
Abstract
The Plain community is the fastest-growing religious minority in Wisconsin. This community has a high incidence of genetic disorders, many of which are identifiable through newborn screening. We describe efforts by the Wisconsin Newborn Screening Program (WNSP) to improve health care in the Plain community by targeting early identification of, and intervention for, patients with inherited metabolic disorders. WNSP formed partnerships with families and health care providers to increase awareness of screening procedures and the intended benefits of screening, modify testing algorithms to enhance detection, and establish medical homes for patients with confirmed disorders. The estimated number of Plain newborns screened increased by 25.5% during the study period, from 547 in 2011 to 736 in 2017; 122 persons underwent carrier testing, and 143 newborns received second-tier testing. From 2014 to 2017, affected patients received 71 metabolic evaluations in their community medical home without travel to major health centers. This article demonstrates how a comprehensive public health program can help increase screening rates, enhance detection, and establish follow-up care in a hard-to-reach religious community. A key lesson learned was the importance of communication among all stakeholders to develop an effective public health program.
The Plain community, which includes Amish and Mennonites, is a “Christian group that lives simply, dresses plainly, and lives in the modern world but remains separate from it.” 1 Originating from the Anabaptist movement in Europe, the Plain community settled in Pennsylvania during the 1700s. 2 However, in the early 1900s, because of the need for farmland, the community expanded westward into rural regions of Wisconsin; it had grown to an estimated 21 000 persons living in Wisconsin as of 2018. 3,4 This community presents unique challenges to state public health systems because of cultural barriers. Families do not typically receive preventive health care, including routine physical examinations, prenatal care, or immunizations, and they often have limited knowledge of the health care system. Children with special needs are viewed as part of God’s plan, and treatment may not be sought. Most members do not have health insurance or use government-funded health care programs; the costs of medical services are absorbed by individuals, families, or the church community. 2
Because of a small founder population, few converts, and infrequent outside marriages, more than 150 genetic disorders have been diagnosed within the Plain community. 5 Many of these disorders are defects of metabolism that affect newborns and require medical intervention to reduce morbidity and mortality. 6 Two of the most common disorders within the Plain community are maple syrup urine disease (MSUD, OMIM #248600) and propionic acidemia (PA, OMIM #606054) (https://omim.org). Mennonites with MSUD have a common mutation (BCKDHA c.1312T>A) that leads to severe encephalopathy, presenting as early as the second day of life. Carrier frequency for this autosomal recessive disorder within the Plain community is high and estimated to be 1 in 10 persons, with an approximate incidence of 1 in 1000. 7 In the general population, the incidence of MSUD is substantially lower at approximately 1 in 185 000. 7 Early diagnosis of MSUD in the newborn period has been shown to reduce morbidity, avoiding metabolic crisis, hospitalization, and death. 6 Amish persons with PA share a common mutation in the PCCB gene (c.1606A>G), which has variable clinical presentations and a mild biochemical phenotype. 8 The incidence and carrier frequency of this autosomal recessive disorder in the Plain community are unknown but appear to be higher than in the general population (1:100 000 to 1:130 000); more than 75 Plain persons with PA are described in the literature. 8 -10 Amish persons with PA may present with neurologic sequelae in infancy, with cardiomyopathy in adolescence, or remain asymptomatic. The total number of affected Wisconsin Plain community patients with either MSUD or PA is not precisely known. Between 2011 and 2017, the Wisconsin Newborn Screening Program (WNSP) identified 3 newborns with MSUD and 5 newborns with PA. MSUD and PA are both treated with diet modifications, acute sick management, long-term monitoring for complications, and frequent clinical assessments by metabolic specialists. 11
Newborn screening provides early identification of congenital disorders in newborns, whose timely treatment can prevent adverse outcomes. WNSP is administered through the Wisconsin Department of Health, with testing at the Wisconsin State Laboratory of Hygiene (WSLH). 12 In 2017, Wisconsin had approximately 64 000 births, and >99.5% of infants were screened for the panel of 44 disorders, which includes MSUD and PA. Dried blood spot specimens are collected by hospitals or midwives at 24-48 hours of life and transported by courier to WSLH within 48 hours after collection. Test results are reported in the first 5-7 days of life.
The total number of births and newborn screening rates in the Wisconsin Plain community is largely unknown. Plain families typically do not apply for birth certificates, which are the primary means of calculating birth rates. In the Plain community, births typically occur at home under the care of birth attendants (licensed and lay midwives), who are also responsible for performing the newborn screen. A 2014 survey of the Wisconsin Plain community revealed that 74% of the 297 households surveyed received newborn screening for their infant; however, 23% of these respondents indicated they were either unlikely to screen future children or unsure if they would do so. 13 When asked about reasons for not screening, 32% of respondents indicated a lack of personal knowledge or a lack of information communicated by their health care provider, and 16% listed other concerns, such as beliefs, costs, travel, privacy, or the need for follow-up testing. 13
WNSP provides long-term care for all persons diagnosed with metabolic disorders through screening at specialty clinics in urban medical centers. In the Plain community, routine medical care for newborns is provided through local birth attendants and community health care providers. Travel to medical centers is not often feasible because most Plain community members do not drive. There are also substantial financial barriers to seeking medical attention outside the community because of a lack of health insurance.
With the knowledge that treatable disorders identified by newborn screening are more common in the Plain community than in the general population, survey data highlighting the education of both parents and community health care providers as a barrier to screening, and concerns about access to specialized medical care, approximately 20 key stakeholders formed a partnership in 2011 to address these challenges. Key stakeholders included community practitioners and birth attendants, the Wisconsin Department of Health and WSLH, clinical specialists, and families.
Studies on newborn screening in the Plain community are scant. We aimed to fill an important research gap by assessing the number of newborns in the Wisconsin Plain community who received screening for metabolic disorders and describe efforts during a 6-year period to (1) provide education for families and health care providers on the benefits of newborn screening, (2) enhance screening algorithms, and (3) expand access to health care for affected newborns.
Activities and Outcomes
Screening in the Plain Community
In 2012, WNSP organized the first public meeting with Plain community members to identify cultural and logistic barriers to screening. D. Holmes Morton, MD, a leading physician and founder of the Clinic for Special Children within the Plain community of Lancaster, Pennsylvania, provided insight and guidance for the discussion. From 2013 to 2017, 5 more community meetings were held with Plain families to describe the benefits of screening, clarify the population needs, minimize any communication barriers, and provide best practices for the long-term care of persons with inherited metabolic disorders. Women in the Plain community do not routinely seek prenatal care, nor do they typically discuss the risk for inherited genetic disorders with their health care provider or family members. In addition, parents of children with a genetic disorder may not always seek medical evaluation and treatment because the disorder can be viewed as part of God’s plan. The goal with many of these community meetings was to raise awareness, increase communication, prevent misunderstandings, and address the need for treatment, all within the context of the Plain community’s religious practices.
From 2016 to 2017, WNSP organized 8 informational meetings for birth attendants, highlighting the importance of screening and providing recommendations for proper specimen collection. WNSP provided information on specimen collection and transport quarterly at local midwifery guild meetings. In September 2016, a 2-day conference focused on “practical approaches to inherited disease in the Plain community” brought together community members and health care providers to share current care recommendations for affected children. All educational activities were held near or within the Plain communities to facilitate access and provide an environment that was familiar to families (Figure).
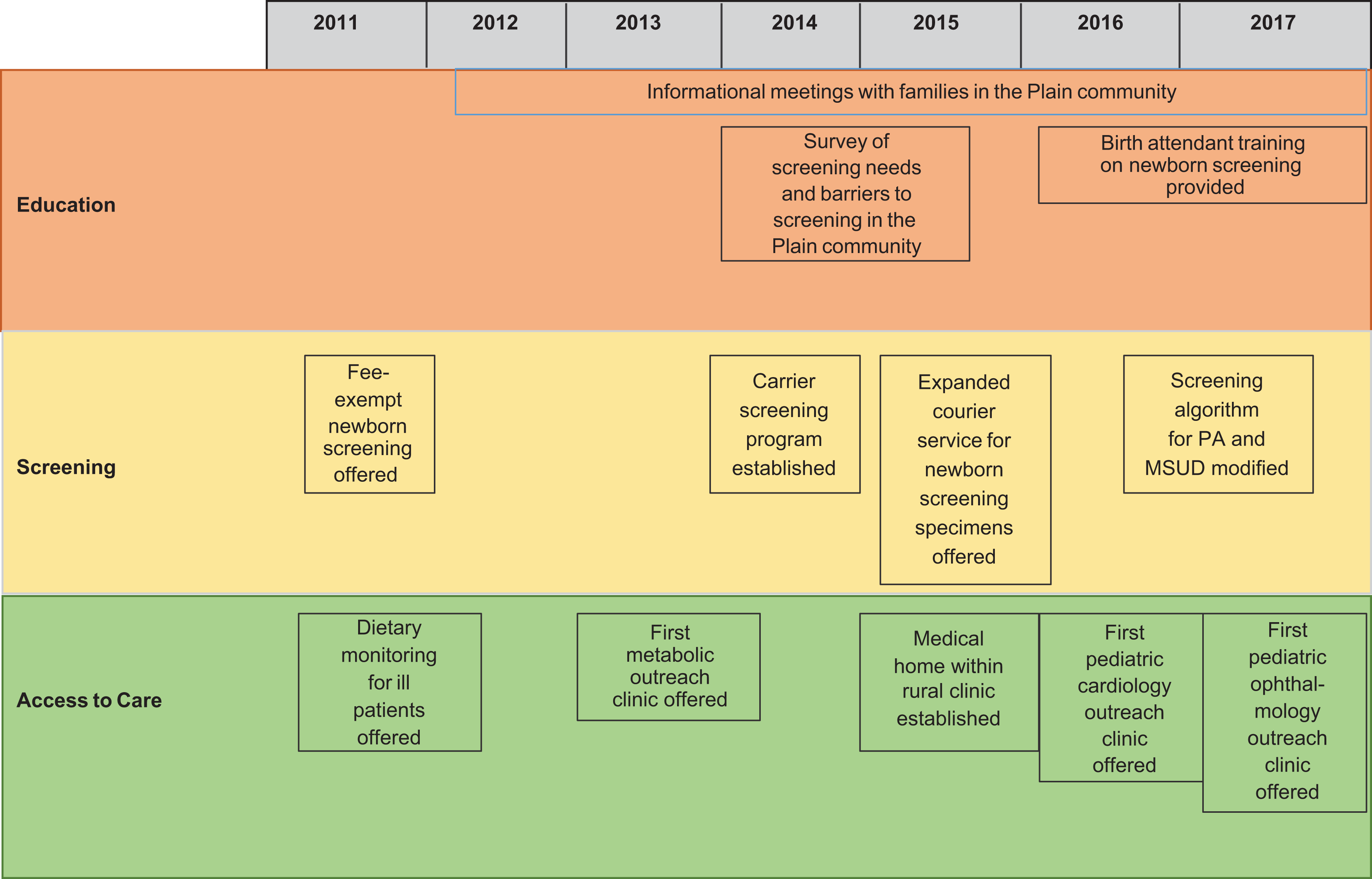
Timeline of projects and activities for newborn screening for maple syrup urine disease (MSUD) and propionic acidemia (PA) in the Plain community, Wisconsin, 2011-2017. The Plain community is a religious group in Wisconsin that includes Amish and Mennonites. The timeline shows outreach efforts by the Wisconsin Newborn Screening Program (WNSP) to enhance newborn screening for a panel of 44 disorders, including MSUD and PA, through education, adapted screening algorithms, and expansion of clinical services for affected persons.
Through discussions with birth attendants and Plain community families, 2 logistic barriers to screening, cost and difficulty of transporting specimens to the laboratory, were identified. In Wisconsin, the cost of newborn screening is $109 per specimen. These funds are used for laboratory testing and programmatic needs (education and courier service), long-term care, and treatment of affected persons. Since 2011, WNSP has offered fee-exempt cards to birth attendants who serve low-income, uninsured families. WNSP addressed logistic difficulties in transporting specimens through an expanded courier service, beginning in January 2015, from the homes of birth attendants to WSLH within 48 hours, consistent with the timing of specimen transport achieved by 95% of hospitals in the state (Figure). Before 2015, birth attendants used the postal service for specimen transport, but delays were as long as 4 days.
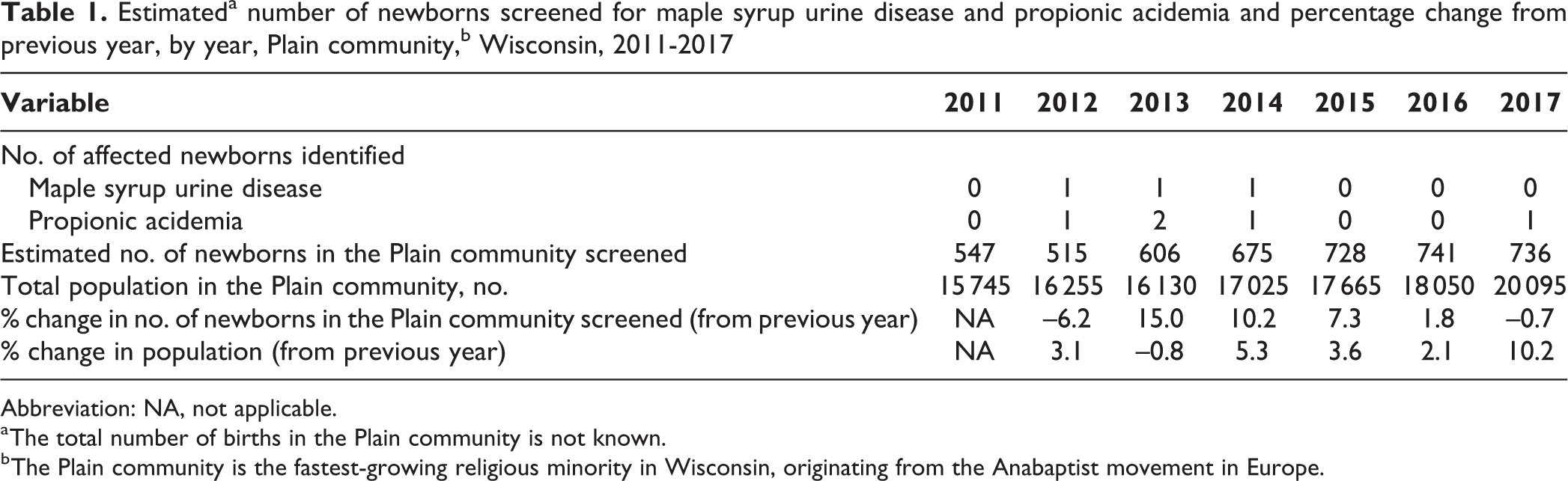
To obtain an estimate of the number of Plain community newborns who received screening, WSLH queried its specimen database and extracted data on the number of infants born at home or at clinics that serve the Plain community. These data were then filtered by the number of newborns with common Amish and Mennonite surnames. For each year of the study, WSLH compared this estimate of Plain community screened newborns with the census data on the number of Plain persons in Wisconsin. WSLH also calculated a screening rate and population growth rate for the same period. 3,4 The number of screened newborns in the Plain community increased 25.7%, from 547 in 2011 to 736 in 2017. The total Plain population in Wisconsin grew by 21.7% during this period. WNSP attributed the higher screening rates from 2013 to 2016, as compared with the population growth rates, to the implementation of educational programs targeted at birth attendants and families, fee-exempt cards, and improved logistics (Table 1). However, no single intervention could be identified as having the greatest impact. In 2017, the rate of screening appeared to have stagnated, perhaps due to natural fluctuations in birth rates and compounded by a substantial change in the migration of Plain persons to the region. The total number of births in the population is not known. This case study could assess only the number of infants screened.
Estimateda number of newborns screened for maple syrup urine disease and propionic acidemia and percentage change from previous year, by year, Plain community,b Wisconsin, 2011-2017
Abbreviation: NA, not applicable.
a The total number of births in the Plain community is not known.
b The Plain community is the fastest-growing religious minority in Wisconsin, originating from the Anabaptist movement in Europe.
During the study period, from 2011 to 2017, WNSP identified 3 newborns with MSUD and 5 newborns with PA through the newborn screening algorithm (Table 1). One additional newborn with PA received screening, but the illness was not detected (false negative) until the onset of clinical symptoms. This baby was born prior to implementation of the more sensitive second-tier test discussed hereinafter. Two additional PA patients, born before 2011, did not receive screening but were identified during the study period because of the onset of clinical symptoms.
Enhancement of Screening Algorithms
To identify persons in the Plain community who were at highest risk for MSUD and PA, WSLH developed modified screening algorithms that addressed the unique features of each disease (Table 2). Because of the high carrier frequency in the Plain community, WNSP recommends prenatal or preconception molecular DNA carrier testing for MSUD and PA to all persons in the Plain community, as described by Kuhl et al. 14 WSLH performs this testing at no charge, and results are provided to the individual and the provider. If the carrier test results are positive for an expectant couple (indicating that both parents are carriers for MSUD), an in-person appointment is made to discuss recommendations for delivery and subsequent screening. Owing to the severity of MSUD, the same molecular DNA test for the common mutation is offered within hours after delivery to determine if the infant is affected with the disease (2 copies of the mutation). Biochemical testing to detect patients affected with MSUD, provided by routine newborn screening, cannot be performed until 24 hours of life. The molecular tests allow for earlier detection and treatment.
Screening algorithm and care recommendations for maple syrup urine disease (MSUD) and propionic acidemia (PA) in the Plain community, Wisconsin, 2017a
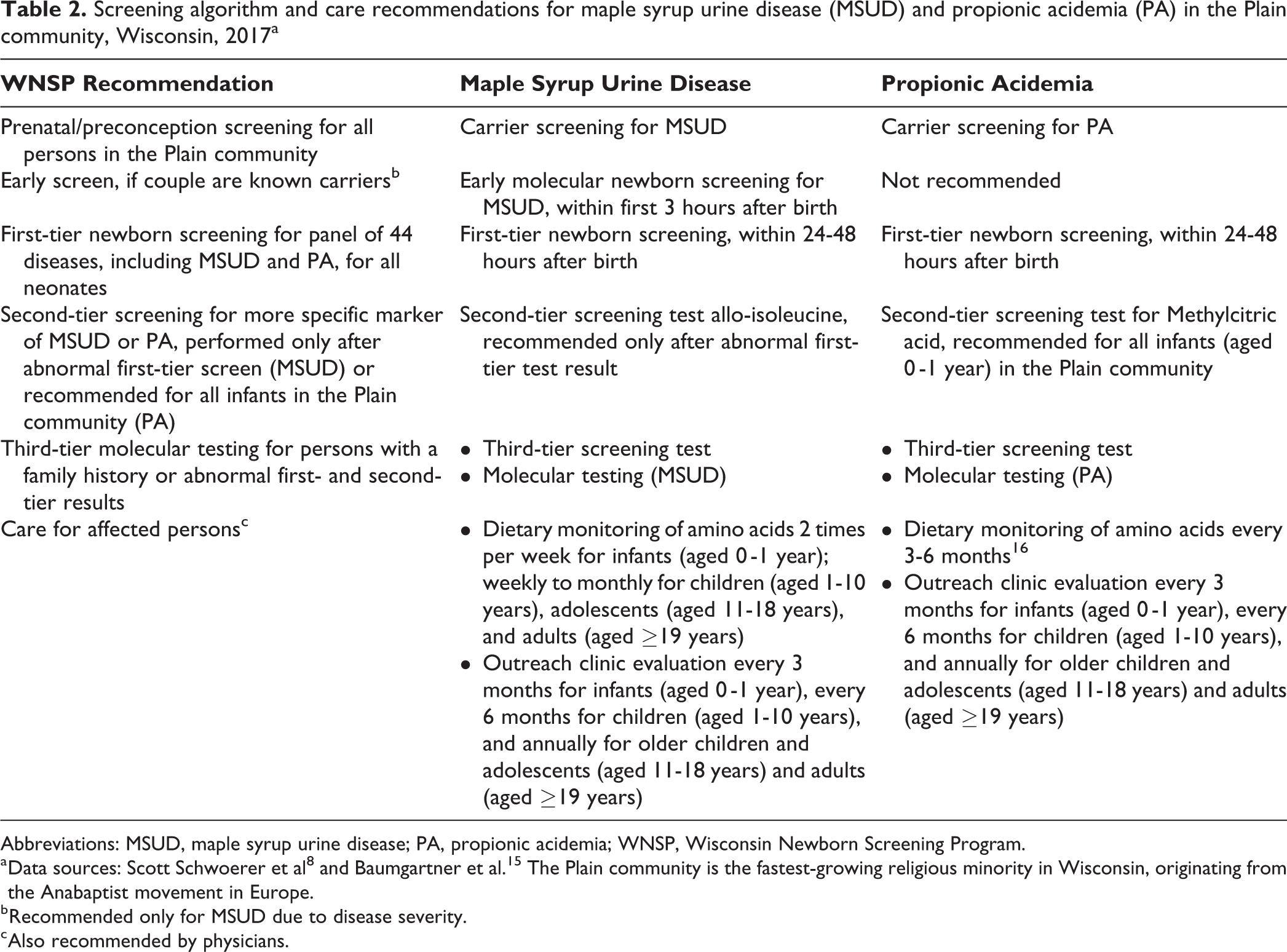
Abbreviations: MSUD, maple syrup urine disease; PA, propionic acidemia; WNSP, Wisconsin Newborn Screening Program.
a Data sources: Scott Schwoerer et al 8 and Baumgartner et al. 15 The Plain community is the fastest-growing religious minority in Wisconsin, originating from the Anabaptist movement in Europe.
b Recommended only for MSUD due to disease severity.
c Also recommended by physicians.
The Wisconsin newborn screening panel (first-tier test) tests all neonates for 44 conditions, including PA and MSUD. A second-tier test for PA is performed only on specimens collected from newborns whose parents elected to identify themselves as Amish or Mennonite on the newborn screening card, or for any neonate with an abnormal first-tier PA test result. Because a mild biochemical phenotype is found in Amish patients with PA, the risk for false negatives is increased. The second-tier screening test for PA quantifies methylcitric acid as a more specific marker for this disease. Likewise, for MSUD, if the first-tier test is abnormal, a more specific second-tier biochemical test that measures allo-isoleucine is performed. If both the first-tier test and the second-tier test are consistent and suggestive of either PA or MSUD, a third-tier molecular test is performed.
These 2 modified screening algorithms, which include carrier testing and a tiered approach to screening, reduce the time between diagnosis and treatment and minimize the risk of false negatives. In the 3 years (2015-2017) that carrier testing was offered, 122 persons participated. In addition, from June 2017 through December 2017, 143 newborns received both first-tier and second-tier testing for PA because their parents identified themselves as part of the Amish or Mennonite community. Participation in these additional tests highlights the Plain community’s growing trust in WNSP.
Access to Care
For optimal outcomes, patients with metabolic disorders should be regularly evaluated by metabolic specialists (Table 2). However, because of the distance between the Plain communities and medical centers, compliance with this recommendation is poor. Modeled after the Clinic for Special Children in Lancaster, Pennsylvania, Wisconsin established the Center for Special Children at a rural Plain community clinic to serve as a medical home for affected persons. Staff members include community practitioners and a clinic coordinator. Clinical specialists remotely coordinate patient care with the primary team and periodically provide onsite assessment. Metabolic specialists work with practitioners to develop plans for home care of ill patients, including dietary modification when the patient is sick, administration of medications when symptomatic, and home monitoring of urine ketones to determine metabolic status. These tools manage the acute needs of the patient without expense and travel to medical facilities or hospitalization. Metabolic care has been available since June 2014, and cardiac care and ophthalmic care, as needed for disease-related complications, were added in 2016 and 2017, respectively (Figure). From June 2014 through December 2017, 71 appointments for patients with PA or MSUD occurred: 39 appointments (13 patients) for PA and 32 appointments (9 patients) for MSUD.
Physicians recommend that newly diagnosed infants with MSUD and PA receive frequent dietary monitoring (Table 2). 8,15 WSLH provides dietary monitoring by amino acid analysis in dried blood spots at an affordable rate. Specimens can be collected at home and mailed to the laboratory. During times of illness, the diet monitoring samples can be couriered to WSLH, along with the newborn screening specimens, with results available the following day. Frequent monitoring affords a more accurate assessment of metabolic control and has minimized long-term complications associated with each disease. 8
Lessons Learned
Newborn screening is an essential public health program whose success depends on communication among all stakeholders, including birth attendants, Plain community families, physicians, and laboratorians, toward the common goal of early identification, treatment, and long-term care of newborns with congenital disorders. From 2011 to 2017, WNSP established relationships with Plain families to foster acceptance and willingness to participate in screening for their children. To prevent misunderstandings and reduce communication barriers, information on newborn screening was provided at community meetings, with awareness of cultural differences. Educational opportunities were also provided to birth attendants on the logistics of specimen collection, specimen transport, and program funding. Together, these outreach efforts set a foundation for acceptance of screening and adherence to recommended protocols. Modified screening algorithms provide results for the most severe diseases affecting the population within an optimal timeframe. The Center for Special Children in Wisconsin enables long-term, consistent care of affected persons; manages acute illness; and facilitates direct communication among clinical specialists, community practitioners, and patients. Trust between the community and medical providers has been strengthened.
Future challenges for WNSP will be to maintain and foster engagement with all stakeholders. Families need frequent interactions with care providers to obtain information and maintain relationships. Continual education for birth attendants is necessary to provide current recommendations for screening and treatment. As stakeholders’ needs change, it will be important to continually query families and health care providers to ensure satisfaction with WNSP.
Two important considerations for adapting this program to other settings are to (1) be aware of the unique concerns of the target population and (2) develop relationships with key stakeholders that begin with an understanding of cultural differences. It is important to consider ways to adapt the public health program to meet the needs of the population, whether that is by tailoring educational efforts, modifying testing, or planning for continued care in a comfortable environment.
Partnerships and communication among all key stakeholders have helped unify individual efforts, meeting WNSP’s goal to provide early detection and long-term care for affected persons. This case study provides a framework for implementing and maintaining a successful screening program in communities that serve unique populations.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded, in part, by a Wisconsin Partnership Program Opportunity Grant.