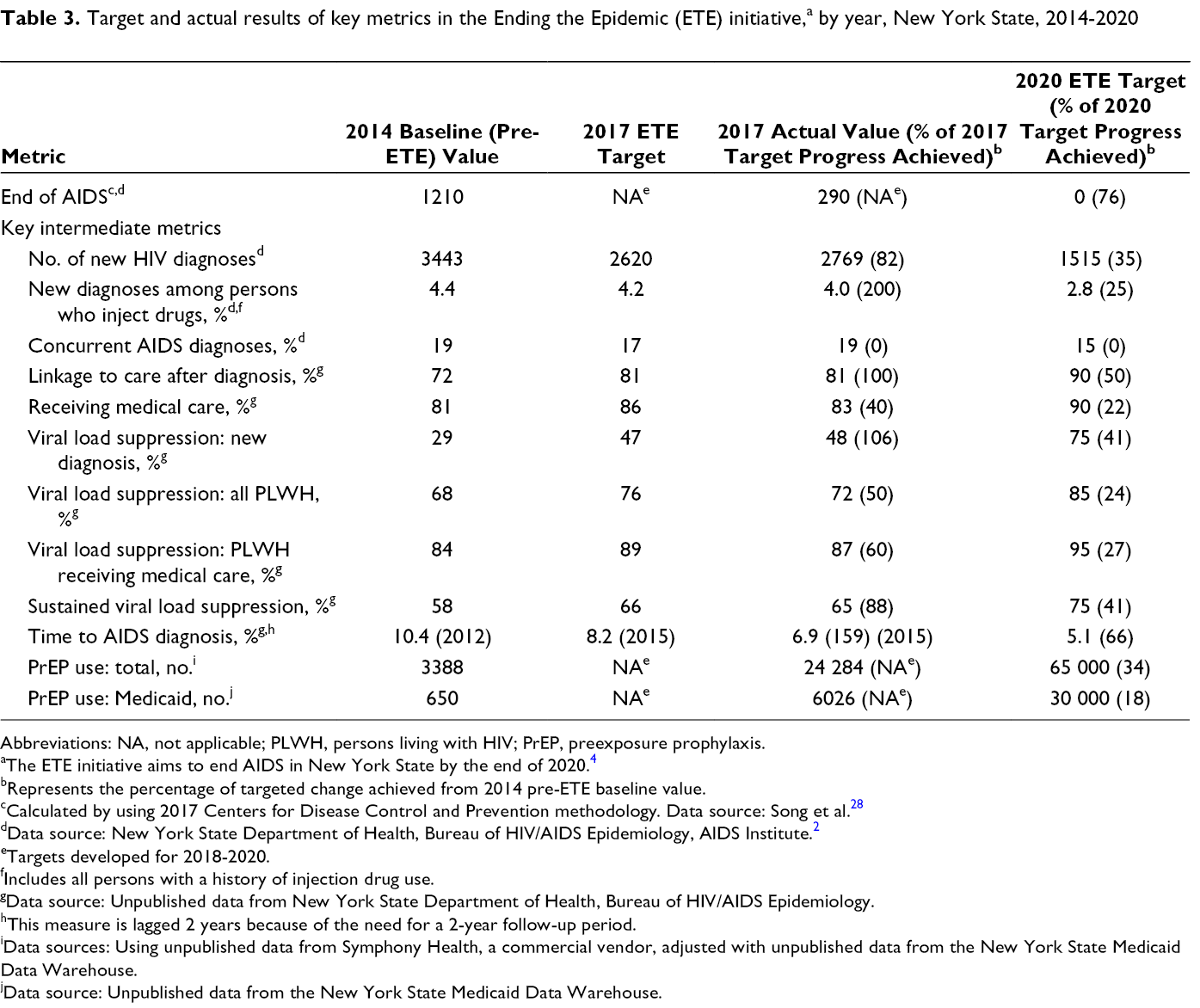
Abbreviations: NA, not applicable; PLWH, persons living with HIV; PrEP, preexposure prophylaxis.
aThe ETE initiative aims to end AIDS in New York State by the end of 2020. 4
bRepresents the percentage of targeted change achieved from 2014 pre-ETE baseline value.
cCalculated by using 2017 Centers for Disease Control and Prevention methodology. Data source: Song et al. 28
dData source: New York State Department of Health, Bureau of HIV/AIDS Epidemiology, AIDS Institute. 2
eTargets developed for 2018-2020.
fIncludes all persons with a history of injection drug use.
gData source: Unpublished data from New York State Department of Health, Bureau of HIV/AIDS Epidemiology.
hThis measure is lagged 2 years because of the need for a 2-year follow-up period.
iData sources: Using unpublished data from Symphony Health, a commercial vendor, adjusted with unpublished data from the New York State Medicaid Data Warehouse.
jData source: Unpublished data from the New York State Medicaid Data Warehouse.
Because ETE programming took time to initiate and because it continues to expand, we consider 35% to 40% of the 2020 target to be on track for any given ETE metric. In 2017, 76% of the 2020 target for ending AIDS had been achieved, providing strong evidence that New York State was on track to reach its primary ETE goal (Table 3). This assessment is bolstered by computer simulation modeling, which also found New York State to be on track to decrease HIV prevalence by the end of 2020. 17 With one exception, New York State has made some progress (18%-34% of 2020 target) on 5 metrics and substantial progress (≥35% of 2020 target) on 7 metrics. The exception is concurrent AIDS diagnoses, which increased over the baseline value. Lack of progress in this metric may be the result of increased efforts to ensure testing of persons with undiagnosed HIV. This metric, along with PrEP uptake among New York State’s highest-risk populations, will be the subject of continued discussion and increased programming through the end of 2020.
The 2020 ETE targets represent a noteworthy increase over historical trends in improvement achieved before the ETE initiative. Pre-ETE historical data of comparable length and measurement were available for 8 of the 13 ETE targets. For each metric, 2020 endpoint targets represent a substantially larger change than that realized in the comparable 6-year period preceding the ETE initiative. For example, new HIV diagnoses fell 24% from 2008 to 2014 (from 4545 to 3443). New HIV diagnoses will need to decrease 56% from 2014 to 2020 (from 3443 to 1515) for New York State to reach its ETE target. Comparably aggressive targets were set for each metric. New York State is outpacing its pre-ETE progress for 5 of 8 metrics with sufficient historical data to permit comparison (data not shown).
Lessons Learned
To our knowledge, this article is the first to comprehensively describe a jurisdiction’s ETE initiative and the first to report progress on key indicators and endpoint targets developed for measuring ETE success. Although several published studies have presented data on Getting to Zero initiatives in San Francisco 29,30 and Miami, 31 those studies did not describe progress related to predetermined targets associated with ETE programming. The only exception was a study in San Francisco that reported progress toward a single target of zero HIV-related stigma. 30
New York State’s ETE initiative embodies the 6 key areas identified as necessary for successful public health programming. 11 The ETE initiative thrives on expanded partnerships with the HIV advocacy community, local health departments, health care providers, and community-based organizations. Government programs increase their likelihood of success and sustainability when they are informed by a robust and engaged cohort of diverse stakeholders. 32 The partnerships in New York State’s ETE initiative have been key to securing political commitment, producing the ETE Blueprint, setting core metrics and targets, and ensuring locally appropriate ETE programming. Jurisdictions considering ETE initiatives should identify the key partnerships necessary for successful ETE implementation in their jurisdictions, including existing and potential partnerships.
Epidemiologic considerations are another important factor for ETE planning and implementation. New York State’s progress on new infections, new diagnoses, HIV care, and viral suppression in the years leading up to its ETE initiative was critical for setting a realistic timeline for ending AIDS. New York State also used epidemiologic data to prioritize its evidence-based technical package, which focuses on HIV testing, improving viral suppression, and facilitating access to PrEP, with an emphasis on communities most affected, such as sexual minority groups and persons of color. 13 Jurisdictions considering ETE initiatives should determine how their key HIV prevention and care metrics have trended during the past 5-10 years, overall, and among relevant demographic and transmission categories.
Jurisdictions contemplating ETE initiatives will need to develop unique innovations in many, if not all, key areas involved in successful public health programming. 11 New York State’s ETE initiative requires innovation through administration and contract management, core programming, evaluation, and performance management.
We recommend that jurisdictions incorporate real-time performance-based measurement and timely communication to key stakeholders into their ETE initiatives. These elements have been cornerstones of New York State’s ETE initiative and have helped to ensure accountability and transparency, keep stakeholders energized, fill knowledge gaps, ensure locally appropriate programming, and, through rapid-cycle evaluation approaches, 33 helped to focus ETE programming in near–real time. Involving key stakeholders in the development of ETE metrics and setting targets that are both ambitious and achievable are important. 34 Failure to set ambitious targets will fail to inspire, whereas setting unattainable targets could serve to quickly disillusion and derail efforts. Most recently, experts used mathematical modeling to deem the current federal administration’s goal of reducing HIV incidence by 90% by 2030 35 likely unachievable without massive scale-up and near-perfect coverage, raising questions about its likelihood of success. 36 It may also be important for jurisdictions to look beyond traditional HIV surveillance metrics when assessing impact. For example, New York State uses facility-produced treatment cascades to assess care use at the provider level, facilitating locally targeted programming. 37
Political support is also necessary to implement a successful ETE initiative. Political commitment realized at the highest level in New York State’s ETE initiative produced dedicated funding, leveraged buy-in, fostered partnerships, and helped to secure several policy and legal changes important to ETE. The advocacy community was instrumental in securing political commitment in New York State and may prove to be a valuable resource for doing so in other jurisdictions. The realization of strong political commitment and the active engagement of the advocacy community increased the level of visibility and accountability of ETE efforts. Both require regular updates on progress toward meeting key metrics and proposed solutions for addressing areas of concern. Transparency and accountability have been accommodated through the creation of a public-facing ETE dashboard and through frequent progress meetings with advocates and executive leadership staff members.
It would be difficult to overstate the amount of coordination that New York State’s ETE initiative has required. The NYSDOH AIDS Institute was heavily involved in, and usually the lead coordinator for, most of the activities or events listed in the ETE timeline. The breadth of activities under ETE has required that virtually every unit in the AIDS Institute become substantively involved in ETE programming. Beyond the challenge of finding the resources (primarily staff member time) to accommodate ETE activities, some units initially struggled to incorporate new ETE programming or to reconcile the ETE initiative with existing initiatives. These challenges were addressed, in part, by having each unit map its existing programming to New York State’s ETE Blueprint, by increasing the amount of cross-unit programming to reduce service duplication and increase synergy, and by permitting programmatic direction changes mid-contract cycle in near–real time. Staff members are also exposed to ETE-related messaging through frequent presentations, an annual ETE Summit, and an annual NYSDOH AIDS Institute director’s update.
The timing and characteristics of any jurisdiction’s ETE initiative must be tailored to its unique political and social climate, HIV epidemiology, fiscal resources, and existing network of HIV service providers. New York State had been priming itself to end AIDS through social, legal, and political reform; the advancement of epidemiologic systems and programming; increasing fiscal commitments; and the development of strong networks of HIV-focused and geographically dispersed service provision for many years leading up to the launch of the ETE initiative. As a result, New York State was able to set the aggressive target to decrease HIV prevalence in just 6 years. Longer ETE endpoints may be necessary for other jurisdictions, depending on their starting points.
Footnotes
Acknowledgments
The authors acknowledge Amy Kelly, Travis O’Donnell, and Wendy Patterson for reviewing and editing the article; Julie Ruttan for legal research; and Maria Welsh and Elham Pourtaher for formatting contributions. The authors also acknowledge the work of the New York State Ending the Epidemic Metrics Committee, which created the metrics used to track progress on ending AIDS as an epidemic in New York State.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.