
Abstract
Research shows that there is no risk-free level of exposure to secondhand smoke (SHS) and that eliminating smoking indoors fully protects nonsmokers from indoor SHS exposure. Casinos often allow smoking indoors and can be a source of involuntary SHS exposure for employees and visitors. We examined attitudes toward smoke-free casino policies among US adults. During June and July 2017, we used a web-based survey to ask a nationally representative sample of 4107 adults aged ≥18 about their attitudes toward smoke-free casinos. Among 4048 respondents aged ≥18, a weighted 75.0% favored smoke-free casino policies, including respondents who visited casinos about once per year (74.1%), several times per year (75.3%), and at least once per month (74.2%). Although the sociodemographic characteristics of respondents who favored smoke-free casino policies varied, the majority in each group, except current smokers (45.4%), supported smoke-free policies. Allowing smoking inside casinos involuntarily exposes casino employees and visitors to SHS, a known and preventable health risk. Further assessment of public knowledge and attitudes toward smoke-free casinos at state and local levels may help inform tobacco control policy, planning, and practice.
Exposure to secondhand smoke (SHS) causes heart disease, stroke, and lung cancer in nonsmoking adults. 1,2 Studies have found no risk-free level of exposure to SHS, and even brief exposure to SHS can be harmful to health. 1 -3 SHS exposure causes approximately 41 000 deaths among nonsmoking adults each year. 2 A 2006 report by the surgeon general concluded that eliminating smoking in indoor spaces fully protects nonsmokers from exposure to SHS and that separating smokers from nonsmokers, cleaning the air, and ventilating buildings cannot eliminate SHS exposure among nonsmokers. 1
Considerable progress has been made during the past 3 decades in protecting nonsmokers from SHS through implementation of comprehensive state and local laws that prohibit smoking in indoor areas of worksites, restaurants, and bars. However, smoke-free laws frequently exempt casinos, 4,5 due in part to opposition from casino owners. Studies of air quality in casinos that allow smoking have found high levels of SHS and have documented that SHS can infiltrate areas of casinos where smoking is not permitted. 5 For example, a study of 3 casinos in Las Vegas, Nevada, found elevated levels of nicotine and chemicals from indoor SHS and also examined biomarker data and found that casino employees had absorbed carcinogens that are present in SHS. 6,7 The American Gaming Association estimates that 34% of US adults aged ≥21 (76 million people) visited casinos in 2012 8 and that more than 361 000 persons were directly employed by commercial casinos nationwide as of 2017. 9 These data suggest that when smoking is allowed in indoor areas of casinos, millions of nonsmoking casino visitors and hundreds of thousands of employees can be involuntarily exposed to SHS and related toxicants. 5 -7,10,11
Studies have reviewed the scientific literature on air quality, SHS exposure, health effects, and economic outcomes related to SHS and smoking restrictions in casinos, as well as on smoking prevalence among casino visitors and problem gamblers. 5 To our knowledge, however, no studies have exclusively assessed adult attitudes toward smoke-free casinos in the United States. For example, a study from 2009-2010 assessed attitudes toward smoke-free bars, casinos, and clubs combined by using a single question but did not determine respondents’ attitudes toward smoking in each venue type. 12 To address this gap in the literature, we assessed attitudes toward smoke-free casinos among US adults in 2017.
Methods
Data Source
Data came from SummerStyles, a proprietary web-based cross-sectional survey of US adults aged ≥18. Porter Novelli conducts SummerStyles via GfK’s KnowledgePanel, the largest online panel that is representative of the US population. 13,14 Through address-based probability sampling, KnowledgePanel members are randomly recruited regardless of whether they have a landline telephone or internet access to maintain a pool of approximately 55 000 panelists. 15 During June and July 2017, a total of 4107 of 5586 randomly selected participants completed SummerStyles, for a response rate of 74%. Consistent with previous years, survey weights were generated to match Current Population Survey proportions to achieve representativeness of the US adult population. 14,16 -18 For SummerStyles 2017, data were weighted to match 2016 Current Population Survey proportions for 8 factors, including sex, age, household income, race/ethnicity, household size, education, US Census region, and metropolitan status.
Measure
To assess attitudes toward smoke-free casino policies, respondents were asked, “Do you favor or oppose smoke-free policies that prohibit smoking tobacco in all areas of a casino?” Response options included “strongly favor,” “somewhat favor,” “somewhat oppose,” and “strongly oppose.” Adults who responded “strongly favor” or “somewhat favor” were considered to favor smoke-free casino policies.
Statistical Analysis
We calculated point estimates and 95% confidence intervals (CIs) overall and by sex (male, female); age (18-24, 25-44, 45-64, ≥65), race/ethnicity (non-Hispanic white, non-Hispanic black, non-Hispanic other, Hispanic), education (<high school graduate, high school graduate, some college, college graduate), annual household income (<$30 000, $30 000-$59 999, $60 000-$99 999, $100 000-$149 000, ≥$150 000), average casino visit frequency (does not visit, every 3 years or more, about once every 2 years, about once a year, several times a year, at least once a month, or don’t know/not sure), US Census region (Northeast: Connecticut, Maine, Massachusetts, New Hampshire, New Jersey, New York, Pennsylvania, Rhode Island, and Vermont; Midwest: Illinois, Indiana, Iowa, Kansas, Michigan, Minnesota, Missouri, Nebraska, North Dakota, Ohio, South Dakota, and Wisconsin; South: Alabama, Arkansas, Delaware, District of Columbia, Florida, Georgia, Kentucky, Louisiana, Maryland, Mississippi, North Carolina, Oklahoma, South Carolina, Tennessee, Texas, Virginia, and West Virginia; West: Alaska, Arizona, California, Colorado, Hawaii, Idaho, Montana, Nevada, New Mexico, Oregon, Utah, Washington, and Wyoming), whether the respondent lived with a tobacco product user (yes, no), cigarette smoking status (current, former, never), and use of other noncigarette tobacco products (current, former, never).
Current cigarette smokers were defined as respondents who smoked ≥100 cigarettes in their lifetime and reported smoking “every day” or “some days” at the time of the survey. Former smokers were defined as respondents who smoked ≥100 cigarettes in their lifetime and reported smoking “not at all” at the time of the survey. Never smokers were defined as respondents who reported no to smoking ≥100 cigarettes in their lifetime. Noncigarette tobacco products included cigars (eg, big cigars, cigarillos, or little cigars that look like cigarettes); electronic vapor products (eg, e-cigarettes, e-hookahs, e-cigars, e-pipes, hookah pens, vape pens, or some other electronic vapor product); smokeless tobacco (eg, chewing tobacco, snuff, dip, snus, or dissolvable tobacco); pipes filled with tobacco; water pipes, also known as hookahs filled with tobacco; or some other tobacco product.
We calculated adjusted prevalence ratios (aPRs) of favorability by using multivariate Poisson regression analysis. We used a 2-tailed t test of significance, with P < .05 considered significant. We conducted all analyses by using R version 3.2.3. 19 Because this study was a secondary analysis of deidentified survey data, the Centers for Disease Control and Prevention considered it exempt from human subjects review.
Results
Overall, 75.0% of US adults favored (55.1% strongly favored and 20.0% somewhat favored), 13.6% somewhat opposed, and 11.4% strongly opposed smoke-free casinos (Tables 1 and 2). Favorability was 71.5% among men and 78.3% among women. By age, favorability ranged from 71.7% among adults aged 25-44 to 81.6% among adults aged ≥65; by race/ethnicity, from 66.4% among non-Hispanic black adults to 80.4% among non-Hispanic other adults; by education level, from 63.4% among adults who did not graduate from high school to 81.7% among adults with a college degree; by income, from 66.7% among adults with <$30 000 in annual household income to 80.8% among adults with ≥$150 000 in annual household income; and by US Census region, from 72.4% in the South to 77.4% in the West.
Attitudes toward smoke-free casinos among US adults, 2017a,b
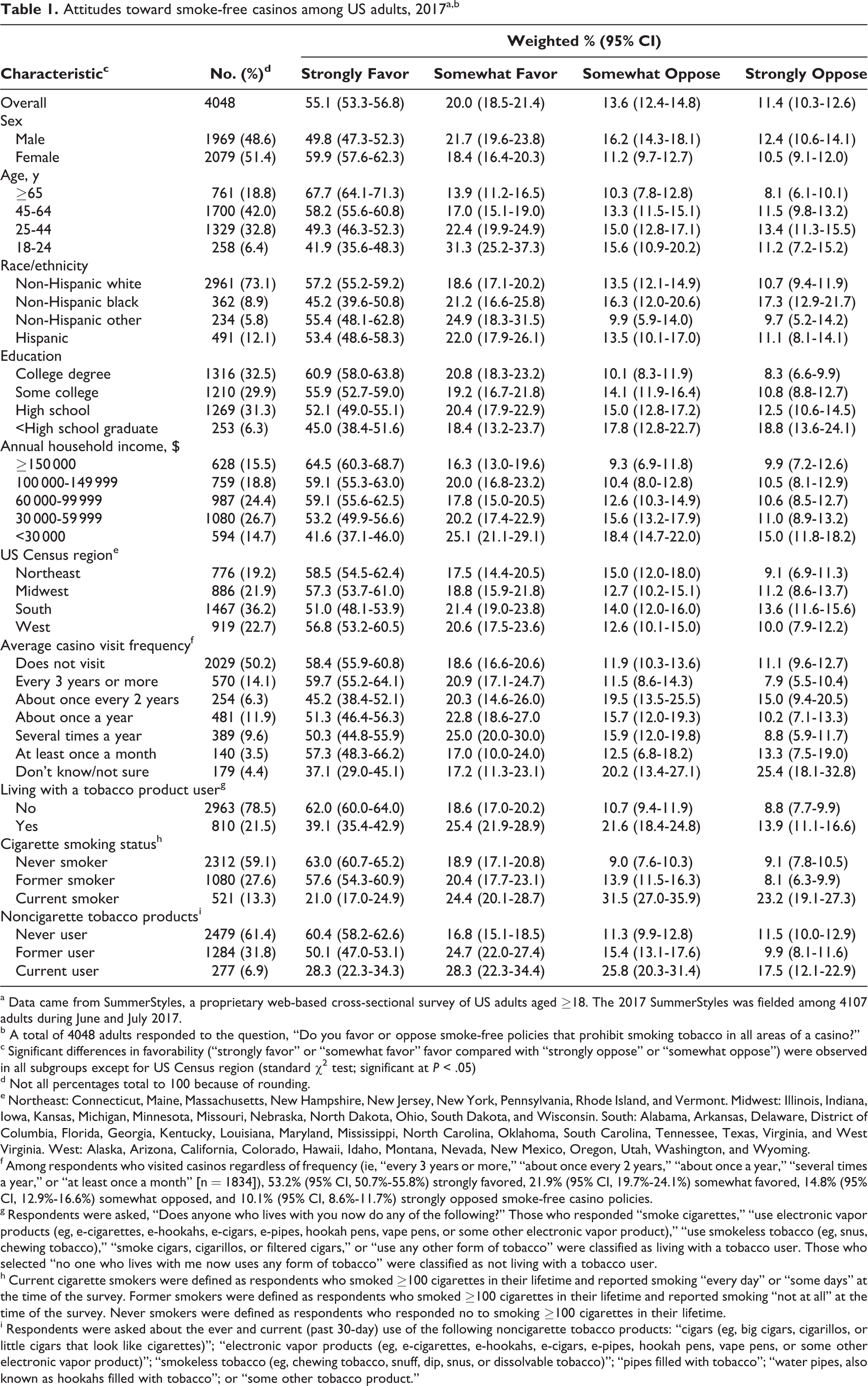
a Data came from SummerStyles, a proprietary web-based cross-sectional survey of US adults aged ≥18. The 2017 SummerStyles was fielded among 4107 adults during June and July 2017.
b A total of 4048 adults responded to the question, “Do you favor or oppose smoke-free policies that prohibit smoking tobacco in all areas of a casino?”
c Significant differences in favorability (“strongly favor” or “somewhat favor” favor compared with “strongly oppose” or “somewhat oppose”) were observed in all subgroups except for US Census region (standard χ2 test; significant at P < .05)
d Not all percentages total to 100 because of rounding.
e Northeast: Connecticut, Maine, Massachusetts, New Hampshire, New Jersey, New York, Pennsylvania, Rhode Island, and Vermont. Midwest: Illinois, Indiana, Iowa, Kansas, Michigan, Minnesota, Missouri, Nebraska, North Dakota, Ohio, South Dakota, and Wisconsin. South: Alabama, Arkansas, Delaware, District of Columbia, Florida, Georgia, Kentucky, Louisiana, Maryland, Mississippi, North Carolina, Oklahoma, South Carolina, Tennessee, Texas, Virginia, and West Virginia. West: Alaska, Arizona, California, Colorado, Hawaii, Idaho, Montana, Nevada, New Mexico, Oregon, Utah, Washington, and Wyoming.
f Among respondents who visited casinos regardless of frequency (ie, “every 3 years or more,” “about once every 2 years,” “about once a year,” “several times a year,” or “at least once a month” [n = 1834]), 53.2% (95% CI, 50.7%-55.8%) strongly favored, 21.9% (95% CI, 19.7%-24.1%) somewhat favored, 14.8% (95% CI, 12.9%-16.6%) somewhat opposed, and 10.1% (95% CI, 8.6%-11.7%) strongly opposed smoke-free casino policies.
g Respondents were asked, “Does anyone who lives with you now do any of the following?” Those who responded “smoke cigarettes,” “use electronic vapor products (eg, e-cigarettes, e-hookahs, e-cigars, e-pipes, hookah pens, vape pens, or some other electronic vapor product),” “use smokeless tobacco (eg, snus, chewing tobacco),” “smoke cigars, cigarillos, or filtered cigars,” or “use any other form of tobacco” were classified as living with a tobacco user. Those who selected “no one who lives with me now uses any form of tobacco” were classified as not living with a tobacco user.
h Current cigarette smokers were defined as respondents who smoked ≥100 cigarettes in their lifetime and reported smoking “every day” or “some days” at the time of the survey. Former smokers were defined as respondents who smoked ≥100 cigarettes in their lifetime and reported smoking “not at all” at the time of the survey. Never smokers were defined as respondents who responded no to smoking ≥100 cigarettes in their lifetime.
i Respondents were asked about the ever and current (past 30-day) use of the following noncigarette tobacco products: “cigars (eg, big cigars, cigarillos, or little cigars that look like cigarettes)”; “electronic vapor products (eg, e-cigarettes, e-hookahs, e-cigars, e-pipes, hookah pens, vape pens, or some other electronic vapor product)”; “smokeless tobacco (eg, chewing tobacco, snuff, dip, snus, or dissolvable tobacco)”; “pipes filled with tobacco”; “water pipes, also known as hookahs filled with tobacco”; or “some other tobacco product.”
Adjusted prevalence ratios of favorability toward smoke-free casinos among US adults, 2017a
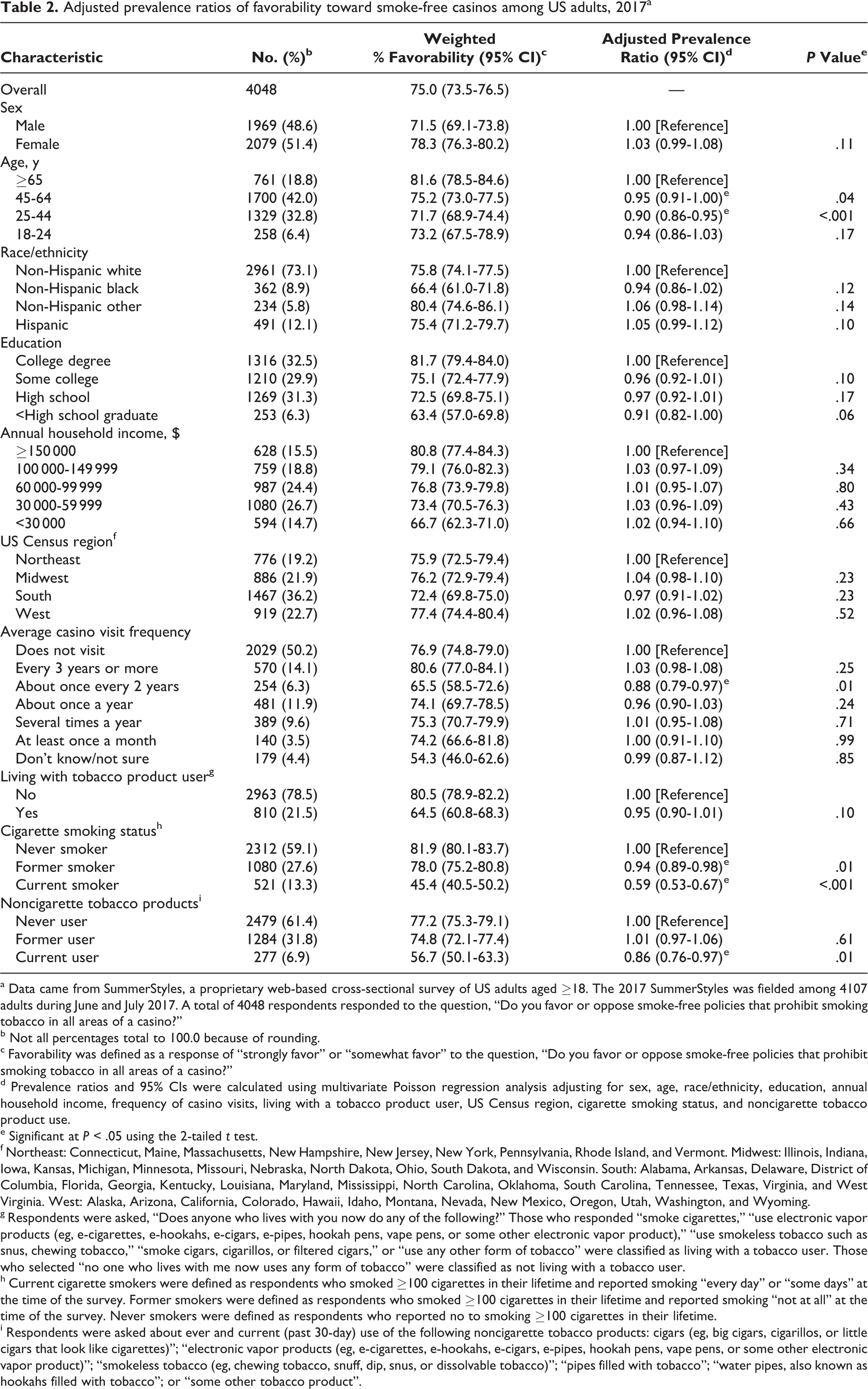
a Data came from SummerStyles, a proprietary web-based cross-sectional survey of US adults aged ≥18. The 2017 SummerStyles was fielded among 4107 adults during June and July 2017. A total of 4048 respondents responded to the question, “Do you favor or oppose smoke-free policies that prohibit smoking tobacco in all areas of a casino?”
b Not all percentages total to 100.0 because of rounding.
c Favorability was defined as a response of “strongly favor” or “somewhat favor” to the question, “Do you favor or oppose smoke-free policies that prohibit smoking tobacco in all areas of a casino?”
d Prevalence ratios and 95% CIs were calculated using multivariate Poisson regression analysis adjusting for sex, age, race/ethnicity, education, annual household income, frequency of casino visits, living with a tobacco product user, US Census region, cigarette smoking status, and noncigarette tobacco product use.
e Significant at P < .05 using the 2-tailed t test.
f Northeast: Connecticut, Maine, Massachusetts, New Hampshire, New Jersey, New York, Pennsylvania, Rhode Island, and Vermont. Midwest: Illinois, Indiana, Iowa, Kansas, Michigan, Minnesota, Missouri, Nebraska, North Dakota, Ohio, South Dakota, and Wisconsin. South: Alabama, Arkansas, Delaware, District of Columbia, Florida, Georgia, Kentucky, Louisiana, Maryland, Mississippi, North Carolina, Oklahoma, South Carolina, Tennessee, Texas, Virginia, and West Virginia. West: Alaska, Arizona, California, Colorado, Hawaii, Idaho, Montana, Nevada, New Mexico, Oregon, Utah, Washington, and Wyoming.
g Respondents were asked, “Does anyone who lives with you now do any of the following?” Those who responded “smoke cigarettes,” “use electronic vapor products (eg, e-cigarettes, e-hookahs, e-cigars, e-pipes, hookah pens, vape pens, or some other electronic vapor product),” “use smokeless tobacco such as snus, chewing tobacco,” “smoke cigars, cigarillos, or filtered cigars,” or “use any other form of tobacco” were classified as living with a tobacco user. Those who selected “no one who lives with me now uses any form of tobacco” were classified as not living with a tobacco user.
h Current cigarette smokers were defined as respondents who smoked ≥100 cigarettes in their lifetime and reported smoking “every day” or “some days” at the time of the survey. Former smokers were defined as respondents who smoked ≥100 cigarettes in their lifetime and reported smoking “not at all” at the time of the survey. Never smokers were defined as respondents who reported no to smoking ≥100 cigarettes in their lifetime.
i Respondents were asked about ever and current (past 30-day) use of the following noncigarette tobacco products: cigars (eg, big cigars, cigarillos, or little cigars that look like cigarettes)”; “electronic vapor products (eg, e-cigarettes, e-hookahs, e-cigars, e-pipes, hookah pens, vape pens, or some other electronic vapor product)”; “smokeless tobacco (eg, chewing tobacco, snuff, dip, snus, or dissolvable tobacco)”; “pipes filled with tobacco”; “water pipes, also known as hookahs filled with tobacco”; or “some other tobacco product”.
Smoke-free casinos were favored by 75.1% of adults who reported going to casinos, with similar favorability among respondents who visited casinos about once a year (74.1%), several times a year (75.3%), and at least once a month (74.2%). Favorability ranged from 65.5% among adults who visited casinos about once every 2 years to 80.6% among adults who visited casinos every 3 years or more (Tables 1 and 2). Favorability was 76.9% among adults who did not visit casinos. Favorability was 64.5% among adults living with a tobacco product user and 80.5% among adults not living with a tobacco product user. By smoking status, favorability ranged from 45.4% among current cigarette smokers to 81.9% among never smokers and from 56.7% among current users of other noncigarette tobacco products to 77.2% among never users.
By age, the adjusted likelihood of favoring smoke-free casinos was significantly lower among adults aged 25-44 (aPR = 0.90; 95% CI, 0.86-0.95) and 45-64 (aPR = 0.95; 95% CI, 0.91-1.00) than among adults aged ≥65 (Table 2). The adjusted likelihood of favoring smoke-free casinos was also significantly lower among current (aPR = 0.59; 95% CI, 0.53-0.67) and former (aPR = 0.94; 95% CI, 0.89-0.98) cigarette smokers than among never smokers and among current users of other noncigarette tobacco products (aPR = 0.86; 95% CI, 0.76-0.97) than among never users. Moreover, the adjusted likelihood of favorability was lower among adults who visited casinos about once every 2 years than among adults who did not visit casinos (aPR = 0.88; 95% CI, 0.79-0.97).
Discussion
Hundreds of thousands of employees work in casinos, and millions of persons visit casinos every year. 8,9 Although state and local laws frequently exempt or exclude casinos, several states, including Colorado, Delaware, Florida, Illinois, Maryland, New York, Ohio, and South Dakota, prohibit smoking in indoor areas of nontribal commercial casinos. 5,20 Some local jurisdictions, including in Baton Rouge and New Orleans, Louisiana, have also implemented laws requiring casinos to be smoke-free. 21 Some critics of smoke-free policies in casinos contend that casino patrons are more likely to smoke than the general population and, as a result, prohibiting smoking may reduce casino revenues. 5,22 -24 Although multiple studies on the economic impact of smoke-free casino policies have yielded differing findings on the impact on gaming revenue, 5 several studies have found that smoking prevalence among casino patrons is similar to smoking prevalence among adults overall. 5,22 Our findings that nearly half (45.4%) of smokers and three-quarters of casino visitors favor smoke-free casinos can further inform discussions on this topic.
At least 15 US states that allow commercial casinos have no smoking restrictions or partial restrictions in casinos, 5,20 and few tribal casinos have implemented smoke-free policies. 21 Examples of state laws partially restricting smoking in casinos include a Pennsylvania state law that establishes smoking and nonsmoking gaming areas and a Nevada state law that allows smoking on casino gaming floors but prohibits smoking in casino restaurants and retail spaces. 5 Air quality and biomarker studies, including studies conducted in casinos, have found that partial smoking restrictions do not prevent SHS from infiltrating nonsmoking areas. 5 -7,10,11
Limitations
Our study had 3 limitations. First, although SummerStyles draws from an existing panel with a nationally representative sample, the web-based survey does not recruit participants by using population-based probability samples, and, thus, our study may have limited generalizability. However, these data were weighted to be nationally representative, and previous tobacco use estimates from SummerStyles have been consistent with findings from other large national household surveys, 16 such as the National Health Interview Survey. Second, data were self-reported, which could result in misreporting of tobacco product use behaviors and frequency of casino visits. Finally, the cross-sectional design of SummerStyles precluded establishing any causal relationships between the assessed covariates and attitudes toward smoke-free casino policies.
Conclusion
Understanding public attitudes toward public health interventions can inform policy and planning of tobacco prevention and control programs. This study found that three-quarters of US adults favored smoke-free casino policies, including three-quarters of adults who visited casinos regularly and nearly half of cigarette smokers. Allowing smoking inside casinos involuntarily exposes millions of casino visitors and hundreds of thousands of casino employees to SHS, a known and preventable health risk. Similar assessments of public knowledge and attitudes toward smoke-free casinos, including assessments of casino worker attitudes and health outcomes, can help further guide tobacco control policy, planning, and practice.
Footnotes
Acknowledgment
The findings and conclusions in this article are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.