
Abstract
Objectives:
American Indian/Alaska Native (AI/AN) adults use smokeless tobacco products (eg, chewing and dip tobacco) more often than other racial/ethnic groups do. Although US adults increasingly use potentially reduced exposure tobacco products (PREPs), such as electronic cigarettes and snus, no studies have examined the use of PREPs among AI/AN smokeless tobacco users. We examined associations between current PREPs use and smokeless tobacco–related measures, including cessation attempts and cotinine levels, in a sample of American Indian adults who currently use smokeless tobacco.
Methods:
We collected survey and tobacco biomarker data from 299 adult American Indian smokeless tobacco users at Cherokee Nation health care facilities and events in 2016 and 2017. We used multivariable analyses to determine associations between current PREPs use and smokeless tobacco–related characteristics.
Results:
Current PREPs users were younger, less likely to be married or living with a partner, less likely to report a chronic medical condition, and more likely to report other tobacco use than PREPs nonusers. Among participants with annual household incomes ≤$30 000, current PREPs users were less likely than PREPs nonusers to report a definite desire to quit smokeless tobacco (P = .02). PREPs use was not associated with planning to quit smokeless tobacco, past 12-month smokeless tobacco quit attempts, amount of smokeless tobacco used per week, cotinine levels, or scores on the Fagerström Test for Nicotine Dependence–Smokeless Tobacco.
Conclusions:
Our study suggests that American Indian smokeless tobacco users may not be using PREPs as a smokeless tobacco cessation aid. Future studies should take this finding into consideration when evaluating the role of PREPs use in smokeless tobacco cessation and in total tobacco cessation in this population.
Use of smokeless tobacco products (eg, chewing and dip tobacco) is linked to major health risks that include oral, esophageal, stomach, and pancreatic cancers and cardiovascular diseases. 1 -4 Although the percentage of the US population who smokes combustible cigarettes declined from 2005 to 2015, 5 use of smokeless tobacco has been steady since 2003, and the sales and availability of smokeless tobacco products increased from 2002 to 2012 in the United States. 6 -8 Although about 3% of all US adults use smokeless tobacco, more than 6% of American Indian/Alaska Native (AI/AN) adults use smokeless tobacco products. 9 Consequently, AI/AN adults are disproportionately affected by smokeless tobacco–related diseases. 10
US adults are increasingly using potentially reduced exposure tobacco products (PREPs), such as electronic cigarettes (e-cigarettes) and snus, a Swedish-style moist powder tobacco pouch containing fewer carcinogens than traditional smokeless tobacco products. 11 -13 Many adult combustible cigarette smokers use PREPs to reduce or quit smoking, 14 -16 even though these products are not approved by the US Food and Drug Administration for smoking cessation, 17 have unknown long-term health effects, 18,19 and have unclear smoking cessation effectiveness. 16,20 -22
Research on PREPs use has focused primarily on combustible cigarette smokers, and only a few studies have focused on smokeless tobacco users. Most studies of PREPs use by smokeless tobacco users have identified only the prevalence of PREPs use, not the associated factors. One study found that 29% of young adult smokeless tobacco users were also e-cigarette users, 23 and another study reported that the prevalence of e-cigarette use among smokeless tobacco users was 9.7%. 24 Yet another study found that, among male current smokeless tobacco users, 51% had ever tried snus and 29% were ever users of snus. 16 Although smoking cessation is often cited as the reason for PREPs use among smokers, 14 -16 it is unknown if smokeless tobacco users are using PREPs to quit smokeless tobacco. To our knowledge, no research has examined whether PREPs use influences or is associated with smokeless tobacco cessation efforts or other smokeless tobacco–related measures, including previous smokeless tobacco quit attempts, intentions to quit smokeless tobacco, smokeless tobacco consumption behaviors, nicotine levels, or nicotine dependence.
In addition to their higher prevalence of tobacco use, American Indians also have a higher prevalence of PREPs use than other racial/ethnic groups. 11 PREPs use among American Indian smokeless tobacco users is an important but unexplored area of research. The primary objective of our study was to explore associations between current PREPs use and definite desire to quit smokeless tobacco, definite plan to quit smokeless tobacco, past smokeless tobacco quit attempts, amount of smokeless tobacco used per week, cotinine levels, and nicotine dependence in a convenience sample of adult American Indian smokeless tobacco users.
Methods
Study Setting and Population
Oklahoma is home to 39 American Indian tribes and has one of the largest American Indian populations in the United States. 25 Cherokee Nation encompasses 14 counties in northeastern Oklahoma and operates the Cherokee Nation Health Services (CNHS). Patients must show proof of AI/AN descent, such as possession of a Certificate of Degree of American Indian or Alaska Native Blood (CDIB) card from a federally recognized tribe, to receive services at CNHS. Although Cherokee Nation citizens comprise the largest group of CNHS patients, persons from more than 300 AI/AN tribes are seen at CNHS facilities.
From December 1, 2016, to September 3, 2017, research staff members recruited participants from the waiting areas of 4 CNHS facilities located throughout the 14 counties within Cherokee Nation and a softball tournament during the Cherokee Nation Holiday, an annual cultural event that takes place in Tahlequah, Oklahoma. 26 Recruitment occurred on a total of 55 days during the study period. During recruitment, research staff members set up a table with information about the study. Research staff members also distributed flyers with information about the study, including eligibility requirements, at clinic and softball tournament registration desks. Prior to recruitment activities, staff members also displayed flyers with study information and eligibility requirements on bulletin boards around the clinics and on Cherokee Nation social media sites. Unless a participant approached the table first, staff members approached potential participants in the clinics and tournament areas and invited them to hear more about the study. Research staff members screened persons for eligibility only if they were interested in the study. Because of high traffic levels in the recruiting areas, the total number of potentially eligible persons could not be determined.
Persons were eligible for the study if they were aged ≥18, were current smokeless tobacco users, and answered affirmatively to the following questions: “Are you American Indian?” and “Do you have a CDIB card?” We defined current smokeless tobacco use as using smokeless tobacco at least 20 times in a lifetime and at least 1 day during the previous 30 days. Among the 323 persons screened for eligibility, 301 persons met the eligibility requirements for the study. Three hundred American Indian smokeless tobacco users consented to and provided survey and biomarker data for the study. For this analysis, we excluded 1 person because it was unclear whether he or she was a current PREPs user. Research staff members obtained informed consent from all participants, each of whom received a $25 gift card upon enrollment. After data collection was complete, and if participants asked about cessation, research staff members referred them to the 1-800 QUITNOW tobacco cessation quit line. In addition, research staff members referred them to their primary care provider for more information. Both the Cherokee Nation and the University of Oklahoma Health Sciences Center institutional review boards approved the study.
Survey Design and Implementation
We used validated measures to develop the cross-sectional survey, such as questions obtained from the American Indian Adult Tobacco Survey, Population Assessment of Tobacco and Health Study, and the National Adult Tobacco Survey. 27 -29 We designed the length of the paper-and-pencil questionnaire to ensure that participants could complete it in about 30 minutes. The survey included questions about sociodemographic characteristics, smokeless tobacco use, combustible cigarette smoking, e-cigarette use, snus use, other tobacco use, and nicotine dependence; tobacco, e-cigarette, and snus knowledge and attitudes; and health history.
Dependent Variables
We categorized a definite desire to quit smokeless tobacco use as either no/don’t know/not sure or yes. We categorized a definite plan to quit smokeless tobacco use within the next 30 days as either yes or no/don’t know/not sure. We categorized past 12-month smokeless tobacco quit attempts as either yes or no. We dichotomized smokeless tobacco cans/pouches used per week as ≥3 and <3.
Participants provided saliva for cotinine assays. 30 We measured salivary cotinine by using a Salimetrics Salivary Cotinine Enzyme-Linked Immunoassay kit (Salimetrics, State College, PA) using the standard protocol provided by the manufacturer, with a lower limit of sensitivity of 0.15 ng/mL. We ran all samples and standards in duplicate, with results reported as mean values of each duplicate set. We calculated results from a 4-parameter logistic curve fit produced using absorbance readings from known cotinine standards (0, 0.8, 2.5, 7.4, 22.2, 66.7, 200.0 ng/mL).
We used the Fagerström Test for Nicotine Dependence–Smokeless Tobacco (FTND-SLT) scale to assess nicotine dependence. The FTND-SLT scale is a self-rated 6-item questionnaire that evaluates the quantity of smokeless tobacco consumption, the compulsion to use, and dependence measures. 31,32 The scale ranges from 0 to 10, with higher scores indicating higher dependence on nicotine.
Independent Variable
We based current PREPs use (no/yes) on self-reported use of e-cigarettes or snus. We classified participants as current PREPs users if they had used e-cigarettes or snus, even once or twice, in the past 30 days.
Covariates
To control for potential confounding variables, we considered several covariates for all analyses. Demographic characteristics included age (18-44, ≥45), sex (male, female), education (<high school, high school/general education diploma, >high school), annual household income (≤$30 000, >$30 000), marital status (not married [ie, divorced, separated, widowed, or single] or married/living with a partner).
For health-related characteristics, respondents reported their general health as excellent, very good, good, fair, or poor, and results were dichotomized as excellent/good and fair/poor. Respondents self-reported a history of depression (no/yes). We dichotomized chronic medical conditions as no/yes based on a self-reported history of having any 1 of the following chronic conditions: cancer, cardiovascular or heart disease, diabetes, chronic obstructive pulmonary disease, or emphysema.
We categorized current combustible cigarette smoking as no/yes, with current combustible cigarette smoking defined as lifetime use of ≥100 combustible cigarettes and any past 30-day use. We based other tobacco use (no/yes) on reported daily, weekly, or monthly use of cigars, cigarillos, filtered cigars, hookahs, or dissolvable tobacco.
Statistical Analysis
We summarized continuous variables by using mean and standard deviation (SD) or median and interquartile range. We conducted comparisons of continuous variables between groups (current PREPs users vs PREPs nonusers) using 2-sample t tests for means or Wilcoxon rank-sum tests, the latter being used when the assumption of normality was questionable.
We summarized categorical variables as number (percentage). We conducted comparisons of categorical variables between groups by using the Pearson χ2 test of independence or the Fisher exact test, the latter being used when expected cell counts were <5. In multivariable analyses, we analyzed dichotomous outcomes by using logistic regression and continuous outcomes by using linear regression.
For all multivariable analyses of outcome variables, we assessed 2-way interactions terms for PREPS by age, sex, and annual household income and removed variables from the model via backwards selection when warranted (P < .05). After removing nonsignificant interaction terms, main-effect terms (eg, age, sex, annual household income, marital status, chronic medical condition, cotinine level, and other tobacco use) were subjected to backwards elimination by using the same criterion (P < .05). For all multivariable analyses of outcome variables, we retained PREPs and cigarette use variables as terms in the final model even if these 2 variables were not significant (P < .05). We performed stratified (on covariate) analyses after identifying significant interactions. When used as a predictor, cotinine levels were subjected to natural-log transformation. 33,34 All tests were 2-sided with P < .05 considered significant. We conducted all analyses by using R version 3.3.1. 35
Results
Of 299 adult American Indian smokeless tobacco users, 64 (21.4%) were current PREPs users, 43 (14.4%) used e-cigarettes, and 35 (11.7%) used snus. Compared with the 235 PREPs nonusers, current PREPs users were significantly younger (85.9% of PREPs users vs 53.2% of PREPs nonusers were aged 18-44; P < .001), less likely to be married/living with a partner (48.4% vs 63.0%; P = .04), and less likely to report having a chronic medical condition (22.6% vs 41.0%; P = .03). Current PREPs users also were significantly more likely than PREPs nonusers to report current cigarette use (73.4% vs 43.4%; P < .001) and current use of other noncigarette tobacco products (23.4% vs 8.1%; P < .001; Table 1).
Demographic and smokeless tobacco–related characteristics, stratified by PREPsa use, among adult American Indian smokeless tobaccob users in Cherokee Nation, 2016-2017c
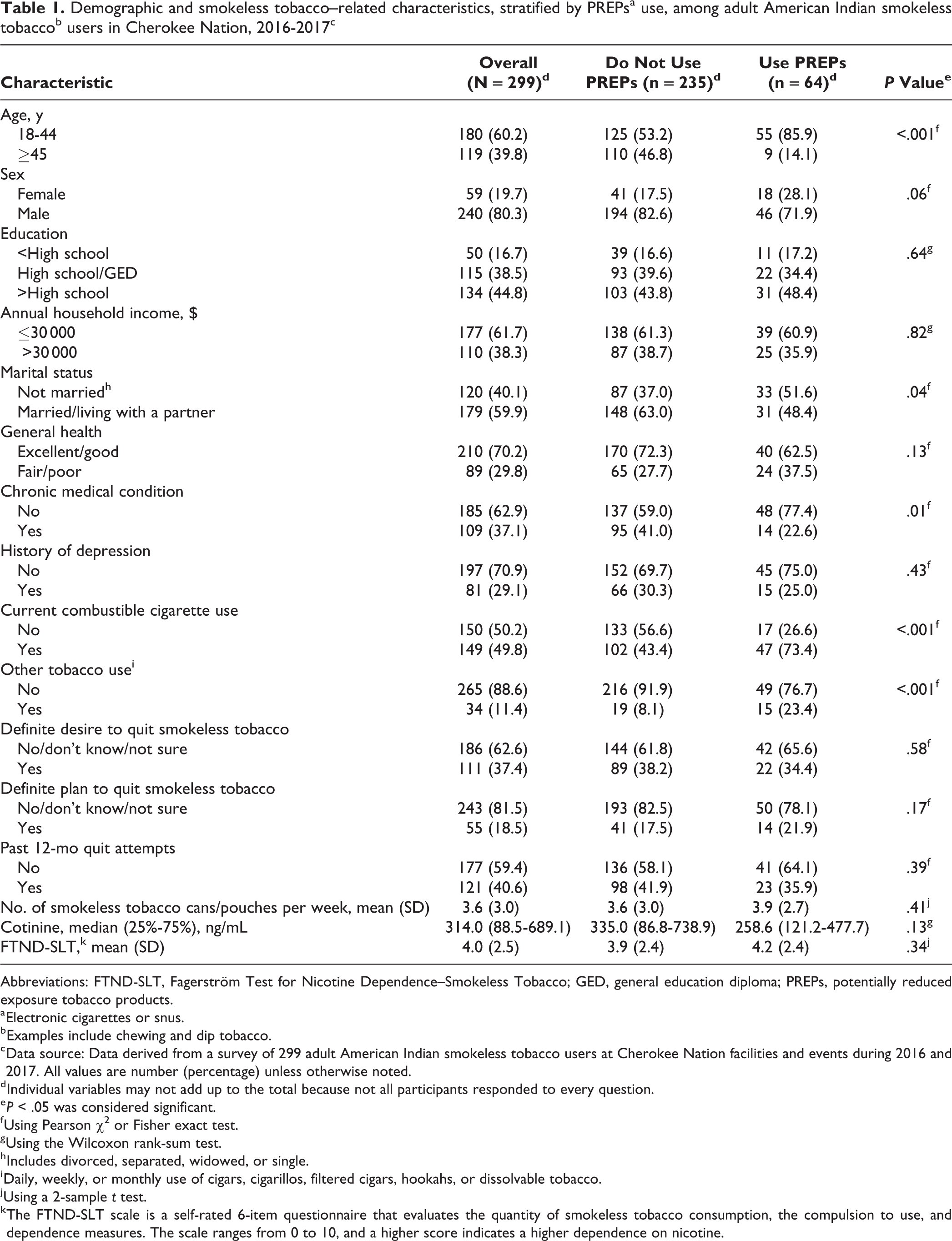
Abbreviations: FTND-SLT, Fagerström Test for Nicotine Dependence–Smokeless Tobacco; GED, general education diploma; PREPs, potentially reduced exposure tobacco products.
a Electronic cigarettes or snus.
b Examples include chewing and dip tobacco.
c Data source: Data derived from a survey of 299 adult American Indian smokeless tobacco users at Cherokee Nation facilities and events during 2016 and 2017. All values are number (percentage) unless otherwise noted.
d Individual variables may not add up to the total because not all participants responded to every question.
e P < .05 was considered significant.
f Using Pearson χ2 or Fisher exact test.
g Using the Wilcoxon rank-sum test.
h Includes divorced, separated, widowed, or single.
i Daily, weekly, or monthly use of cigars, cigarillos, filtered cigars, hookahs, or dissolvable tobacco.
j Using a 2-sample t test.
k The FTND-SLT scale is a self-rated 6-item questionnaire that evaluates the quantity of smokeless tobacco consumption, the compulsion to use, and dependence measures. The scale ranges from 0 to 10, and a higher score indicates a higher dependence on nicotine.
We found a significant interaction between PREPs use and annual household income (P = .01) (Table 2). Among participants with an annual household income ≤$30 000, current PREPs users were significantly less likely than PREPs nonusers to report a definite desire to quit smokeless tobacco (odds ratio = 0.35; 95% confidence interval, 0.15-0.80; P = .02).
Multivariable logistic regression analysis of definite desire to quit smokeless tobacco, stratified by annual household income, among adult American Indian smokeless tobaccoa users in Cherokee Nation, 2016-2017b,c
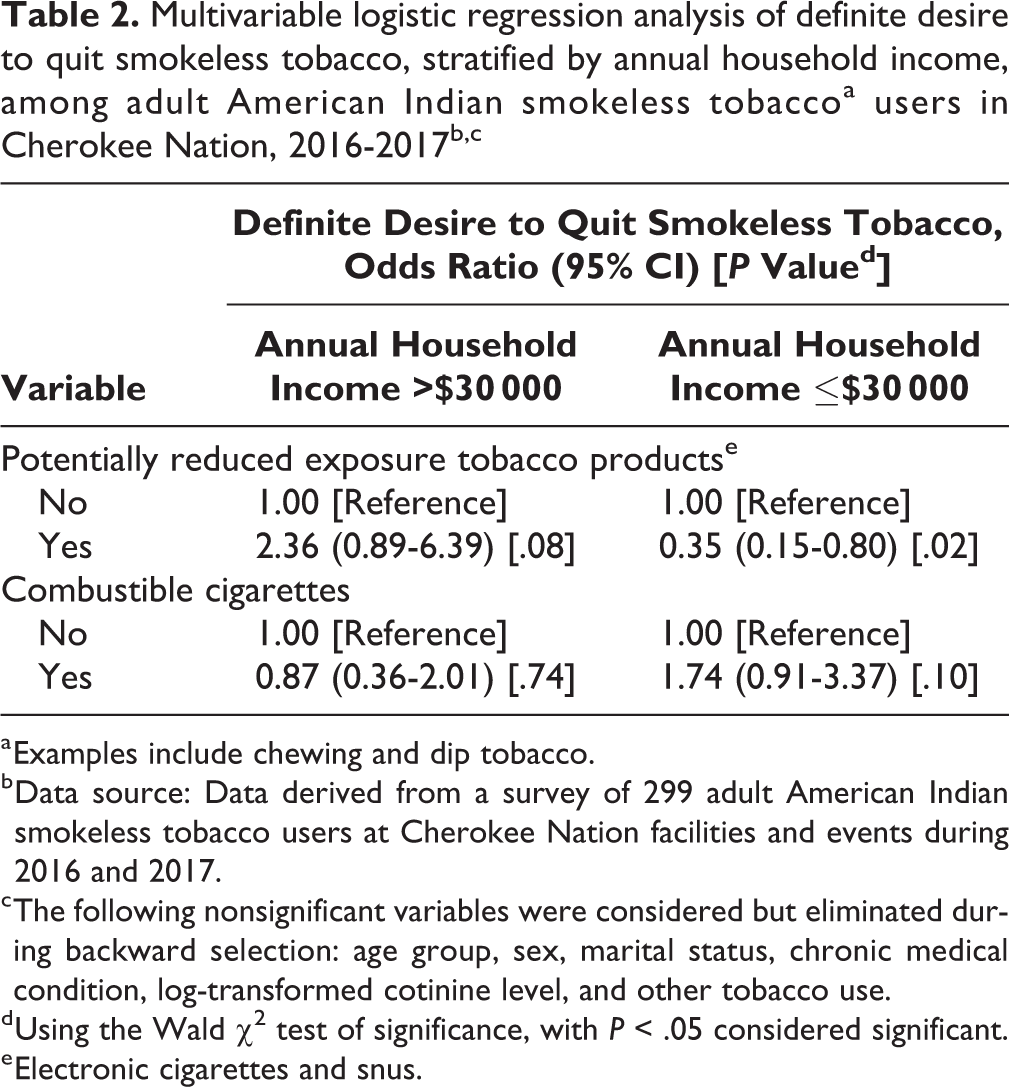
a Examples include chewing and dip tobacco.
b Data source: Data derived from a survey of 299 adult American Indian smokeless tobacco users at Cherokee Nation facilities and events during 2016 and 2017.
c The following nonsignificant variables were considered but eliminated during backward selection: age group, sex, marital status, chronic medical condition, log-transformed cotinine level, and other tobacco use.
d Using the Wald χ2 test of significance, with P < .05 considered significant.
e Electronic cigarettes and snus.
In the multivariable analyses evaluating current PREPs use and a definite plan to quit using smokeless tobacco, the overall interaction between current PREPs use and age on definite plans to quit smokeless tobacco was significant (P = .02; Table 3).
Multivariable logistic regression analysis of definite plan to quit smokeless tobacco, stratified by age, among adult American Indian smokeless tobaccoa users in Cherokee Nation, 2016-2017b,c,d
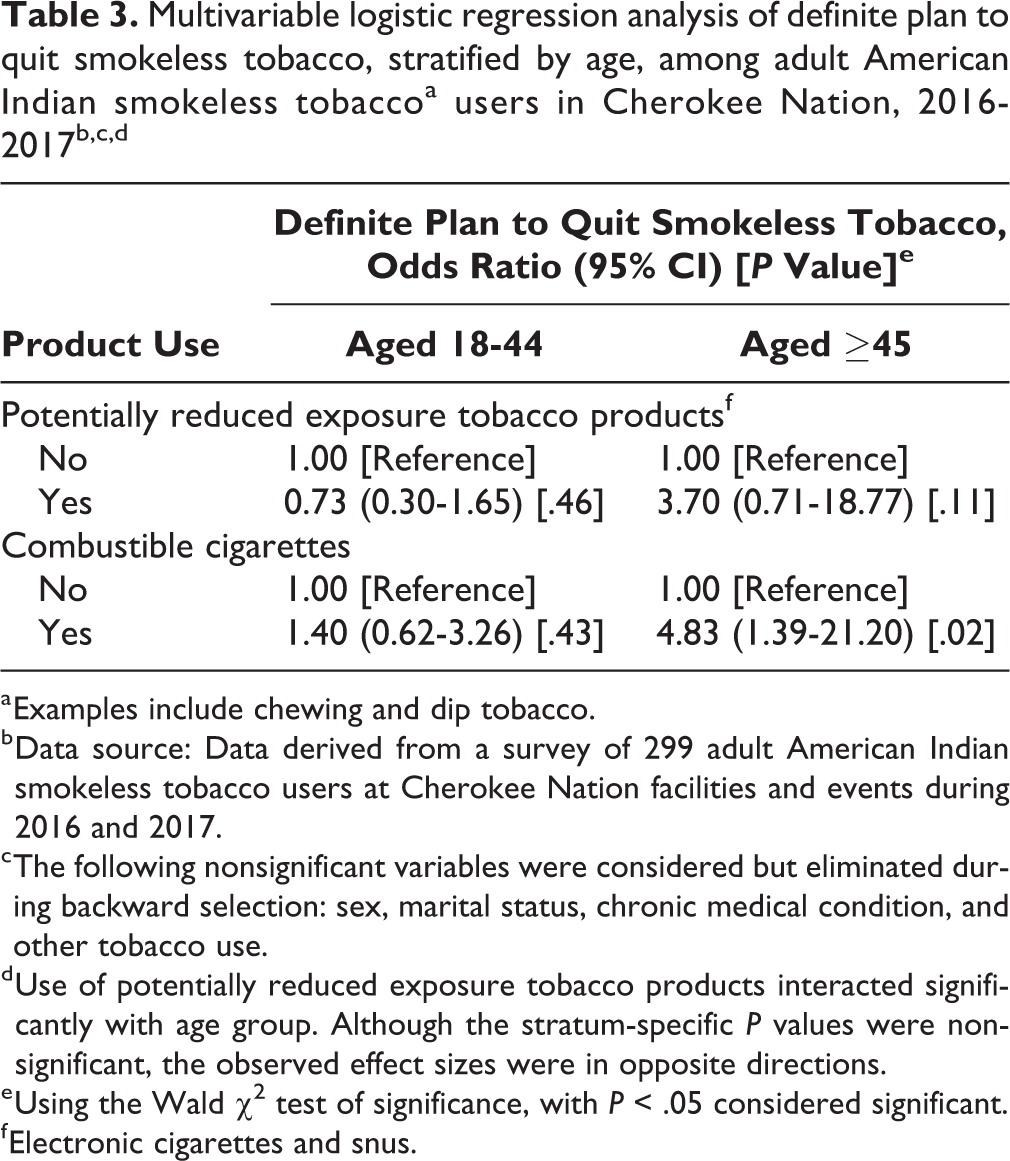
a Examples include chewing and dip tobacco.
b Data source: Data derived from a survey of 299 adult American Indian smokeless tobacco users at Cherokee Nation facilities and events during 2016 and 2017.
c The following nonsignificant variables were considered but eliminated during backward selection: sex, marital status, chronic medical condition, and other tobacco use.
d Use of potentially reduced exposure tobacco products interacted significantly with age group. Although the stratum-specific P values were nonsignificant, the observed effect sizes were in opposite directions.
e Using the Wald χ2 test of significance, with P < .05 considered significant.
f Electronic cigarettes and snus.
In the multivariable analyses evaluating the associations of current PREPs use with 4 outcomes—past 12-month smokeless tobacco quit attempts, amount of smokeless tobacco cans/pouches used per week, cotinine levels, and FTND-SLT scale score—current PREPs use was not significant after adjusting for potential confounders and effect modifiers (Table 4).
Multivariable analyses of smokeless tobacco–related variables among adult American Indian smokeless tobaccoa users in Cherokee Nation, 2016-2017b,c
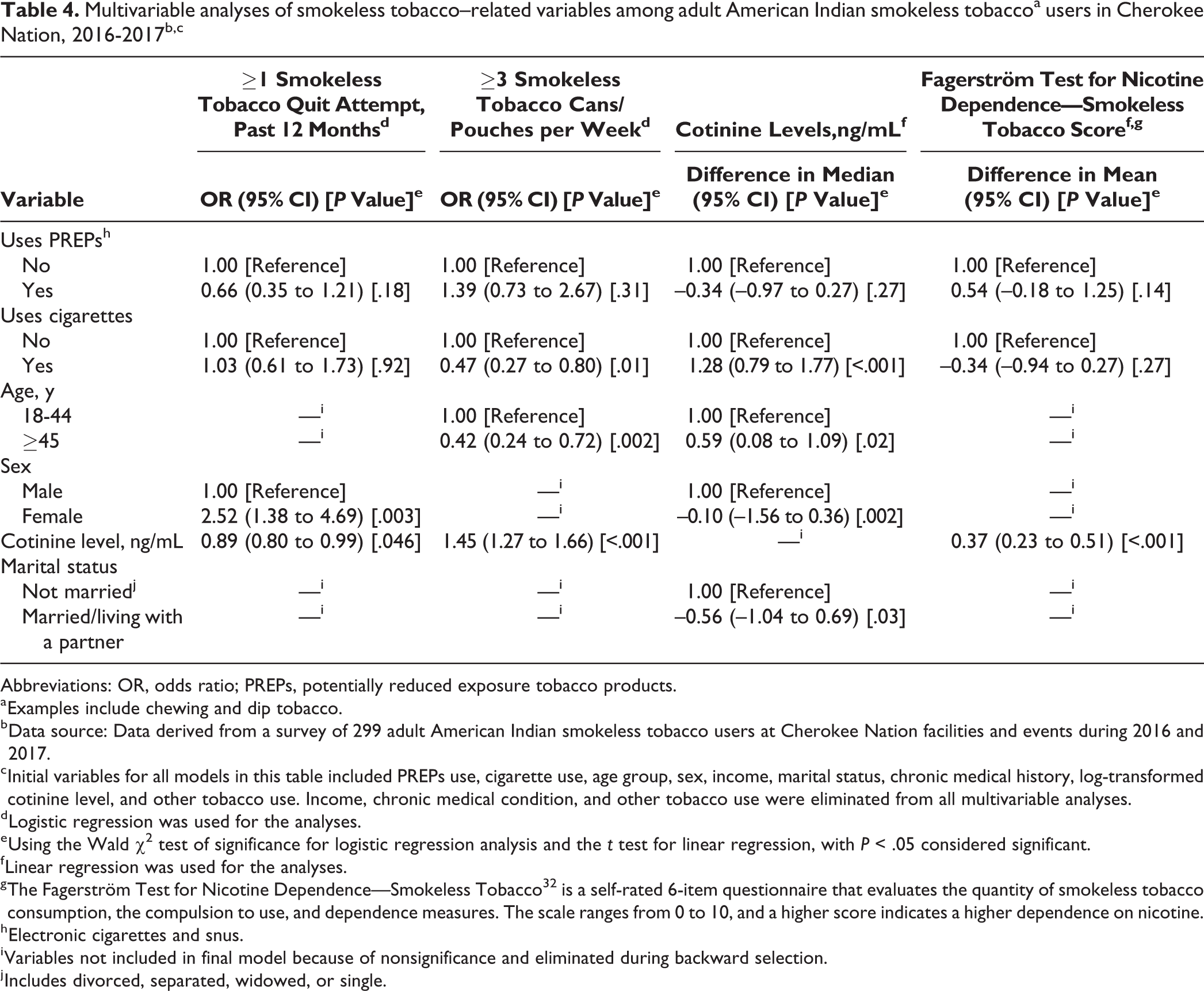
Abbreviations: OR, odds ratio; PREPs, potentially reduced exposure tobacco products.
a Examples include chewing and dip tobacco.
b Data source: Data derived from a survey of 299 adult American Indian smokeless tobacco users at Cherokee Nation facilities and events during 2016 and 2017.
c Initial variables for all models in this table included PREPs use, cigarette use, age group, sex, income, marital status, chronic medical history, log-transformed cotinine level, and other tobacco use. Income, chronic medical condition, and other tobacco use were eliminated from all multivariable analyses.
d Logistic regression was used for the analyses.
e Using the Wald χ2 test of significance for logistic regression analysis and the t test for linear regression, with P < .05 considered significant.
f Linear regression was used for the analyses.
g The Fagerström Test for Nicotine Dependence—Smokeless Tobacco 32 is a self-rated 6-item questionnaire that evaluates the quantity of smokeless tobacco consumption, the compulsion to use, and dependence measures. The scale ranges from 0 to 10, and a higher score indicates a higher dependence on nicotine.
h Electronic cigarettes and snus.
i Variables not included in final model because of nonsignificance and eliminated during backward selection.
j Includes divorced, separated, widowed, or single.
Discussion
Our study found that about 21% of the sample of American Indian smokeless tobacco users also currently used ≥1 PREPs, 14% currently used e-cigarettes, and 12% currently used snus. The prevalence of ever trying snus, in our study population, was 37.8%. The prevalence of current e-cigarette use in our study was lower than in a study of university students, which found that 29% of smokeless tobacco users used e-cigarettes, 23 but higher than in a nationwide study of working adults, which found that 9.7% of smokeless tobacco users used e-cigarettes. 24 In our sample, the prevalence of ever trying snus was lower than in a study conducted in 2 US cities, in which young male adult smokers were oversampled, that reported 51% had ever tried snus. 16 One possible reason for such differences in the prevalence of PREPs product use between our study and other studies may be related to the age of the study participants. In our study, the mean age among participants was 41.2. The use of e-cigarettes and snus has been shown to be more common among younger age groups, 16,36,37 even among AI/ANs. 38 Therefore, it is not unexpected that other studies found a higher prevalence of use than our study. However, compared with the nationwide study of smokers 23 and e-cigarette use, 24 our sample had a higher prevalence of current e-cigarette use.
In our sample, the characteristics of current PREPs users differed from those of PREPS nonusers. Among participants with an annual household income ≤$30 000, current PREPs users were significantly less likely than PREPs nonusers to report having a definite desire to quit smokeless tobacco. Yet, among participants with an annual household income >$30 000, current PREPs users were more likely than PREPs nonusers to report a definite desire to quit smokeless tobacco. Current PREPs use was not associated with other smokeless tobacco–related outcomes, including past quit attempts, cotinine levels, amount of smokeless tobacco used, or nicotine dependence.
Although additional research would be needed to better understand our findings, the sample of persons in our study may not have been using PREPs as a tobacco cessation aid but instead may have been using PREPs as another form of tobacco or nicotine product. In our sample, which comprised only smokeless tobacco users, almost 74% of current PREPs users were also current combustible cigarette smokers, whereas only 43% of PREPs nonusers were also current combustible cigarette smokers. We also found that current PREPs users were more likely than non-PREPS users to report currently using other noncigarette tobacco products. Studies have found that PREPs users were more likely than PREPS nonusers to report polytobacco use, or the concurrent use of ≥2 tobacco products. 39 -42 Use of PREPS as another form of tobacco or nicotine product rather than as a cessation aid may be especially true among lower-income persons; our study indicated that lower-income participants who currently used PREPs were less likely than lower-income participants who did not use PREPs to report a definite desire to quit smokeless tobacco. This finding suggests that low-income persons may not have been using PREPs as a smokeless tobacco cessation aid because they were less likely to report a definite desire to quit smokeless tobacco. A previous study, among combustible cigarette smokers, found that higher-income participants were more likely than lower-income participants to use e-cigarettes as a smoking cessation aid. 43 However, similar research has not been conducted among smokeless tobacco users. The higher likelihood of polytobacco use among current PREPs users than among PREPS nonusers in our sample raises an important issue about the effect of PREPs use on overall tobacco cessation. Future studies are needed to assess the effect of PREPs use not only on smoking cessation but also on total tobacco cessation among polytobacco users.
Limitations
This study had several limitations. First, this study was a cross-sectional analysis; therefore, causality could not be determined. Second, study participants were from a clinic-based convenience sample and not from a sample of the general population. Therefore, selection bias for those who more frequently use health care may have affected the generalizability of our results. However, the advantage of the clinic-based sampling we used was that this primary care setting could serve as an important platform for tobacco cessation services for smokeless tobacco users and an important location for research on this understudied topic. Third, survey data were self-reported and subject to recall bias. We did not survey former smokeless tobacco users and could not assess whether former smokeless tobacco users might have used PREPs successfully for cessation. Surveying this group could provide valuable insight into whether PREPs could be successfully used as a cessation aid in this population. Finally, we defined the use of PREPs as being any use within the past 30 days and did not account for regularity of use. Frequency of PREPs use may have implications for smokeless tobacco cessation.
Conclusions
Our study suggests that PREPs use has a negative association with a definite desire to quit smokeless tobacco among low-income American Indian adults. Furthermore, PREPs use was not associated with other smokeless tobacco cessation behaviors, nicotine dependence, or cotinine levels, and current PREPs users were more likely than PREPS nonusers to be current polytobacco users. These findings may have implications for future studies evaluating the role of PREPs use and overall tobacco cessation among American Indian adults who use smokeless tobacco products. This area of research is important, because American Indian adults have a consistently higher prevalence of both combustible cigarette use and smokeless tobacco use and shoulder a disproportionate burden of tobacco-related morbidity and mortality. Gaining a clear understanding of whether or how PREPS use might reduce this burden should be a public health priority.
Footnotes
Acknowledgments
The authors acknowledge research staff members at the University of Oklahoma and University of Oklahoma Health Sciences Center, as well as staff members at Cherokee Nation, for their support.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Justin D. Dvorak receives salary and equity interests from Bayesic Technologies, LLC.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was supported by grants U5GM104938 and P20CA202921, Sub #5625, and 5P20CA202923 from the National Institutes of Health.