
Abstract
Objectives:
Cognitive difficulties or impairment may be an early step in the development of dementia. Several modifiable risk factors for cardiovascular disease (CVD) may also increase the risk of dementia. The objective of our study was to compare adults with subjective cognitive impairment (SCI), using the Behavioral Risk Factor Surveillance System (BRFSS) cognitive disability measure, with adults who reported CVD.
Methods:
We examined data on 3 key outcomes among 302 008 adult respondents aged ≥45 in the 2017 BRFSS: respondents with SCI only, respondents with CVD only, and respondents with both conditions. We compared measures of disability, quality of life, access to health care, and a composite measure of the following 7 risk factors: current smoking, diabetes, high cholesterol, hypertension, inadequate fruit and vegetable consumption, obesity, and sedentary lifestyle. We also estimated population-attributable risk (PAR).
Results:
Among respondents, 7.9% reported SCI only, 11.1% reported CVD only, and 3.2% reported both conditions, with differences by age and sex. Adults with SCI only were more likely than adults with CVD only to report other disability, worse access to health care, and poorer quality of life, even though adults with CVD were older. Compared with adults with neither condition, adults with any of the 3 outcomes were more likely to report having each of the 7 risk factors; we found a linear association with an increasing number of risk factors. Five or 6 risk factors contributed to PARs for each of the 3 key outcomes. PARs for SCI only were highest for ever smoking (17.2%) and sedentary lifestyle (12.8%), whereas for CVD only, PARs were highest for hypertension (35.5%) and high cholesterol (22.9%).
Conclusion:
Despite differences between adults with SCI and adults with CVD in several demographic and health-related measures, the overall similarity in PARs for SCI and CVD suggests potential benefits from using effective CVD interventions to address SCI.
Keywords
Cognitive difficulties or impairment may be an early step in the development of dementia, including Alzheimer’s disease. 1 Approximately 5.8 million Americans were living with Alzheimer’s disease in 2019. 2 If Alzheimer’s disease were diagnosed in the early stages of cognitive impairment, it could save an estimated >$7 trillion in health care and long-term care costs. 2 When cognitive impairment worsens over time, it is usually referred to as cognitive decline. Not all cognitive impairment worsens or progresses to dementia (Alzheimer’s disease or other), especially when the impairment is due to treatable causes, such as depression or the side effects of medication. 2
Several modifiable risk factors for cardiovascular disease (CVD) have also been found to increase the risk of dementia. 3 -6 One study of 6 such risk factors (current smoking, depression, diabetes, hypertension, obesity, and sedentary lifestyle) documented a dose–response gradient between an increase in the number of risk factors and rates of cognitive decline and CVD. 3 Another study estimated that half of all Alzheimer’s disease cases were attributable to 7 risk factors: cognitive inactivity or low educational attainment, depression, diabetes, midlife hypertension, midlife obesity, physical inactivity, and smoking. 4 A study in 2019 estimated the population-attributable risk (PAR) for 7 CVD risk factors (substituting high cholesterol and inadequate fruit and vegetable consumption for depression and low level of education) and found that about 60% of CVD and 52% of cognitive impairment was attributable to these risk factors, with hypertension contributing the most to CVD and smoking contributing the most to cognitive impairment. 7
The objective of this study was to compare adults with cognitive impairment, using the Behavioral Risk Factor Surveillance System (BRFSS) cognitive disability measure, 8,9 with adults who reported CVD. Specific objectives were (1) to compare the mutually exclusive categories of adults with CVD only, subjective cognitive impairment (SCI) only, and both conditions on a number of health-related measures; (2) to test the hypothesis that SCI has a linear association with CVD risk factors similar to the association shown for cognitive decline, dementia, and CVD 3 ; and (3) to estimate the PAR contributed by each risk factor to the 3 key outcomes (CVD only, SCI only, and both conditions).
Methods
We used publicly available 2017 BRFSS data from 315 397 adults aged ≥45 from all 50 states and the District of Columbia. The BRFSS is a large, ongoing, representative, state-based telephone survey of noninstitutionalized adults. 10 Data were weighted to account for the probability of selection and further adjusted to be representative of the total adult population of each state by age, race, ethnicity, sex, marital status, education, home ownership, and type of telephone service. The median response rate for cell phone and landline telephone surveys combined was 47.2%, ranging from 33.9% to 61.1%. 11 We also used 2015 BRFSS data from 35 states (N = 147 863 adults aged ≥45) that included a question on cognitive decline, so that we could compare our measure of cognitive impairment with that measure of cognitive decline.
Measures
The BRFSS has used the US Census Bureau’s standardized cognitive disability question 12,13 on all telephone surveys since 2013. 8,9 The question is one of several measures used for monitoring various types of disability, 14 and it is now required on all federal surveys under the Affordable Care Act. 12,13 The question is, “Because of a physical, mental, or emotional condition, do you have serious difficulty concentrating, remembering, or making decisions?” Respondents who answer yes to this question are considered to have SCI. This question appears to be consistent with the conclusions and recommendations for a measure of cognitive impairment from the Subjective Cognitive Decline Initiative Working Group, 15,16 but the measure should not be considered cognitive decline because the question did not include a time frame. Respondents who reported that they had ever been told by a physician, nurse, or other health professional that they had had a heart attack, angina, coronary heart disease, or a stroke were considered to have CVD. We chose to study adults aged ≥45 because only 2918 respondents aged 18-44 reported CVD. We grouped respondents into the following mutually exclusive categories: adults with CVD only (n = 37 110), adults with SCI only (n = 21 891), adults with both conditions (n = 9259), and adults with neither condition (n = 233 748); 13 389 respondents were missing values for ≥1 measure.
Demographic measures included sex, age (45-54, 55-64, 65-74, and ≥75), self-reported race/ethnicity (Hispanic of any race and non-Hispanic white, black or African American, American Indian/Alaska Native, Asian/Pacific Islander, and other), education (college graduate, some college, high school graduate, and <high school graduate), and annual household income (unknown, ≥$75 000, $50 000-$74 999, $25 000-$49 999, $15 000-$24 999, and <$15 000).
We created a composite risk factor measure on the basis of 7 risk factors used by the American Heart Association 17 and in a previous study 7 : current smoking, diabetes, high cholesterol, hypertension, inadequate fruit and vegetable consumption (based on responses to 5 questions and defined as consuming a combination of fruit and vegetables, excluding fried potatoes, <5 times per day), obesity, and sedentary lifestyle. We used this risk factor measure as an 8-level measure (from 0 to 7). For estimates of PAR, we substituted lifetime smoking for current smoking.
Additional health-related measures included the following: 3 measures of disability (difficulty walking or climbing stairs, bathing or dressing, and doing errands alone), 8 inability to work (in response to a question on employment status, for which response options were employed, self-employed, out of work, homemaker, student, retired, or unable to work), health care access (having health insurance [yes/no] and unable to see a physician in past year because of cost [yes/no]), and 5 quality of life measures: a diagnosis of depression, health status (fair or poor vs excellent, very good, or good), frequent mental distress (≥14 days in past month), frequent physical distress (≥14 days in past month), and frequent activity limitation (≥14 days in past month).
Statistical Analysis
We analyzed data in 2019 by using Stata version 14.1, 18 which accounted for the complex sample design of the BRFSS and used the landline/cell phone weight. We excluded respondents who refused to answer or answered “don’t know/not sure” for any component (eg, risk factor) of a measure from analysis involving that measure. This exclusion resulted in the maximum number of respondents for the measure with the mutually exclusive groups of CVD only, SCI only, both conditions, and neither condition (N= 302 008) and for the composite measure of 7 risk factors (n = 258 468).
We tabulated weighted prevalence and 95% confidence intervals (CIs) for SCI only, CVD only, and both conditions by selected demographic and health-related measures. We made direct comparisons by reporting the percentage of adults in each group (SCI only, CVD only, both conditions, and neither condition). We used the Pearson χ2 test with an α of .05 to determine significant differences among groups. Logistic regression used SCI only, CVD only, and both conditions as the 3 key outcomes and included the demographic and risk factor measures plus the measure on whether the respondent was unable to see a physician because of cost. We also added measures of disability, quality of life, and being unable to work one at a time to the logistic regression models. When including the composite measure to test the hypothesis that SCI showed a dose–response gradient with the 7 risk factors, we combined data on respondents who reported 6 or 7 risk factors because of the small number of respondents who reported all 7 risk factors. We estimated PAR in Microsoft Excel according to Levin’s formula 19 using adjusted odds ratios (aORs). Logistic regression models included all 7 risk factors, using “ever smoked in lifetime” instead of current smoking. In PAR estimations, we included only risk factors found in other studies to be causally associated with the outcome. 7 A combined PAR was computed by using the following formula 4 to avoid totals >100%: combined PAR = (1 – [1 – PAR 1] × [1 – PAR 2] × [1 – PAR 3] ×…[1 – PAR 7]).
Results
Unadjusted Results
For the weighted sample of respondents aged ≥45 in all 50 states and the District of Columbia, 47.1% were male, 71.8% were non-Hispanic white, 38.4% were aged ≥65, 13.7% had <high school education, and 9.0% had an annual household income <$15 000. Prevalence rates for the risk factors were 14.6% for current smoking, 17.6% for diabetes, 46.1% for ever smoking, 43.6% for high cholesterol, 48.1% for hypertension, 84.7% for inadequate fruit and vegetable consumption, 33.0% for obesity, and 29.8% for sedentary lifestyle. The highest prevalence rate for CVD only and both CVD and SCI was among adults with 6 or 7 risk factors, whereas the highest prevalence rate for SCI only was for adults with household income <$15 000 (Table 1).
Demographic characteristics of adults aged ≥45 (N = 302 008) reporting cardiovascular disease (CVD) only, subjective cognitive impairment (SCI) only, or both conditions, Behavioral Risk Factor Surveillance System, 2017a,b
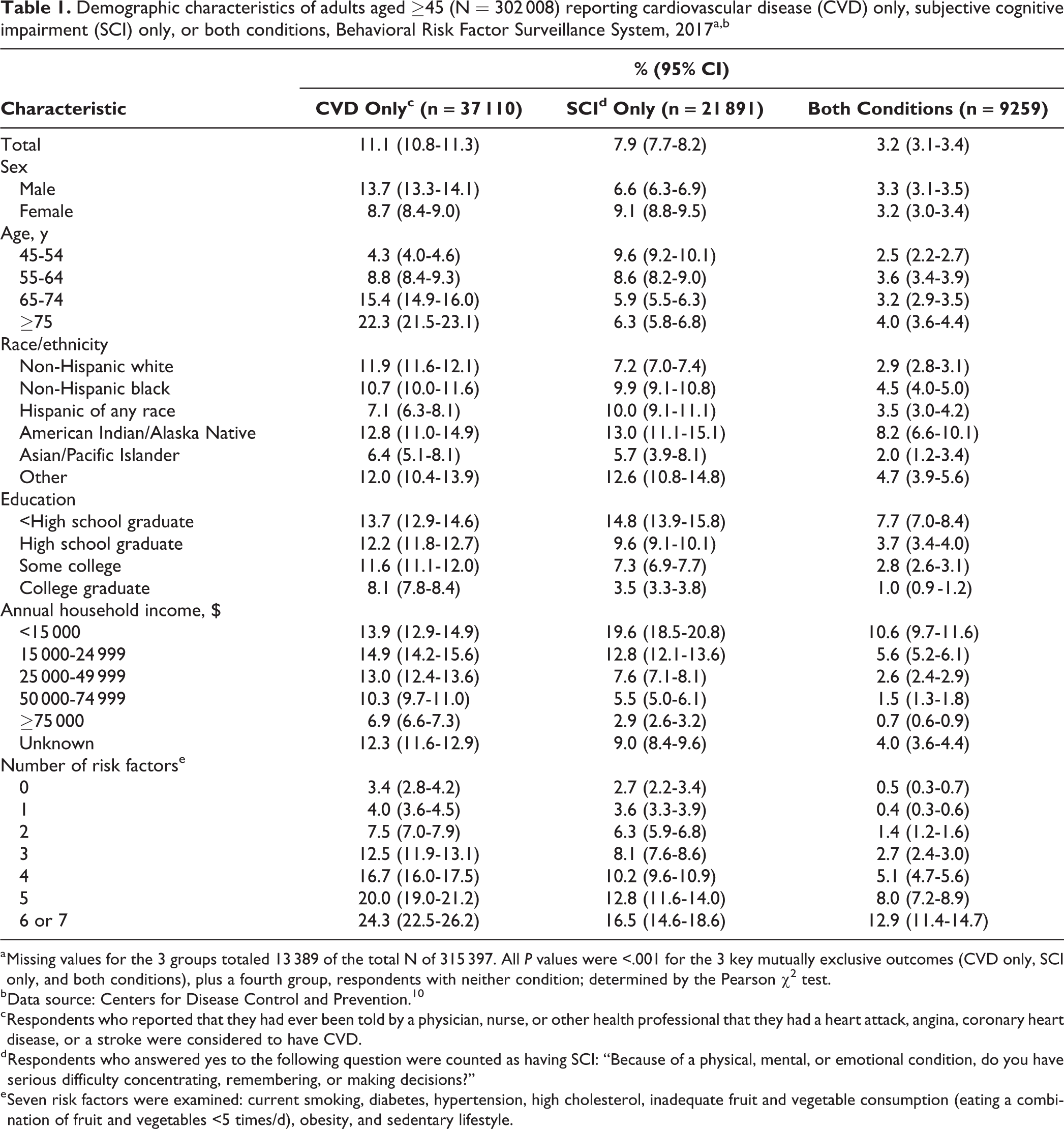
a Missing values for the 3 groups totaled 13 389 of the total N of 315 397. All P values were <.001 for the 3 key mutually exclusive outcomes (CVD only, SCI only, and both conditions), plus a fourth group, respondents with neither condition; determined by the Pearson χ2 test.
b Data source: Centers for Disease Control and Prevention. 10
c Respondents who reported that they had ever been told by a physician, nurse, or other health professional that they had a heart attack, angina, coronary heart disease, or a stroke were considered to have CVD.
d Respondents who answered yes to the following question were counted as having SCI: “Because of a physical, mental, or emotional condition, do you have serious difficulty concentrating, remembering, or making decisions?”
e Seven risk factors were examined: current smoking, diabetes, hypertension, high cholesterol, inadequate fruit and vegetable consumption (eating a combination of fruit and vegetables <5 times/d), obesity, and sedentary lifestyle.
The co-occurrence of SCI among all adults with CVD was 22.6%, ranging from 15.2% among respondents aged ≥75 to 36.8% among respondents aged 45-54. The co-occurrence of CVD among all adults with SCI was 29.0%, ranging from 20.5% among respondents aged 45-54 to 39.1% among respondents aged ≥75 (not shown). We avoided this overlap in our analysis by using mutually exclusive categories. In addition, the 2015 BRFSS data from 35 states on cognitive decline showed that 57.5% of adults aged ≥45 with SCI also reported cognitive decline. This percentage was similar across all 4 age groups (range, 53.9%-59.4%), all with overlapping 95% CIs.
We found several differences between respondents with CVD only, respondents with SCI only, respondents with both conditions, and respondents with neither condition (Table 2). Compared with respondents with CVD only, respondents with SCI only had significantly higher or worse rates of disability, inability to work, access to health care, and quality of life measures. A smaller percentage of respondents with SCI only (29.2%) than with CVD only (63.3%) were aged ≥65. Overall, 95.8% of respondents aged ≥45 reported ≥1 of the 7 risk factors, and 52.5% reported ≥3 risk factors.
Health-related measures among adults with cardiovascular disease (CVD) only, subjective cognitive impairment (SCI) only, both conditions, and neither condition among respondents aged ≥45 (N = 302 008), Behavioral Risk Factor Surveillance System, 2017a
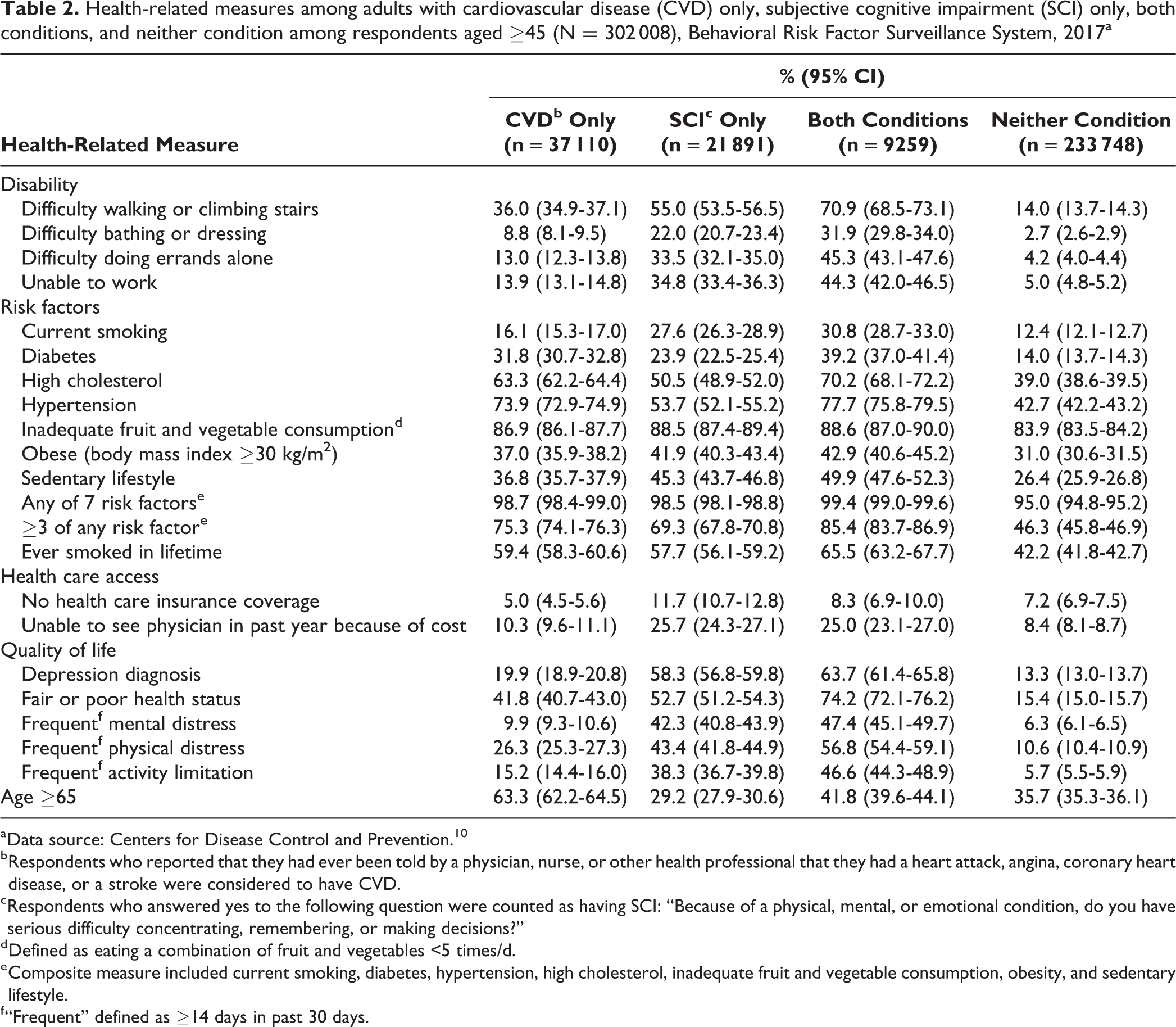
a Data source: Centers for Disease Control and Prevention. 10
b Respondents who reported that they had ever been told by a physician, nurse, or other health professional that they had a heart attack, angina, coronary heart disease, or a stroke were considered to have CVD.
c Respondents who answered yes to the following question were counted as having SCI: “Because of a physical, mental, or emotional condition, do you have serious difficulty concentrating, remembering, or making decisions?”
d Defined as eating a combination of fruit and vegetables <5 times/d.
e Composite measure included current smoking, diabetes, hypertension, high cholesterol, inadequate fruit and vegetable consumption, obesity, and sedentary lifestyle.
f “Frequent” defined as ≥14 days in past 30 days.
Adjusted Results
Results of logistic regression confirmed unadjusted results for all 3 key outcomes (Table 3). When the 7 risk factors were entered in the model separately (vs not having the risk), hypertension was the risk factor with the highest aOR among respondents with CVD only (aOR = 2.15; 95% CI, 2.01-2.30) and among respondents with both CVD and SCI (aOR = 2.37; 95% CI, 2.07-2.71), whereas current smoking was the risk factor with the highest aOR among respondents with SCI only (aOR = 1.55; 95% CI, 1.42-1.70). Logistic regression also confirmed that respondents with SCI only were more likely than respondents with CVD only to report the 3 disabilities, inability to work, and poorer quality of life. Among adults with CVD only, aORs ranged from not significantly greater than 1.0 for depression and frequent mental distress to 2.07 (95% CI, 1.93-2.22) for fair or poor health, whereas among adults with SCI only, aORs ranged from 2.76 (95% CI, 2.51-3.03) for fair or poor health to 6.21 (95% CI, 5.70-6.76) for depression (not shown).
Adjusted odds ratiosa for the outcomes of cardiovascular disease (CVD) only, subjective cognitive impairment (SCI) only, and both conditions among respondents aged ≥45 (n = 251 167), Behavioral Risk Factor Surveillance System, 2017b
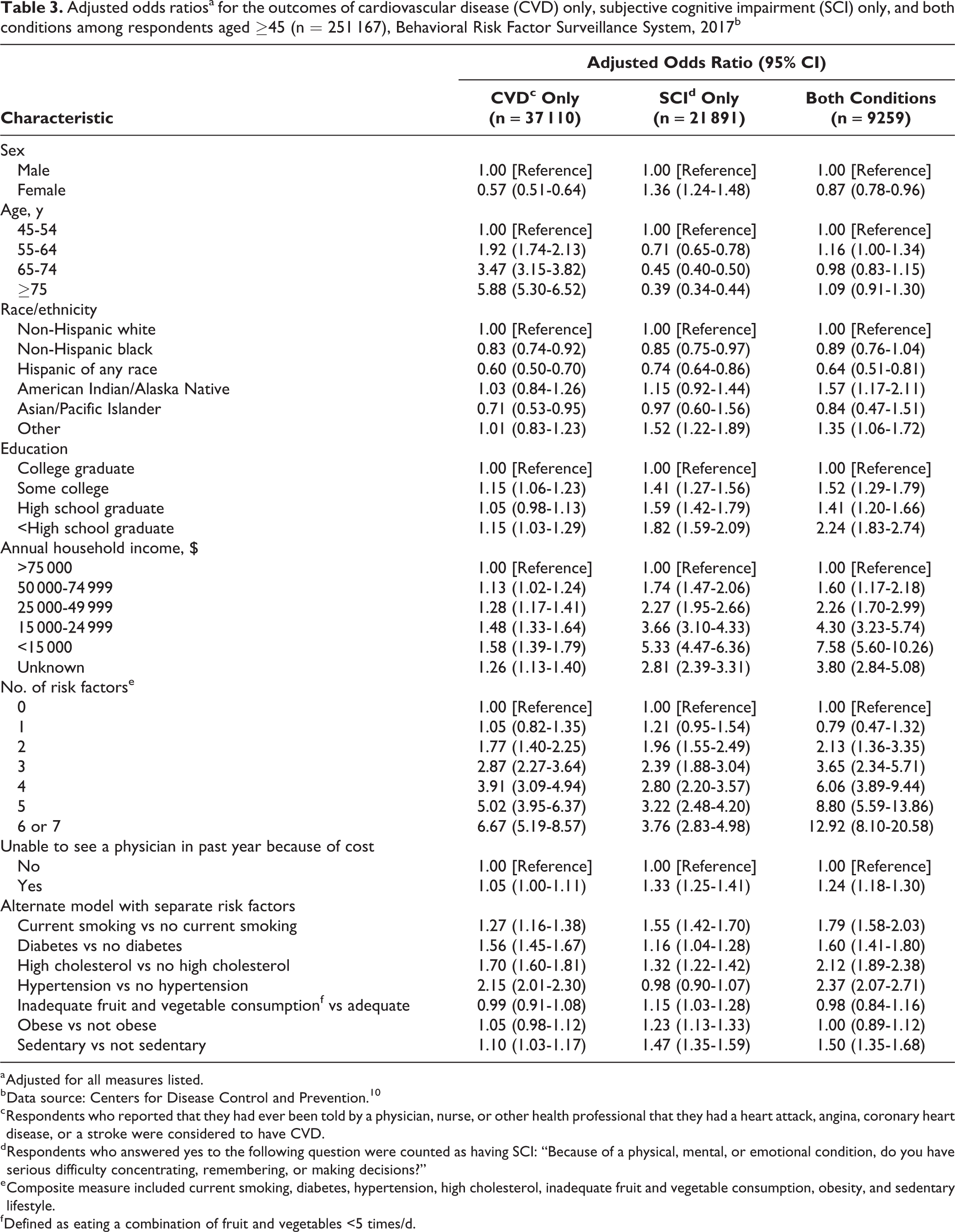
a Adjusted for all measures listed.
b Data source: Centers for Disease Control and Prevention. 10
c Respondents who reported that they had ever been told by a physician, nurse, or other health professional that they had a heart attack, angina, coronary heart disease, or a stroke were considered to have CVD.
d Respondents who answered yes to the following question were counted as having SCI: “Because of a physical, mental, or emotional condition, do you have serious difficulty concentrating, remembering, or making decisions?”
e Composite measure included current smoking, diabetes, hypertension, high cholesterol, inadequate fruit and vegetable consumption, obesity, and sedentary lifestyle.
f Defined as eating a combination of fruit and vegetables <5 times/d.
Combined PARs ranged from 41.6% among respondents with SCI only to 76.0% among respondents with both conditions, with 5 or 6 risk factors contributing to PARs for each of the 3 key outcomes (Table 4). For diabetes, hypertension, and sedentary lifestyle, PARs among adults with both CVD and SCI roughly approximated the total PARs for CVD only and SCI only. Among the 7 risk factors, the PARs for CVD only and for both conditions were highest for hypertension (35.5% and 39.5%, respectively) and high cholesterol (22.9% and 32.5%, respectively), whereas the PARs for SCI only were highest for ever smoked in lifetime (17.2%) and sedentary lifestyle (12.8%).
Population-attributable risk (PAR) for cardiovascular disease (CVD) only, subjective cognitive impairment (SCI) only, and both conditions, among respondents aged ≥45 (n = 251 308) in the Behavioral Risk Factor Surveillance System, 2017a,b
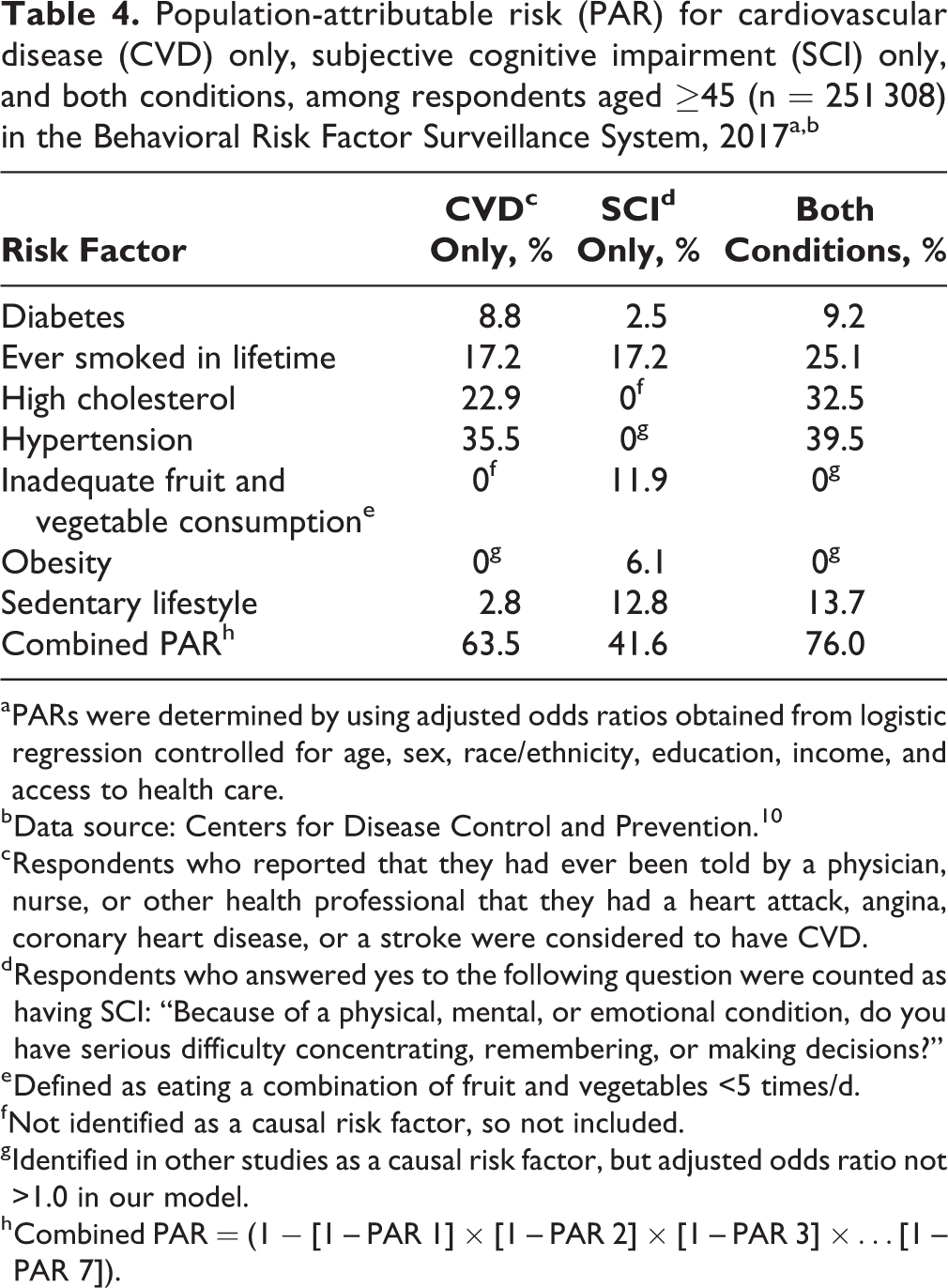
a PARs were determined by using adjusted odds ratios obtained from logistic regression controlled for age, sex, race/ethnicity, education, income, and access to health care.
b Data source: Centers for Disease Control and Prevention. 10
c Respondents who reported that they had ever been told by a physician, nurse, or other health professional that they had a heart attack, angina, coronary heart disease, or a stroke were considered to have CVD.
d Respondents who answered yes to the following question were counted as having SCI: “Because of a physical, mental, or emotional condition, do you have serious difficulty concentrating, remembering, or making decisions?”
e Defined as eating a combination of fruit and vegetables <5 times/d.
f Not identified as a causal risk factor, so not included.
g Identified in other studies as a causal risk factor, but adjusted odds ratio not >1.0 in our model.
h Combined PAR = (1 − [1 – PAR 1] × [1 – PAR 2] × [1 – PAR 3] ×…[1 – PAR 7]).
Discussion
Our study showed that adults with SCI only are consistently more likely than adults with CVD only to report disabilities, inability to work, and poorer quality of life even though they tend to be younger. Among the 3 groups studied (CVD only, SCI only, and both conditions), the results for the aforementioned measures were best among respondents with CVD only, worse among respondents with SCI only, and worst among respondents with both conditions. Each risk factor was more likely to be reported by respondents with any of the 3 key outcomes than by respondents with none of the outcomes. Results of multivariate logistic regression generally confirmed these results, although dose–response gradients for these risk factors were not significantly different for each added risk factor. An earlier study, 3 which clearly showed a dose–response gradient between cognitive decline and dementia and several risk factors, included depression as a risk factor. Our omission of depression may account for this discrepancy. The use of mutually exclusive categories of health conditions provides details on CVD and SCI that might otherwise be missed and shows the effect of the combination of the 2 health conditions. The differences in age and sex association between SCI and CVD were also clarified, along with attenuation of both differences when SCI and CVD co-occurred.
Although our measure of SCI does not represent a specific diagnosis, our findings are important. Our limited comparison of 2015 BRFSS data and 2017 BRFSS data showed that about half of respondents who reported SCI also reported cognitive decline. When considered in the context of other studies indicating that adults recognize and self-report memory problems up to 15 years before they can be diagnosed, 20 our results suggest that our measure of SCI might include adults who are at a stage of being able to self-report memory problems but are undiagnosed. If so, these adults with SCI may be in early cognitive decline at a stage when they should be encouraged to seek help. 21 Few adults with memory problems discuss their memory problems during visits with a health care provider, 22 even though such visits offer a chance for cognitive assessment and possibly a diagnosis of dementia. 23 One study found that 41.8% of adults aged ≥45 who reported memory concerns and saw a health care provider reported getting treatment for their memory problems. 22 The Medicare Annual Wellness visit is one such opportunity, although our results and the results of others 22 suggest that adults aged 45-64 might also benefit. Some adults with SCI might have intellectual disabilities, developmental disabilities, acquired brain injuries, or learning disabilities, 24 but adults without a definitive diagnosis of any of these disorders might especially benefit from talking to a health care provider. Other adults reporting SCI might have depression or other treatable and potentially reversible causes of memory problems that could be identified in a visit with a health care provider. 22
We found that one-quarter of study respondents with SCI (with or without CVD) reported being unable to see a physician in the past year because of cost. This cost barrier could be affecting respondents’ health care in various ways. For example, they may be reluctant to schedule a routine checkup, which presents an opportunity for a discussion about their cognitive difficulties. 22 Of course, adults with SCI only were more likely than those with CVD to be aged <65, so they were also less likely to be covered by Medicare and, thus, not eligible for a Medicare Annual Wellness visit. Any barrier to health care could be a concern if co-occurring chronic conditions are present. In our study, more than 22% of respondents with either CVD or SCI also reported the other condition, but they likely had additional conditions, especially when we recognize that diabetes, hypertension, and high cholesterol can also be considered chronic conditions that require ongoing monitoring. 25
Women were more likely than men to report SCI only, but the opposite was true for CVD only, and we found no difference between men and women with both SCI and CVD. Adjusted ORs for CVD only increased with increasing age, whereas aORs for SCI only declined with increasing age, and we found no association with age among adults with both conditions. These age associations merit further investigation. Lower income had a more noticeable association among adults with SCI only and both SCI and CVD than among adults with CVD only.
PAR is an important consideration when formulating strategies for interventions. Although we used mutually exclusive measures and focused on adults aged ≥45, our results are consistent with the results of previous studies using similar risk factors but different measures and ages. 7,19 The similarity between SCI and CVD in their association with these 7 risk factors is perhaps even more meaningful than their differences, because it differs from findings on other chronic conditions. For example, for each of our study’s 3 key outcomes, at least 5 of the 7 risk factors contributed to combined PARs. In contrast, when chronic obstructive pulmonary disease, arthritis, asthma, diabetes, and kidney disease were studied 7 with these same 7 risk factors, a maximum of 3 of the risk factors contributed to PARs for each of these 5 outcomes. Our results also suggest that the risk factors to target in interventions to address SCI are the same risk factors already being used to target CVD.
Limitations
Our study had several limitations. First, the study was limited by the reliability and validity of the self-reported data. 26 However, the measure of cognitive disability has been well-studied by the US Census Bureau. 8,9,14 Second, cross-sectional studies such as BRFSS do not prove causal relationships; however, we used only risk factors showing causality in other studies of CVD and cognitive decline for estimating PARs. 4,5,7 Reverse causality, especially for sedentary lifestyle, cannot be ruled out. Including other risk factors, such as depression, might yield different results. Third, the generalizability of results from all 50 states and the District of Columbia is unknown. The BRFSS surveys only noninstitutionalized adults, so persons in long-term care, who may be more likely to have SCI or CVD, are excluded. Adults who live in households but are physically or mentally unable to respond to a survey are also excluded, which may omit some potential respondents with these conditions, as noted in a BRFSS study in 2017. 27 That 2017 study compared respondents with cognitive decline from the BRFSS cognitive decline module with proxy responses for nonrespondents and found that nonrespondents (who did not need to be deemed able to respond to the survey) were more likely to have dementia and functional difficulties due to cognitive decline. The effect of excluding persons unable to respond to a telephone survey implies that adults in our study may have been less affected by their SCI than other adults with SCI in the community. The exclusion of persons unable to respond to a telephone survey may also help explain our finding that aORs for SCI decreased with increasing age. This phenomenon could result when SCI progresses with age: older adults become unable to respond to a survey and so they are no longer included in a study. The phenomenon could also affect results for racial/ethnic groups if they are affected differently by SCI.
Strengths
Our study also had several strengths. First, the data were from a single, large, representative survey of all 50 states and the District of Columbia. Second, the study employed a widely used standard measure of cognitive disability along with validated measures of risk factors and chronic disease. Third, examination of the mutually exclusive categories of CVD only, SCI only, and both conditions underscored differences and similarities between CVD and SCI. Fourth, PAR estimates may assist in developing interventions to address SCI.
Conclusion
Our study found both similarities and differences between adults with CVD and adults with SCI on a number of demographic and health-related measures. Although adults with SCI only tended to be younger than adults with CVD only, they had poorer quality of life, had worse access to health care, and were more likely to report other disabilities. Even the possibility that some persons with SCI might eventually progress to dementia should be seen as an opportunity to encourage dialogue with primary care providers. Such discussions might uncover treatable causes of their cognitive difficulties unrelated to dementia or could potentially lead to earlier diagnosis and treatment with associated long-term clinical benefits and cost savings. 2 By adding PARs for 7 risk factors for adults with only CVD or SCI, our results on risk factors are similar to the results of other studies 3 -7 and suggest that building on existing prevention activities for CVD may be worth exploring to address SCI.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Centers for Disease Control and Prevention (grant/cooperative agreement No. 1U58DP006069-01).