
Abstract
Violence is a leading source of morbidity and mortality in the United States. In this article, we suggest a public health framework for preventing community violence, intimate partner violence and sexual violence, and suicide as key forms of interpersonal and self-directed violence. These types of violence often co-occur and share common risk and protective factors. The gender, racial/ethnic, and age-related disparities in violence risk can be understood through an intersectionality framework that considers the multiple simultaneous identities of people at risk. Important opportunities for cross-cutting interventions exist, and intervention strategies should be examined for potential effectiveness on multiple forms of violence through rigorous evaluation. Existing evidence-based approaches should be taken to scale for maximum impact. By seeking to influence the policy and normative context of violence as much as individual behavior, public health can work with the education system, criminal justice system, and other sectors to address the public health burden of interpersonal violence and suicide.
Community violence, intimate partner violence, and sexual violence (collectively referred to as “interpersonal violence”) and suicide are among the most common and severe forms of violence, and they exact an enormous public health toll. 1 -7 Nearly 45 000 suicides and 19 362 homicides occurred in the United States in 2016. 2 That same year, homicide and suicide were leading causes of death in the United States for people aged <45. 1,2 An estimated 36% of US women have experienced nonfatal intimate partner violence in their lifetime, 8 and 21% of women have experienced an attempted or completed rape according to US surveillance data from 2015. 8 More than 2 million people were treated in an emergency department for health consequences of violence in 2015. 2
Key forms of interpersonal violence are distinguished by their context and the nature of the perpetrator–victim relationship. Community violence refers to violence that occurs between strangers, friends, or acquaintances, and it typically takes place outside of residential dwellings. It includes physical fighting and assault with or without the use of firearms and other weapons. Much of the most serious forms of violence among young people (also known as “youth violence”) are encompassed within community violence. 9 Intimate partner violence includes physical, sexual, or psychological harm, including stalking, caused by a current or former partner or spouse. 10 Sexual violence refers to sexual activity when consent is not obtained or not given freely. 11 In addition to forced penetration, often referred to as rape, sexual violence can include unwanted sexual contact or coerced sexual penetration. Because current or former intimate partners are primary perpetrators of sexual violence against women, 7 intimate partner violence and sexual violence are closely linked.
Self-directed violence includes suicide, defined as death caused by self-directed injurious behavior with the intent to die as a result of the behavior. 4 A suicide attempt is a nonfatal injurious act with intent to die and refers to intentional self-inflicted poisoning, injury, or other self-harm. 4
These forms of violence are closely intertwined. They often co-occur, 12,13 as exemplified by intimate partner homicide–suicide (ie, simultaneous fatalities to both members of a relationship dyad). 14 They also share numerous risk factors. 15,16 They are often most visible in their first peak risk period of adolescence and early adulthood, yet trajectories of violence often are rooted in far earlier life experiences, including childhood adversity and maltreatment, 17,18 making early prevention and response essential.
The public health toll of violence also comes from nonfatal experiences and witnessing these forms of violence, which can have substantial health and social consequences, such as poor physical and mental health, substance use, stunted academic achievement, and reductions in long-term earning potential. 19 -24
In this article, we outline the basic epidemiology of community violence, intimate partner violence and sexual violence, and suicide. Our article is organized around the 3 mutually reinforcing pillars of comprehensive violence prevention and response 25 : (1) using primary and secondary prevention to prevent violence and its recurrence, (2) identifying and supporting survivors to mitigate the health and social impact of violence after it has occurred, and (3) promoting equitable, accessible justice processes that hold offenders accountable.
To advance prevention, we propose a public health prevention framework that draws on key risk and protective factors and highlights opportunities for intervention. We further summarize the evidence on violence prevention programs and policies and suggest shared strategies and priorities to strengthen the survivor support and justice pillars of violence prevention and response. We focus on solutions that can address all 3 forms of violence simultaneously.
Epidemiology: Patterns of Violence Risk by Gender, Race/Ethnicity, and Age
Gender, race/ethnicity, and age distinguish key populations at risk for violence. These characteristics are best considered by using an intersectionality framework that examines multiple simultaneous factors and social identities that interactively influence risk. Intersectionality explicitly encourages a focus on oppression, structural inequality, and disparate power dynamics to understand and reduce health and social disparities. 26,27
Gender
Men are more likely to carry out lethal and nonlethal forms of interpersonal violence than women. 6,28,29 In 2008, homicide victimization rates per 100 000 population were approximately 4 times higher among men (8.5) than women (2.3). 28 Yet, for women, homicide is one of the top 5 leading causes of death. 30,31 Intimate partner violence is implicated in more than half of homicides perpetrated against women. 28,30,32 Women’s experiences of nonfatal intimate partner violence and sexual violence are distinct from men’s experiences in their severity, complexity, and health and social impact. 7,28,32 Gender differences also exist for suicide. In 2014, the age-adjusted suicide rate per 100 000 population for men (20.7) was more than 3 times that of women (5.8). The gender gap as measured by the ratio of male-to-female suicide rates narrowed from 1999 (4.5) to 2014 (3.6). 6 Women are more likely than men to attempt suicide, yet men’s methods are more lethal. In 2016, women were 20% more likely than men to be treated for a suicide attempt, yet men represent 86% of all suicide firearm victims. 2 From 2003 to 2006, firearms were used in 58% of men’s suicides and 31% of women’s suicides. 6 These data illustrate a need for sustained attention to suicide risk via gender-specific approaches.
Race/Ethnicity
Profound racial/ethnic disparities exist in rates of violence. Among non-Hispanic black males, homicide was the leading cause of death for those aged 15-34 and the leading cause of the loss of years of productive life in 2015. 2,3 Homicide was the second-leading cause of death for black women aged 15-24 in 2015, 30,31 and nonfatal interpersonal violence was most prevalent among women of color in 2010. 7 In 2016, suicide rates per 100 000 population were highest among non-Hispanic white people (17.0) and non-Hispanic American Indian/Alaska Native people (21.2). 2 Age–race–gender disparities in suicide trends have emerged for young people: suicide rates per 1 million population increased significantly between 1993-1997 and 2008-2012 for Hispanic and non-Hispanic black boys aged 5-11 (from 1.8 to 3.5) and decreased significantly for their Hispanic and non-Hispanic white peers (from 2.0 to 1.3). 33,34
Adolescents and Young Adults
Adolescents and young adults aged 15-24 have a disproportionately high incidence of all forms of violence; suicide and homicide are the second- and third-leading causes of death, respectively, in this age group. 1 Community violence is pervasive among young people. National surveillance of high school students conducted in 2017 found high rates of past-year physical fighting (17% among female students, 30% among male students) and past-month weapon carrying (24% among male students, 7% among female students). 29 Intimate partner violence and sexual violence are concentrated among young people; approximately 80% of women who experience penetrative sexual violence will experience it for the first time by age 25. Twenty-six percent of female victims first experience intimate partner violence before age 18 and 45% between 18 and 24 years of age. 8 In 2016, the US suicide rate per 100 000 population was highest among men aged >85 (48.0). Yet across all genders, the suicide rate accelerates during adolescence and young adulthood, from 2.1 among children aged 10-14, to 10.0 among teenagers aged 15-19, to >14.0 among adults aged 20-84. 2 Suicide rates per 100 000 population rose for young women aged 15-24, from 3.0 in 1999 to 4.6 in 2014. Suicide rates rose by 200% among teenaged girls aged 10-14, from 0.5 in 1999 to 1.5 in 2014. 6
A Public Health Framework for Violence Prevention
Public health draws on a sound understanding of the biological, social, and policy forces that affect health and safety to formulate both individual- and population-level interventions. Consistent with leading frameworks for violence prevention, 35 -37 we outline a public health framework (Figure) rooted in social epidemiology, 38 social ecology, 39 and a life-course developmental perspective 40 that considers developmental phases in understanding current behavior. This approach provides an understanding of the layers of influence across individual, interpersonal, community, and social/structural factors. Extending past frameworks that are specific to violence, we identify key intervention approaches at each level. We also provide examples of pathways by which higher-order forces influence individual-level risk. The framework is illustrative rather than comprehensive, with key risk determinants depicted at each level.
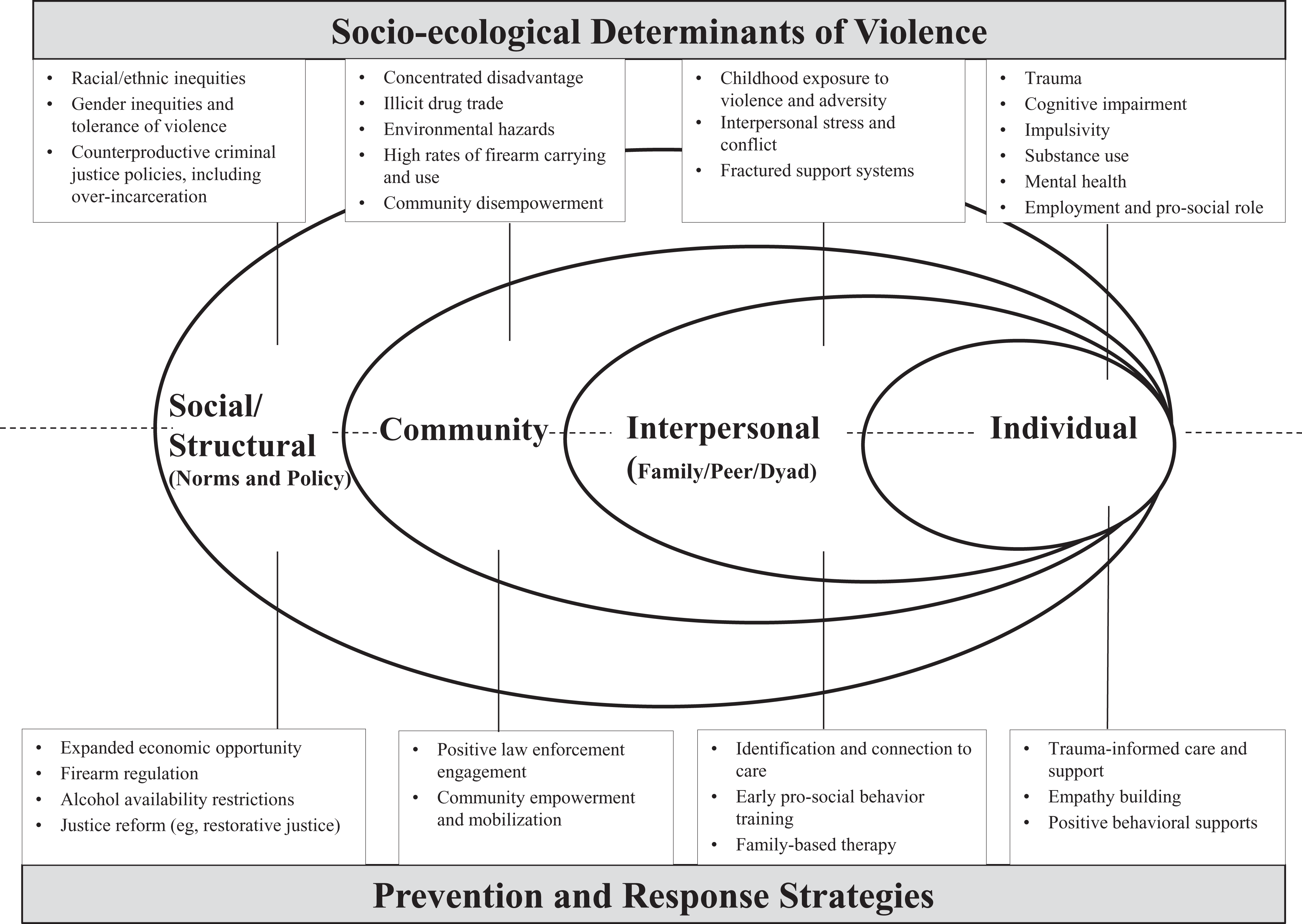
A socio-ecological framework for determinants of violence and strategies for prevention and response.
Three key points can be drawn from the framework. First, community violence, intimate partner violence and sexual violence, and intentional self-harm behaviors are complex, with multiple determinants and many shared risk factors across levels. 16,35,41,42 Second, shared factors protect against multiple forms of violence. 16 Third, individual-level factors are best understood when considered within the context of relationship, community, social norm, and policy factors. Levels of the framework are discussed hereinafter.
Individual Factors
Economic adversity is one shared individual-level risk factor 43 ; for example, unemployment can exacerbate stress and interpersonal conflict. 44 Poor mental health 44,45 and impulsivity 16 also increase the risk of violence, particularly for young people, in whom developmental factors affect important executive functions, including emotional control. 46 Alcohol and other substance use can increase the risk of violence, 44,47 -49 in part through enabling disinhibition and dampening executive function. Shared individual-level protective factors include social connectedness, coping, and problem-solving skills in nonviolent conflict resolution. 16 Employment and other pro-social roles that afford relative social status may also buffer against violence.
Relationships and Interpersonal Factors
Early relationship and family stressors such as child maltreatment, witnessing violence, and family dysfunction can set children on a difficult path early in life. 17,44,50 The so-called intergenerational transmission of violence, by which witnessing or experiencing violence in the family of origin enables subsequent victimization or perpetration, is thought to be mediated via such risk pathways as maladaptive brain development, substance use, and poor conflict-resolution role modeling, and it can be interrupted via resilience and relationship support. 44,51 Later in life, interpersonal stress, conflict, and disruption (eg, neighborhood violence and disorder) can enable violence, particularly in situations in which models for pro-social, effective communication and problem solving are lacking. 52 Intimate partner estrangement or separation is a uniquely risky period for intimate partner violence homicide. 53
Community Factors
Hazardous conditions, including concentrated social and economic disadvantage, high rates of male incarceration, tolerance and normalization of violence, low neighborhood collective efficacy (ie, a shared belief in the ability to effect change), and environmental threats such as lead exposure, enable multiple forms of violence through various mediating pathways. 44,54 -62 A vicious circle effect also exists; community violence enables individual violence 22,63 by inducing aggression and substance use. 22 Community redesign offers the potential for relief. For example, green spaces can reduce violence and enhance the perception of safety among community members. 64,65
Social Norms and Policies
Structural factors can create conditions that enable or prevent individual-level risk factors for violence. Harmful housing and urban development policies, such as the practice of redlining (ie, systematic denial of mortgage lending and economic development to communities, often based on race), have created inequity and poverty and, as a result, have supported conditions that foster violence. 66 Norms and practices that tolerate violence and gender-based inequity enable intimate partner violence. 67 In turn, policies that reduce inequity, address economic disadvantage, and establish strong norms of respect and equality across race and gender can reduce the risk of violence. 66,67
Prevention Approaches
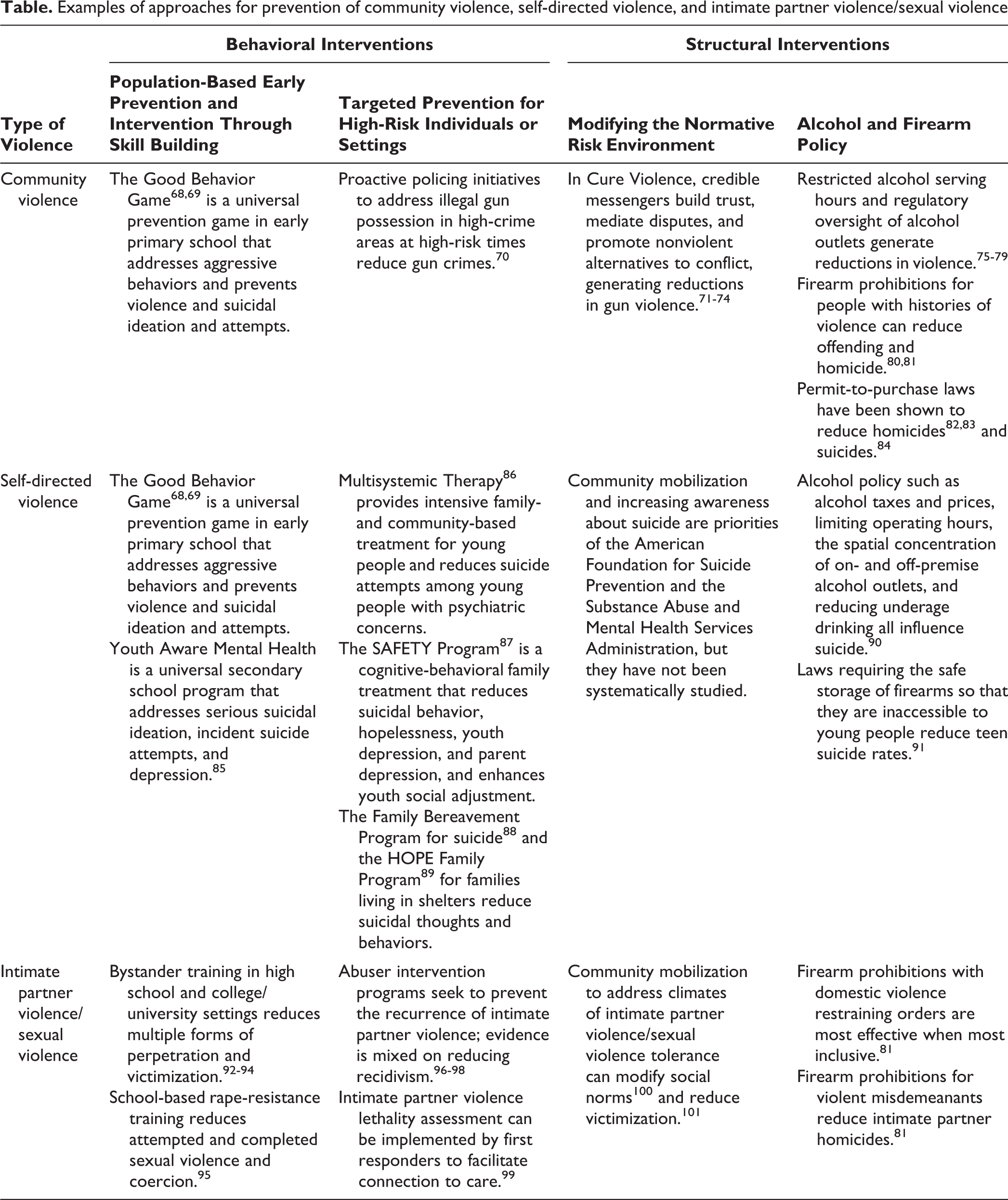
Several prevention approaches are effective for at least one form of violence and may be effective across multiple forms of violence. To explicate the strategies presented by level of the socio-ecological framework in the Figure, we review prevention strategies by approach and type of violence (Table) and illustrate opportunities, and evidence where available, for cross-cutting impact.
Examples of approaches for prevention of community violence, self-directed violence, and intimate partner violence/sexual violence
Behavioral Interventions
Viewing violence as a behavior that can be prevented or deterred is the cornerstone of many prevention models.
Early, universal school- and community-based prevention
Early, developmentally appropriate prevention has the potential to reduce morbidity and mortality on a population level, particularly given the roots of violence in early childhood mistreatment and adversity. For example, home visiting and related social supports for new parents are associated with reductions in the risk of abuse and its antecedents. 102
Schools are an important setting for reaching large populations of young people for prevention. Programs such as the Good Behavior Game help students develop communication and problem-solving skills, emotional regulation, conflict resolution, help seeking, and coping skills. 68,69 The Good Behavior Game is a game that addresses violent behaviors, implemented in first- and second-grade classrooms, 103 with a cross-cutting effect on preventing suicide attempts and juvenile court and/or adult incarceration for violent behavior. 68,69 An education and skill-building suicide prevention curriculum, Youth Aware of Mental Health Program, was found to reduce suicide attempts and suicidal ideation in a large-scale trial. 85 Gatekeeper training entails training for professionals and laypeople, including teachers and counselors, to recognize and respond to people at risk for suicide. 104 This model may be valuable for preventing other forms of violence. 41
School-based intimate partner violence and sexual violence prevention emphasizes prosocial engagement, including bystander training. These trainings engage people to recognize and intervene in situations that may become violent. Bystander approaches for intimate partner violence and sexual violence were first introduced in college settings and are effective in reducing multiple forms of violence victimization and perpetration among high school students, 92 including those implemented through athletic programs. 94 School-based rape-resistance programming can reduce the risk for attempted and completed sexual violence and coercion. 95 Prevention programs must recognize that participants may include victims of intimate partner violence and sexual violence and provide a survivor-centered response that includes appropriate referrals to support services. Additional evidence-based interventions for violence prevention at the school or community level are available. 105
Targeted, intensive interventions for individuals or settings at highest risk for incident violence and recidivism
Targeted interventions focus on individuals at the highest risk for violence perpetration or victimization. For example, multisystemic therapy is a targeted intervention that provides intensive family- and community-based treatment for young people with delinquency and antisocial issues; it has been shown to positively influence a range of delinquency, interpersonal, and self-directed violence outcomes. 86,106
For intimate partner violence, an evidence-based lethality assessment has been developed to help people assess their risk for intimate partner violence homicide. 107 Implementation by first responders then facilitates connection to care. 99,108 Abuser intervention programs seek to prevent recurrence of intimate partner violence. Evidence on their effect is mixed and confounded by methodological challenges. 96 -98 Isolated abuser intervention programs often fail to address underlying co-occurring risk factors such as substance use 109,110 ; emergent evidence suggests that joint behavioral therapies that address intimate partner violence and substance use can extend benefits to victims of violence. 110 -112 A trauma-informed, group-based abuser prevention program was found to be effective in reducing men’s use of physical and psychological intimate partner violence among military veterans. 113
Other targeted approaches include the Family Bereavement Program for suicide, 88 which is a multicomponent program for parentally bereaved children and adolescents that targets depression, grief, externalizing behaviors, and surviving parent’s depression. The HOPE Family Program 92 for families living in shelters is a family-strengthening approach that includes family communication, family decision-making, parental leadership and supervision, and coping and problem solving for young people. Both programs reduced participants’ suicidal thoughts and behaviors. 88,89
Targeted interventions for community violence include proactive policing initiatives designed to deter crime in designated areas of high risk. In high-crime areas during high-risk times known as “hot spots,” directing officers to identify and arrest people who are illegally carrying firearms has been effective in reducing shootings. 70
Structural Interventions: Modifying the Risk Environment Through Policy and Norms Change
This public health framework also identifies opportunities for interventions at the structural level, focusing on policies and social norms that influence conditions that spur or prevent violence or increase its lethality.
Alcohol-related policy
Environmental change through alcohol-related policy has been effective in reducing violence. Local restrictions on the density and number of alcohol outlets in communities appear to reduce alcohol-related violence, including sexual violence. 114 Restrictions on alcohol serving hours 75 -78 and enhanced regulatory oversight of alcohol outlets have also been shown to reduce violence. 79 Alcohol taxes, although protective, 115 need to be substantial to achieve moderate protective effects. 90,116
Community mobilization for policy and norms change
Community mobilization empowers individuals and groups to facilitate change on shared goals by taking action. 117,118 This approach has addressed hazardous alcohol use and the policy and social climates that enable it; advocacy campaigns have led to enhanced oversight of alcohol sellers and increased enforcement of drunk-driving laws, thereby reducing assaults and injuries. 119
The Cure Violence model (cureviolence.org) addresses gun violence by engaging credible messengers from affected communities to build trust with those at highest risk, mediate disputes, promote nonviolent alternatives to conflict, and facilitate connections to social services and job opportunities. The program appears to have reduced gun violence in most neighborhoods where it has been implemented, 71 -74 and evidence suggests that it may promote norms that eschew the use of guns to settle disputes. 120,121 Community mobilization has been a longstanding approach to addressing the social norms that tolerate and perpetuate intimate partner violence and sexual violence; emergent evidence shows that this approach can be powerful in changing norms, 100 as well as violence victimization. 101
Firearm policy
Policies that affect the availability of firearms, especially to high-risk people, can reduce the risk of violence-related deaths. Extending firearm prohibitions to violent misdemeanants is a method of restricting firearm access that can reduce the risk of criminal offending 80 and reduce intimate partner homicides. 81 Removing legal restrictions on gun carrying in public places appears to increase violent crime, 122 including homicides. 123
Firearm prohibitions can accompany restraining orders related to domestic violence. Such prohibitions are likely to be most effective when they are most comprehensive and inclusive (eg, where firearms prohibitions are included in emergency protective orders and where relationships are not limited to marital partnerships). 81,124 Restricting access to firearms has reduced firearm suicide rates 125 and is a potent strategy for preventing suicide because more than half of all suicides in the United States are by firearm (roughly 23 000 in 2016). 2 Laws requiring the safe storage of firearms so that they are inaccessible to underage people reduce teen suicide rates. 91 Other methods of restricting access to means of suicide, including means-restriction counseling for parents (ie, to limit access to firearms for at-risk family members), 126 are likewise important for suicide prevention.
Firearm policies at the federal level and for many states have 2 fundamental weaknesses whose correction could result in substantial reductions in lethal violence: (1) standards for legal gun ownership and concealed carry in public are too low, often allowing people with a history of violence and young people aged <21 to possess handguns, and (2) systems of accountability that are intended to prevent the transfer of firearms to prohibited people are too weak. 127 Two vital components of effective accountability systems are comprehensive background checks that include private-party transfers and availability of adequate data for sellers to effectively screen gun purchasers. As of 2018, 19 states had legal requirements of this type, 9 of which required some form of permit to purchase by firearm purchasers, issued by law enforcement agencies. The other 10 states had implemented comprehensive background checks via point-of-sale background checks. Permit-to-purchase laws appear to reduce homicides 82,83,128 and suicides 84 ; however, point-of-sale comprehensive background check laws without permit requirements have not been shown to reduce firearm deaths. 128 -130 Mandatory waiting periods for handgun purchases are also linked to reductions in homicide and suicide rates. 131
Multilayered Interventions
Mutually reinforcing gains can be achieved through interventions that address multiple levels of the socio-ecological framework simultaneously, as exemplified by the US Air Force Suicide Prevention Program. 132 This leadership-supported, comprehensive, evidence-based intervention includes surveillance, prevention services, supportive social networks, and changes to norms and policies. The program’s cross-cutting impact is demonstrated by a 33% reduction in the relative risk of suicide for the 1997-2002 cohort exposed to service-wide program implementation compared with the 1990-1996 pre-exposure cohort. Suicide rates per 100 000 population ranged from 10.0 to 16.4 during 1990-1996 and from 5.6 to 12.1 during 1997-2002. 132
Supporting Survivors of Violence
The survivor support pillar of comprehensive violence prevention and response has traditionally been the domain of the health care sector, where identifying survivors of violence and mitigating the physical and mental health impact of violence have been a primary focus. Trauma-informed care, which recognizes and responds to trauma, promotes safety and healing, and provides opportunities for survivors of violence to regain a sense of control and empowerment, 133,134 is a valuable approach for working with individuals and communities with recent and historic exposure to violence. Cognitive behavior therapy (CBT), a therapy that teaches clients skills in modifying harmful thinking and behavior, 135 is one approach that can mitigate the mental health effect of multiple forms of violence. Randomized clinical trials evaluating CBT have found 50%-60% reductions in suicide reattempt rates among high-risk suicidal patients, 136,137 immediate and sustained reduction in posttraumatic stress disorder among those who have had childhood sexual abuse, 138 and decreased likelihood of interpersonal violence victimization among survivors of interpersonal trauma. 139 CBT principles have been used within comprehensive interventions for at-risk young people with resulting reductions in violent crime perpetration. 140
The health care sector is increasingly engaged in secondary violence prevention (ie, prevention of violence recurrence) to break the cycle of violence and reduce recidivism for violent injury and suicide attempts. Whereas some studies suggest that health care sector interventions can generate positive changes in injury and violent recidivism, most have not documented reductions in violence, and some studies have had insufficient statistical power. 141,142
Intimate partner violence–related screening in the health care sector has been recommended by professional organizations since the early 1990s; in 2013, the US Preventive Services Task Force recommended interpersonal violence–related screening and referral for care.143,144 Several trials show that provider-initiated screening, referral, and brief interventions can improve health and reduce revictimization, 143 -145 particularly when integrated into ongoing health care via home visiting models. 146 This approach enables survivors to access additional systems of care, including the community support programs that provide important assistance to victims, 147 -150 mitigate mental health impact, 149,151 and, in some cases, reduce risk for revictimization. 152 -154 Health sector referral functions in part by helping survivors overcome issues such as self-blame 155,156 and lack of knowledge 155 -157 that are barriers to seeking violence-related support services.
The health care sector is highly engaged in suicide prevention and response. Mental health–related assessment and care can reduce suicidal behaviors and suicide rates 158 and can efficiently identify at-risk young people. 159,160 For suicide attempters, survivor support can serve as a powerful secondary prevention strategy, as illustrated by the SAFETY program, which provides cognitive–behavioral family treatment for adolescent suicide attempters recruited from emergency departments, 87 with resulting reductions in hopelessness, youth and parental depression, subsequent suicidal behavior, and enhanced youth social adjustment. A systems approach based on multicomponent health services interventions has been effective in suicide prevention; suicides decrease with an increase in the number of implemented evidence-based mental health service recommendations. 161 The Zero Suicide Initiative in the United States is based on a comprehensive framework for systematic, clinical suicide prevention in behavioral health and health care systems with a focus on safety and error reduction in health care. It also provides a set of best practices and tools for health systems and providers. 162
A clear and actionable target for supporting survivors is systems strengthening and reform, which prepares first responders in law enforcement, education, and health systems to effectively connect victims with necessary health care, community-based violence support, and mental health services.
Justice
The justice pillar of comprehensive violence prevention and response is primarily supported by the criminal and civil justice systems responsible for holding offenders responsible for interpersonal violence. Although suicidal behaviors do not demand a justice response similar to community and intimate partner violence/sexual violence, law enforcement does play a role in prevention of, and response to, this form of violence as well because its officers often serve as first responders after suicidal behaviors. Moreover, risk of suicidal behavior is elevated after contact with police, during detention, and postrelease, 163,164 and the justice system can be considered an important setting in which to identify and assist those at high risk for suicide. 165
The criminal justice system can be better integrated with prevention and survivor support efforts. In some cases, it has fostered the conditions that create cycles of violence. Discriminatory practices (eg, overincarceration with its roots in racial profiling, mandatory minimum prison sentences, cash bail, and inadequate legal defense) fuel distrust in the formal justice system 166,167 and further the cycle of violence by undermining cooperation with law enforcement 168 and enabling familial disruption and adversity for young people. Bipartisan calls for criminal justice reform reflect the growing recognition that the current law enforcement approach has not yielded the intended results.
The justice response to intimate partner violence and sexual violence is undermined by persistent barriers to engagement with the justice sector, such as mistrust, concerns for minimization of violence, and fear of retribution or retraumatization. 169 -171 As a result, intimate partner violence and sexual violence are among the most underreported violent crimes, 172,173 even with provisions for sensitivity training for law enforcement and court systems and coordination of victim services in the 1994 Violence Against Women Act. 174 Programs and policies must continue to encourage self-determination, also known as autonomy, as a guiding principle for victim decision-making on engaging with law enforcement. To overcome victims’ fears of mistreatment or violence minimization, justice systems must take active steps to foster trust and promote and monitor law enforcement accessibility.
Restorative justice principles offer a means to align public health and criminal justice across forms of violence. Restorative justice emphasizes repairing the harm that results from violence and providing nonviolent means of conflict resolution; its dual goals include supporting victims and facilitating community and offender rehabilitation. 175,176 For community violence, restorative practices include focused deterrence to hold individuals and groups accountable for violence and incentivizing nonviolence, while offering services and supports to offenders who want alternatives to crime and violence. Some evidence exists for reductions in gun violence as a result of such practices. 177 Emerging restorative models for intimate partner violence and sexual violence involve methods such as supported face-to-face accountability sessions in which offenders take responsibility for harm, written acknowledgement of harm, and apology. 175,176,178 Restorative practices are increasingly seen in early, school-based prevention and response programs. 179 Although the evidence base is limited, promoting restorative practices early in the life course may build important skills in positive coping, emotional regulation, conflict management, and empathy that could influence prevention of all 3 forms of violence.
Strengthening the justice pillar of comprehensive violence prevention and response also requires implementing and monitoring policies and procedures that promote police officers’ professionalism and accountability to prevent police misconduct and abuse. For example, proactive policing initiatives must be monitored carefully to root out unconstitutional and unprofessional practices that harm people, increase disparities, and erode community trust in law enforcement. Recent evidence linking police violence against unarmed black citizens with adverse mental health outcomes among black citizens in the general population 180 reveals the widespread and detrimental public health impact of police violence.
Future Directions
The epidemiology of violence illustrates the urgency of addressing racial/ethnic- and gender-based inequities in risk of violence, the vital need to promote stable and nurturing environments in early childhood, 51 and the opportunity for intervening during the peak risk period of adolescence and young adulthood. By understanding and tracking the connections among forms of violence, public health leaders can develop and implement strategies to reduce common risk factors and promote common protective factors. 15 Effective use of data and careful evaluation and attention to implementation of such strategies will be essential to success.
Strategies that simultaneously address multiple forms of violence hold the promise of efficiency and cross-cutting impact. Strategies that demonstrate evidence of reductions in violence outcomes, particularly those addressing early childhood adversity as a shared risk factor, 15 should be widely implemented and taken to scale. Large-scale implementation and dissemination must be accompanied by rigorous evaluation to enable ongoing learning. Monitoring and implementation science are also necessary, as exemplified by the compliance and enforcement issues that have hampered the implementation of firearm policy. 181 -184 Strategies that show promise for cross-cutting impact should be priorities for rigorous evaluation of effectiveness for multiple forms of violence.
Advancing violence prevention and response requires intervention strategies that address shared risk and protective factors and integrate factors across the full range of the socio-ecological framework to maximize impact. Structural interventions are in their earliest phases of development and represent an important area for future innovation. Intervention evaluation research too often focuses on outcomes of individual behavior without understanding the impact of intervention on a community’s normative and structural conditions. Advanced statistical methods are necessary to better understand causal pathways and effect mediators at the family, community, and policy levels of the socio-ecological framework, as well as of the mechanisms by which interventions exert their impact. Ecological, multilevel, and spatial analysis can clarify the geographic and social distribution of violent events 59,185,186 and identify the social and community conditions under which interventions and policies can be most effective.
Greater public health access to timely and complete data is essential. The National Violent Death Reporting System could be strengthened, for example, with data on legality of firearm possession for homicide suspects. Nearly all law enforcement agencies participate in the Federal Bureau of Investigation’s Uniform Crime Reports program; expanding this system to include nonfatal shootings and other serious injuries resulting from violent crimes would generate important advances in the study of violence and its prevention. The CDC WISQARS injury data visualization tool should identify intimate partner homicide; federal crime database reports should be more comprehensive, including providing data on same-sex relationships and former and casual dating as it relates to the victim–offender relationship for homicides. 124 Nonfatal suicide monitoring would be improved by adopting a comprehensive national or international system for documentation and standardization of nomenclature. 187 Data systems should link, wherever possible, past nonfatal outcomes with subsequent fatal outcomes.
As public health agencies and researchers become more involved in addressing violence, they should pursue deeper engagement with other sectors, including policing, housing, economic development, education, and social services. For example, engaging law enforcement in its role as a first responder can help connect victims to support services to aid in the response to community violence, intimate partner violence and sexual violence, and suicide alike. 99,188 Through collaborative efforts, communities can promote justice, address social inequities, and achieve measurable improvements in violence-related morbidity and mortality.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This article was produced with the support of the Bloomberg American Health Initiative, which is funded by a grant from the Bloomberg Philanthropies. It was also supported by the National Institute on Minority Health and Health Disparities, 1L60MD012089-01 to Charvonne N. Holliday.