
Abstract
Objectives:
Before implementation of the Affordable Care Act, many uninsured women in Illinois received care through safety-net programs. The new law allowed them to acquire health insurance through Medicaid or the Illinois Health Exchange. We examined (1) the health care experiences of such women who previously used a safety-net program and acquired this new coverage and (2) persisting gaps in coverage for breast and cervical cancer services and other health care services.
Methods:
We interviewed a stratified random sample of 400 women aged 34-64 in Illinois each year during 2015-2017 (total N = 1200). We used multivariable logistic regression models to determine the association between health insurance status (Illinois Health Exchange vs Medicaid) and past 12-month gaps in coverage (ie, delaying care, not having a recent mammogram, having a medical cost, and having a medical cost not covered) for the 360 women who were former participants of the Illinois Breast and Cervical Cancer Program. We calculated odds ratios (ORs) and 95% confidence intervals (CIs), adjusting for race/ethnicity, age, income, and education.
Results:
We found no significant differences by health insurance status in the prevalence of delaying preventive, chronic, or sick care; timeliness of the most recent mammogram; and having a major medical cost. However, of women who reported a major medical cost, women with health insurance through the Illinois Health Exchange had a higher prevalence of not having a cost covered than women with Medicaid (adjusted OR = 4.86; 95% CI, 1.48-16.03).
Conclusions:
The results of this study suggest that many women who gained health insurance lacked adequate coverage and services. Safety-net programs will likely continue to play an essential role in supporting women as they navigate a complex system.
Keywords
After implementation of the Patient Protection and Affordable Care Act, 1 the percentage of US women aged 19-64 who were uninsured fell from 17% in 2013 to 11% in 2016. 2 Women who gained health insurance after implementation of the Affordable Care Act had 2 pathways to coverage: through Medicaid or through state or federal health exchanges. Benefits for women under the Affordable Care Act include preventive care services, many without cost sharing, but little is known about women’s experiences with their new health care coverage.
A 2016 study documented changes in women’s benefits after implementation of the Affordable Care Act and suggested the need for further research to determine how women’s access to health care has been affected, including exploring gaps in coverage and services. 3 A systematic review of studies focused on barriers that were associated with high-deductible health plans showed a decrease in the use of health care services, including preventive services. This review advocated for future research to differentiate the use of services between plans obtained through a health exchange and all private, high-deductible plans. 4 To our knowledge, no studies have captured data on differences in the experiences of previously uninsured women who gained coverage through Medicaid versus the health exchanges. Documenting these differences is important for ensuring that the benefits of the Affordable Care Act are maximized.
The Illinois Breast and Cervical Cancer Program (IBCCP), funded through the Centers for Disease Control and Prevention’s National Breast and Cervical Cancer Early Detection Program, has served as a safety-net program for women in Illinois since 1995. 5 IBCCP provides free mammograms, breast examinations, pelvic examinations, Papanicolaou (Pap) tests, clinical navigation (for uninsured and insured women), and a program to pay for the high deductibles of insured women in need of diagnostic testing, including mammograms, through lead agencies (local health departments, federally qualified health centers, hospitals, and community-based organizations) across the state. Since implementation of the Affordable Care Act, many Illinois women have gained health insurance coverage and transitioned out of IBCCP. However, it is unclear if these women are then able to access the needed services that were previously offered to them through IBCCP.
Because of the changes in health insurance coverage as a result of the Affordable Care Act, the University of Illinois at Chicago (UIC) School of Public Health IBCCP evaluation team conducted Women’s Health Surveys in 2015, 2016, and 2017 of current, former, and new IBCCP enrollees. One aim of these surveys was to assess how women who were previously eligible for IBCCP were faring in the health care system transition. Another aim was to document the access and service delivery issues they encountered. The primary objective of our study, which was based on the unpublished results of these surveys, was to examine the health care experiences of women who previously used IBCCP and transitioned to Medicaid or obtained coverage through the Illinois Health Exchange. A secondary objective was to determine any gaps in coverage for breast and cervical cancer services and other health care services for these women.
Methods
We drew a stratified random sample of participants from the IBCCP administrative database (1600 women in 2015, 1600 women in 2016, and 1471 women in 2017) based on enrollee group (current IBCCP participants, former IBCCP participants, new IBCCP participants) and IBCCP lead agency location (Cook County and surrounding suburban “collar” counties [ie, DuPage, Kane, Lake, McHenry, and Will) vs other counties) for the Women’s Health Survey. We oversampled former IBCCP participants versus current and new IBCCP participants in a ratio of 2:1. We also oversampled women not in Cook County or the surrounding suburban counties to ensure that at least 50% of the sample was from outside of the metropolitan Chicago area. Lead agency location is defined by the location of the lead agency according to the Urban–Rural Classification System. 6 Women were informed by mail that they would be contacted by the IBCCP evaluation team at the UIC School of Public Health. The IBCCP lead agencies facilitated mailings by allowing the use of their own envelopes to ensure that participants would recognize the organization’s mailing address. The University of Illinois Institutional Review Board approved this study.
Participants included in the current study were Illinois women aged 34-64 who were former IBCCP clients. A team of 6 UIC School of Public Health graduate students, including one of the authors (C.J.B.), conducted telephone interviews in English and Spanish and entered data into a secure, web-based REDCap database. 7 Women received a $10 gift card for participating.
The interview included the following questions about current health insurance and gaps in coverage: What type of health insurance do you currently have or are registered for? Options were: insurance from the Illinois Health Exchange, Medicaid, insurance through a current or former employer or union, and uninsured. In the past 12 months, have you delayed or gone without preventive care, screening tests, or a check-up? In the past 12 months, have you delayed or gone without care for a chronic condition such as diabetes or hypertension? In the past 12 months, have you delayed or gone without care when you were sick, such as when you had the flu or an infection? When was the month and year of your last mammogram? During the past 12 months, did you have any major medical costs that were not covered by your insurance or Medicaid? We considered participants to have had a major medical cost if they answered, “Had a major medical cost, covered or not covered.”
We defined gaps in coverage as the following: whether participants delayed or went without preventive care, care for a chronic condition, or care when they were sick; whether they did not have a mammogram in the past 12 months (recent mammogram according to IBCCP protocol); and whether they had a major medical cost and that cost was not covered by their current health insurance. Survey responses were linked to demographic data from the IBCCP administrative database.
Interviews were completed with 400 women each in 2015, 2016, and 2017 (total N = 1200). We restricted our current study to women who were formerly enrolled in IBCCP, reported health insurance coverage at the time of the interview, and were not lost to follow-up (n = 360); we excluded 840 women from the study who did not meet inclusion criteria. We further restricted most analyses to former IBCCP participants who self-reported current health insurance coverage obtained through either Medicaid or the Illinois Health Exchange. We weighted data according to the probability of being sampled and completing the survey in each stratum, to be representative of all former IBCCP participants. In all analyses, we accounted for the complex sampling design to estimate standard errors.
We calculated weighted percentages with 95% confidence intervals (CIs). We used the Pearson χ2 test to examine significant differences by current health insurance group, with P < .05 considered significant. We used multivariable logistic regression models to determine the associations between current health insurance status (Illinois Health Exchange vs Medicaid) and gaps in coverage (ie, delaying care, timeliness of most recent mammogram, having a major medical cost, and having a major medical cost not covered), adjusting for race/ethnicity, age, income, and education. We conducted quantitative analyses by using SAS version 9.4. 8
Interviewers also recorded qualitative responses to 3 open-ended questions about women’s experiences with health care, current health insurance, and IBCCP: (1) How would you describe your health care experiences, in general, in the past year? (2) What are the most important positive or negative issues or experiences with your insurance situation that you would like to share? and (3) Is there anything else you would like to share about the IBCCP?
A total of 209 women provided qualitative comments. Two independent raters read responses to the 3 questions and grouped the comments into 5 categories: (1) experiences with health care, (2) experiences with IBCCP, (3) experiences with health insurance, (4) comments about personal health, and (5) other. The raters then recategorized each comment as positive, negative, or neutral and developed the following subcategories: perception of health insurance as expensive, experiencing confusion about health insurance, and other issues. We analyzed categories for co-occurrence and stratified them by current health insurance status. We used Dedoose version 8.0.35 for the qualitative analysis. 9
Results
Of 360 formerly enrolled IBCCP participants from 2015-2017, 69 (weighted 18.5%) obtained health insurance through the Illinois Health Exchange, 179 (weighted 56.7%) obtained Medicaid coverage, 60 (weighted 13.3%) had employer-based health insurance, and 52 (weighted 11.4%) were uninsured. Most women had been IBCCP recipients at local health department lead agencies (n = 237, weighted 71.6%), were aged 50-59 (n = 201, weighted 57.4%), were non-Hispanic white (n = 200, weighted 64.3%), had only a high school education (n = 157, weighted 47.5%), had an annual household income <138% of the federal poverty level (FPL) (n = 254, weighted 74.8%), and spoke English (n = 312, weighted 91.7%). Women who obtained Medicaid coverage were significantly more likely than women who obtained health insurance through the Illinois Health Exchange to have an income <138% FPL (P = .01) (Table 1).
Characteristics of women aged 34-64 who were formerly enrolled in the Illinois Breast and Cervical Cancer Program and participated in the 2015, 2016, and 2017 Women’s Health Survey (N = 360), by current health insurance status, Illinois
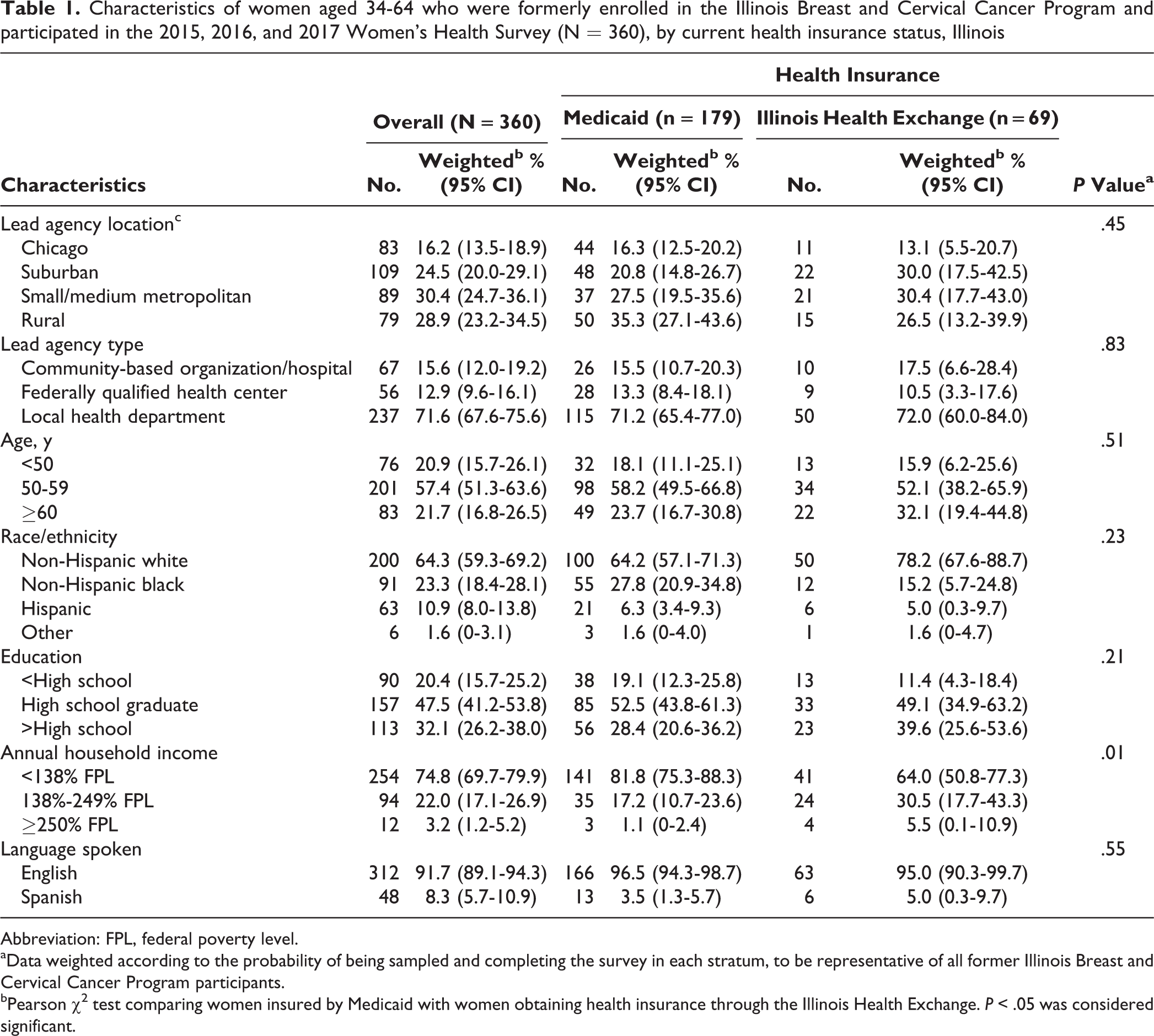
Abbreviation: FPL, federal poverty level.
aData weighted according to the probability of being sampled and completing the survey in each stratum, to be representative of all former Illinois Breast and Cervical Cancer Program participants.
bPearson χ2 test comparing women insured by Medicaid with women obtaining health insurance through the Illinois Health Exchange. P < .05 was considered significant.
We found no significant differences between women insured by Medicaid and women who obtained health insurance through the Illinois Health Exchange in the prevalence of the following outcomes: delaying preventive, chronic, or sick care; timeliness of most recent mammogram; or having a major medical cost in the past 12 months (Table 2). Of 119 women who reported a major medical cost and were currently insured through Medicaid or the Illinois Health Exchange, however, women who obtained health insurance through the Illinois Health Exchange had a higher prevalence than women insured by Medicaid of not having the cost covered (odds ratio [OR] = 4.58; 95% CI, 1.63-12.92). This association remained significant in the fully adjusted model (adjusted odds ratio [aOR] = 4.86; 95% CI, 1.48-16.03) (Table 3).
Past 12-month gaps in coverage among women aged 34-64 who were formerly enrolled in the Illinois Breast and Cervical Cancer Program and participated in the 2015, 2016, and 2017 Women’s Health Survey (N = 360), by current health insurance status, Illinois
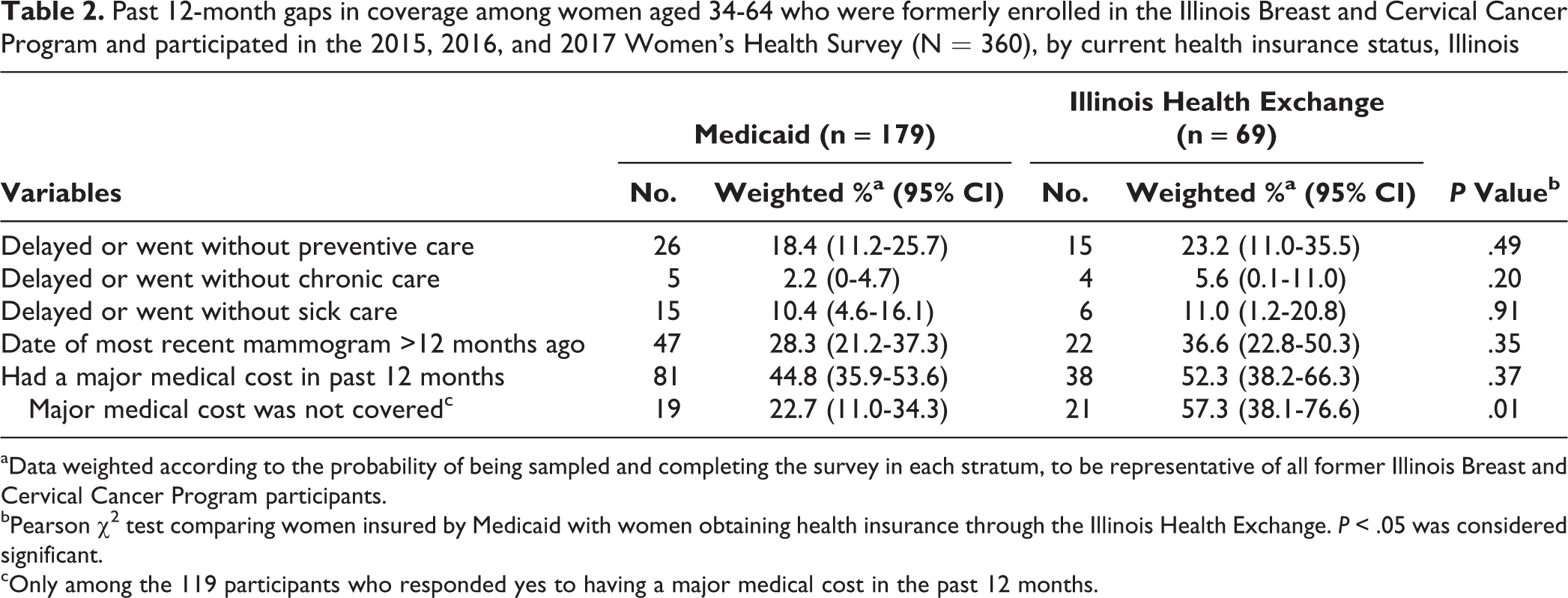
aData weighted according to the probability of being sampled and completing the survey in each stratum, to be representative of all former Illinois Breast and Cervical Cancer Program participants. bPearson χ2 test comparing women insured by Medicaid with women obtaining health insurance through the Illinois Health Exchange. P < .05 was considered significant.
cOnly among the 119 participants who responded yes to having a major medical cost in the past 12 months.
Association between experiences in health care access for women aged 34-64 who were formerly enrolled in the Illinois Breast and Cervical Cancer Program and participated in the 2015, 2016, and 2017 Women’s Health Survey (N = 360), by health insurance coverage through Medicaid or the Illinois Health Exchange, Illinois
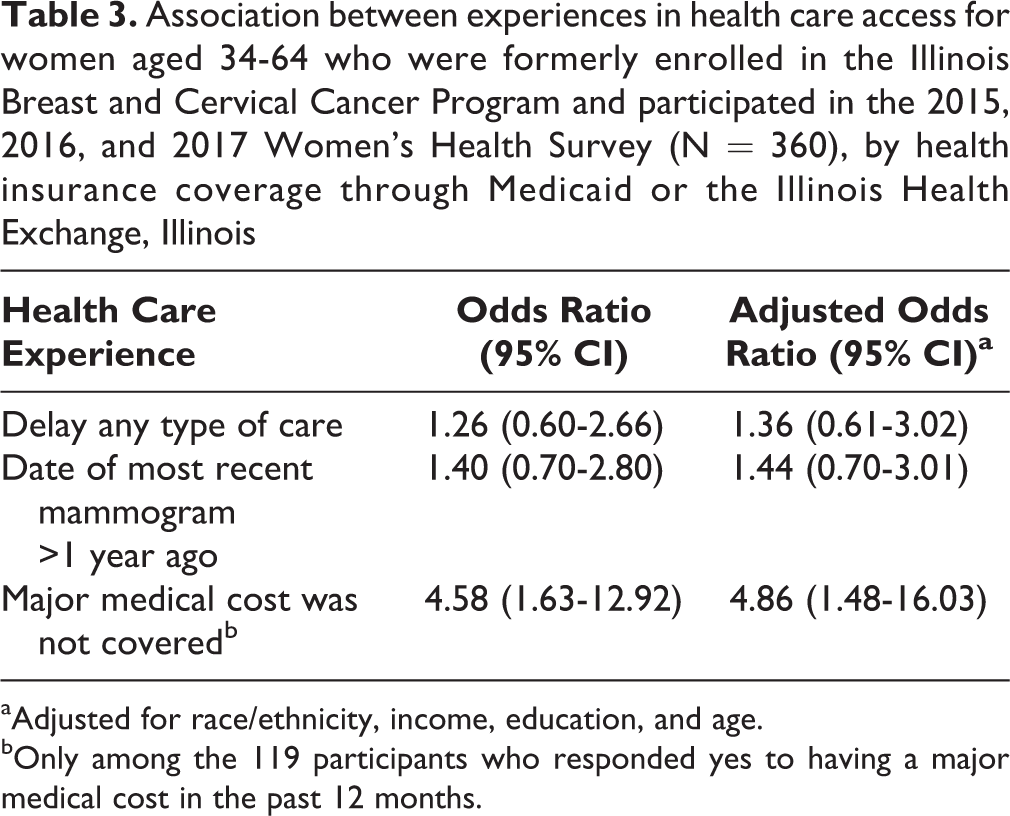
aAdjusted for race/ethnicity, income, education, and age.
bOnly among the 119 participants who responded yes to having a major medical cost in the past 12 months.
Qualitative comments supported the quantitative findings. Although women who obtained health insurance coverage through the Illinois Health Exchange comprised a smaller percentage (18.5%) of women who were formerly enrolled in IBCCP than women insured by Medicaid (56.7%), they had more negative comments about their health insurance. Twenty-five women who obtained health insurance through the Illinois Health Exchange said that their insurance was expensive, 18 women reported confusion in navigating insurance, and 13 reported other issues (eg, inability to find physicians who were covered under their insurance, not knowing which services were covered). Forty-four women pointed to having a negative experience with the Illinois Health Exchange. According to one respondent, “Because I had Obamacare, I did not qualify for the program [IBCCP]. My Obamacare has a high deductible and premiums, though, which I can’t pay. So even though I have insurance, I can’t pay for it. I’m not getting anything good out of having insurance.” Another woman emphasized her lack of consistency in care: “[I] have had a lot of difficulties with the marketplace coverage. When [I] initially switched coverage, [I] confirmed that [the] doctor was in network only to find out, once switched, that the doctor was only in network for the non-marketplace part of the insurance company’s coverage and, therefore, [I] was not able to get care.”
In contrast, only 7 women insured by Medicaid reported having a negative experience (1 said insurance was too expensive, 5 experienced confusion with insurance, and 1 had another issue). One woman said: “Prior to getting on Medicaid, I went years without any services, any testing because I could not afford it. I would say since I have gotten on Medicaid it has been wonderful because I can get things I need done.” Another woman on Medicaid highlighted the importance of receiving help from IBCCP in obtaining coverage: “I was connected to Medicaid through IBCCP and once covered able to get all the services needed.”
Discussion
This study explored the health care experiences of women who previously used a safety-net program, IBCCP, and transitioned to Medicaid or obtained coverage through the Illinois Health Exchange after passage of the Affordable Care Act and identified any gaps in coverage. Findings suggest that compared with women on Medicaid, women who obtained health insurance through the Illinois Health Exchange more frequently reported negative health care experiences, including a lack of affordability and accessibility. These issues were reported in both the quantitative data (ie, not having major medical costs covered) and the qualitative data.
Although women who obtained health insurance through the Illinois Health Exchange have access to Pap tests and screening mammograms without a copay as part of the Essential Health Benefits provided through the Affordable Care Act, access to other nonpreventive services may be more challenging. Differences between the 2 groups in having major medical costs covered may be due to barriers such as high deductibles and copays associated with insurance obtained through the Illinois Health Exchange, which are not barriers for women covered by Medicaid. Studies have found that women with high-deductible plans decreased their use of all types of care, including preventive care, because of not being able to afford any follow-up. 4 Furthermore, high out-of-pocket expenses through high-deductible plans have been shown to be a barrier to efficient breast cancer services. 10
Health insurance premium subsidies are available for some women who obtain coverage through the Illinois Health Exchange, but they are not provided to women with household incomes higher than $47 520 (single woman) or $97 200 (family of 4). As such, some newly insured women may not be able to afford services (beyond Pap tests and screening mammograms) that they had previously received through IBCCP. Although IBCCP offers a high-deductible payment program for diagnostic testing, including mammograms, for women leaving IBCCP and obtaining insurance through the Illinois Health Exchange, many women and providers may not be aware of this program. Increased education is needed to inform women and providers about the high-deductible program and a similar program that provides clinical navigation to breast and cervical cancer services by IBCCP staff members for recently insured women. Both programs are open to all newly insured women, not just previous IBCCP enrollees.
A 2014 report details the extent to which health insurance plans nationwide narrowed provider networks in health exchange plans to balance affordability of the plans. 11 In addition, plans obtained through health exchanges compared with Medicaid have been associated with an increase in out-of-pocket spending, a decrease in affordability, and less continuity of coverage. 12,13 A lack of available and geographically accessible in-network providers and an increase in out-of-pocket costs for women gaining some types of insurance through the Illinois Health Exchange may also be driving the negative health care experiences reported in our study.
Because population incomes of women insured by Medicaid and women who obtained health insurance through the Illinois Health Exchange differ, women newly enrolled in Medicaid might have more difficulty accessing health care than women who obtain insurance through the Health Exchange because of poor health status and access barriers associated with living in poverty. For example, women on Medicaid are at higher risk for chronic conditions associated with their low income level than women with private insurance; however, because Medicaid does not have any deductibles, women on Medicaid appear to have fewer barriers to accessing health care than women who gain coverage through private health insurance plans. 14
Limitations
This study had several limitations. First, data on demographic characteristics may have been outdated, particularly for former IBCCP participants who had not recently used IBCCP, because the IBCCP administrative database may not have had the most up-to-date information. Second, current health insurance status was self-reported and not otherwise verified. Third, although telephone calls were made at all times of the day, every day of the week, and each woman was contacted at least once, nonresponse bias may have affected the findings. Fourth, interviews were conducted in English and Spanish, which may have excluded women who spoke other languages. Finally, these data reflect only the experiences of recently insured women living in Illinois who were previously served by a breast and cervical cancer safety-net program and may not be generalizable to states that did not expand Medicaid as part of Affordable Care Act implementation.
Conclusion
The findings of our study illustrate the experiences of previously uninsured women as they transition to Medicaid and the health exchange. Our findings resonate with the findings of other studies of women’s and families’ frustrations with insurance obtained through health exchanges. 15 Although our data suggest that recently uninsured women with health insurance obtained through the Illinois Health Exchange are more likely than women insured by Medicaid to report not having all major medical costs covered, our study did not directly address the barriers resulting in these negative experiences. Future research is needed to gain a deeper understanding of the barriers women face when transitioning to services provided through their new health insurance coverage.
IBCCP, a safety-net provider, ensures that breast and cervical cancer health needs are met for uninsured and insured women through the high-deductible and clinical navigation components of the program. As a result of the Affordable Care Act, many previously uninsured women can access health insurance coverage either through Medicaid, if their incomes are low enough and they live in a Medicaid expansion state, or through private insurance plans offered through the state or the federal health exchange. However, transitioning from safety-net health programs to health insurance coverage does not guarantee an improvement in women’s health care experiences. Our study provides evidence that for women who were previously uninsured, Medicaid appears to provide more predictable, stable, and comprehensive coverage than health care coverage obtained through the health exchanges. These findings also suggest that safety-net programs such as IBCCP continue to play an essential role in supporting women as they navigate an often complex delivery system. Both phenomena deserve attention as we seek to improve access to care and health outcomes for low-income women and their families.
Footnotes
Acknowledgments
The authors thank the staff members of IBCCP for their help and support.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors declared the following financial support for the research, authorship, and/or publication of this article: the Illinois Department of Public Health, Office of Women’s Health (July 1, 2016–June 30, 2017: FY2017-OWH-002; August 16, 2017–June 30, 2018: 86100009F; July 1, 2018–June 30, 2019: DD-19-96100004G).