
Abstract
Objectives:
Despite cancer prevention benefits associated with the human papillomavirus (HPV) vaccine, uptake in the United States is relatively low among males and females. Our objective was to use the Healthy People 2020 social determinants of health framework to determine the availability and characteristics of data on economic, educational, social, health care, and community factors affecting HPV vaccine uptake in the United States.
Methods:
We included the most recent data sets from 6 publicly available, US-based, federally funded surveys that contained at least 1 measure of HPV vaccination among adolescents and young adults. We searched each data set for any social determinants of health measures within the 5 domains of the framework: economic stability, education, social and community context, health and health care, and neighborhood and built environment.
Results:
The social determinants of health domains of education, economic stability, and health and health care appeared in all data sets. The domains of social and community context and neighborhood and built environment appeared in only 3 data sets. Even when domains were represented, we discovered gaps in the data sets, in which only limited measures of the social determinants were available.
Conclusion:
The addition of questions about the social determinants of health to the surveys that generate these data sets, particularly in the domains of social and community context and neighborhood and built environment, would strengthen the ability of public health researchers, policy makers, and professionals to identify associations between the social determinants of health and HPV vaccine uptake.
Human papillomavirus (HPV) is the most common sexually transmitted infection in the United States and a causal agent for genital warts and cervical, anal, vaginal, vulvar, penile, and oropharyngeal cancers. 1,2 Primary prevention for HPV-related genital warts and cancers is available through a safe and effective vaccine. A 2-shot series is usually recommended for adolescents aged 11 or 12. For those who do not start the series of shots as adolescents, vaccination is still recommended up to age 26 (a “catch-up” vaccination, which involves 3 shots). 2 In 2006, the Advisory Committee on Immunization Practices recommended routine vaccination for girls aged 11 or 12. In 2011, the recommendation for routine HPV vaccination expanded to boys aged 11 or 12. 3
Despite these recommendations and the prevention benefits associated with the HPV vaccine, uptake in the United States is relatively low among males and females. 2,4 As of 2017, 68.6% of adolescent females and 62.6% of adolescent males aged 13-17 had received at least 1 HPV vaccine dose, and 48.6% of adolescents aged 13-17 had completed the recommended 2-shot series. 4 In comparison, Scotland, which has a successful school-based HPV immunization program, reported 2017 vaccination rates >90%. 5 The most recent HPV vaccination rates in the United States may have been even lower if not for the passage of the Patient Protection and Affordable Care Act in 2010. With implementation of the Affordable Care Act, more adolescents were covered by insurance and had access to preventive health care, and insurance carriers were required to cover HPV vaccination. Although the Affordable Care Act may have positively influenced HPV vaccine uptake, there is room for improvement. 6
One approach to increasing HPV vaccine uptake in the United States is to assess the social determinants of health that may influence uptake of the HPV vaccine. 5 Data on HPV vaccination from multiple large US surveys can be used to assess sociodemographic factors that influence uptake. Although they are not designed to measure the social determinants of health, these surveys often include questions about sociodemographic factors, and some of the responses may also serve as proxies for the social determinants of health. The social determinants of HPV vaccine uptake have been assessed in various countries (eg, England, Madagascar), but each country has its own unique policies, cultures, and social norms that make it important to study social determinants of health within those country-dependent contexts. 7 -9 In the United States, it is unclear in the literature whether the databases resulting from national surveys sufficiently measure the social determinants of health that might influence HPV vaccine uptake. Thus, more deeply examining these social determinants of health in US databases could provide information about the sociodemographic factors related to HPV vaccine uptake that might enable structural-level, barrier-reducing policy interventions and, potentially, improvements in HPV vaccination rates.
The social-ecological model of health promotion posits that factors influencing health exist at multiple levels, including the individual, interpersonal, community, and societal levels. 10 According to this model, interpersonal factors are close relationships (peers, partners, and family members) that may influence health, community factors are relationships among organizations and networks, and societal factors are the social and cultural norms, as well as the health, economic, educational, and social policies, that may play a role in health and prevention of disease. 10 Although sociodemographic factors influencing HPV vaccine uptake in the United States have been examined extensively at the individual and interpersonal levels (by examining attitudes, beliefs, knowledge, and communication), 11 -15 these factors have been investigated to a lesser degree at the community and societal levels. 16 -18
The influence of community- and societal-level factors on HPV vaccine uptake might be more thoroughly investigated by using a social determinants of health framework. The integration of a social determinants of health framework into public health research has become a national priority. Healthy People 2020 has a formal social determinants of health framework to help set national objectives for improving the health of all Americans. 19 Rather than focusing on the individual and interpersonal factors that influence health (eg, individual knowledge, beliefs, and attitudes or interactions among persons), this comprehensive framework concentrates on the broad range of economic, educational, social, health care, and community factors affecting health. Despite the availability of this comprehensive framework, little public health research has been conducted by using this framework or one similar to it. 20
The primary objective of our study was to use the Healthy People 2020 social determinants of health framework to determine the availability and characteristics of data on economic, educational, social, health care, and community factors that affect HPV vaccine uptake in publicly available, US-based, federally funded databases. A secondary objective was to identify and enumerate any gaps in data so that researchers working on the databases and other researchers could use this information to strengthen the data on sociodemographic factors that are available in the future, particularly for use in determining public health policies and practices related to HPV vaccination.
Methods
To identify data sets for inclusion in our study, we examined websites of the Centers for Disease Control and Prevention, the National Center for Health Statistics (NCHS), and the Inter-university Consortium for Political and Social Research. For the purposes of this study, we chose data sets from publicly available, US-based, federally funded surveys that contained at least 1 measure of HPV vaccination among adolescents and young adults. We included data sets regardless of whether both sexes and all ages were represented.
Once we identified the data sets to include, a single co-author (S.B.M.) extracted and reviewed the public data dictionaries (ie, online files that allow users to view the survey questions) for each data set. Then, to search each data set for social determinants of health variables, we used the definitions for the Healthy People 2020 social determinants of health framework. 19 This framework consists of 5 domains, each of which has 3 or 4 key areas (Table 1). The domain (and key area) variables that we searched for in the databases were as follows: economic stability (poverty, employment, food security, housing stability), education (high school graduation, enrollment in higher education, language and literacy, early childhood education and development), social and community context (social cohesion, discrimination, civic participation, incarceration), health and health care (access to health care, access to primary care, health literacy), and neighborhood and built environment (access to healthy foods, crime and violence, environmental conditions, quality of housing).
Domains and key areas of the Healthy People 2020 social determinants of health framework,a identified in 6 publicly available, US-based, federally funded data sets from surveys that ask about human papillomavirus (HPV) vaccination, 2007-2016b
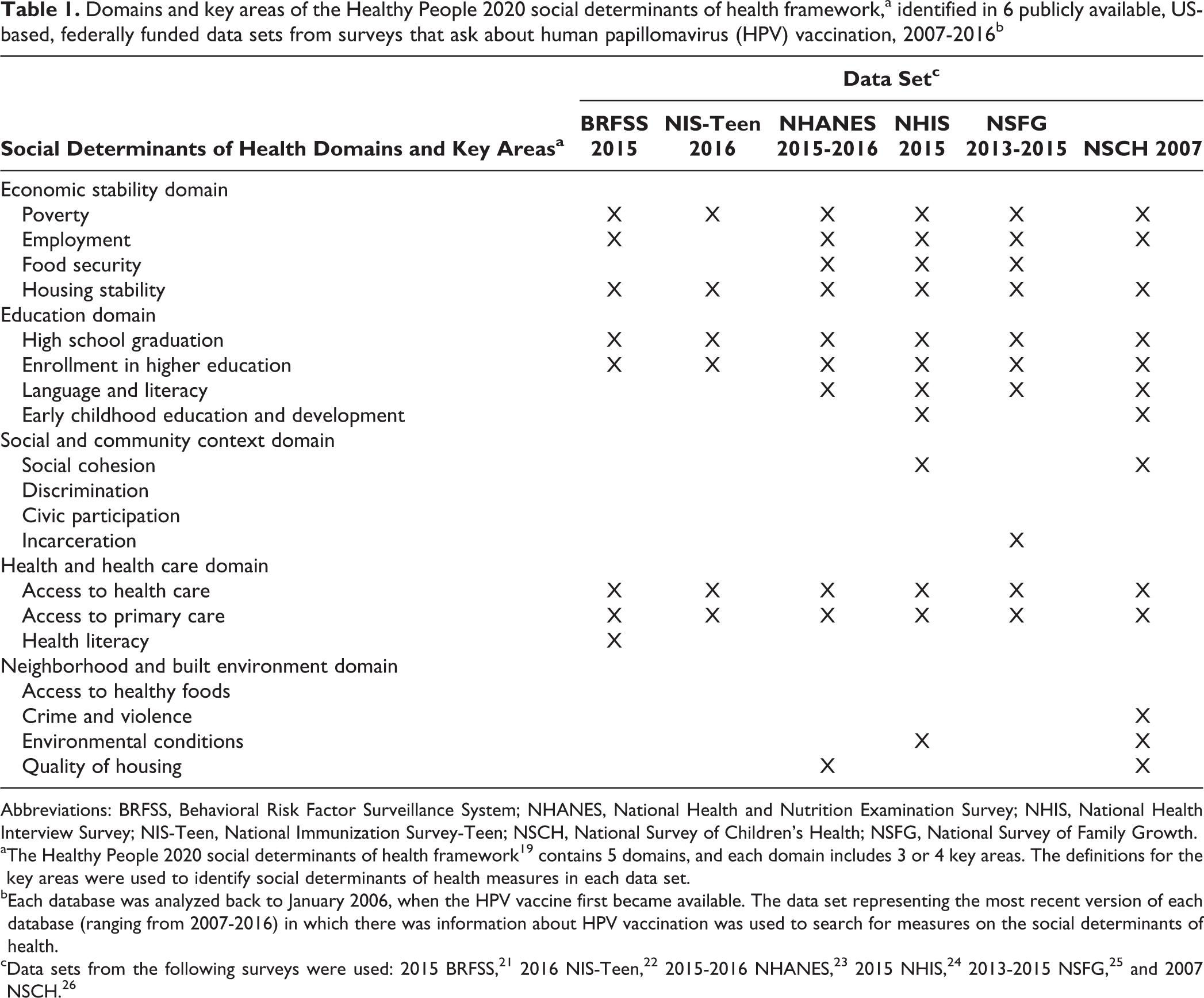
Abbreviations: BRFSS, Behavioral Risk Factor Surveillance System; NHANES, National Health and Nutrition Examination Survey; NHIS, National Health Interview Survey; NIS-Teen, National Immunization Survey-Teen; NSCH, National Survey of Children’s Health; NSFG, National Survey of Family Growth.
aThe Healthy People 2020 social determinants of health framework 19 contains 5 domains, and each domain includes 3 or 4 key areas. The definitions for the key areas were used to identify social determinants of health measures in each data set.
bEach database was analyzed back to January 2006, when the HPV vaccine first became available. The data set representing the most recent version of each database (ranging from 2007-2016) in which there was information about HPV vaccination was used to search for measures on the social determinants of health.
Within each data set, we reviewed surveys as far back as January 2006, when the HPV vaccine first became available. However, for this study, we used only the most recent version of each data set that contained information about HPV vaccination. Because we used the most recent versions of data sets and because some of the data sets stopped including information about HPV vaccination (eg, the National Survey of Children’s Health [NSCH] after 2007), we analyzed data sets from 2007-2016.
The 6 data sets that we included in our study were the 2015 Behavioral Risk Factor Surveillance System (BRFSS), 21 2016 National Immunization Survey–Teen (NIS-Teen), 22 the 2015-2016 National Health and Nutrition Examination Survey (NHANES), 23 the 2015 National Health Interview Survey (NHIS), 24 the 2013-2015 National Survey of Family Growth (NSFG), 25 and the 2007 NSCH 26 (Table 2).
Descriptions of data sets from 6 publicly available, US-based, federally funded databases that contain human papillomavirus (HPV) vaccination information and were used to search for social determinants of health factors, 2007-2016a
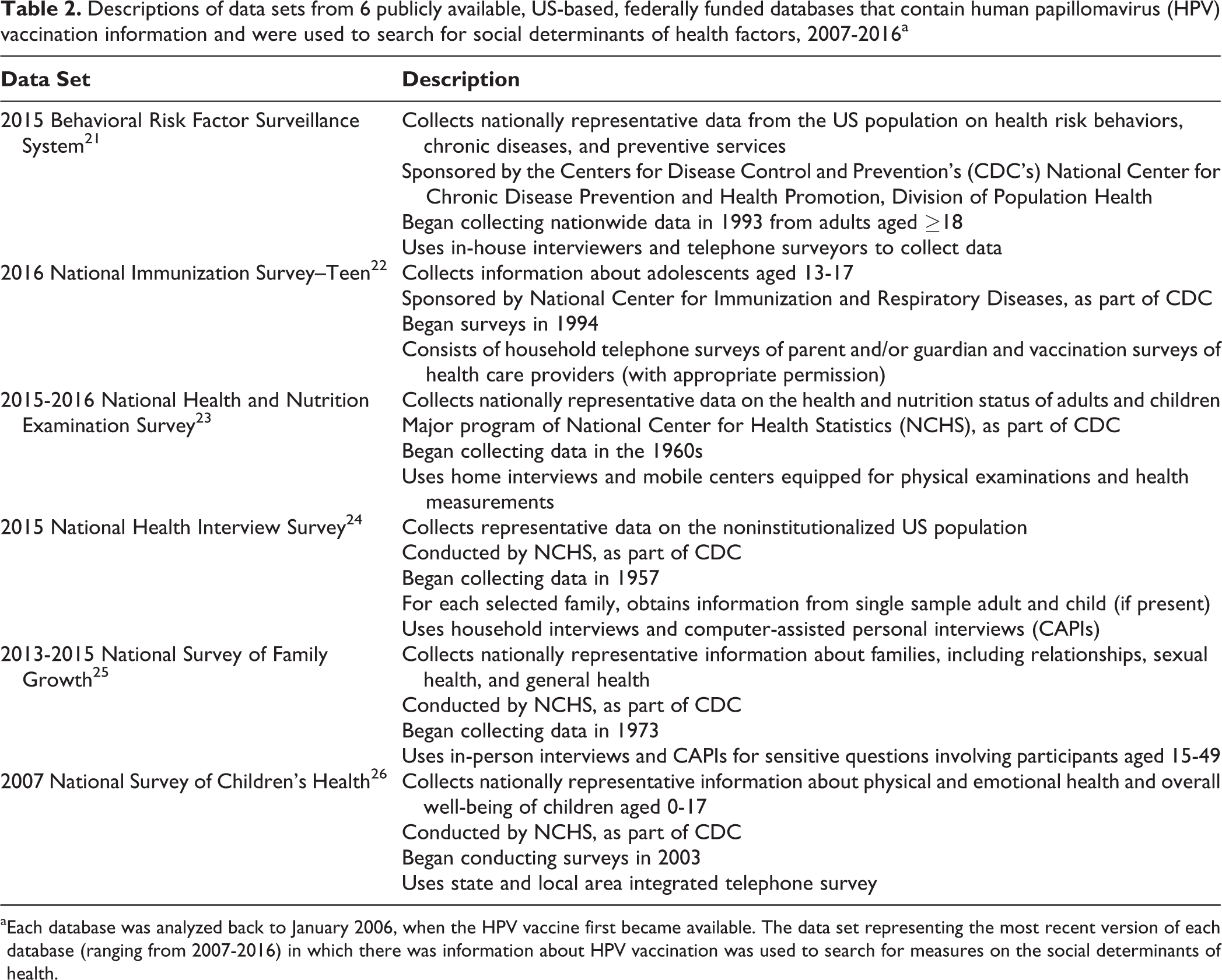
aEach database was analyzed back to January 2006, when the HPV vaccine first became available. The data set representing the most recent version of each database (ranging from 2007-2016) in which there was information about HPV vaccination was used to search for measures on the social determinants of health.
Results
HPV Vaccination
Each of the 6 data sets contained at least 2 items on HPV vaccine uptake and/or completion (Table 3). The age range of participants who were asked about HPV vaccination differed among the 6 surveys. In addition, the NSFG and NSCH surveys asked questions about HPV vaccination only among females, which limited the data available about males to the other 4 data sets.
Survey participants and human papillomavirus (HPV) vaccination survey questions used in data sets from 6 publicly available, US-based, nationally funded databases, 2007-2016a
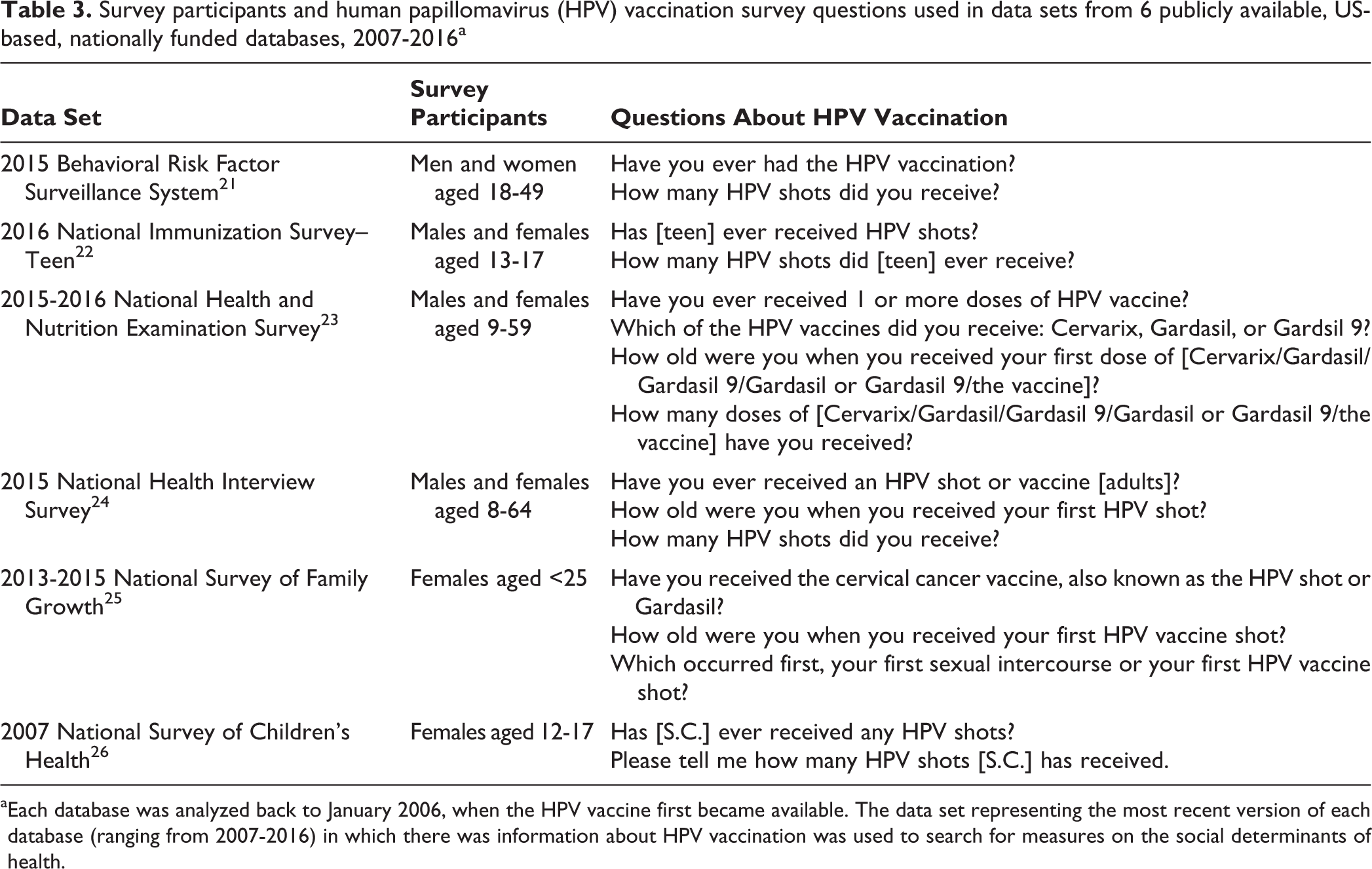
aEach database was analyzed back to January 2006, when the HPV vaccine first became available. The data set representing the most recent version of each database (ranging from 2007-2016) in which there was information about HPV vaccination was used to search for measures on the social determinants of health.
Overview of Social Determinants of Health Framework
None of the 6 data sets contained measures pertaining to all key areas of the social determinants of health as defined by the Healthy People 2020 social determinants of health framework (Table 1). The number of key areas covered by each data set varied. The NSCH contained data on measures pertaining to the most key areas (n = 13), and the NIS-Teen contained data on measures pertaining to the fewest key areas (n = 6).
Three social determinants of health domains appeared in all 6 data sets: education, economic stability, and health and health care (Table 1). The domain of social and community context appeared in only the NHIS, NSFG, and NSCH data sets, and the domain of neighborhood and built environment appeared in only the NHANES, NHIS, and NSCH data sets.
Economic stability domain
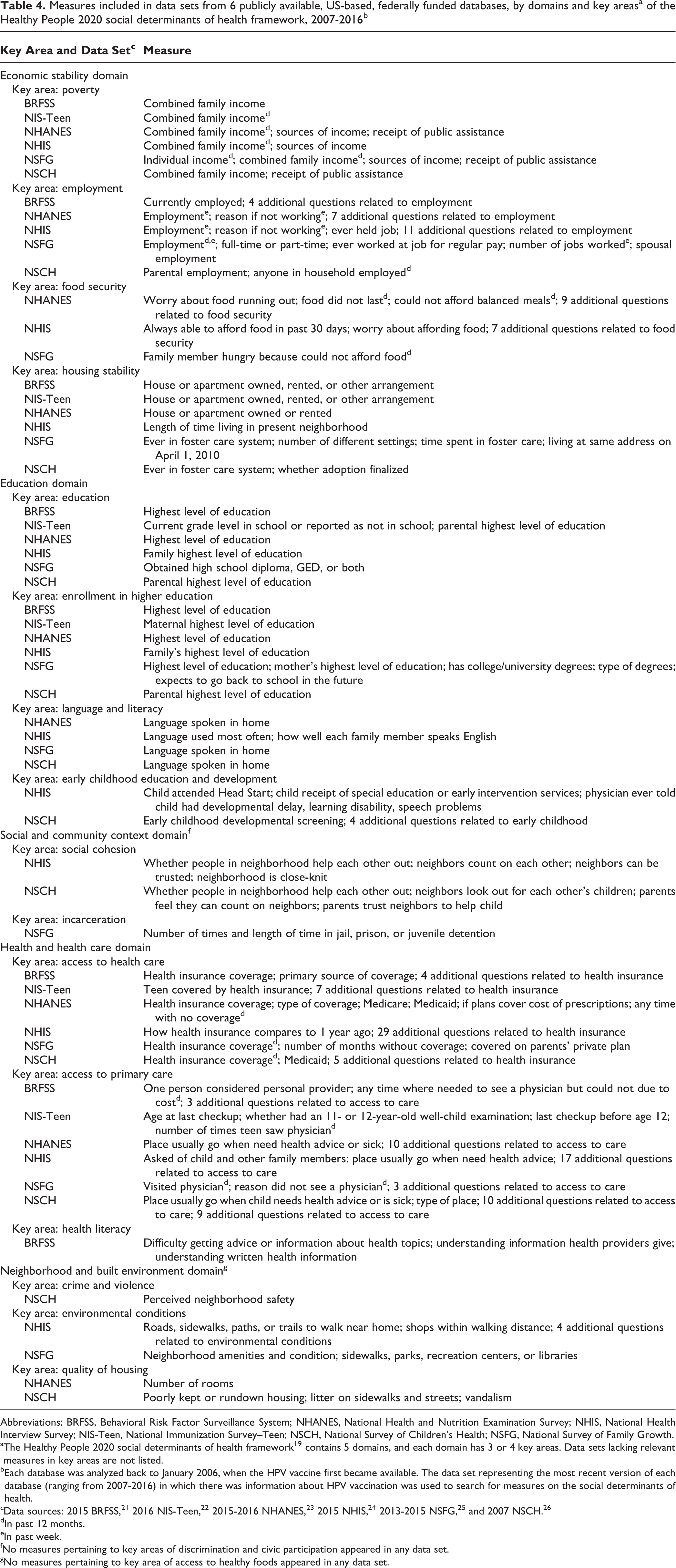
Each data set included measures pertaining to at least 2 of the 4 key areas in the economic stability domain (Table 4). Three data sets (NHANES, NHIS, and NSFG) included measures pertaining to all 4 key areas (poverty, employment, food security, and housing stability) of the economic stability domain. All 6 data sets included at least 1 measure pertaining to poverty and housing stability. All data sets except NIS-Teen also included a measure pertaining to employment. Finally, 3 data sets (NHANES, NHIS, and NSFG) included a measure pertaining to food security.
Measures included in data sets from 6 publicly available, US-based, federally funded databases, by domains and key areasa of the Healthy People 2020 social determinants of health framework, 2007-2016b
Abbreviations: BRFSS, Behavioral Risk Factor Surveillance System; NHANES, National Health and Nutrition Examination Survey; NHIS, National Health Interview Survey; NIS-Teen, National Immunization Survey–Teen; NSCH, National Survey of Children’s Health; NSFG, National Survey of Family Growth.
aThe Healthy People 2020 social determinants of health framework 19 contains 5 domains, and each domain has 3 or 4 key areas. Data sets lacking relevant measures in key areas are not listed.
bEach database was analyzed back to January 2006, when the HPV vaccine first became available. The data set representing the most recent version of each database (ranging from 2007-2016) in which there was information about HPV vaccination was used to search for measures on the social determinants of health.
cData sources: 2015 BRFSS, 21 2016 NIS-Teen, 22 2015-2016 NHANES, 23 2015 NHIS, 24 2013-2015 NSFG, 25 and 2007 NSCH. 26
dIn past 12 months.
eIn past week.
fNo measures pertaining to key areas of discrimination and civic participation appeared in any data set.
gNo measures pertaining to key area of access to healthy foods appeared in any data set.
Education domain
Each data set included measures pertaining to the key areas of high school graduation and enrollment in higher education (Table 4). Four data sets (NHANES, NHIS, NSFG, and NSCH) included a measure pertaining to the key area of language and literacy, and 2 data sets (NHIS and NSCH) included a measure pertaining to early childhood education and development.
Social and community context domain
None of the data sets included measures pertaining to the key areas of discrimination and civic participation (Table 4). Only 2 data sets (NHIS and NSCH) included measures pertaining to the key area of social cohesion, and only the NSFG data set included a measure pertaining to incarceration.
Health and health care domain
All 6 data sets included measures pertaining to the key areas of access to health care and access to primary care (Table 4). Only the BRFSS included measures pertaining to health literacy.
Neighborhood and built environment domain
None of the data sets included measures pertaining to the key area of access to healthy foods (Table 4). However, 2 data sets (NHIS and NSCH) included measures pertaining to environmental conditions, 2 data sets (NHANES and NSCH) included measures pertaining to quality of housing, and 1 data set (NSCH) included a measure pertaining to crime and violence.
Discussion
Identifying social determinants of health factors that contribute to health disparities is a public health priority. 19 We discovered numerous gaps in data on social determinants of health measures in national databases that include information about HPV vaccination. We also identified inconsistencies in the presence of social determinants of health measures in national surveys. For example, whereas all 6 data sets contained information about access to health care (most often these were results of survey questions about health insurance), only the BRFSS data set contained measures pertaining to health literacy. This finding is noteworthy because health literacy skills enable persons to make informed decisions about their health and, as such, may influence HPV vaccine uptake. 27
All data sets included measures in the economic stability domain. On one hand, high vaccine costs are not a proven barrier to vaccination for lower-income persons who are not covered by Medicaid or the Vaccines for Children Program. On the other hand, the economic stability domain (as measured by poverty, employment, food security, and housing stability) may influence the rate of HPV vaccine uptake. Before implementation of the Affordable Care Act, the economic stability domain may have played an even bigger role in HPV vaccine uptake than it does currently because of both the high cost of the vaccine and the fewer numbers of persons with health insurance coverage. 28,29
All 6 data sets contained measures pertaining to the key areas of high school graduation and enrollment in higher education in the education domain, yet only 2 data sets included measures pertaining to all 4 key areas in this domain. This finding suggests that the surveys could be improved by asking about more than just levels of advancement through the education system, for example, early childhood education and literacy.
None of the data sets included measures pertaining to the key areas of discrimination or civic participation in the social and community context domain. Furthermore, most of the data sets also lacked measures pertaining to the key areas of incarceration (n = 5) and social cohesion (n = 6). Yet measures pertaining to all 4 of the key areas in this domain may contribute to disparities in HPV vaccine uptake. For example, parental incarceration may affect whether a child or teen is vaccinated. In addition, community cohesion, particularly as it applies to developing positive attitudes about HPV vaccination, could play a role in herd protection (ie, when a sufficient proportion of a population is made immune to an infectious disease [eg, through vaccination] to make its spread from person to person unlikely) from HPV. 30 Interestingly, family structure was a key area previously included in the social and community context domain in the Healthy People 2020 social determinants of health framework, but it was removed in the 2015 update.
All 6 data sets contained measures pertaining to the key areas of access to primary care and access to health insurance in the health and health care domain. This information is important because HPV vaccines are typically delivered in a health care setting, and health insurance coverage is often required to gain access to this setting. Conversely, only 1 data set (BRFSS) included measures pertaining to the key area of health literacy. Health literacy plays a potentially important role in HPV vaccination, because low levels of understanding about HPV and the HPV vaccine could be associated with a reduced likelihood of adopting protective behaviors, including vaccination. 31
Most of the data sets in our study included only a few measures pertaining to key areas in the neighborhood and built environment domain. Yet measures in the key areas of access to healthy foods, crime and violence, environmental conditions, and quality of housing may each be relevant as proxy measures for social stability and are therefore relevant to vaccination. Low levels of social stability may contribute to disparities in HPV vaccination rates; as such, including survey questions about these measures may be valuable for assessing these disparities.
Overall, most of the data sets evaluated in this study contained measures pertaining to most of the social determinants of health domains and key areas. The NSCH and NHIS data sets had the best coverage of key areas of the social determinants of health. However, even these 2 data sets provided only limited information about the social and environmental factors that might affect HPV vaccine uptake. We acknowledge that the surveys generating these data sets may not have been built for studying the social determinants of health. However, because the social determinants of health framework is used as a guiding framework to assess public health issues, integration of more of these social determinants of health measures into future surveys is important.
Limitations
This study had several limitations. First, we did not extract data on race/ethnicity from the data sets because these data were not included in the Healthy People 2020 social determinants of health framework that we used. However, the relationship between race/ethnicity and HPV vaccine uptake may be confounded by underlying differences in social class, which would tend to be captured by using other social determinants of health factors. 32,33 Second, we included the older 2007 data set version from the NSCH database because subsequent versions of this database (2008-2016) did not include any questions on HPV vaccination. We would advocate for national data sets to retain questions on HPV vaccine uptake and completion measures in their questionnaires to allow trends in this priority area to be followed. Third, 2 of the surveys used to generate the data sets in our study were limited to females aged 11-26, and age ranges differed among all surveys. Limiting the age range and sex studied could make future research difficult to compare, especially because in 2018, the FDA approved vaccine uptake for males and females up to age 45. 34 National surveys should include HPV vaccination questions for males and females and for the entire age range for which HPV vaccination is recommended. Although approaches to HPV and its vaccine have historically been feminized, sex-neutral approaches to HPV vaccination should be pursued in the future. 35 Future evaluations should test for multicollinearity between the various social determinants of health predictor variables to reduce unstable coefficient estimates and difficulty interpreting results.
Conclusions
Most publicly available, US-based, federally funded data sets that include data on HPV vaccination lack comprehensive measures of the social determinants of health. Future research should examine the gaps in social determinants of health data in these data sets. Adding questions about the social determinants of health to the surveys that generate these data sets, particularly in the domains of social and community context and neighborhood and built environment, would strengthen the ability of public health researchers, policy makers, and professionals to identify associations between the social determinants of health and HPV vaccination. It could also lead to improved HPV vaccine uptake and prevention of HPV-related diseases.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.