
Abstract
Objectives:
Foodborne disease is a pervasive problem caused by consuming food or drink contaminated by infectious or noninfectious agents. The 55 US poison centers receive telephone calls for advice on foodborne disease cases that may be related to a foodborne disease outbreak (FBDO). Our objective was to assess whether poison center call records uploaded to the National Poison Data System (NPDS) can be used for surveillance of noninfectious FBDOs in the United States.
Methods:
We matched NPDS records on noninfectious FBDO agents in the United States with records in the Foodborne Disease Outbreak Surveillance System (FDOSS) for 2000-2010. We conducted multivariable logistic regression analysis comparing NPDS matched and unmatched records to assess features of NPDS records that may indicate a confirmed noninfectious FBDO.
Results:
During 2000-2010, FDOSS recorded 491 noninfectious FBDOs of known etiology and NPDS recorded 8773 calls for noninfectious foodborne disease exposures. Of 8773 NPDS calls, 469 (5.3%) were matched to a noninfectious FBDO reported to FDOSS. Multivariable logistic regression indicated severity of medical outcome, whether the call was made by a health care professional, and etiology as significant predictors of NPDS records matching an FDOSS noninfectious FBDO.
Conclusions:
NPDS may complement existing surveillance systems and response activities by providing timely information about single cases of foodborne diseases or about a known or emerging FBDO. Prioritizing NPDS records by certain call features could help guide public health departments in the types of noninfectious foodborne records that most warrant public health follow-up.
Foodborne disease is a pervasive problem caused by consuming contaminated food or drink. An estimated 48 million foodborne illnesses occur annually in the United States, resulting in more than 128 000 hospitalizations and 3000 deaths each year. 1 A foodborne disease outbreak (FBDO) is defined as an incident in which 2 or more persons have a similar illness resulting from ingesting a common food at a comparable time and place. 2 Foods and beverages can be contaminated with infectious agents or noninfectious agents. 3 Noninfectious agents implicated in FBDOs include marine toxins (eg, ciguatera toxin, scombroid toxin), mushroom toxins (eg, muscimol, amanita), heavy metals (eg, arsenic, mercury), food additives (eg, monosodium glutamate), and pesticides (eg, insecticides, herbicides). 2 Although a wide range of agents can be implicated in a noninfectious FBDO, most are caused by marine toxins such as ciguatera or scombroid. 2
Surveillance for FBDOs is critical for responding to and preventing foodborne diseases. Public health investigations after detection of an outbreak can identify common or rare foods associated with FBDOs. Data from outbreaks of noninfectious FBDOs, although limited, may provide information on sources of foods most likely associated with outbreaks and can help target interventions to reduce incidence of foodborne illness. Data from outbreaks also can help researchers identify trends in commonly implicated foods and provide insight into the effectiveness of regulations and control measures. 3
Many national foodborne disease surveillance systems, such as the Foodborne Diseases Active Surveillance Network (FoodNet) and the Molecular Subtyping Network for Foodborne Disease Surveillance (PulseNet), focus on timely identification of foodborne infections and infectious FBDOs through microbial identification and laboratory confirmation of bacterial and parasitic contaminants. 4,5 However, these national surveillance systems do not track noninfectious FBDOs. The Centers for Disease Control and Prevention (CDC) tracks investigations of infectious and noninfectious FBDOs in the United States through the Foodborne Disease Outbreak Surveillance System (FDOSS). 6,7 State, local, and territorial public health departments identify and investigate outbreaks and report these outbreaks to FDOSS. 3
A small but nonetheless important percentage of FBDOs reported to FDOSS are attributed to noninfectious agents. 3 Ciguatera and scombroid toxin poisonings, only 2 of the many noninfectious agents potentially associated with a foodborne outbreak, account for more than 50 000 illnesses and 500 hospitalizations in the United States annually. 8
FDOSS is a repository of information about noninfectious FBDOs investigated in the United States. Because FDOSS collects completed reports of outbreaks after an investigation has occurred, the system can be used as a standard for determining whether other surveillance systems capture data on the same outbreaks that are investigated at the state and local level. The National Poison Data System (NPDS) is a national poison reporting database that conducts near–real-time electronic surveillance of noninfectious FBDOs. 9
Fifty-five poison centers across the United States offer free, confidential medical advice 24 hours per day, 7 days per week, through a 1-800 national helpline to help manage hazardous exposures. Poison center service areas vary by jurisdiction; some poison centers service multiple states, some service 1 state, and, in some jurisdictions, multiple poison centers service 1 state. Call data from local poison centers are uploaded approximately every 8 minutes to NPDS. State and federal public health agencies collaborate with poison centers to use the system for near–real-time surveillance of disease conditions or exposures and for situational awareness during incidents of public health importance. 9,10 Previous studies had mixed findings on whether poison center data can be useful for early detection of FBDOs. Derby et al 11 in 2005 found that data collected by 2 poison centers in Arizona differed from data collected by a county public health department and concluded that poison control data may be a useful addition to surveillance data reported to state public health agencies for the early detection of infectious FBDOs. Gruber et al 12 in 2015 found that unusual changes in the number of FBDO-related telephone calls to poison centers occurred after announcements of national outbreaks and recalls, citing limitations in using poison center data for foodborne disease surveillance.
Noninfectious foodborne illnesses are regularly reported in telephone calls to poison centers. Although frequently reported, these illnesses represent a fraction of all illnesses that occur in the United States, because only a small subset of the population seeks medical care or advice by calling a poison center. 10 Alternatively, for an illness to be reported to FDOSS, the illness must be part of an outbreak that is recognized, investigated, reported to public health authorities, and then reported to CDC. Thus, both systems have their own limitations to representativeness (Figure).
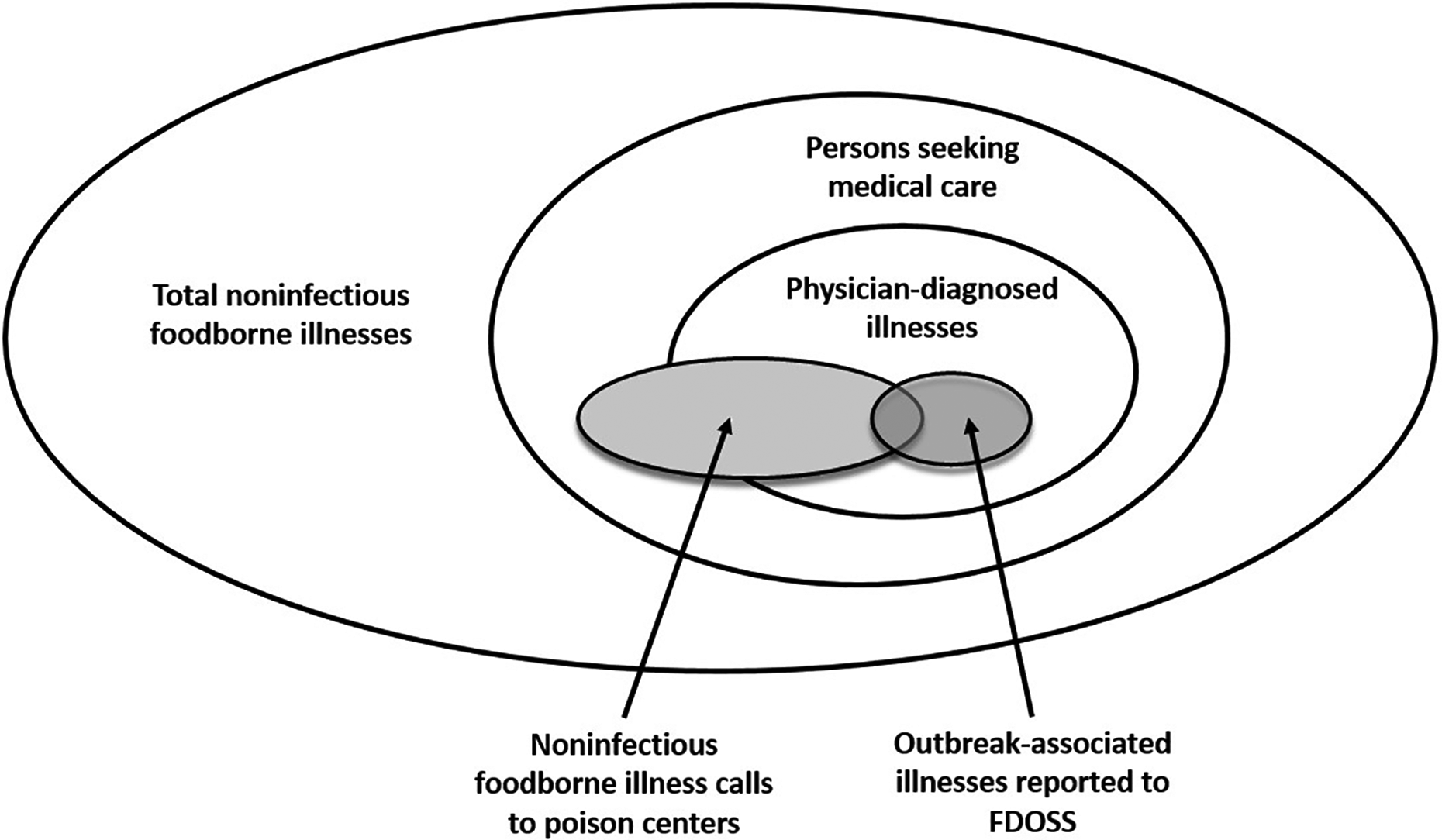
Schematic of total foodborne illnesses from noninfectious agents and the proportions of illnesses reported to poison centers and the Foodborne Disease Outbreak Surveillance System (FDOSS). 8
The primary objective of our study was to assess whether NPDS records can be used for surveillance of noninfectious FBDOs. We did this by determining whether outbreaks recorded in FDOSS were also captured in NPDS records. A second objective was to assess whether certain features of NPDS records were more likely than others to be associated with a noninfectious FBDO reported to FDOSS.
Methods
Data Sources
FDOSS
From 1998 through 2008, FBDO data were reported to FDOSS through a standard form in the electronic Foodborne Outbreak Reporting System. Since 2009, these data have been collected through a standard form in the web-based National Outbreak Reporting System. 7 Annual summaries and analyses of FDOSS reports are used to provide updates on the effects of FBDOs on human health. 3 We reviewed data on all outbreaks reported to FDOSS from 2000 through 2010 that had a noninfectious etiology. We excluded outbreaks with an unknown chemical or toxic etiology from the analysis because NPDS does not have a corresponding category for those etiologies. For our descriptive analysis and the matching process, we collected the following information on each outbreak: etiology, date of illness onset, reporting state, and number of persons affected.
NPDS
Poison centers collect standardized information on each call. This information includes the reported substance of exposure, the age and sex of the patient, and clinical and management data. Poison centers collect data into a local database and upload it to NPDS in real time (approximately every 8 minutes). We queried all NPDS records whose implicated substance matched the list of noninfectious FBDO etiologies in FDOSS data. Substances queried in NPDS were the following: amanita, ciguatera toxin, heavy metals (selenium, chromium, and cadmium), methomyl, monosodium glutamate, paralytic shellfish poison, scombroid toxin, and tetrodotoxin. 13 We queried data for the 11-year period 2000 through 2010. For our descriptive analysis and the matching process, we collected the following information from each NPDS record: date of call, sex and age of exposed person, reported state where the exposure occurred, whether the call was made by a health care professional, and severity of medical outcome. 10
Matching Poison Center–Reported Exposures to FDOSS Outbreaks
We matched NPDS records to outbreaks reported in FDOSS by etiology, state, and call date or date of first reported illness (±7 days) to identify events reported to FDOSS and captured by NPDS. We used 7 days before or after the date of first reported illness as the time frame for matching as a conservative estimate between the beginning of an outbreak as reported to FDOSS and a call to a poison center. 11,14 An NPDS record was coded as 1 if the call matched an outbreak reported to FDOSS by etiology, state, and date of illness (±7 days) and 0 if the call did not match an FDOSS outbreak.
In sensitivity analyses, we also matched reported events for shorter periods (±1 day, ±3 days, and ±5 days) than the ±7-day period.
Measures
The dependent variable was a dichotomous variable indicating whether or not the NPDS record was matched to an FDOSS outbreak by etiology, state, and date of illness (±7 days).
This study had 2 main independent variables. The first independent variable was whether the call to NPDS was made by a health care professional at a health care facility, coded as 1 if it was and 0 if the call was made by a member of the public (eg, patient, parent). The second independent variable was severity of medical outcome, which was ascertained by a follow-up call from a poison center staff member.
Severity of outcome was defined as death, major effect (the patient had symptoms as a result of the exposure that were life threatening or resulted in substantial residual disability or disfigurement), moderate effect (the patient had symptoms as a result of the exposure that were more pronounced than minor symptoms), minor effect (the patient had some symptoms that were minimally bothersome to the patient), no effect (the patient developed no symptoms as a result of the exposure), or not followed (the patient was not followed because the exposure was likely to result in only minimal toxicity). We tested a restricted definition of severity of medical outcome in the model, with “severe” defined as any reported illness resulting in death or major effect and “not severe” defined as any illness resulting in moderate effect, minor effect, no effect, or not followed.
Additional covariates of interest were etiology and age. Because of the many etiology types and different schemes for coding age in NPDS and to achieve the minimally acceptable level of statistical power and model stability, we transformed etiology into a dichotomous variable, which was coded 1 as marine-related (defined as illnesses related to ciguatera toxin, scombroid toxin, paralytic shellfish poison, or tetrodotoxin) and 0 as not marine-related. 15 We transformed age to a dichotomous variable: we coded patients aged ≥18 as 1 and patients aged <18 as 0. We included the dichotomous age variable in the model because poison centers receive a disproportionate number of calls related to children.
Analytic Approach
We addressed the first objective by assessing the percentage concordance of NPDS records with FDOSS outbreaks for time, state, and etiology. We hypothesized, on the basis of studies concluding that NPDS records have concordance with infectious FBDOs, that a high percentage of FDOSS noninfectious FBDO outbreaks would be included in NPDS exposure reports.
We addressed the second objective by using multivariable logistic regression on NPDS records to assess the relationship between an NPDS record that matched a confirmed noninfectious FBDO (dependent variable) and the 2 main independent variables (whether the call was made by a health care professional and severity of medical outcome).
We hypothesized that, compared with calls from members of the public, calls to poison centers by a health care professional would more accurately indicate a noninfectious FBDO. Not only would calls from health care professionals have a higher rate of case confirmation than calls from members of the public, but also health care professionals might be more likely than members of the public to report a potential FBDO to public health authorities. 14 We also hypothesized that NPDS records of exposures that had a severe medical outcome were more likely related to a reported noninfectious FBDO than were records with nonsevere medical outcomes.
We tested covariates and interactions between all predictors in the model. We determined model selection by using predefined criteria based on the Akaike information criterion. 15 We calculated odds ratios (ORs) for predictors in the model with 95% confidence intervals (CIs) and assessed goodness of fit by using the Hosmer-Lemeshow test. 15 We performed collinearity diagnostics to rule out multicollinearity among predictors. We considered P < .05 to be significant, and we conducted all analyses by using SAS version 9.3. 16
The Centers for Disease Control and Prevention Institutional Review Board reviewed this study and determined that it did not involve identifiable human subjects; therefore, further review was not required.
Results
During 2000-2010, FDOSS recorded information on 614 noninfectious FBDOs. Of these, 491 (80.0%) had a known etiology. Most of the 491 outbreaks of known etiology were caused by scombroid toxin (n = 287; 58.5%) or ciguatera toxin (n = 159; 32.4%) (Table 1). A median of 3 persons per outbreak were reported ill (range, 2-166).
Etiology of noninfectious outbreaks reported to the Foodborne Disease Outbreak Surveillance System (FDOSS) and exposure telephone calls reported to the National Poison Data System (NPDS) before and after matching, by etiology, 2000-2010a
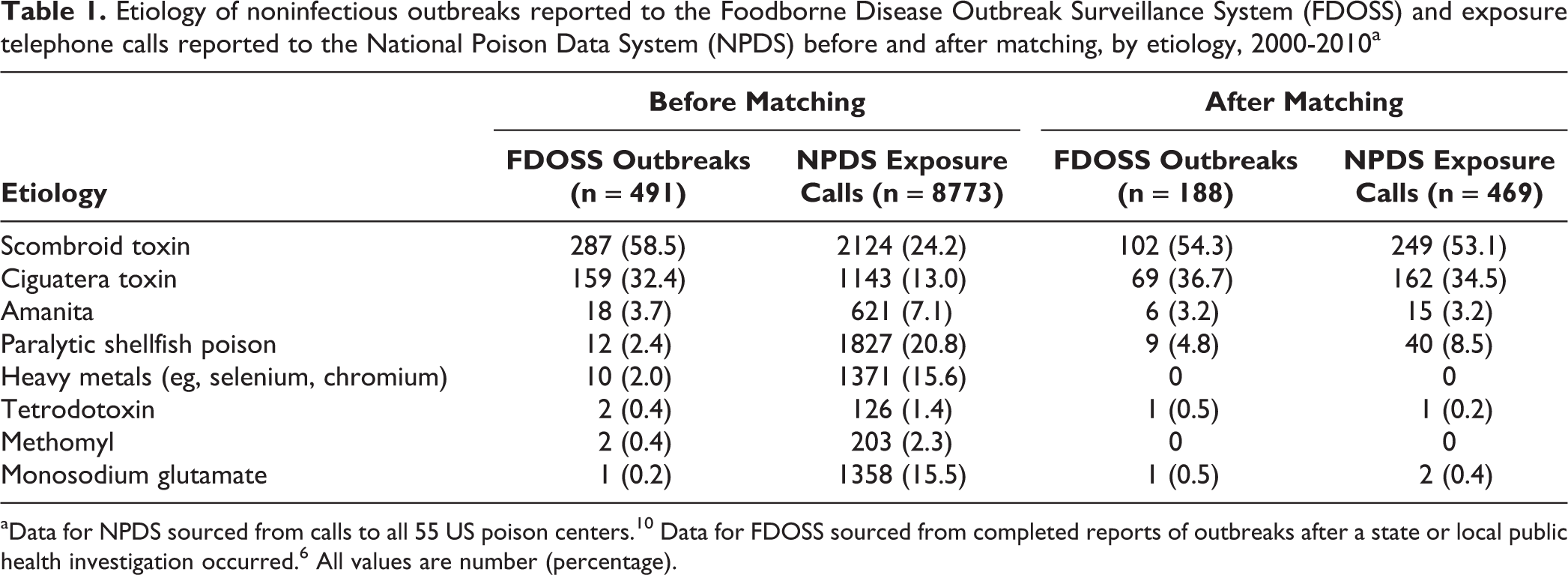
During 2000-2010, NPDS recorded information from 8773 telephone calls describing exposure to noninfectious foodborne disease. Of these, 2124 (24.2%) involved an exposure to scombroid toxin, 1827 (20.8%) to paralytic shellfish poison, and 1143 (13.0%) to ciguatera toxin (Table 1). Most calls were from members of the public (n = 7071; 80.6%) rather than from a health care professional (n = 1702; 19.4%). Most reports did not have a severe medical outcome (n = 8596; 98.0%).
Of 8773 NPDS records, 469 (5.3%) were matched to a noninfectious FBDO reported to FDOSS. These records represented 38.3% (188 of 491) of noninfectious FBDOs of known etiology in FDOSS. Of 469 matched NPDS records, 249 (53.1%) were for scombroid toxin and 162 (34.5%) were for ciguatera toxin (Table 1).
In the sensitivity analyses that matched records for shorter periods than the ±7-day period, we found a 56.3% (264 of 469) match for the ±1-day period, 78.9% (370 of 469) match for the ±3-day period, and 91.3% (428 of 469) match for the ±5-day period. Descriptive statistics of variables in NPDS records stratified by matching showed that most matched NPDS records did not have a severe medical outcome (n = 451; 96.2%), and most calls were made by members of the public (n = 322; 68.7%) (Table 2).
Characteristics of exposure telephone calls in the National Poison Data System (NPDS) matched and unmatched to a noninfectious outbreak reported in the Foodborne Disease Outbreak Surveillance System (FDOSS), 2000-2010a
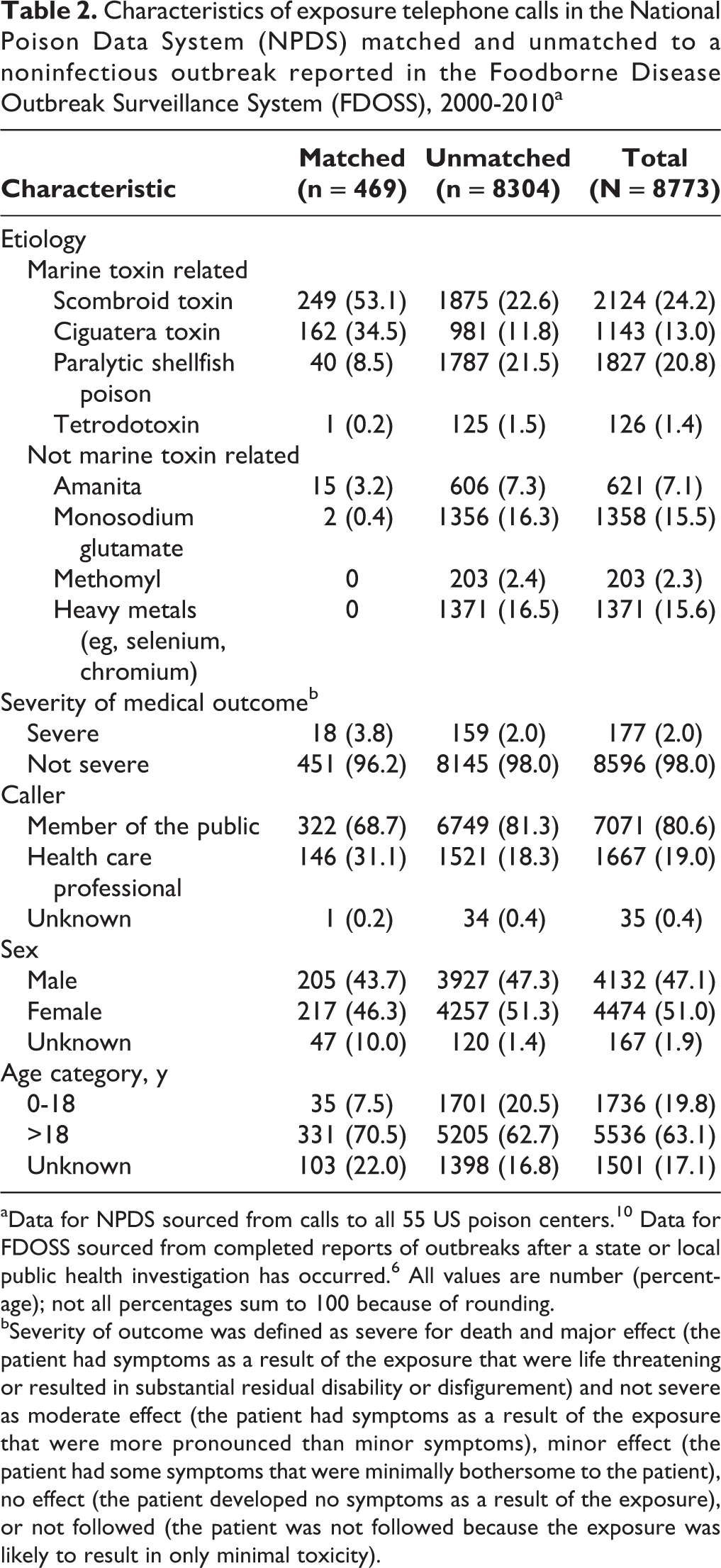
aData for NPDS sourced from calls to all 55 US poison centers. 10 Data for FDOSS sourced from completed reports of outbreaks after a state or local public health investigation has occurred. 6 All values are number (percentage); not all percentages sum to 100 because of rounding.
bSeverity of outcome was defined as severe for death and major effect (the patient had symptoms as a result of the exposure that were life threatening or resulted in substantial residual disability or disfigurement) and not severe as moderate effect (the patient had symptoms as a result of the exposure that were more pronounced than minor symptoms), minor effect (the patient had some symptoms that were minimally bothersome to the patient), no effect (the patient developed no symptoms as a result of the exposure), or not followed (the patient was not followed because the exposure was likely to result in only minimal toxicity).
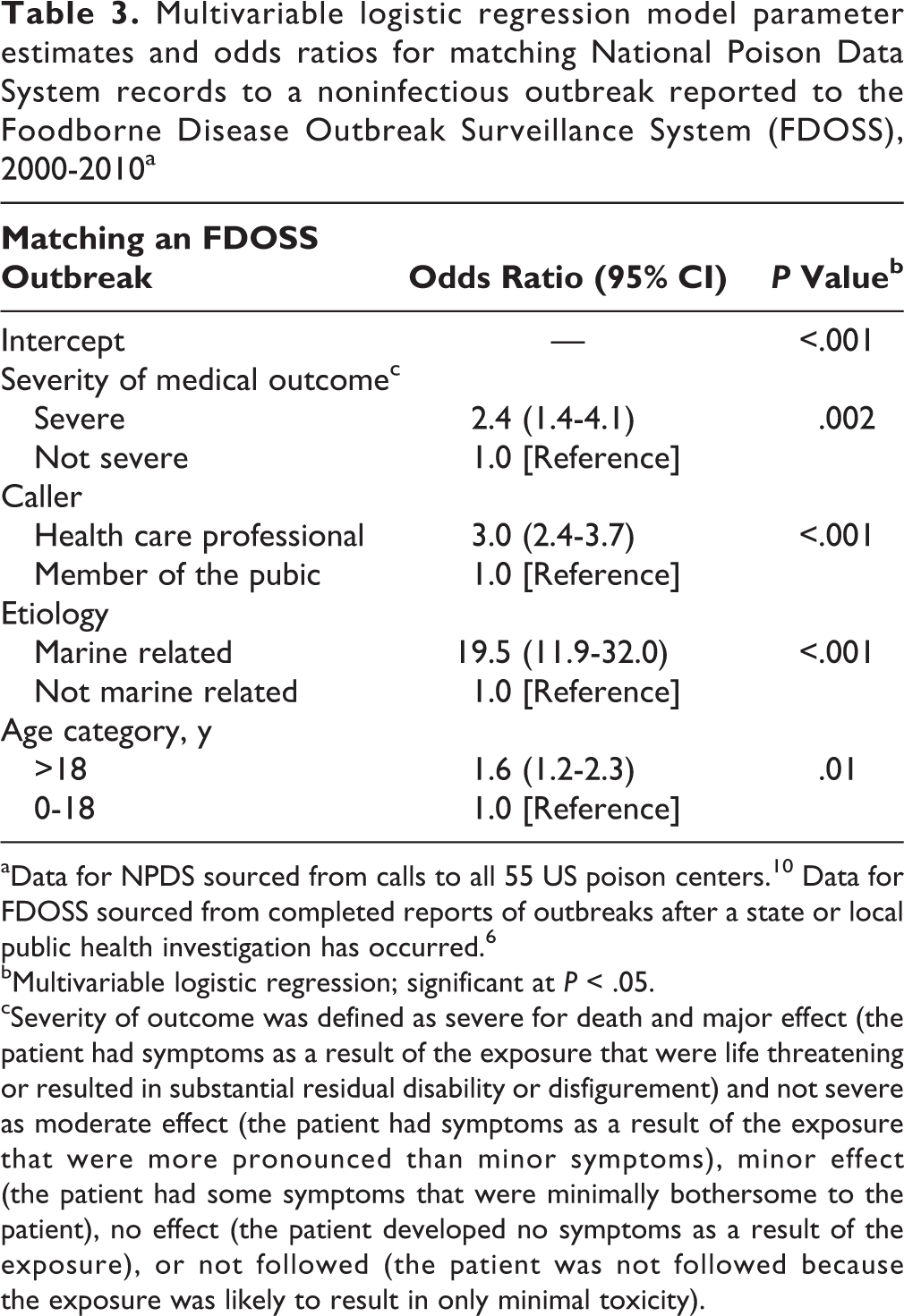
The multivariable logistic regression model indicated significant predictors of concordance between NPDS and FDOSS: severity of medical outcome, whether the call to NPDS was made by a health care professional, etiology, and age of patient. No interactions of model predictors were significant. As the severity of medical outcome of an NPDS call increased, so did the odds of the call being matched to a noninfectious FBDO (OR = 2.4; 95% CI, 1.4-4.1). Calls originating from a health care professional had higher odds of being matched to a noninfectious FBDO than did calls originating from members of the public (OR = 3.0; 95% CI, 2.7-3.7). Calls related to marine toxin exposures had higher odds of being matched to a noninfectious FBDO than did calls not related to a marine toxin exposure (OR = 19.5; 95% CI, 11.9-32.0) (Table 3).
Multivariable logistic regression model parameter estimates and odds ratios for matching National Poison Data System records to a noninfectious outbreak reported to the Foodborne Disease Outbreak Surveillance System (FDOSS), 2000-2010a
aData for NPDS sourced from calls to all 55 US poison centers. 10 Data for FDOSS sourced from completed reports of outbreaks after a state or local public health investigation has occurred. 6
bMultivariable logistic regression; significant at P < .05.
cSeverity of outcome was defined as severe for death and major effect (the patient had symptoms as a result of the exposure that were life threatening or resulted in substantial residual disability or disfigurement) and not severe as moderate effect (the patient had symptoms as a result of the exposure that were more pronounced than minor symptoms), minor effect (the patient had some symptoms that were minimally bothersome to the patient), no effect (the patient developed no symptoms as a result of the exposure), or not followed (the patient was not followed because the exposure was likely to result in only minimal toxicity).
All indices of model predictor conditions were low (1 to 4), suggesting no collinearity in the model predictors. The Hosmer-Lemeshow goodness-of-fit test suggested good fit (χ2 = 7.58; P = .37).
Discussion
Our findings suggest that NPDS captures data on a small percentage of noninfectious foodborne outbreak–associated illnesses, and they are consistent with the findings of a study by Derby et al 11 in 2005 that showed NPDS records can be a useful complement to existing state and local activities for surveillance of infectious foodborne illnesses. Our findings also suggest, as Derby et al also stated, that NPDS records represent a separate source of data that might indicate noninfectious FBDOs that were either not investigated or not reported. An NPDS record represents a single reported exposure or illness and might not indicate an outbreak. However, the specificity of data collected and the timeliness of data for public health use allow public health officials to respond to potential outbreaks sooner than they might when using other surveillance sources.
Our findings from the multivariable logistic regression model predictors suggest that particular features of NPDS records might be better than other features at indicating a noninfectious FBDO reported to FDOSS. NPDS records that indicated severe medical outcomes (rather than outcomes that were not severe) that originated from a health care professional (rather than a member of the public) and that were associated with exposures to marine toxins (rather than nonmarine toxins) had higher odds of being matched (rather than not matched) to a noninfectious FBDO reported to FDOSS. The rarity of noninfectious FBDO conditions may increase the likelihood that a health care professional will call a poison center. Physicians and other health care professionals may be more likely to call a poison center when they encounter an illness they do not commonly encounter. In addition, in some states, particularly in coastal regions, certain marine toxin exposures are reportable conditions, and such illnesses may be more likely to lead to a public health response. 17 -19
Our analysis suggests that in conducting surveillance for noninfectious FBDOs by using NPDS records, public health officials should pay particular attention to calls indicating a severe medical outcome, calls made by a health care professional, and calls indicating a marine toxin exposure. In addition, using these call features to identify subsets of NPDS records with noninfectious foodborne etiology that do not match an FDOSS outbreak might reveal suspected cases of noninfectious foodborne illness and noninfectious FBDOs that were either not investigated or not reported to FDOSS.
The results from this study show potential utility in conducting surveillance using NPDS for noninfectious foodborne-related exposures. However, because of resource limitations, public health officials might not be able to investigate every poison center call indicating a noninfectious source. We found that almost 40% of noninfectious FBDOs reported to FDOSS had a matching NPDS record, but only 5% of NPDS records matched an event in FDOSS. An NPDS record not matched to an FDOSS event might be a single case of noninfectious foodborne disease that was never reported to FDOSS because it was not part of an outbreak or did not warrant further public health action. Because of the high percentage of records potentially not related to a noninfectious FBDO, criteria for prioritizing the types of NPDS records most indicative of a noninfectious FBDO should be used to determine which NPDS calls warrant further investigation to most effectively use NPDS as a surveillance tool. The results from our study provide information on features of calls associated with a confirmed noninfectious FBDO and an initial framework for prioritizing which types of calls public health officials may want to investigate further.
This study focused on assessing whether NPDS can be used to identify outbreaks of noninfectious illness by comparing historical data from NPDS with data in FDOSS. Given that each surveillance system might capture a different subset of data on noninfectious foodborne illnesses in the United States, quantifying the differences as well as the overlap is critical to understanding the roles both systems can play in the surveillance of noninfectious FBDOs. Further studies are needed to assess how best to use NPDS for noninfectious foodborne surveillance.
Physicians call poison centers about toxins they are unfamiliar with, and the remote consultation that poison centers provide continues to be a valuable asset for health care professionals. By examining NPDS data, public health agencies can identify exposures that treating physicians may be unfamiliar with and can then provide appropriate education and outreach. An improved understanding of how and what types of noninfectious foodborne exposures NPDS captures can improve the collaboration among physicians, poison centers, and public health communities. This interaction will ultimately improve the ability to treat and respond to individual noninfectious foodborne exposures and noninfectious FBDOs.
Future studies should examine NPDS records not matched with FDOSS to quantify whether clusters of NPDS records represent noninfectious FBDOs not investigated by state and local public health or not reported to FDOSS. Future studies should also further examine the temporal relationship between NPDS records and illness onset reported to FDOSS to understand whether NPDS records precede or lag reported FBDOs.
Limitations
Our study had several limitations. Because the analysis matched NPDS records to outbreaks by etiology, state, and date of call, we cannot conclude that the NPDS records were definitively linked to an FDOSS outbreak. Also, we could assess only whether an NPDS record matched with an FDOSS outbreak, but we could not discern which case within the outbreak was matched or whether the matched NPDS record preceded or lagged the illness onset date of the noninfectious FBDO reported to FDOSS. Moreover, many records in NPDS rely on self-reported data from an exposed person or family member. Poison centers also receive calls about various substances for which no exposure is identified, so some noninfectious foodborne illnesses may have been missed. In contrast, outbreaks in FDOSS are related to probable or confirmed cases as reported by a local public health agency. 7
Conclusion
To our knowledge, our analysis is the first to assess the ability of NPDS to capture information on noninfectious FBDO-associated cases. We found that NPDS could be a potential source of near–real-time surveillance data to detect noninfectious foodborne illnesses. NPDS may complement existing noninfectious FBDO surveillance systems and response activities by providing timely information about single cases of foodborne disease or about a known or emerging outbreak. Prioritizing NPDS records by particular call features, such as calls originating from a health care facility, severity of medical outcome, and type of etiology, could help guide public health professionals in the types of noninfectious foodborne records that most warrant public health follow-up.
Footnotes
Authors’ Note
The findings and conclusions in this article are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention or the Agency for Toxic Substances and Disease Registry.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.