
Abstract
Objective:
Much of the research on the effects of childhood adversity on mental health has focused on adults. The objective of our study was to examine the individual and cumulative effect of childhood adversity on mental health service use among children.
Methods:
We used data from the 2011-2012 National Survey of Children’s Health (n = 79 834) to determine the use of mental health services in the past 12 months among children aged 2-17. The independent variables of interest were experiencing any 1 of 9 adverse family experiences (AFEs). We used logistic regression models to determine if each AFE was associated with mental health service use. We also examined AFEs as a continuous measure, representing the number of AFEs (ranging from 0 to 9) that summed them individually, and we examined age-by-AFE and age-by-need interaction terms. We adjusted all models for confounders.
Results:
Compared with not experiencing an AFE, experiencing all AFEs was associated with higher odds of mental health service use. Neighborhood violence was associated with the greatest increase in odds of mental health service use (adjusted odds ratio [aOR] = 2.35; 95% confidence interval [CI], 2.00-2.77). When measured as a continuous scale, each additional AFE was associated with higher odds of mental health service use (aOR = 1.33; 95% CI, 1.28-1.37). The effect of AFEs on mental health service use decreased with age.
Conclusions:
The observed association between AFEs and use of mental health services may be attributable to more severe or poorly managed mental illness among these children. Efforts are needed to increase access to and quality of mental health care among children affected by AFEs.
Childhood adversities, such as child abuse and household dysfunction, are associated with various negative health outcomes and health behaviors. Children who experience childhood adversities are more likely than children who do not experience these adversities to have conditions such as chronic obstructive pulmonary disease and sexually transmitted diseases as adults. 1,2 However, the most consistent association between childhood adversity and health is with mental illness. Experiences of adversity are associated with higher odds of mental illness, including depression, anxiety, suicide attempts, hallucinations, and substance use, among adults with a history of childhood adversity than among adults without a history of adversity. 3 -8 At a population level, childhood adversities account for almost 30% of cases of mental illness. 9 Of all adversities, experiencing child abuse and being exposed to violence in the family are the most consistent predictors of mental illness. 10 Among children who are experiencing or have experienced adversity, elevated rates of various mental illnesses are also seen. 11 -14 The reasons for these associations are multifaceted and include (1) changes in brain chemistry and function, 15,16 (2) social and cognitive impairments, and (3) adoption of risky health behaviors, including substance use, to cope with trauma and stress. 17
The elevated burden of mental illness among adults with a history of childhood adversity may correspond with an elevated use of health services in general and mental health services in particular. Compared with adults without a history of child abuse, adults with a history of child abuse have higher rates of using a range of health services, including mental health, emergency department, hospital outpatient, pharmacy, primary care, and specialty care. 18 Also, reporting childhood adversity predicts future prescriptions for a wide variety of psychotropic medications (ie, antidepressants, antipsychotics, mood stabilizers, and anxiolytics) among adults. 19 Among adults with psychosis, parental separation is associated with longer admissions to psychiatric wards and lower rates of compliance with medications, as compared with adults without psychosis, suggesting that adversity may increase the use of some services because of more intense symptoms or poorer disease management. 20
Some research has examined the effect of early life adversity on use of mental health services among children. For example, persons who experience child abuse and bullying have higher levels of mental health service use than persons who do not experience child abuse or bullying. 21,22 This finding is exacerbated by the finding that children in the foster care system, who may have extensive experience with adversity, represent a disproportionate share of mental health service use. 23 However, other research examining the broader category of important life events shows that experiencing a life event during the past year was not associated with use of mental health services in children but was associated with increased parental perceptions that a child was exhibiting problematic behavior. 24 Thus, parents may become more attentive to their children when they exhibit problematic behavior but not necessarily to the point at which they seek care for their children.
The current body of research has several shortcomings. First, much of the work has examined how childhood adversities affect the use of mental health services among adults. Thus, we do not fully know if the pattern of use develops before adulthood. Relatedly, we do not know at what age the association between early life adversity and use of mental health services manifests, if the effect of early life adversity varies with age among children, or if this association is observed only among children with a need for mental health services (eg, having a behavioral, mental, congenital, or developmental condition). Second, when children are the focus, studies examine only a single adversity or use generalized measures of stressors. As a result, it is not known how a wide variety of early life adversities affects the use of mental health services in the same population.
To address shortcomings in the research, we examined which childhood adversities are associated with the use of mental health services, whether the effect of adversity is cumulative, and whether this effect varies with age or presence of a behavioral, mental, congenital, or developmental condition.
Methods
Data
Data for our study came from the 2011-2012 National Survey of Children’s Health (NSCH). This cross-sectional, multistage, random-digit-dial telephone survey of the civilian, noninstitutionalized US population interviewed parents or guardians of children aged 0-17. 25 Respondents answered questions about themselves and about a randomly selected child living in the household. 25 The survey was conducted in English, Spanish, Cantonese, Mandarin, Vietnamese, and Korean. Surveys were completed from February 2011 through June 2012. Because data were publicly available and devoid of sensitive or identifying information, no institutional review board approval was required. Although more recent NSCH data have been released, the 2016 NSCH includes >40 000 fewer respondents than the 2011-2012 NSCH. Thus, we used the 2011-2012 NSCH to provide greater statistical power.
A total of 95 677 surveys were completed. 25 Because mental health services questions were asked only about children aged 2-17, the sample was restricted to the 85 637 children in this age range. We excluded respondents who were missing data on any study variable, with the exception of household income, yielding an analytic sample of 79 834 children. Because a sizable proportion of respondents were missing data on household income, we included them in the sample and listed data on household income as missing.
Measures
The outcome measure was a dichotomous indicator of mental health service use. Respondents were asked if the selected child had received any treatment or counseling from a mental health professional in the past 12 months. Respondents were told that mental health professionals included psychiatrists, psychologists, psychiatric nurses, and clinical social workers; however, the survey did not obtain data on the type of mental health professional(s) from whom services were obtained. The children of respondents who answered yes were classified as having used mental health services.
The main independent variable of interest comprised a 9-item adverse family experiences (AFEs) scale. The AFE scale is similar to the adverse childhood experiences (ACEs) scale 26 but does not include measures of child abuse; instead, it includes measures of economic hardship, racial or ethnic discrimination, death of a parent, and neighborhood violence. In the NSCH, the AFE scale asked parents or guardians to report on the experiences of children in their households (Table 1). Each AFE item measured whether the child had ever experienced that AFE during his or her lifetime. The AFEs represented lifetime exposure and did not include information about when the AFE occurred. For our analyses, we treated the 9 AFEs in 2 ways: (1) 9 individual dichotomous variables and (2) a continuous scale representing the number of AFEs the child had experienced.
Questions about adverse family experiences, National Survey of Children’s Health, 2011-2012a
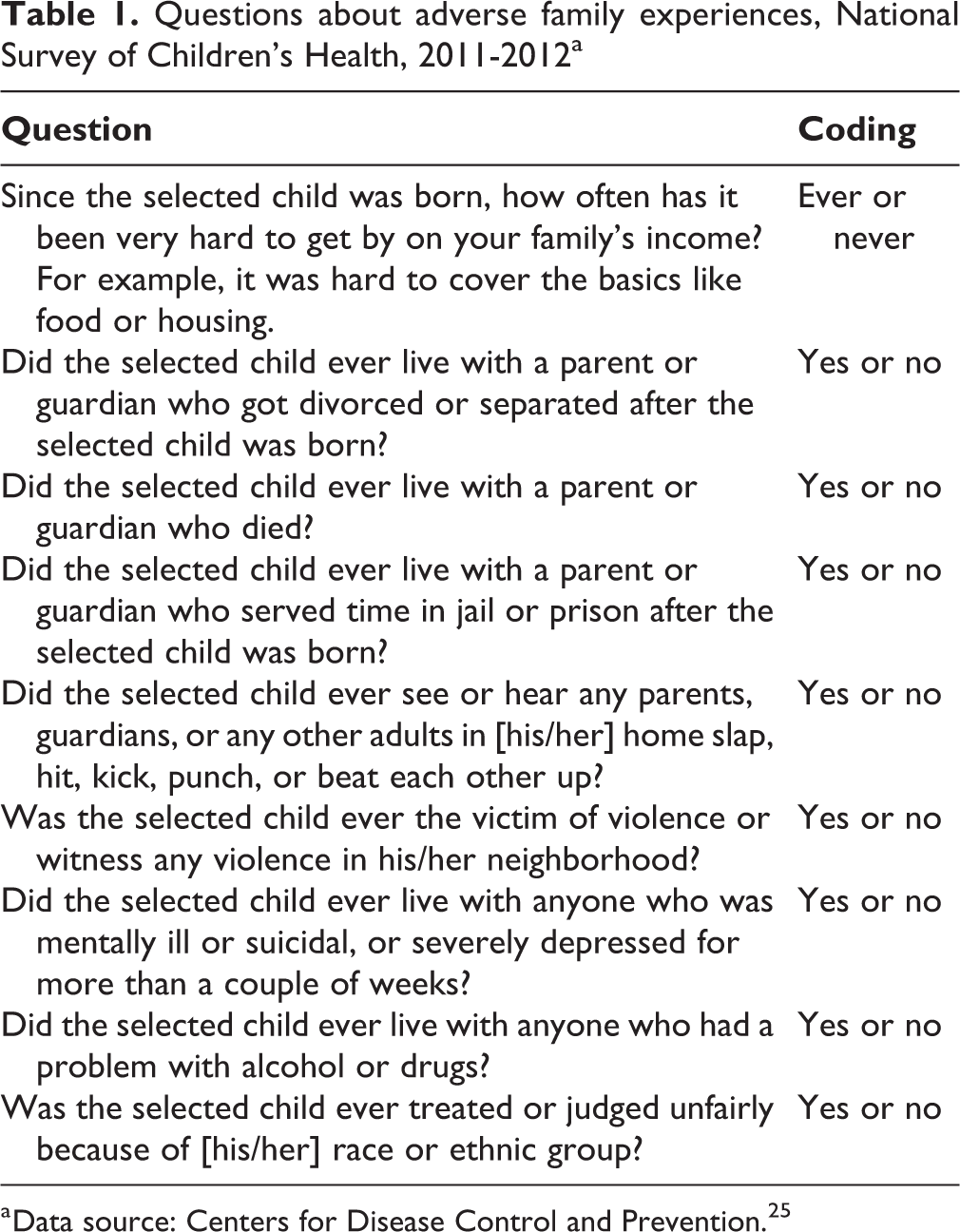
a Data source: Centers for Disease Control and Prevention. 25
Correlation coefficients between AFE items did not exceed 0.40. The strongest correlations were between children who lived with someone who had problems with drugs or alcohol and children who lived with a parent or guardian who had been jailed or incarcerated (r = 0.40) or lived with adults who abused each other (r = 0.40). All other items had correlation coefficients of ≤0.36. In an assessment of multicollinearity between AFE items, variance inflation factors ranged from 1.02 to 1.39. These values were below the recommended variance inflation factor threshold of 10, 27 suggesting that multicollinearity was not an issue.
We included several variables as confounders based on the Behavioral Model of Health Service Use and known correlates of mental health service use among children, such as age, sex, and race/ethnicity. 28,29 Briefly, this model states that use of health services is shaped by predisposing factors (eg, demographic, social structure, and health beliefs), enabling factors (eg, access to care, family resources), and need. 28 Predisposing factors included demographic characteristics of the child, such as age, sex, ethnicity (Hispanic or non-Hispanic), and race (black, white, or other), as well as parental or household factors, including primary language spoken at home (English or other) and the respondent’s relationship to the child (mother, father, or other). Enabling factors included a child’s health insurance status (insured or uninsured), whether a child had a usual source of health care (yes or no), and household income as a percentage of the federal poverty level (FPL) (0%-100%, 101%-200%, ≥201%, and missing). Finally, we measured need by using a child’s health status (fair or poor vs excellent, very good, or good) and having at least 1 behavioral, mental, congenital, or developmental condition in his or her lifetime. These conditions included attention deficit disorder, attention deficit hyperactivity disorder, depression, anxiety, behavioral conduct, autism, Asperger syndrome, developmental delays, intellectual disabilities, cerebral palsy, or Tourette syndrome. The measure of health status was a single item asking a parent or guardian to report on the child’s health status, in general. As a result, the measure captured data on facets of both physical and mental health. Furthermore, because this measure was independent of reports of other health conditions, reported health status reflected the degree to which these conditions were successfully treated or managed.
Analyses
We conducted all analyses by using Stata version 14.2 30 and using survey weights to account for survey design. We calculated univariate statistics for all variables. We conducted logistic regression models by calculating the odds of mental health service use with each of 9 AFEs, including all confounders. We then used a model with all AFEs and confounders in the same model to determine whether AFEs had an effect on the outcome, independent of all other AFEs. We then tested interaction terms for age and each AFE item. To illustrate interactions, we stratified models into broad age groups (2-5, 6-11, 12-17), treating age as a categorical variable. We built these interaction models on the models in which each AFE was in a separate model. We tested interaction terms for lifetime behavioral, mental, congenital, or developmental condition and each AFE item by using interactions and stratified analyses. We assessed significance using t-tests, and we considered P < .05 to be significant.
Results
Of 79 834 children in the sample, 9.4% (95% CI, 8.9%-9.9%) had used mental health services in the past 12 months (Table 2). On average, children had more than 1 adversity (mean = 1.3; 95% CI, 1.3-1.4). The most common AFE was financial hardship (58.2%; 95% CI, 57.5%-59.0%). Most children were non-Hispanic/Latino (77.5%; 95% CI, 76.7%-78.3%); were white (66.8%; 95% CI, 66.0%-67.6%); were insured (94.3%; 95% CI, 93.9%-94.7%); were in excellent, very good, or good health (96.8%; 95% CI, 96.5%-97.1%); and lacked any behavioral, mental, congenital, or developmental condition (79.1%; 95% CI, 78.5%-79.7%). Most respondents were mothers of selected children (70.9%; 95% CI, 70.2%-71.6%), and most children lived in households that spoke primarily English (85.6%; 95% CI, 84.9%-86.3%).
Characteristics of children aged 2-17 (N = 79 834) in a study examining the association between adverse family experiences and use of mental health services, National Survey of Children’s Health, United States, 2011-2112a
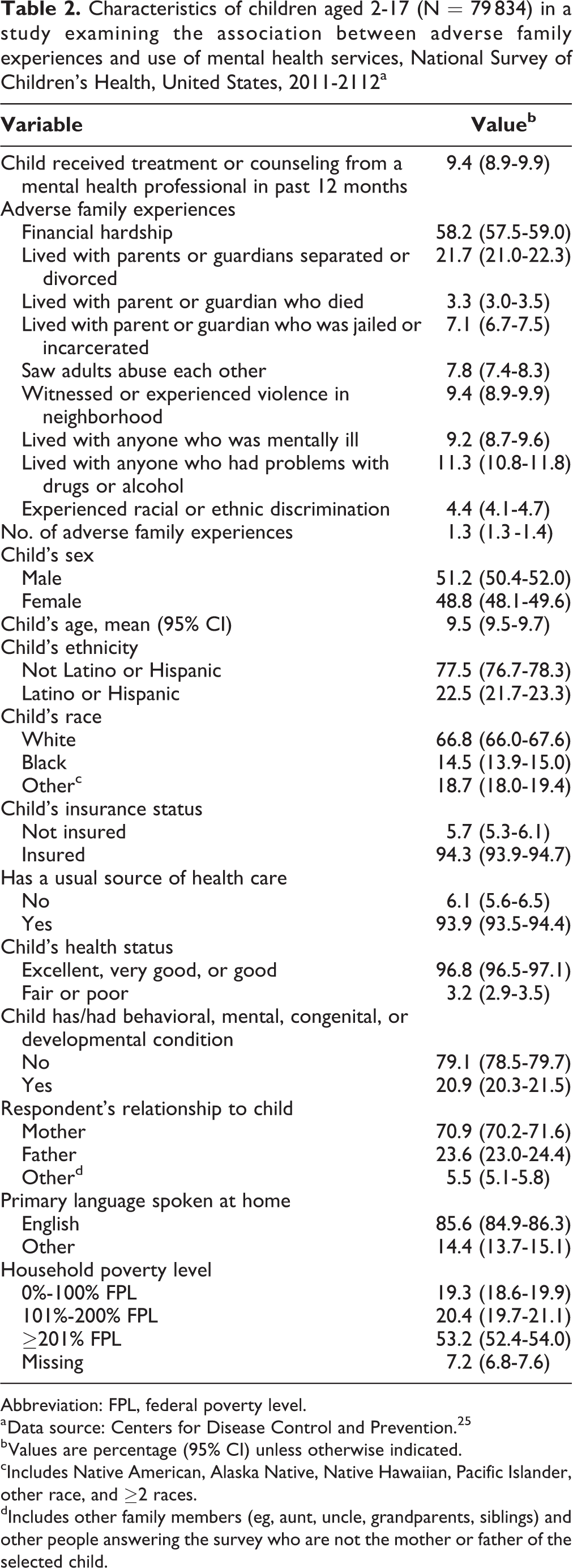
Abbreviation: FPL, federal poverty level.
a Data source: Centers for Disease Control and Prevention. 25
b Values are percentage (95% CI) unless otherwise indicated.
cIncludes Native American, Alaska Native, Native Hawaiian, Pacific Islander, other race, and ≥2 races.
dIncludes other family members (eg, aunt, uncle, grandparents, siblings) and other people answering the survey who are not the mother or father of the selected child.
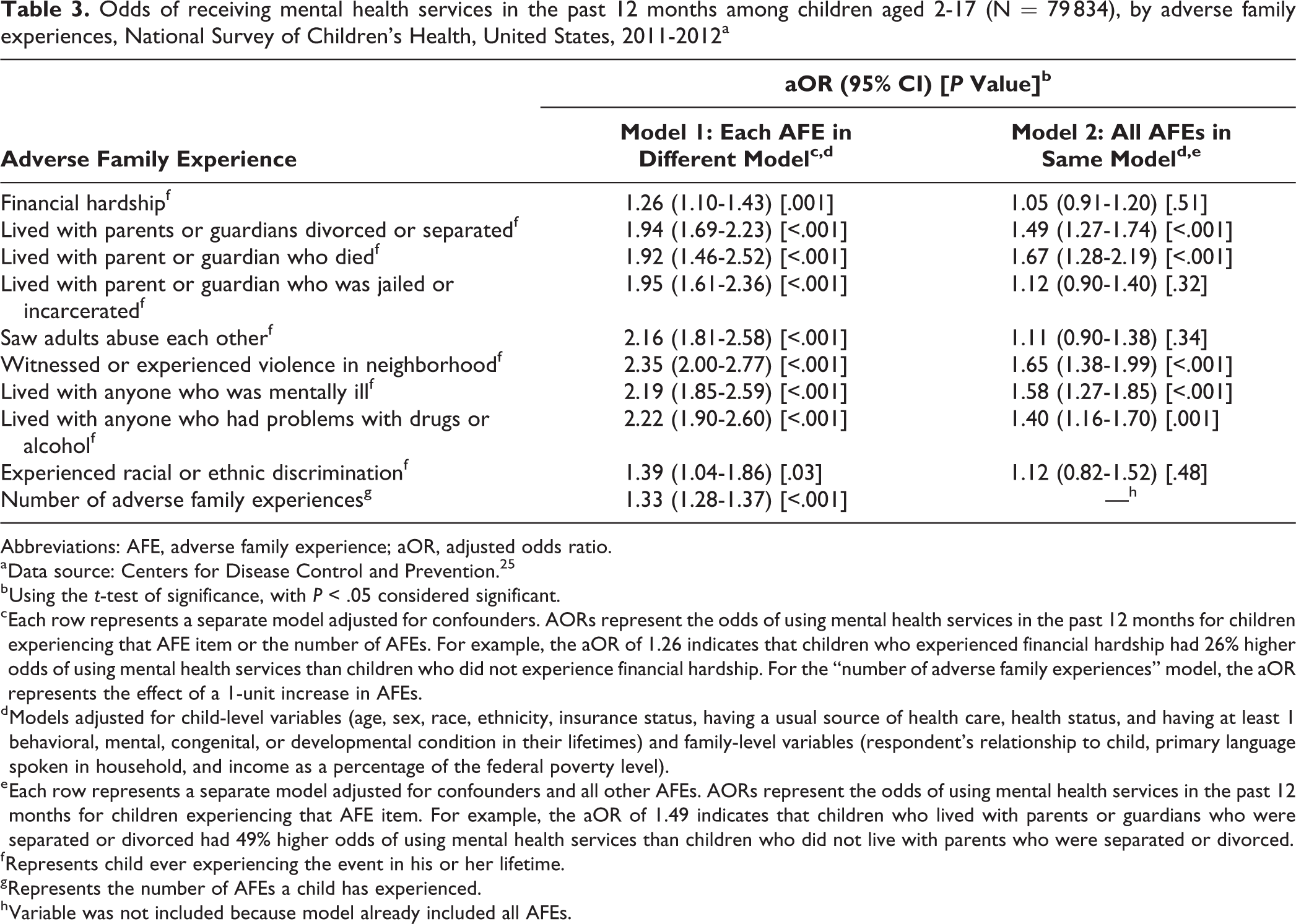
All AFEs were associated with increased odds of using mental health services (Table 3). Witnessing or experiencing neighborhood violence was associated with the greatest increase in adjusted odds of using mental health services (aOR = 2.35; 95% CI, 2.00-2.77). When measured continuously, each additional AFE was associated with 33% higher odds of using mental health services (aOR = 1.33; 95% CI, 1.28-1.37).
Odds of receiving mental health services in the past 12 months among children aged 2-17 (N = 79 834), by adverse family experiences, National Survey of Children’s Health, United States, 2011-2012a
Abbreviations: AFE, adverse family experience; aOR, adjusted odds ratio.
a Data source: Centers for Disease Control and Prevention. 25
b Using the t-test of significance, with P < .05 considered significant.
c Each row represents a separate model adjusted for confounders. AORs represent the odds of using mental health services in the past 12 months for children experiencing that AFE item or the number of AFEs. For example, the aOR of 1.26 indicates that children who experienced financial hardship had 26% higher odds of using mental health services than children who did not experience financial hardship. For the “number of adverse family experiences” model, the aOR represents the effect of a 1-unit increase in AFEs.
d Models adjusted for child-level variables (age, sex, race, ethnicity, insurance status, having a usual source of health care, health status, and having at least 1 behavioral, mental, congenital, or developmental condition in their lifetimes) and family-level variables (respondent’s relationship to child, primary language spoken in household, and income as a percentage of the federal poverty level).
e Each row represents a separate model adjusted for confounders and all other AFEs. AORs represent the odds of using mental health services in the past 12 months for children experiencing that AFE item. For example, the aOR of 1.49 indicates that children who lived with parents or guardians who were separated or divorced had 49% higher odds of using mental health services than children who did not live with parents who were separated or divorced.
f Represents child ever experiencing the event in his or her lifetime.
g Represents the number of AFEs a child has experienced.
h Variable was not included because model already included all AFEs.
In the model in which all AFEs were simultaneously introduced as independent variables, not all AFEs were associated with increased odds of using mental health services (Table 3). In particular, living with parents or guardians who were separated or divorced (aOR = 1.49; 95% CI, 1.27-1.74), having lived with a parent or guardian who died (aOR = 1.67; 95% CI, 1.28-2.19), having witnessed or experienced neighborhood violence (aOR = 1.65; 95% CI, 1.38-1.99), living with someone who was mentally ill (aOR = 1.58; 95% CI, 1.27-1.85), and living with someone who had problems with drugs or alcohol (aOR = 1.40; 95% CI, 1.16-1.70) were associated with higher odds of using mental health services.
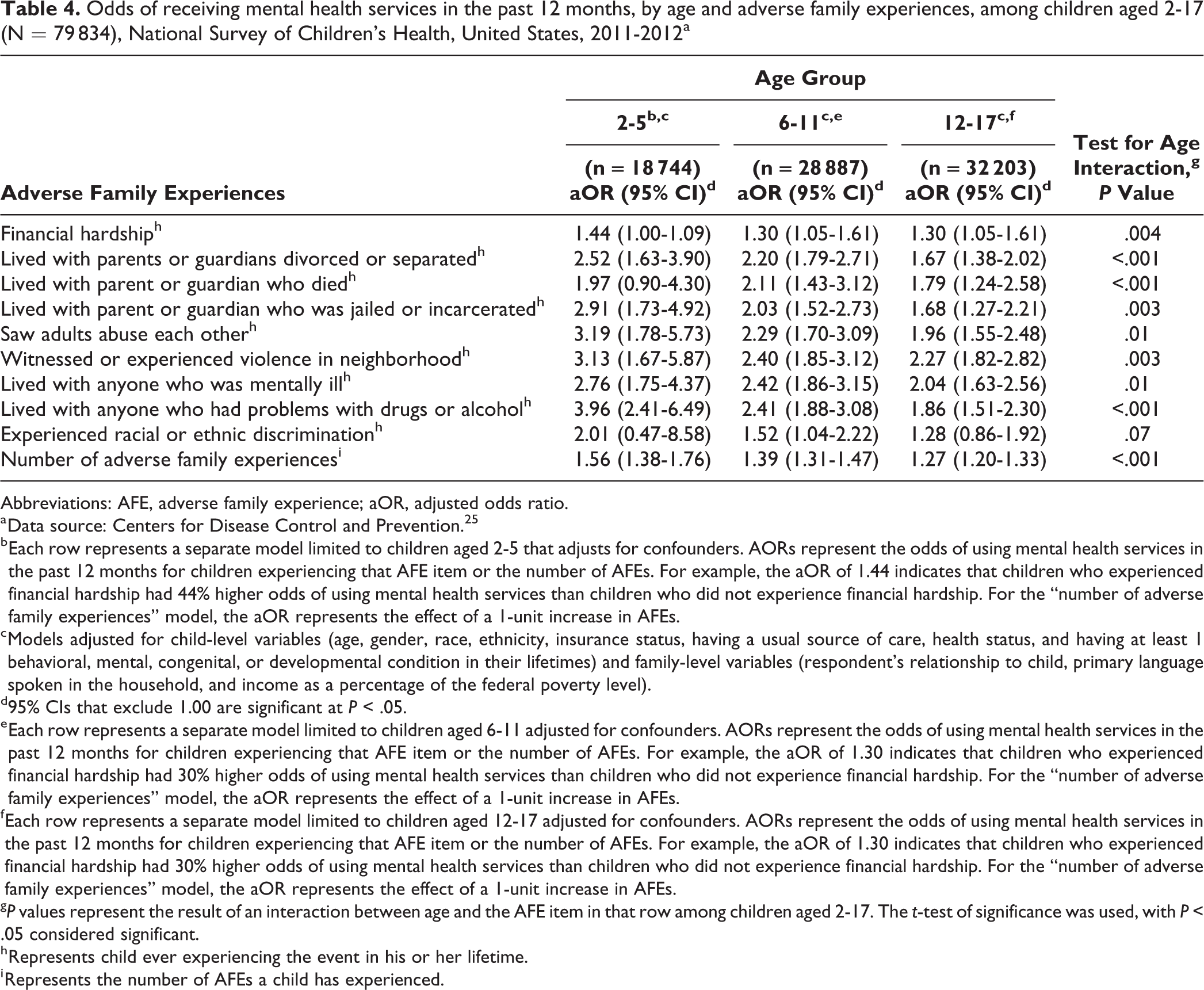
With the exception of experiencing racial or ethnic discrimination, the effect of all AFE items varied significantly by age (Table 4). In stratified analyses, the strength of the association between AFE items and use of mental health services was strongest among the youngest age group and tended to decrease with increasing age. This relationship was also true for the continuous measure of AFEs (P < .001).
Odds of receiving mental health services in the past 12 months, by age and adverse family experiences, among children aged 2-17 (N = 79 834), National Survey of Children’s Health, United States, 2011-2012a
Abbreviations: AFE, adverse family experience; aOR, adjusted odds ratio.
a Data source: Centers for Disease Control and Prevention. 25
b Each row represents a separate model limited to children aged 2-5 that adjusts for confounders. AORs represent the odds of using mental health services in the past 12 months for children experiencing that AFE item or the number of AFEs. For example, the aOR of 1.44 indicates that children who experienced financial hardship had 44% higher odds of using mental health services than children who did not experience financial hardship. For the “number of adverse family experiences” model, the aOR represents the effect of a 1-unit increase in AFEs.
c Models adjusted for child-level variables (age, gender, race, ethnicity, insurance status, having a usual source of care, health status, and having at least 1 behavioral, mental, congenital, or developmental condition in their lifetimes) and family-level variables (respondent’s relationship to child, primary language spoken in the household, and income as a percentage of the federal poverty level).
d95% CIs that exclude 1.00 are significant at P < .05.
e Each row represents a separate model limited to children aged 6-11 adjusted for confounders. AORs represent the odds of using mental health services in the past 12 months for children experiencing that AFE item or the number of AFEs. For example, the aOR of 1.30 indicates that children who experienced financial hardship had 30% higher odds of using mental health services than children who did not experience financial hardship. For the “number of adverse family experiences” model, the aOR represents the effect of a 1-unit increase in AFEs.
f Each row represents a separate model limited to children aged 12-17 adjusted for confounders. AORs represent the odds of using mental health services in the past 12 months for children experiencing that AFE item or the number of AFEs. For example, the aOR of 1.30 indicates that children who experienced financial hardship had 30% higher odds of using mental health services than children who did not experience financial hardship. For the “number of adverse family experiences” model, the aOR represents the effect of a 1-unit increase in AFEs.
g P values represent the result of an interaction between age and the AFE item in that row among children aged 2-17. The t-test of significance was used, with P < .05 considered significant.
h Represents child ever experiencing the event in his or her lifetime.
i Represents the number of AFEs a child has experienced.
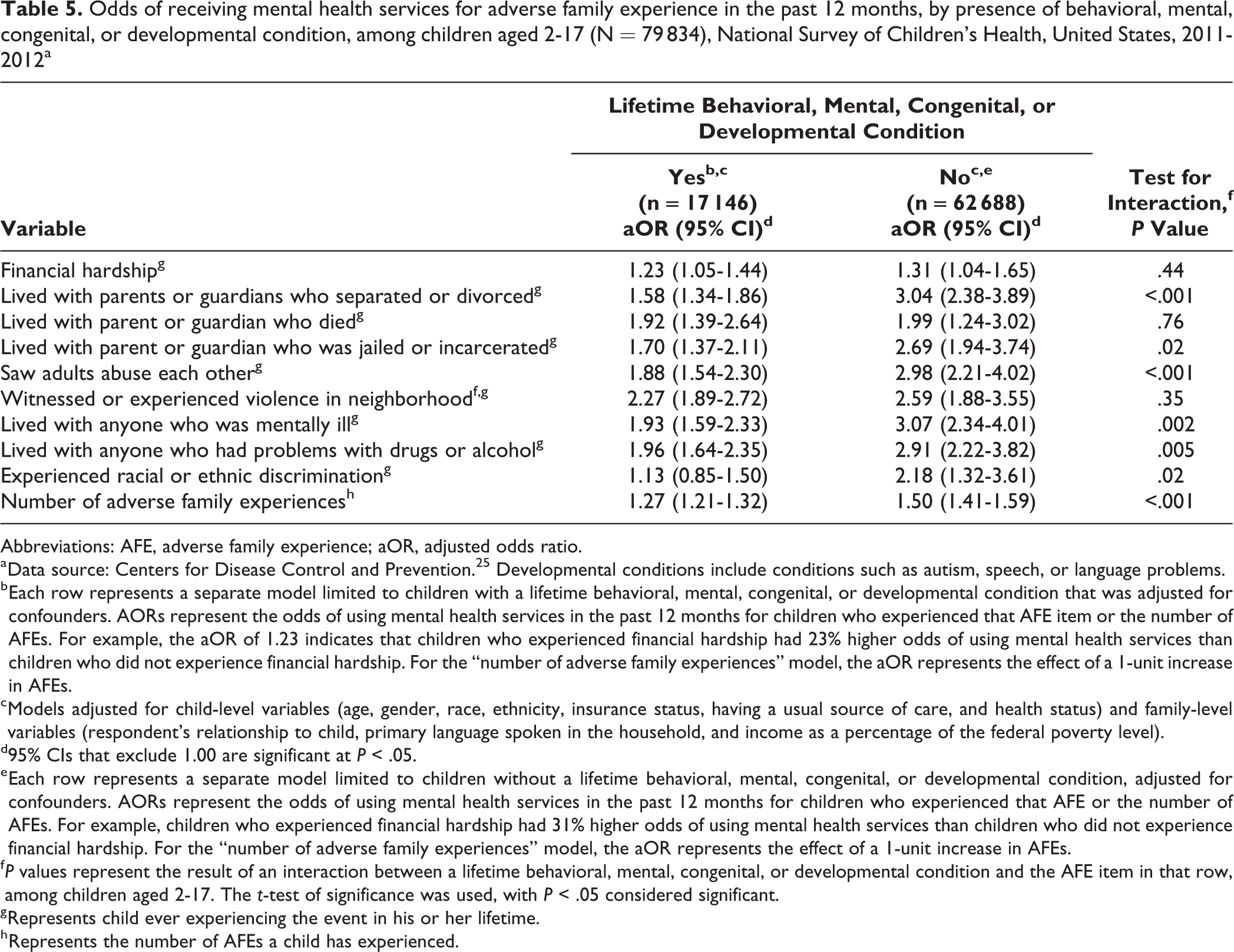
With the exception of financial hardship, living with a parent or guardian who died, and witnessing or experiencing neighborhood violence, the impact of all AFE items varied significantly by diagnosed behavioral, mental, congenital, or developmental condition (Table 5). In stratified analyses, the strength of the association between AFE items and use of mental health services was strongest among children who did not have a behavioral, mental, congenital, or developmental condition. This relationship was also true for the continuous measure of AFEs (P < .001).
Odds of receiving mental health services for adverse family experience in the past 12 months, by presence of behavioral, mental, congenital, or developmental condition, among children aged 2-17 (N = 79 834), National Survey of Children’s Health, United States, 2011-2012a
Abbreviations: AFE, adverse family experience; aOR, adjusted odds ratio.
a Data source: Centers for Disease Control and Prevention. 25 Developmental conditions include conditions such as autism, speech, or language problems.
b Each row represents a separate model limited to children with a lifetime behavioral, mental, congenital, or developmental condition that was adjusted for confounders. AORs represent the odds of using mental health services in the past 12 months for children who experienced that AFE item or the number of AFEs. For example, the aOR of 1.23 indicates that children who experienced financial hardship had 23% higher odds of using mental health services than children who did not experience financial hardship. For the “number of adverse family experiences” model, the aOR represents the effect of a 1-unit increase in AFEs.
c Models adjusted for child-level variables (age, gender, race, ethnicity, insurance status, having a usual source of care, and health status) and family-level variables (respondent’s relationship to child, primary language spoken in the household, and income as a percentage of the federal poverty level).
d95% CIs that exclude 1.00 are significant at P < .05.
e Each row represents a separate model limited to children without a lifetime behavioral, mental, congenital, or developmental condition, adjusted for confounders. AORs represent the odds of using mental health services in the past 12 months for children who experienced that AFE or the number of AFEs. For example, children who experienced financial hardship had 31% higher odds of using mental health services than children who did not experience financial hardship. For the “number of adverse family experiences” model, the aOR represents the effect of a 1-unit increase in AFEs.
f P values represent the result of an interaction between a lifetime behavioral, mental, congenital, or developmental condition and the AFE item in that row, among children aged 2-17. The t-test of significance was used, with P < .05 considered significant.
g Represents child ever experiencing the event in his or her lifetime.
h Represents the number of AFEs a child has experienced.
Discussion
Our results showed that all AFEs were associated with increased odds of using mental health services in the past 12 months. To our knowledge, our study is the first to examine the association between a wide array of childhood adversities and use of mental health services among children. These results are promising considering the elevated mental health risk among children with a history of childhood adversity. Thus, our findings suggest that children are receiving needed care. A review of studies published in 2016 showed that adults who experienced adversity as children and received mental health treatment as adults had improvements in various outcomes, including depression, posttraumatic stress disorder, dissociation, sleep, substance use, risky sexual behavior, interpersonal functioning, emotional regulation, and quality of life. 31 The effect of receiving therapy during childhood may be better than the effect of receiving therapy later in life because it can help prevent the development of more serious mental illness and manage chronic mental illness in its early stages.
We found that all AFEs were associated with increased odds of using mental health services. However, because associations persisted even after accounting for health status and presence of behavioral, mental, congenital, or developmental conditions, children who experienced AFEs may still have a greater need for these services for other reasons, as compared with children who did not experience AFEs. This need may be fueled, for example, by worse symptom severity, poorer management of symptoms, or presence of another underlying condition. Experiencing ACEs is prospectively associated with higher scores on continuous measures of depression among young adults, suggesting greater symptom severity among young adults with a history of ACEs compared with young adults without a history of ACEs. 32 Furthermore, adherence to antipsychotic medication is poorer among adults with a history of child physical abuse and adults who witnessed violence as children compared with adults who did not experience physical abuse or witness violence as children, 33 suggesting that these experiences make mental illness harder to manage. However, these associations need to be examined among children. 34
Our findings also highlight that AFEs have unique and cumulative effects on the use of mental health services. The strength of association varied by AFE. For example, neighborhood violence had the strongest association with use of mental health services. Although the relative effect of this finding has not been examined, this AFE was the only one we examined that might directly result in the child being taken to receive medical treatment as a result of injuries, which may make it easier to receive care for mental health problems stemming from the experience.
The number of AFEs also increased the odds of using mental health services. As such, there appear to be both individual and cumulative effects of AFEs. This finding is important because research has focused on examining ACEs and AFEs as cumulative exposures, thus obscuring important differences. Our study showed that the effect of AFEs differed by AFE, suggesting that treating these items as a cumulative scale may obscure the effect of individual AFEs. The importance of examining AFE items individually is particularly evident when all AFEs were included in the same model and only some AFEs were associated with the use of mental health services, potentially stemming from the co-occurrence of AFEs. Future research should consider whether these items should be summed into a scale for the outcome in question.
Our study findings also inform the larger literature that examines health across the life course. At least 2 competing views of how risk affects health across the life span exist: (1) the accumulation model, in which the total or sum of exposure to risk factors is important for health, and (2) the critical period model, in which the timing of exposure to risk factors is important for health. 35,36 Although these perspectives are typically used to examine health outcomes, our study suggests that risk (ie, AFEs) has both cumulative effects and a greater negative effect at certain points in childhood (ie, early childhood). However, because we could not determine when an AFE event occurred relative to the reported use of mental health services, additional research is needed to determine what is driving this association. Also, the greater the number of AFEs, regardless of age, the greater the use of mental health services, likely reflecting the greater burden of these additional experiences. However, to disentangle how these experiences develop during the course of childhood, longitudinal data are needed.
Finally, because associations between AFEs and mental health service use were strongest among children lacking behavioral, mental, congenital, or developmental conditions, having a condition that already requires mental health services may lead to better response to stressors, such as AFEs, and a diminished need for services in response to stressors.
Limitations
This study had several limitations. First, because the data were cross-sectional, causality could not be established, and several biases could not be ruled out. For example, we did not know when a condition that potentially required the use of mental health services occurred relative to the ultimate use of services. Future research should examine the associations in this study by using a longitudinal study design. Second, because parents or guardians provided all responses on behalf of their children, biases in responses may have resulted in overestimation or underestimation. Parents reporting on behalf of their children may be ideal for toddlers but not for school-aged children (aged 4-17). Third, measures of mental health service use did not include important details, such as reason for use, type of provider used, or treatment received, thus limiting the ability to rule out important confounders. Relatedly, data on health insurance status did not include information on insurance type. As a result, differences in the observed associations could not be examined by insurance status, provider type, or reason for use. Fourth, the data on AFEs did not allow us to determine at which point in time the AFEs occurred. Therefore, examining AFEs across ages can provide a measure of lifetime exposure only and not a measure of current exposure. Fifth, the use of mental health care encompassed only the past 12 months, thereby limiting the ability to fully account for history of mental health care use. Finally, because measures of mental illness included in the NSCH did not capture data on symptom severity, medication usage, or adherence to treatment, we could not account for these factors as potential drivers of observed differences.
Conclusions
Because the findings of our study were based on a nationally representative and community-dwelling sample, results highlight a population-wide demand for mental health services for children with a history of AFEs. Given the long-term mental health consequences of adversity, medical and public health systems must place greater emphasis on providing treatment early and to children with the greatest adversity. Also, because the demand for mental health services among children with a history of AFEs is not accounted for by the presence of a condition that may necessitate these services, providers must be better equipped to handle patients with more severe or poorly managed disease. Efforts to address this need for mental health services may include screening patients who are receiving mental health treatment for a history of child adversity and delivery of care in a trauma-informed manner. 37 At a systems level, hospitals may wish to screen their patients for AFEs when they seek treatment or provide reminders to patients or parents to improve adherence to treatment. In this way, patient outcomes can be improved, and the costs associated with poorly managed disease can be reduced. Also, because the effect of AFEs was strongest for children without an existing need due to an underlying condition, we must consider the possibility of undiagnosed or subclinical problems among children that may affect how they experience or react to AFEs. For example, AFEs may make diagnosing conditions less likely because of differential use of health care, differential quality of care, or differential treatment by providers.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.