
Abstract
Objectives:
In North America, the illicit drug supply is increasingly contaminated by illicitly manufactured fentanyl. We sought to assess the level and source of fentanyl risk knowledge, defined as knowledge of the overdose risks associated with fentanyl, and characterize the prevalence and correlates of perceived risk of personally having a fentanyl overdose among persons who use illicit drugs (PWUD) in Vancouver, British Columbia.
Methods:
We derived data from 3 prospective cohorts of PWUD in Vancouver from December 2016 through May 2017. We used multivariable ordinal regression analysis to identify factors associated with a lower perceived risk of having a fentanyl overdose.
Results:
Of 1166 participants, 1095 (93.9%) had fentanyl risk knowledge. Of 1137 participants who answered questions about their perceived risk of having a fentanyl overdose, 398 (35.0%) perceived having no risk, 426 (37.5%) perceived having low risk, and 313 (27.5%) perceived having moderate or high risk. Never or rarely using opioids (n = 541, 65.7%) was the most common reason for reporting no or low perceived risk (n = 824), whereas 137 (16.6%) participants reported daily heroin use. In multivariable analysis, compared with participants who perceived a moderate or high risk, participants who perceived a lower risk were less likely to report a recent nonfatal overdose (adjusted odds ratio [aOR] = 0.28; P < .001), recent injection drug use (aOR = 0.34; P < .001), and awareness of recent exposure to fentanyl (aOR = 0.34; P < .001).
Conclusion:
Despite a high level of fentanyl risk knowledge, most study participants did not translate this knowledge into a risk of having an overdose. Although participants who perceived a lower risk were less likely to have had an overdose, a considerable proportion was engaged in daily opioid use, suggesting the need to improve overdose prevention efforts.
Opioids are the largest contributor to drug-related deaths worldwide: North America accounted for 25% of these deaths in 2016. 1 In that year, 63 632 deaths were caused by drug overdose in the United States, 66.4% of which were attributable to opioids. 2 These rates are likely underestimated as a result of incomplete cause-of-death reports. 3 In Canada, 3987 deaths were attributable to opioids in 2017, with the province of British Columbia having the highest rates. 4 In British Columbia, the key driver of the rise of overdose fatalities is fentanyl, a highly potent synthetic opioid, which has contaminated the illicit drug supply. 5 The rate of detection of fentanyl in illicit drug overdose deaths rose from 29% in 2015 to 84% in 2017. 6 In addition, the proliferation of fentanyl in the illicit drug supply was documented in a drug-checking pilot program in Vancouver, British Columbia. More than 90% of heroin samples and 5.9% of amphetamine/methamphetamine samples tested positive for fentanyl. 7
Research conducted before the fentanyl era found a range of risk factors for having a fatal or nonfatal opioid overdose. These risk factors included demographic characteristics (eg, male sex, young age, and <9 years of education), behavioral factors (eg, binge drug use, polydrug use, injecting alone, overdose within previous 5 years), and structural factors (eg, recent release from prison, time spent incarcerated, and engagement in drug treatment). 8 -11
As fentanyl-related deaths continue to rise in North America, research on fentanyl is needed to understand the distinct risk environment created by the contamination of the illicit drug supply with fentanyl. 1,2 The objective of our study was to describe the level and source of fentanyl risk knowledge and factors associated with perceiving a low risk of personally having a fentanyl overdose among persons who use illicit drugs (PWUD) in Vancouver, British Columbia.
Methods
We collected data from 3 ongoing prospective cohort studies of PWUD in Vancouver: the Vancouver Injection Drug Users Study (VIDUS), the AIDS Care Cohort to Evaluate Exposure to Survival Services (ACCESS), and the At-Risk Youth Study (ARYS). Details of these cohorts are available elsewhere. 12 -14 In brief, VIDUS enrolls HIV-seronegative adults (aged ≥18) who injected illicit drugs in the month before enrollment. ACCESS enrolls HIV-seropositive adults who used an illicit drug other than or in addition to cannabis in the month before enrollment. ARYS enrolls street-involved adolescents and young adults aged 14-26 who used an illicit drug other than or in addition to cannabis in the month before enrollment. The studies use harmonized data collection and follow-up procedures to allow for merged data analyses. Trained interviewers administer identical questionnaires and urine drug screens, and nurses draw blood samples for serologic tests for HIV and hepatitis C virus every 6 months. At each biannual study visit, participants receive CaD $40. All 3 studies received approval from the University of British Columbia/Providence Health Care Research Ethics Board.
We used data from the questionnaire administered from December 1, 2016, through May 31, 2017. We included in our analyses all participants who completed this questionnaire and reported using illicit drugs in the previous 6 months. Items on the questionnaire explored participants’ knowledge of the risks of fentanyl overdose, where they learned about overdose risks, and their perceived risk of personally having a fentanyl overdose.
We used 2 outcome variables. The first was a binary measure of fentanyl risk knowledge, defined as being able to identify an overdose risk associated with exposure to fentanyl (yes vs no). Participants were asked, “What do you know about the risks of fentanyl?” Responses categorized as having fentanyl risk knowledge were any of the following: “increased risk of overdose,” “high risk of fatal overdose,” “one dose of naloxone may not be effective,” and “fentanyl can cause respiratory complications.” The second outcome was defined as an ordinal variable of perceived risk of fentanyl overdose, derived from participants’ self-reported beliefs about how high or low they perceived their personal overdose risk to be due to fentanyl exposure. Trained interviewers provided a 4-category scale (no risk, low risk, moderate risk, and high risk) to participants, who then selected a response. If participants believed they had no risk or low risk, interviewers asked them to provide a reason for why they thought so. We merged the categories of moderate risk and high risk after inspecting the frequency of responses. Therefore, we coded the variable into 3 categories: no risk, low risk, and moderate or high risk (the reference category). A combination of open-ended and fixed-answer questions was used to assess both outcome measures. We created the fixed-answer questions on the basis of our 2 decades of experience working with this study population.
The explanatory variables of interest were the following demographic characteristics: age (continuous); sex (female vs male); ethnicity/ancestry (white vs nonwhite); residence in the Downtown Eastside neighborhood of Vancouver, an area known to be the epicenter of drug use in British Columbia 15 ; HIV status (positive vs negative); and education (≥secondary school vs <secondary school). Drug use–related variables were the following: injection drug use; daily use of heroin, stimulants (defined as powder/crack cocaine or crystal methamphetamine), prescription opioids (nonmedical use), or cannabis; previous nonfatal overdose of any kind of drugs; and exposure to fentanyl, derived from combining participants’ self-reports of possible exposure to fentanyl and results of the urine drug screen for fentanyl. We used a rapid chromatographic immunoassay, the BTNX Rapid Response Multi-drug Test Panel (BTNX Inc, Markham, Ontario), to qualitatively screen for fentanyl and norfentanyl at a cutoff value of 100 ng/mL and 20 ng/mL, respectively. We coded this variable into 3 categories of fentanyl exposure: no exposure (the reference category), defined as testing negative for fentanyl in a urine drug screen and self-reporting no possible exposure to fentanyl; unaware of exposure, defined as testing positive for fentanyl in a urine drug screen and self-reporting no possible exposure to fentanyl; and aware of exposure, defined as self-reporting having used fentanyl or any drugs they believe were contaminated with fentanyl, regardless of urine drug screen results. Other social/structural exposures were involvement in drug dealing, incarceration, and engagement in addiction treatment. We included the absence of fentanyl risk knowledge as an explanatory variable in a second analysis, which focused on the perceived risk of overdosing on fentanyl. All variables except for age, sex, education, and ethnicity/ancestry referred to the past 6 months. We coded all variables as yes or no unless otherwise stated.
We used bivariable logistic regression analysis to examine associations between the explanatory variables and a self-reported absence of fentanyl risk knowledge. We did not proceed to a multivariable model because a small number of participants identified as having no fentanyl risk knowledge. We used multivariable ordinal regression to identify factors associated with the perceived risk of fentanyl overdose. We verified the proportional odds assumption by using an unconstrained baseline logit model and a likelihood ratio test. 16,17 To merit inclusion into the multivariable model, explanatory variables had to be associated at the P < .10 level in bivariable analyses. In subanalyses, we examined descriptive statistics of participants’ reported source of knowledge of the risks associated with fentanyl use among participants who were characterized as having fentanyl risk knowledge. We also examined the reasons participants gave for reporting low risk or no risk of fentanyl overdose. In addition, we repeated the ordinal logistic regression analysis in a restricted sample of participants who reported using any opioids in the past 6 months. As a sensitivity analysis to account for the effect of residence in Downtown Eastside, we also constructed a generalized linear mixed model using Markov chain Monte Carlo techniques with the ordinal outcome of perceived risk of fentanyl overdose and the Downtown Eastside variable as random effects. We compared these results with the results of the conventional ordinal logistic regression models. 18 All P values were 2-sided and considered significant at P < .05, and all statistical analyses were conducted using R version 3.4.2. 19
Results
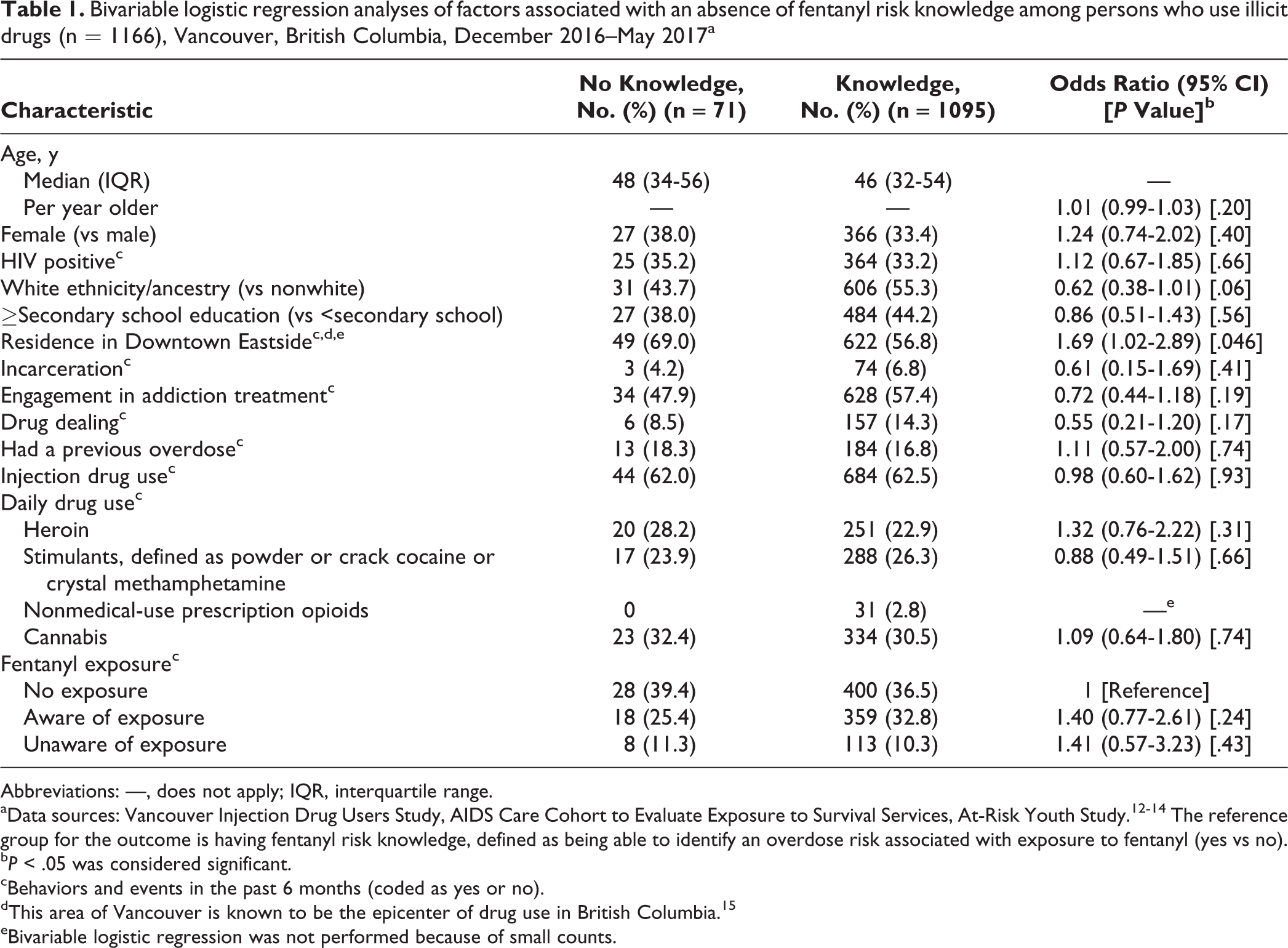
The sample consisted of 1166 participants; 393 (33.7%) were female, 637 (54.6%) were white, and the median age was 46 (interquartile range [IQR], 32-54). Most (n = 1095, 93.9%) participants had fentanyl risk knowledge; only 71 (6.1%) participants reported no fentanyl risk knowledge (Table 1). The demographic characteristics in both groups were generally similar. The only significant difference was that a higher percentage of participants who reported no fentanyl risk knowledge compared with participants who had fentanyl risk knowledge were living in Downtown Eastside (69.0% vs 56.8%; odds ratio [OR] = 1.69; 95% confidence interval [CI], 1.02-2.89).
Bivariable logistic regression analyses of factors associated with an absence of fentanyl risk knowledge among persons who use illicit drugs (n = 1166), Vancouver, British Columbia, December 2016–May 2017a
Abbreviations: —, does not apply; IQR, interquartile range.
aData sources: Vancouver Injection Drug Users Study, AIDS Care Cohort to Evaluate Exposure to Survival Services, At-Risk Youth Study. 12 -14 The reference group for the outcome is having fentanyl risk knowledge, defined as being able to identify an overdose risk associated with exposure to fentanyl (yes vs no).
bP < .05 was considered significant.
cBehaviors and events in the past 6 months (coded as yes or no).
dThis area of Vancouver is known to be the epicenter of drug use in British Columbia. 15
eBivariable logistic regression was not performed because of small counts.
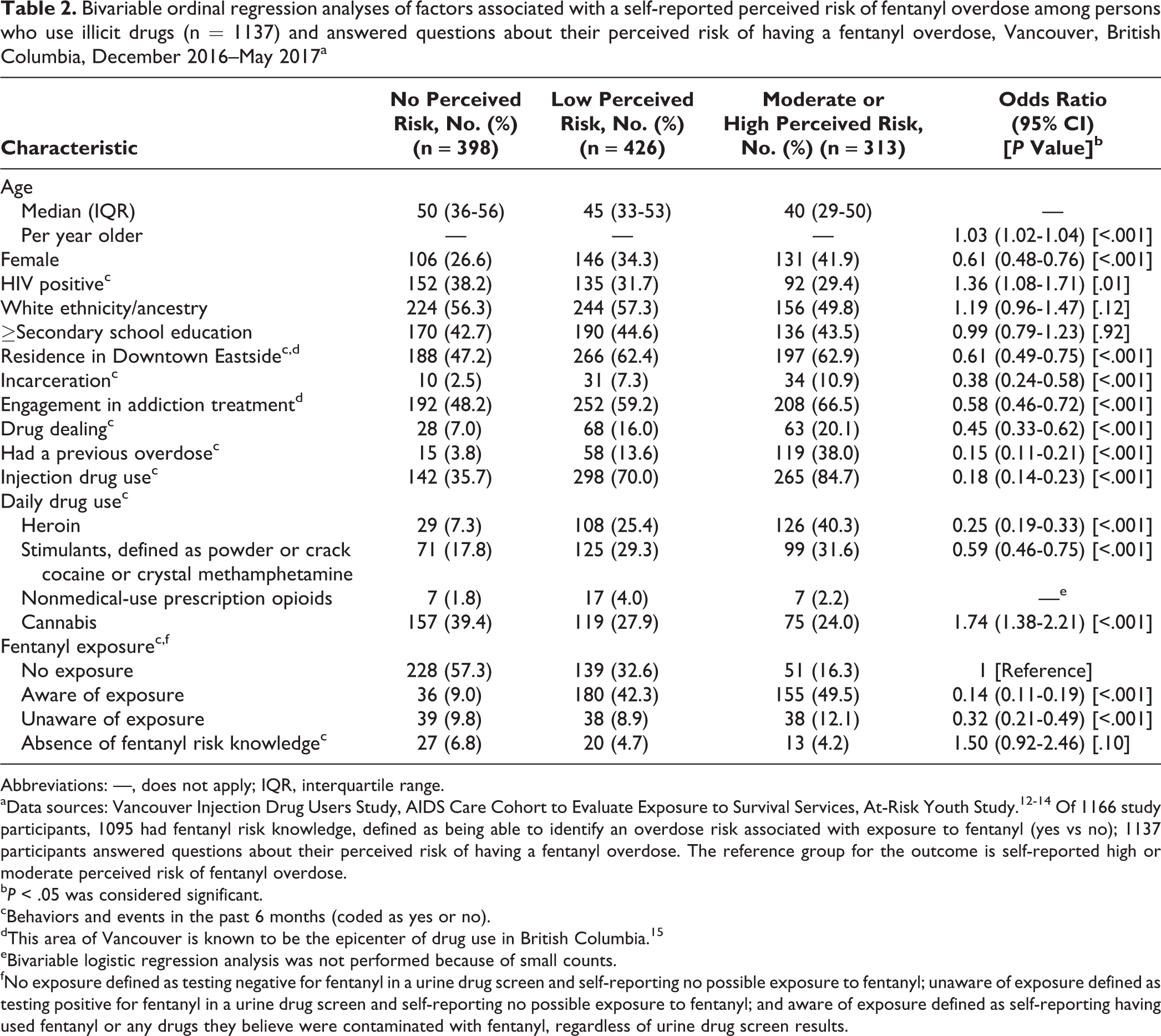
Of 1137 participants who answered questions about their perceived risk of fentanyl overdose, 383 (33.7%) were female, 624 (54.9%) were white, and the median age was 46 (IQR, 32-54) (Table 2). Among this sample, 398 (35.0%) reported having no risk, 426 (37.5%) reported having low risk, and 313 (27.5%) reported having a moderate or high risk of fentanyl overdose. Among 824 participants who perceived no risk or low risk of overdosing on fentanyl, 137 (16.6%) reported daily heroin use and 77 (9.3%) were unknowingly exposed to fentanyl.
Bivariable ordinal regression analyses of factors associated with a self-reported perceived risk of fentanyl overdose among persons who use illicit drugs (n = 1137) and answered questions about their perceived risk of having a fentanyl overdose, Vancouver, British Columbia, December 2016–May 2017a
Abbreviations: —, does not apply; IQR, interquartile range.
aData sources: Vancouver Injection Drug Users Study, AIDS Care Cohort to Evaluate Exposure to Survival Services, At-Risk Youth Study. 12 -14 Of 1166 study participants, 1095 had fentanyl risk knowledge, defined as being able to identify an overdose risk associated with exposure to fentanyl (yes vs no); 1137 participants answered questions about their perceived risk of having a fentanyl overdose. The reference group for the outcome is self-reported high or moderate perceived risk of fentanyl overdose.
bP < .05 was considered significant.
cBehaviors and events in the past 6 months (coded as yes or no).
dThis area of Vancouver is known to be the epicenter of drug use in British Columbia. 15
eBivariable logistic regression analysis was not performed because of small counts.
fNo exposure defined as testing negative for fentanyl in a urine drug screen and self-reporting no possible exposure to fentanyl; unaware of exposure defined as testing positive for fentanyl in a urine drug screen and self-reporting no possible exposure to fentanyl; and aware of exposure defined as self-reporting having used fentanyl or any drugs they believe were contaminated with fentanyl, regardless of urine drug screen results.
The multivariable analysis showed that participants who perceived a lower risk of fentanyl overdose, compared with participants who perceived a moderate or high risk, were significantly less likely to report the following within the previous 6 months: incarceration (adjusted OR [aOR] = 0.50; 95% CI, 0.27-0.93), engagement in addiction treatment (aOR = 0.73; 95% CI, 0.55-0.96), an overdose (aOR = 0.28; 95% CI, 0.19-0.42), injection drug use (aOR = 0.34; 95% CI, 0.24-0.47), and awareness of exposure to fentanyl (aOR = 0.34; 95% CI, 0.24-0.48) (Table 3). Age remained independently and positively associated with a lower perceived risk of fentanyl overdose (aOR = 1.02; 95% CI, 1.01-1.04). Absence of fentanyl risk knowledge was not significantly associated in bivariable analyses (OR = 1.50; 95% CI, 0.92-2.46) and therefore was not included in the multivariable model. The generalized linear mixed model used to account for the effects of residence in Downtown Eastside did not alter our results.
Multivariable ordinal regression analysis of factors associated with a self-reported perceived risk of fentanyl overdose among persons who use illicit drugs (n = 1137) and answered questions about their perceived risk of having a fentanyl overdose, Vancouver, British Columbia, December 2016–May 2017a
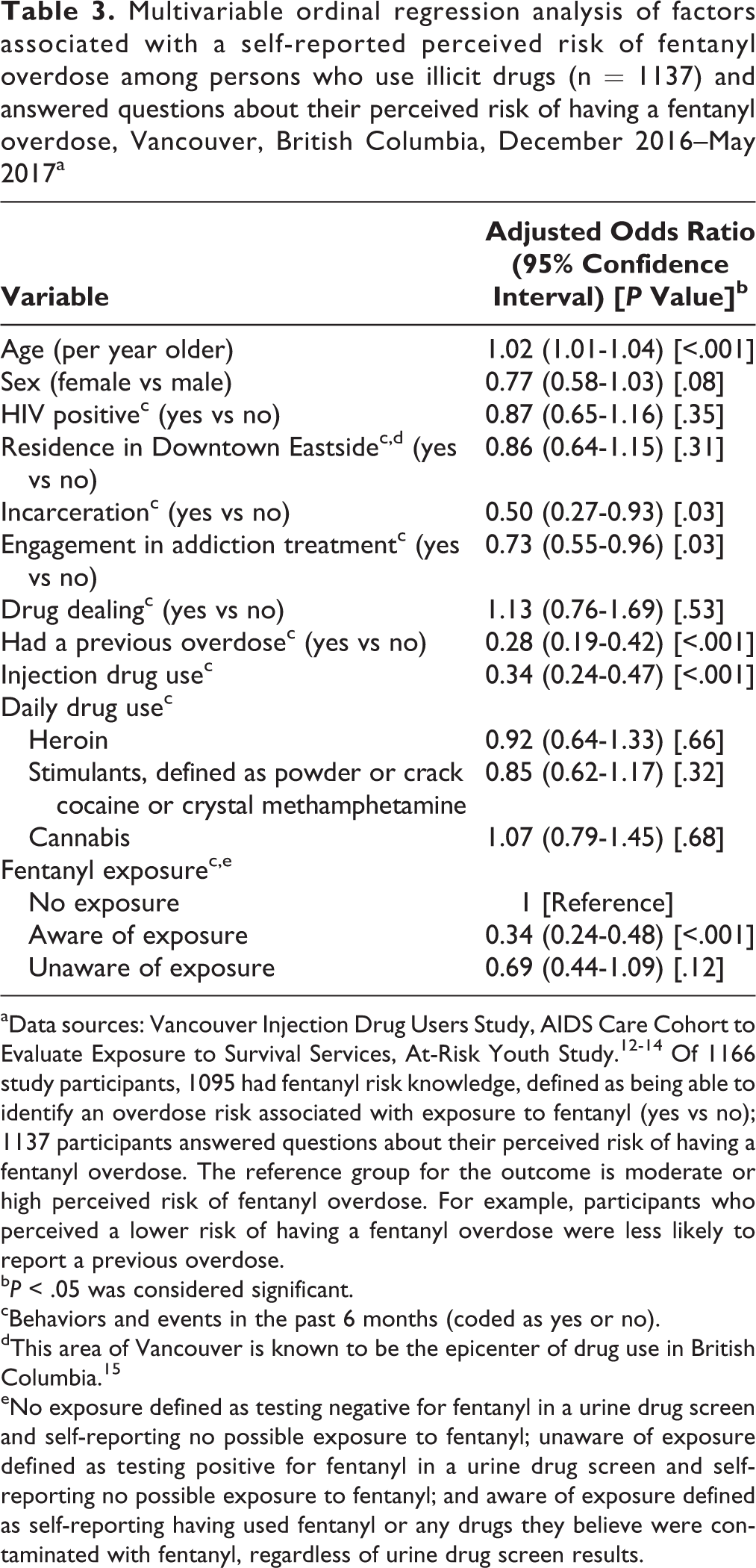
aData sources: Vancouver Injection Drug Users Study, AIDS Care Cohort to Evaluate Exposure to Survival Services, At-Risk Youth Study. 12 -14 Of 1166 study participants, 1095 had fentanyl risk knowledge, defined as being able to identify an overdose risk associated with exposure to fentanyl (yes vs no); 1137 participants answered questions about their perceived risk of having a fentanyl overdose. The reference group for the outcome is moderate or high perceived risk of fentanyl overdose. For example, participants who perceived a lower risk of having a fentanyl overdose were less likely to report a previous overdose.
bP < .05 was considered significant.
cBehaviors and events in the past 6 months (coded as yes or no).
dThis area of Vancouver is known to be the epicenter of drug use in British Columbia. 15
eNo exposure defined as testing negative for fentanyl in a urine drug screen and self-reporting no possible exposure to fentanyl; unaware of exposure defined as testing positive for fentanyl in a urine drug screen and self-reporting no possible exposure to fentanyl; and aware of exposure defined as self-reporting having used fentanyl or any drugs they believe were contaminated with fentanyl, regardless of urine drug screen results.
In a subanalysis, of the 1095 participants with fentanyl risk knowledge, most (60.3%; n = 660) participants reported learning about the risks of fentanyl from other PWUD (Table 4). Other common sources of knowledge were related to knowledge of a fentanyl overdose. For example, 242 (22.1%) participants reported knowing someone who had overdosed on fentanyl. Similarly, 167 (15.3%) participants reported witnessing a stranger overdosing on fentanyl, and 95 (8.7%) participants reported having their own fentanyl overdose as a source of knowledge.
Self-reported sources of fentanyl risk knowledge among study participants categorized as having fentanyl risk knowledge (n = 1095) among persons who use illicit drugs, Vancouver, British Columbia, December 2016–May 2017a
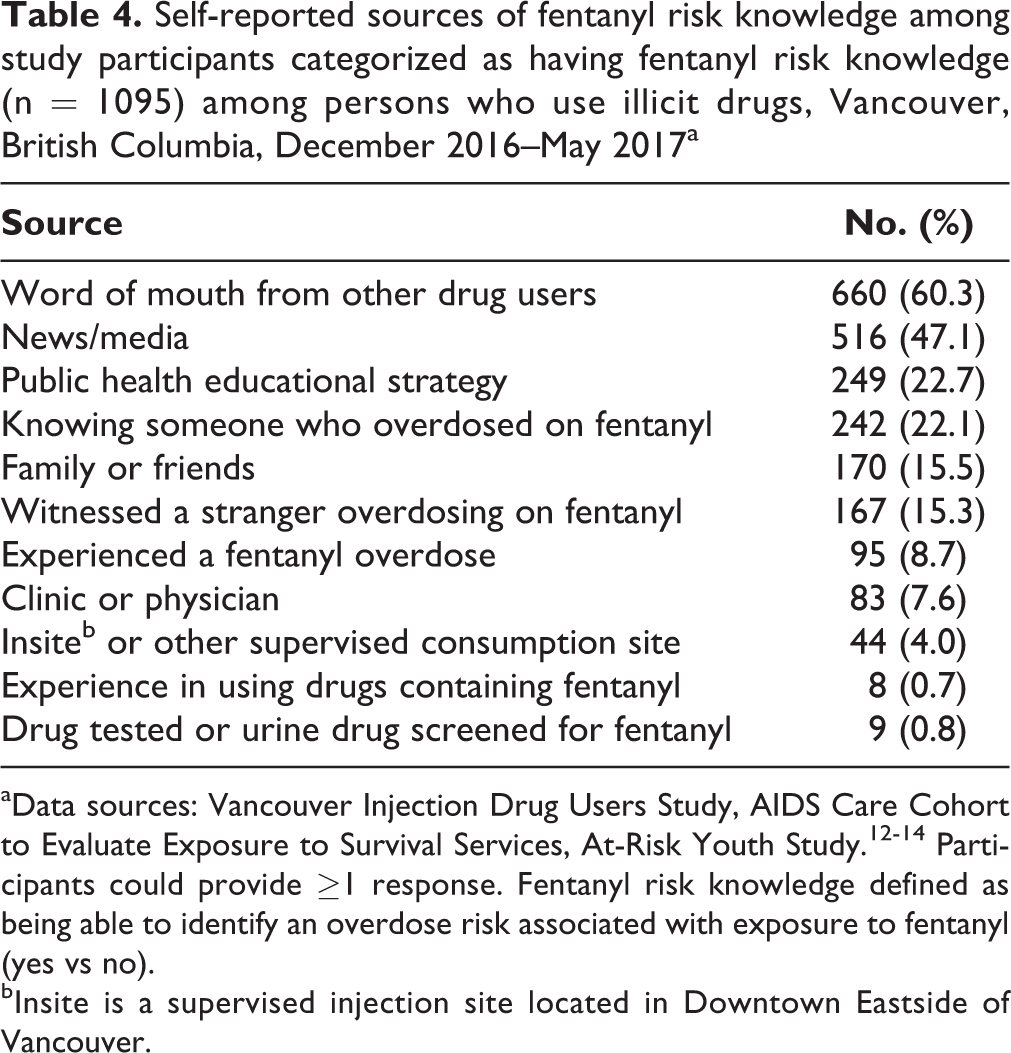
aData sources: Vancouver Injection Drug Users Study, AIDS Care Cohort to Evaluate Exposure to Survival Services, At-Risk Youth Study. 12 -14 Participants could provide ≥1 response. Fentanyl risk knowledge defined as being able to identify an overdose risk associated with exposure to fentanyl (yes vs no).
bInsite is a supervised injection site located in Downtown Eastside of Vancouver.
In total, 824 participants provided reasons for reporting no or low risk of fentanyl overdose (Table 5). The most commonly reported reason was never or rarely using opioids (65.7%; n = 541), followed by knowing the source or provider of drugs obtained (20.9%; n = 172) and taking cautious measures (12.5%; n = 103).
Reasons given by study participants (n = 824) for having no perceived risk or low perceived risk of a fentanyl overdose among persons who use illicit drugs, Vancouver, British Columbia, December 2016–May 2017a
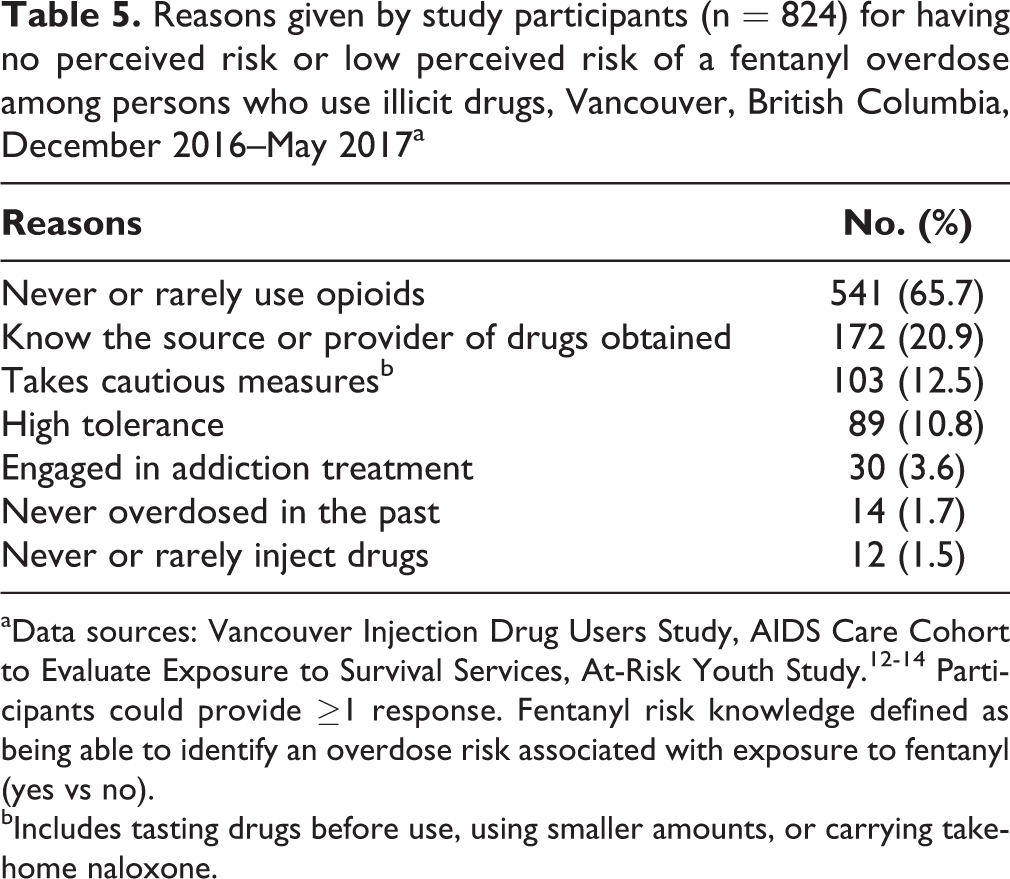
aData sources: Vancouver Injection Drug Users Study, AIDS Care Cohort to Evaluate Exposure to Survival Services, At-Risk Youth Study. 12 -14 Participants could provide ≥1 response. Fentanyl risk knowledge defined as being able to identify an overdose risk associated with exposure to fentanyl (yes vs no).
bIncludes tasting drugs before use, using smaller amounts, or carrying take-home naloxone.
Among a subsample of 585 opioid users, 98 (16.8%) reported having no risk, 253 (43.2%) reported having low risk, and 234 (40.0%) reported having a moderate or high risk of overdosing on fentanyl. When repeating the ordinal logistic regression analysis among this sample, the results essentially remained the same, except that engagement in addiction treatment was not significantly associated with the perceived risk of overdosing on fentanyl.
Discussion
In our community-recruited sample of PWUD, almost all participants (93.9%) had knowledge of fentanyl risk. Despite this high level of knowledge, almost three-quarters (72.5%) of the sample (or 60.0% of opioid users) perceived their risk of fentanyl overdose as nonexistent or low. Never or rarely using opioids was the main reason for perceiving low risk, but substantial proportions of those who perceived no risk or low risk used heroin daily (16.6%) or were unknowingly exposed to fentanyl (9.3%). Furthermore, 20.9% reported feeling safe because they knew the source or provider of the drugs they consumed. Given the documented proliferation of illicit fentanyl in the local drug supply, including nonopioids, knowing a source or provider of drugs may not reduce the risk of overdose. Some PWUD had an overdose, despite reporting a consistent provider of illicit drugs. 20,21
To our knowledge, ours is the first study to examine perception of fentanyl overdose risk. Participants who perceived their risk of fentanyl overdose as lower were less likely than those who perceived a moderate or high risk to have had a nonfatal overdose or to self-report exposure to fentanyl. This finding is consistent with previous literature showing that experiences of nonfatal overdose are associated with higher perceived risk of opioid overdose. 9,22 Because nonfatal overdose is a risk factor for subsequent overdoses, 8,22 -25 it is important to emphasize overdose prevention interventions among persons who have had an overdose. Our findings suggest that persons who have recently had a nonfatal overdose might be amenable to overdose prevention interventions because they have a higher perceived risk of overdosing on fentanyl. However, it may only be a matter of time before persons who perceive a low risk of overdosing on fentanyl will have an opioid overdose, considering that opioid use and exposure to fentanyl were common among our study participants. Therefore, it is important to improve overdose education efforts among this population. A drug-checking service (a service that allows persons to chemically screen their substances for contaminants) may be a useful strategy to increase awareness of overdose risk due to fentanyl contamination. 7 However, evidence of the effect of such drug testing interventions is lacking. 26
Participants who injected drugs were less likely than participants who did not inject drugs to perceive a lower risk of fentanyl overdose. Our findings are consistent with research that established injection drug use as a risk factor for fatal and nonfatal overdose. 8,10 Our findings suggest that the perception of overdose risk was generally accurate among our sample of PWUD. A previous study among a sample of persons who inject drugs found an association between a higher perceived susceptibility to having a nonfatal overdose and intention to engage in harm-reduction behavior. 27 However, the extent to which heightened perception of overdose risk influences behavioral harm-reduction strategies remains to be scrutinized. Although motivating persons who inject drugs to engage in protective behavioral strategies is important, structural changes are also necessary to prevent contamination of the illicit drug supply. For example, several studies have shown that medication-assisted treatments were the most effective treatment for persons with opioid use disorder. 28 -31 However, medications available for prescription are limited in Canada and the United States, especially for persons who inject illicit opioids. 28,32,33 A systematic review in 2006 showed how improving access to opioid agonist treatments, such as heroin maintenance therapy, was an effective treatment for persons who inject illicit opioids. 28
Our findings also suggest that within the previous 6 months, persons who were incarcerated were less likely than persons who were not incarcerated to perceive their risk of fentanyl overdose as lower. This finding is in line with previous qualitative research showing that incarcerated PWUD had difficulties with abstinence after release; these difficulties could increase the risk of overdose because drug tolerance may have been reduced during incarceration. 34 Incarceration is a well-documented risk factor for overdose, particularly immediately after release. 34 -36 Interventions are needed to assist in the transition between correctional settings and the community; this transition should include the continuum of, and linkages to, opioid agonist treatments among persons who use opioids. 37 In addition, upstream policy changes, such as decriminalization of personal use and possession of illicit substances, could alleviate the overdose risk created by incarceration of persons with such charges. This strategy reduced drug-related mortality in Portugal. 38
The negative association between engagement in addiction treatment and a lower perceived risk of fentanyl overdose appears to be a new finding. One possible interpretation is that a higher perceived risk of fentanyl overdose may elevate willingness to engage in addiction treatment. This finding is harmonious with motivational models of treatment engagement, in which a primary reason to participate in treatment is to evade adverse consequences of use. 39 -41 One study reported that known fentanyl exposure may elicit treatment-seeking behaviors. 20 Furthermore, engagement in addiction treatment, specifically opioid agonist treatments, was shown to be associated with reduced overdose and all-cause mortality. 8,24,42 However, previous research has also shown that addiction treatment may increase the risk of overdose among some patients, particularly patients who prematurely terminate treatment and use drugs or resume using drugs after a period of abstinence through withdrawal management or other treatment modalities. 43 -45 Our finding may reflect this potential adverse consequence of treatment and emphasize the need to provide overdose prevention education and tools to patients in treatment.
Most of our sample had fentanyl risk knowledge, and the most commonly reported source of receiving this knowledge was through word of mouth. Internationally, peer-based interventions have increased positive health outcomes for drug-using populations. 46 -48 Our finding suggests that peer-led overdose education may improve the spread of knowledge among PWUD social networks.
Limitations
This study had several limitations. First, as with all studies that use self-reported data, our study methods may have introduced response bias. Second, most of our sample was aware of the risk of fentanyl, which limited our ability to explore an absence of fentanyl risk knowledge in the multivariable model. Third, the cohorts were not randomly recruited, and recruitment was done through nonprobability sampling methods. These methods reduced the generalizability of our results to all populations of PWUD. Finally, because our study had a cross-sectional design, temporal relationships could not be established between exposures and outcomes.
Conclusions
Our findings indicate that despite high levels of knowledge of the risks of fentanyl, only about one-quarter of our sample of PWUD perceived their risk of overdosing on fentanyl as moderate or high. Among study participants who perceived their overdose risk as nonexistent or low, the prevalence of heroin use and exposure to fentanyl was not low. Although these study participants were less likely than those who perceived a moderate or high risk to have had an overdose or have known risk factors for overdose, they are not immune to an overdose, given the proliferation of fentanyl in the illicit drug supply in our study setting. Overall, our findings suggest that knowledge of fentanyl overdose risk may be insufficient to motivate protective behaviors among PWUD at risk of being exposed to fentanyl. Innovative measures to address the contaminated drug supply and better connect PWUD with overdose prevention services are warranted.
Footnotes
Acknowledgments
The authors thank the study participants for their contribution to the research, as well as current and past researchers and staff members.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was supported by the US National Institutes of Health (U01DA038886, U01DA021525). This research was undertaken, in part, thanks to funding from the Canada Research Chairs program through a Tier 1 Canada Research Chair in Inner City Medicine, which supports Evan Wood (Director of BC Centre on Substance Use), and the Canadian Institutes of Health Research (CIHR) through the Canadian Research Initiative on Substance Misuse (SMN-139 148). Kanna Hayashi is supported by a CIHR New Investigator Award (MSH-141 971), a Michael Smith Foundation for Health Research (MSFHR) Scholar Award, and the St. Paul’s Foundation. MJ Milloy is supported by a CIHR New Investigator Award, an MSFHR Scholar Award, and the US National Institutes of Health (U01DA0251525). His institution received an unstructured gift from NG Biomed, Ltd, to support his research. He is the Canopy Growth Professor of Cannabis Science at the University of British Columbia, a position established by arm’s-length gifts to the university by Canopy Growth, a licensed producer of cannabis, and the Government of British Columbia’s Ministry of Mental Health and Addictions. Kora DeBeck is supported by an MSFHR/St. Paul’s Hospital Foundation-Providence Health Care Career Scholar Award. Nadia Fairbairn is supported by an MSFHR/St. Paul’s Hospital Foundation Scholar Award.