
Abstract
Objectives:
Virtual tabletop exercises (VTTXs) simulate disaster scenarios to help participants improve their emergency-planning capacity. The objectives of our study were to (1) evaluate the effectiveness of a VTTX in improving preparedness capabilities specific to children’s needs among pediatricians and public health practitioners, (2) document follow-up actions, and (3) identify exercise strengths and weaknesses.
Methods:
In February 2017, we conducted and evaluated a VTTX facilitated via videoconferencing among 26 pediatricians and public health practitioners from 4 states. Using a mixed-methods design, we assessed participants’ knowledge and confidence to fulfill targeted federal preparedness capabilities immediately before and after the exercise. We also evaluated the degree to which participants made progress on actions through surveys 1 month (n = 14) and 6 months (n = 14) after the exercise.
Results:
Participants reported a greater ability to identify their state’s pediatric emergency preparedness strengths and weaknesses after the exercise (16 of 18) compared with before the exercise (10 of 18). We also observed increases in (1) knowledge of and confidence in performing most pediatric emergency preparedness capabilities and (2) most dimensions of interprofessional collaboration. From 1 month to 6 months after the exercise, participants (n = 14) self-reported making progress in increasing awareness for potential preparedness partners and in conducting similar pediatric exercises (from 4-7 for both).
Conclusions:
Participants viewed the VTTX positively and indicated increased pediatric emergency preparedness knowledge and confidence. Addressing barriers to improving local pediatric emergency preparedness—particularly long term—is an important target for future tabletop exercises.
Keywords
Children aged ≤18 comprise 25% of the US population, yet incorporation of their needs into emergency planning at local, state, and federal levels remains incomplete. 1 -3 Nationally representative data indicate that nearly 1 in 7 US children has experienced a natural or man-made disaster during their lifetime. 4 Recent crises, including the 2010 Haiti earthquake, the 2014 enterovirus D68 outbreak, and 2015 Zika virus outbreak, are reminders of children’s often adverse outcomes in emergencies (eg, disproportionate incidence of infectious disease), rooted in distinct physiological, social, and developmental characteristics that enhance vulnerability.
Partnerships between pediatric health care providers and public health entities are essential for including children in disaster preparedness, management, and recovery planning. 5 -9 Although emergency preparedness exercises have promoted local collaboration and enhanced preparedness capacity, 10 -12 most exercise reports have been prepared for a single state or selected groups of stakeholders. Few describe large-scale, multistate exercises that are relevant to children. 9,13 Emergencies frequently necessitate coordination across sectors and state boundaries 5,9,14,15 ; accordingly, exercises that span multiple jurisdictions and target pediatric considerations of children’s needs in emergencies (eg, family reunification after disasters) are warranted.
A promising approach to promoting awareness and planning in disasters is the use of virtual tabletop exercise (VTTX) models implemented by the Federal Emergency Management Agency (FEMA), which simulate emergency scenarios to help participants generate discussion and identify strategies and gaps in their preparedness, response, and recovery planning. 16 In February 2017, the American Academy of Pediatrics (AAP) and Centers for Disease Control and Prevention (CDC) hosted an exercise that simulated a multistate disease outbreak among children. Because hosting an in-person multistate exercise can be costly and time-consuming, 17 the organizations developed and piloted a VTTX. Adapted from an in-person tabletop exercise, 18 the VTTX aimed to replicate a realistic multijurisdictional response in which state leaders would remain in their own states and communicate electronically. We evaluated the VTTX to understand its effectiveness, follow-up actions taken by state teams, and areas of strength and weakness to inform future exercises.
Methods
Virtual Tabletop Exercise
The CDC/AAP planning team selected participants from FEMA Region VII (Iowa, Kansas, Missouri, and Nebraska) to participate in the VTTX; the AAP and CDC had not previously conducted exercise activities in this region. Each state team included at least 2 pediatricians chosen by the AAP state chapter and 2 local public health officials recommended by CDC-funded Public Health Emergency Preparedness state health department contacts. Participants attended orientation telephone calls to review expectations, although we withheld the exercise content until the exercise itself.
We facilitated the 4-hour exercise from CDC headquarters, and states joined remotely via Zoom software version 3.5. 19 The exercise consisted of 3 modules depicting an outbreak of smallpox (Box). 20 The exercise facilitator tasked teams with addressing 3 objectives that targeted communication and collaboration (Table 1). To meet these objectives, state teams deliberated on plans and procedures and each sector’s response role after they received new information in the scenario (ie, injects) and watched CDC expert videos. AAP Disaster Preparedness Advisory Council members (ie, pediatricians) and public health experts facilitated debriefings among all state teams after the completion of each module.
Description of content of a Centers for Disease Control and Prevention/American Academy of Pediatrics virtual tabletop exercise to enhance pediatric emergency preparedness, Atlanta, Georgia, February 2017a
On February 2, 2017, the American Academy of Pediatrics (AAP) and the Centers for Disease Control and Prevention (CDC) conducted a virtual tabletop exercise with a team from each of 4 states (Iowa, Kansas, Missouri, and Nebraska) committed to enhancing pediatric emergency preparedness through strategic collaboration and discussion. Steven Krug, MD, of the AAP Disaster Preparedness Advisory Council (DPAC) moderated the opening session and welcomed the state team participants and observers to the exercise. He introduced Georgina Peacock, MD, MPH, division director of CDC’s Division of Human Development and Disability, who provided opening remarks. Dr Peacock acknowledged the longstanding partnership between AAP and CDC’s Children’s Preparedness Unit (CPU) through pediatric emergency preparedness and response and shared the exercise background as an adaptation of a previous in-person exercise in 2016.
An exercise “hotwash,” or after-action discussion, was conducted immediately after the final module and offered an opportunity for participants to reflect on the exercise objectives and discussions and report on what went well, what was learned, and areas for improvement in future exercises. Dr Peacock then closed by thanking state teams and the several groups and individuals who played an instrumental role in successfully executing the exercise.
aA tabletop exercise is an activity that simulates a real-life disaster scenario to promote discussion for agencies and professionals involved in emergency preparedness. Virtual tabletop exercises convene participants over videoconference technology.
Objectives and affiliated measures designated by the planning team for the Centers for Disease Control and Prevention/American Academy of Pediatrics virtual tabletop exercise to enhance pediatric emergency preparedness, Atlanta, Georgia, February 2017a
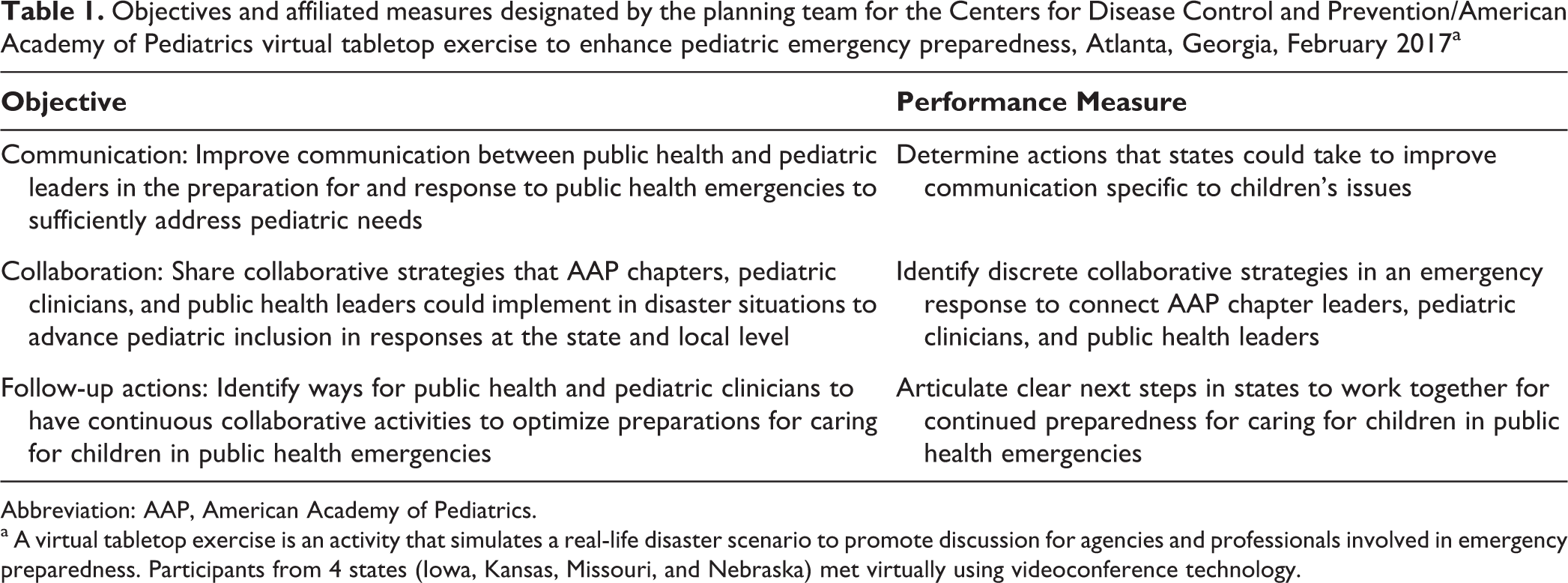
Abbreviation: AAP, American Academy of Pediatrics.
a A virtual tabletop exercise is an activity that simulates a real-life disaster scenario to promote discussion for agencies and professionals involved in emergency preparedness. Participants from 4 states (Iowa, Kansas, Missouri, and Nebraska) met virtually using videoconference technology.
Evaluation Approach
Following exercise evaluation best practices,
21
we applied a mixed-methods design informed by the Kirkpatrick Training Evaluation Model
22
and US Department of Homeland Security Exercise Evaluation Program.
23
The planning team, which comprised public health experts, Disaster Preparedness Advisory Council members, and state representatives, iteratively convened to develop evaluation questions: Exercise effectiveness: To what extent and how does participating in the VTTX result in improved pediatric preparedness capabilities at the state or local level? Follow-up actions: To what extent and in what ways do participants engage in actions that support improved planning as a result of participating in the VTTX? Strengths and weaknesses: What aspects of the VTTX structure, process, and/or logistics helped or hindered meeting VTTX objectives?
To optimize the evaluation’s utility, accuracy, and feasibility, 24 the planning team vetted the overarching evaluation questions, pilot-tested surveys for clarity and relevance, and member-checked summary reports to facilitate interpretation.
Data Sources and Data Collection
To document how we would evaluate the exercise, we developed an evaluation methods grid 24 aligning evaluation questions with methods, data sources, evaluators, and analyses (available upon request). To operationalize pediatric emergency preparedness, we considered participants’ (1) self-rated knowledge and confidence to fulfill key preparedness capabilities (Likert scale response), (2) perceptions of state strengths and weaknesses in pediatric emergency preparedness (Likert scale response), (3) collaboration and communication strategies suggested after participation (open-ended response), (4) intended changes after participation (open-ended response), (5) perceived degree of collaboration between sectors (Likert scale response), (6) perceptions of the exercise’s most and least beneficial aspects (open-ended response), and (7) set of questions probing participants about the extent to which stated exercise objectives were met (Likert scale response). We developed a survey covering these topics and administered the survey at 2 points: 24 hours before the VTTX and 24 hours after the VTTX.
For the survey section on self-rated knowledge and confidence to fulfill key preparedness capabilities, we developed a list of 12 capabilities. Because no consensus guidelines on pediatric emergency preparedness planning exist, the planning team reviewed US Department of Homeland Security 23 and CDC 25 standards and rank-ordered 12 capabilities that were most applicable to children’s needs and reflected the spectrum of disaster preparedness and response (Box). Survey response options were given on a 10-point Likert scale, where 1 = least knowledgeable or confident and 10 = most knowledgeable or confident.
For the Likert scale question on perceptions of state strengths and weaknesses in pediatric emergency preparedness, we asked participants to respond to the following statement: “I am able to identify my jurisdictions’ own strengths and weaknesses when it comes to pediatric preparedness planning” (1 = strongly disagree, 5 = strongly agree). For the open-ended question on collaboration and communication strategies suggested after participation, we requested, “Please state additional communication or collaboration strategies you would suggest that public health and pediatric staff could consider for improving pediatric preparedness at the state level.” For the open-ended question on intended changes after participation, we requested, “Please share what specific actions you are considering taking, especially regarding communication and collaboration.”
To assess intersectoral collaboration, we used the Strategic Alliance Formative Assessment Rubric (SAFAR), 26 a validated assessment tool for evaluating collaborative goals and strategies across sectors. Participants rated themselves on 4 dimensions: (1) goals and purpose; (2) activities, strategies, and tasks; (3) decision making and leadership; and (4) interagency communication and information sharing. The SAFAR uses a 6-point Likert scale, where 0 = least integrated and 5 = most integrated.
We evaluated (1) responses to the surveys, (2) observation forms completed by independent evaluators, (3) notes from the postexercise participant debriefing (ie, hotwash) about strengths and weaknesses of the exercise, (4) notes from an after-action review of planning committee members to debrief about the exercise, and (5) follow-up surveys collected 1 month and 6 months after the exercise (details available on request). We administered all surveys via SurveyMonkey. Response-rate optimization strategies 27 included tailored emails from professional peers, follow-up telephone calls to nonrespondents, and certificates of appreciation. Evaluators collected observation-based data activity without attributing data to individuals to limit observer effects. We enhanced our evaluation’s trustworthiness by soliciting feedback on result summaries from planning team members (ie, member checking 28 ), maintaining an audit trail outlining analytic decisions, and using multiple analysts. 29
Data Analysis
We used Stata version 14.1 30 to calculate descriptive statistics and 2-tailed nonparametric Wilcoxon signed-rank tests to compare median scores across time points. We handled missing data by using available-case analysis.
We qualitatively analyzed raw, open-ended, discussion-based, and observational data collectively by using the framework method. 28 In the framework method, 3 investigators (M.S., J.L.F., K.C.-O.) developed a priori codes based on evaluation objectives, read through the data to assign initial codes, iteratively modified the code list until they attained a complete understanding of possible codes, and recorded reflective notes 28 throughout. We resolved coding discrepancies via discussion until consensus was achieved. Finally, we clustered codes into categories to identify recurrent themes, and we assessed both basic frequencies and the degree to which a theme emerged across multiple sources to understand which themes were most prominent.
Four state teams, including 10 pediatricians and 16 state public health representatives, participated in the VTTX. The planning team was aware of only 18 participants before the exercise; thus, the 8 participants who joined the exercise ad hoc were included only in the 1- and 6-month follow-up surveys. The AAP Institutional Review Board determined that the evaluation was not subject to human subjects review.
Results
Effectiveness of the VTTX
In the postexercise survey, 13 of 18 participants reported that they determined actions to improve communication in their state; 8 participants agreed that collaborative strategies were determined, and 10 participants agreed that next steps for children’s preparedness were determined. Most participants perceived that the exercise generated productive discussion (n = 16) and that they could apply the knowledge gained from this exercise to their routine work (n = 15). The number of participants who were able to identify their state’s pediatric emergency preparedness strengths and weaknesses rose from 10 of 18 before the VTTX to 16 of 18 after the VTTX (W = 27, P = .01).
Knowledge and confidence to perform capabilities
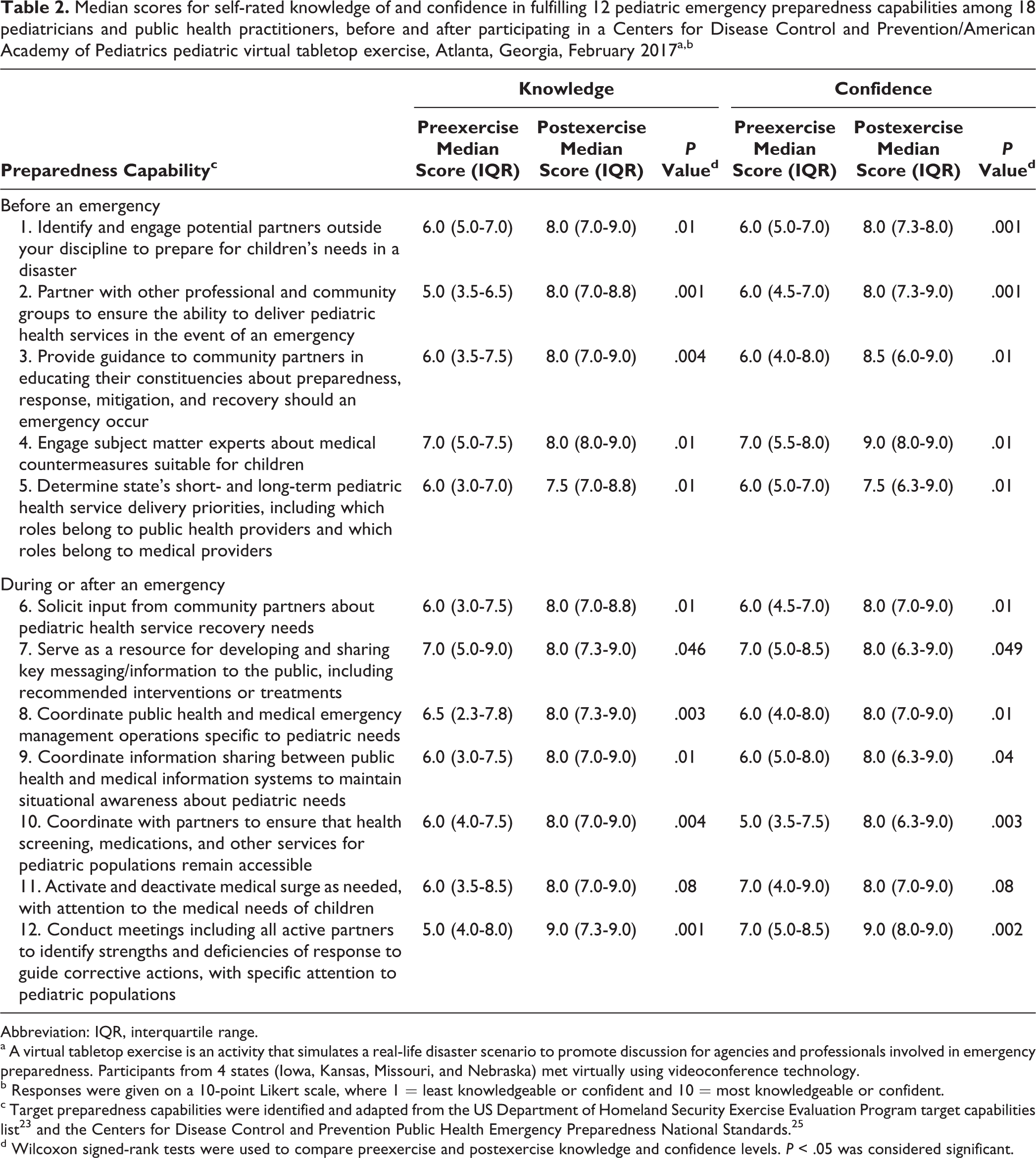
Average participant scores in 12 pediatric emergency preparedness capabilities improved after the VTTX, 11 of which represented significant changes for both knowledge and confidence (Table 2). The knowledge (W = 33, P = .08) and confidence (W = 34, P = .08) increases for the medical surge activation/deactivation capability were not significant.
Median scores for self-rated knowledge of and confidence in fulfilling 12 pediatric emergency preparedness capabilities among 18 pediatricians and public health practitioners, before and after participating in a Centers for Disease Control and Prevention/American Academy of Pediatrics pediatric virtual tabletop exercise, Atlanta, Georgia, February 2017a,b
Abbreviation: IQR, interquartile range.
a A virtual tabletop exercise is an activity that simulates a real-life disaster scenario to promote discussion for agencies and professionals involved in emergency preparedness. Participants from 4 states (Iowa, Kansas, Missouri, and Nebraska) met virtually using videoconference technology.
b Responses were given on a 10-point Likert scale, where 1 = least knowledgeable or confident and 10 = most knowledgeable or confident.
c Target preparedness capabilities were identified and adapted from the US Department of Homeland Security Exercise Evaluation Program target capabilities list 23 and the Centers for Disease Control and Prevention Public Health Emergency Preparedness National Standards. 25
d Wilcoxon signed-rank tests were used to compare preexercise and postexercise knowledge and confidence levels. P < .05 was considered significant.
Collaboration between pediatrics and public health
Participant self-ratings on the SAFAR dimensions increased significantly in 3 of 4 SAFAR domains from preexercise to postexercise: (1) activities, strategies, and tasks (W = 56, P = .001), (2) decision making (W = 47, P = .004), and (3) interagency communication and information sharing (W = 49, P = .004; Figure). These collaboration ratings were not different across the disciplines (supplemental analyses not shown).
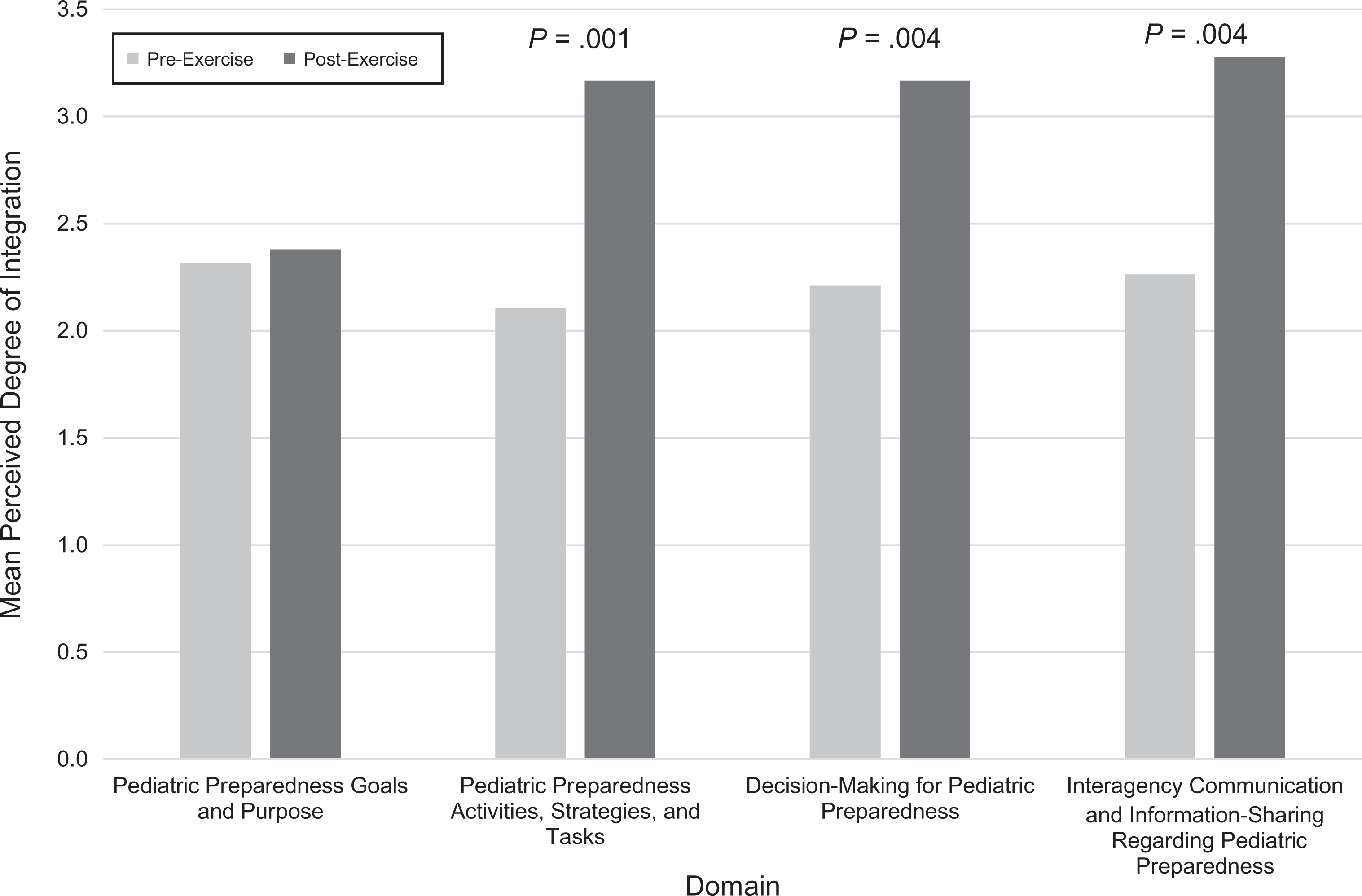
Mean self-ratings for each domain of the Strategic Alliance Formative Assessment Rubric (SAFAR) among pediatricians and public health practitioners (n = 18) in a virtual tabletop exercise on improving pediatric emergency preparedness, Atlanta, Georgia, February 2017. A virtual tabletop exercise is an activity that simulates a real-life disaster scenario to promote discussion for agencies and professionals involved in emergency preparedness. Participants from 4 states (Iowa, Kansas, Missouri, and Nebraska) met virtually using videoconference technology. The preexercise survey was conducted 24 hours before the exercise and the postexercise survey 24 hours after the exercise. Both surveys were administered via SurveyMonkey. SAFAR is a validated assessment tool for evaluating collaborative goals and strategies across sectors. 26 It is evaluated on a 6-point Likert scale, where 0 = least integrated and 5 = most integrated. Respondents were asked the following question: “Consider how integrated your state is across pediatric and public health sectors for pediatric preparedness. Integration refers to how well these 2 sectors align and collaborate to optimally prepare your state for a potential disaster. On a scale of 0-5, with 0 being not integrated at all and 5 being completely integrated, please rate how much you think your state is integrated across pediatric and public health sectors, specifically regarding [domains 1-4 in the figure].”
Qualitative responses
The main theme underlying participants’ comments on the VTTX’s influence on perceptions of their jurisdiction’s pediatric emergency preparedness knowledge, collaboration, and communication was the benefit of establishing connections between the 2 sectors. One participant wrote, “The connections just from the exercise are already looking to be invaluable moving forward.” Many participants also noted that each group had “the same interest in safeguarding kids.”
Furthermore, several participants noted an increase in knowledge of content areas as the result of conversations during the exercise, including health communication topics (eg, state secure email systems for infectious disease, tailored messaging to vulnerable populations, communication with bordering states), the roles and responsibilities of the other sector’s staff members in emergency preparedness, and state public health law. Some participants recognized their limited personal knowledge of available state resources and existing preparedness plans. One participant explained, “[The] discussion generated made me realize how much I did not know.”
Observation-based data revealed an exchange of information between sectors. Public health staff members queried pediatric providers about the best way to communicate with physicians (eg, Health Alert Network), hospital surge capacity for highly infectious patients in quarantine situations, and hospital surge capacity criteria. Questions from pediatricians to public health personnel concerned the state’s emergency response infrastructure, the state laboratory’s role in confirming disease outbreaks, and communications with bordering states and vulnerable populations.
Follow-up Actions
Intended actions
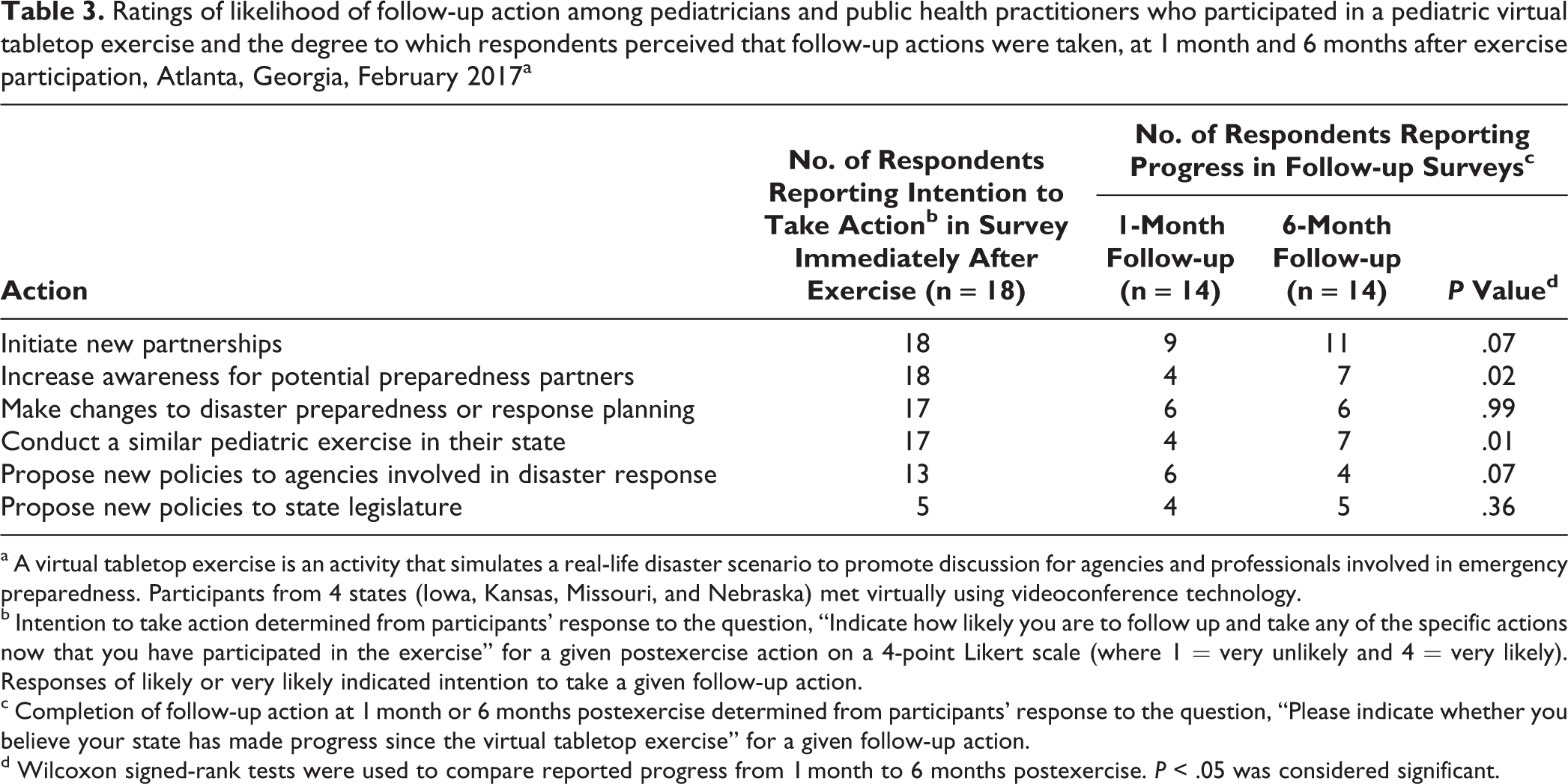
Immediately after the exercise, all respondents indicated they would be likely or very likely to initiate new partnerships and increase awareness for potential preparedness partners (Table 3). Seventeen participants indicated they would be likely to make changes to pediatric emergency preparedness planning and conduct a similar pediatric exercise in their state. Conversely, participants indicated it was not likely that they would engage in efforts to effect policy changes (to agencies involved in disaster response and to state legislature) to the same extent.
Ratings of likelihood of follow-up action among pediatricians and public health practitioners who participated in a pediatric virtual tabletop exercise and the degree to which respondents perceived that follow-up actions were taken, at 1 month and 6 months after exercise participation, Atlanta, Georgia, February 2017a
a A virtual tabletop exercise is an activity that simulates a real-life disaster scenario to promote discussion for agencies and professionals involved in emergency preparedness. Participants from 4 states (Iowa, Kansas, Missouri, and Nebraska) met virtually using videoconference technology.
b Intention to take action determined from participants’ response to the question, “Indicate how likely you are to follow up and take any of the specific actions now that you have participated in the exercise” for a given postexercise action on a 4-point Likert scale (where 1 = very unlikely and 4 = very likely). Responses of likely or very likely indicated intention to take a given follow-up action.
c Completion of follow-up action at 1 month or 6 months postexercise determined from participants’ response to the question, “Please indicate whether you believe your state has made progress since the virtual tabletop exercise” for a given follow-up action.
d Wilcoxon signed-rank tests were used to compare reported progress from 1 month to 6 months postexercise. P < .05 was considered significant.
Responses to open-ended survey questions and the debriefing elaborated on their ratings. Consistently reported intended actions included organizing similar drills, planning educational programs (eg, grand rounds), and establishing communication between the health department and state AAP chapter. Unique intended actions included reaching out to pediatricians to increase awareness, including a broader range of stakeholders (eg, family physicians), and better integrating pediatricians into local preparedness planning processes.
Completed actions
Of the 14 participants who completed both the 1- and 6-month follow-up surveys, participants at 1 month postexercise indicated making progress in initiating new partnerships (n = 9), making changes in disaster preparedness or response planning (n = 6), proposing new policies to agencies involved in disaster response (n = 6), increasing awareness for potential preparedness partners (n = 4), and conducting a similar pediatric exercise in their state (n = 4). At 6 months postexercise, respondents reported significant progress in increasing awareness for potential preparedness partners (W = 15, P = .01) and conducting similar pediatric exercises in their state (W = 15, P = .01). We did not observe significant changes for other actions from 1 month to 6 months after the exercise (Table 3).
Participants described actions they had pursued by 1 month postexercise that would not have occurred without VTTX participation, including developing connections to conduct a pediatric-centric exercise, broadly enhancing statewide awareness of pediatric emergency preparedness activities to stakeholders, and developing new pediatric policies and pediatric information for existing in-state exercises. At 6 months postexercise, participants described actions to incorporate pediatric considerations (eg, family reunification) into state preparedness plans and implement exercises focusing on pediatric needs. Several public health agency respondents reported improvements in their health department’s relationship with private practice pediatricians, the local AAP chapter, and diverse community partners (eg, Emergency Medical Services for Children).
Exercise Strengths and Weaknesses
Most participants reacted positively to how the VTTX was operated, agreed that their overall experience was positive, and indicated that the pre-VTTX materials helped them understand expectations. Of the 23 participants, 20 reported that the web-based platform ran smoothly, and 19 described the exercise length as appropriate; others suggested the length be reduced. Observers documented attentiveness and engagement during the VTTX, as well as during breaks, and indicated that the communications software enabled continuous communication among participants and administrators.
Participants identified 2 primary benefits of the exercise: (1) meeting and developing relationships with partners in public health and pediatrics and (2) understanding each other’s role in pediatric emergency preparedness. More than half of participants said that the VTTX needed to be improved by adding components that leverage pediatric expertise (ie, the VTTX “was not very pediatric”); the lack of such components made it “difficult for public health partners to determine how AAP could be engaged.” To remedy this issue, several respondents offered concrete examples of content to incorporate into future scenarios: family reunification, preventing disease spread in family networks, preparing childcare settings, pediatric surge capacity, response considerations specific to developmental status (eg, infant patients), and leveraging social media for risk communication. Other areas for improvement suggested by some participants were involving other professionals (eg, education, public information officers) and improving the usefulness of scenario endings and the live teleconferencing call to AAP leadership.
In both follow-up surveys, participants noted barriers to stimulating change in pediatric emergency preparedness at the local level (4 of 23 in the 1-month survey and 4 of 14 in the 6-month survey), including lack of staff member time and financial resources to engage state partners. Furthermore, in the 6-month survey, 2 participants noted that children’s preparedness was not a health department priority (as it is for hospitals); others reported that some VTTX participants had since left the department.
Lessons Learned
The VTTX helped participants clarify roles and responsibilities, facilitate knowledge transfer between sectors, and identify systems-level challenges. These benefits align with evaluations of in-person tabletop exercises, 11,12 including exercises targeting children’s needs. 31,32 However, barriers including resource constraints, staff turnover, and inconsistent planning priorities were noted, consistent with previous studies. 8 Our findings expand upon limitations of extant research 10 -12 by identifying the degree to which improvements persist and translate to concrete local preparedness actions 6 months later. That participants demonstrated a largely positive, engaged experience as well as clear improvements in knowledge and confidence—even with the virtual format—attests to the VTTX model’s viability.
Interprofessional partnership remains a key knowledge gap 9 for, and essential component of, preparedness planning for vulnerable populations. 8,14,33 Thus, the inclusion of a validated measure of collaboration that has not previously been demonstrated for pediatric tabletop exercises is notable. The changes documented reflect validated instruments where available (eg, SAFAR) as well as national standards informed by both evidence and legislative directives and applied to the pediatric population in accordance with practitioner expertise. 34
Our mixed-method study design enabled us to understand both the degree and content of enacted changes. This robust approach enhances the likelihood that these indicators reflect the capability of states in an actual emergency. Our approach departs from most research on disaster preparedness “lessons learned,” which has historically neglected strategies for measure selection and study design that could augment internal and external validity. 9,10,35
Limitations and Future Directions
This study had several limitations. First, our sampling approach limited the generalizability of our findings to other sectors that might be involved in an emergency response. However, gathering a selected group of professionals reflects both what an actual outbreak response would involve and how most tabletop exercises are conducted. 11 Second, we drew qualitative data from open-ended sources, presenting difficulty in understanding respondents’ true intent. This risk was somewhat tempered through measures such as member checking and methodological triangulation. 29 Third, because several planning team members were involved in funding decisions for participants’ organizations, social desirability bias was a concern. Fourth, we were unable to include persons who provided data at 1 month postexercise but not 6 months postexercise, which limited the power of our analysis.
Ultimately, a continuous quality improvement approach is essential in emergency preparedness planning. 6 More rigorous investigations using larger and more professionally diverse samples, and prospective linkages with performance measures after actual emergencies, would further our progress toward understanding and improving the VTTX’s effectiveness. Additional evaluations of VTTXs and other emerging strategies (eg, virtual simulation models 17 ) are particularly needed as children’s preparedness gains increasing attention 18,36 and could identify which approaches merit broad dissemination. 3
Finally, although exercise-planning conventions dictate that exercises be evaluated according to standardized core capabilities, 23,34 none specific to children’s needs exist, limiting the comparability of existing studies. 33 Efforts to validate guidelines using expert consultation or operationalize existing resources (eg, Save the Children Report Card 2 ) into target capabilities could help similar initiatives more objectively measure their impact.
Implications for Practice
When designing future pediatric tabletop exercises, emergency preparedness planners could include content that better leverages pediatric expertise, targets skills important for influencing state or local policy environments, focuses on medical surge activation/deactivation, or intentionally facilitates the 2 sectors in aligning goals. They might also consider ongoing technical assistance after exercise administration, because respondents reported progress in only 2 of 6 actions assessed from 1 month to 6 months postexercise, indicating that barriers to long-term change in pediatric preparedness persist.
Health departments can implement mechanisms (eg, quality improvement teams) to facilitate collaborative planning and policy development for pediatric emergency preparedness, given staff member time and funding as documented barriers to change. Health departments can also examine topics discussed by the 2 sectors to guide tailored communication and outreach to clinicians. Finally, pediatric providers and regional coalitions can consider how to incorporate VTTXs to build preparedness capacity while facilitating relationship building between public health and physicians.
A central concept reported by participants was the need for substantive inclusion of children’s unique medical and developmental characteristics in the VTTX beyond simply placing them in the scenario. Knowledge about children’s vulnerabilities is well-documented by academics, 6,36,37 government agencies, 1,38 and authoritative organizations safeguarding children. 2,5 In combination with suggestions proposed herein, this literature can inform future exercise content.
Conclusions
Tabletop exercises have limited reach because they often require in-person participation or fail to consider at-risk populations. We determined that a half-day pediatric VTTX was feasible and effective in promoting pediatric emergency preparedness capabilities and interprofessional collaboration. With proper attention to potential dissemination and sustainment barriers, such an exercise could enhance local preparedness capacity and protect more of the nation’s children during crises.
Footnotes
Acknowledgments
The authors thank the pediatric virtual tabletop exercise participants; Laura Aird, Kate Klein, Sean Diederich, and Breanna Smith (American Academy of Pediatrics); Rebecca Leeb, Frank Long, Scott Wilson, Brett Petersen, Susan Gorman, and Dan Sosin (Centers for Disease Control and Prevention); and the pediatric virtual tabletop exercise Planning Committee (list of members available at: ![]() ).
).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This publication was supported by cooperative agreement #5NU38OT000167-04, funded by CDC. Its contents are solely the responsibility of the authors and do not necessarily represent the official views of CDC or the US Department of Health and Human Services.