
Abstract
Environmental quality has a profound effect on health and the burden of disease. In the United States, the environment-related burden of disease is increasingly dominated by chronic diseases. At the local level, public health practitioners realize that many policy decisions affecting environmental quality and health transcend the authorities of traditional health department programs. Healthy decisions about the built environment, including housing, transportation, and energy, require broad collaborative efforts. Environmental health professionals have an opportunity to address the shift in public health burden toward chronic diseases and play an important role in the design of healthy communities by bringing data and tools to decision makers. This article provides a guide for community leaders to consider the public health effects of decisions about the built environment. We present a conceptual framework that represents a shift from compartmentalized solutions toward an inclusive systems approach that encourages partnership across disciplines and sectors. We discuss practical tools to assist with environmental decision making, such as Health Impact Assessments, environmental public health tracking, and cumulative risk assessment. We also identify priorities in research, practice, and education to advance the role of public health in decision making to improve health, such as the Health Impact Assessment, as a core competency for environmental health practitioners. We encourage cross-disciplinary communication, research, and education that bring the fields of planning, transportation, and energy in closer collaboration with public health to jointly advance the systems approach to today’s environmental challenges.
Keywords
In the early part of the 20th century, public health agencies focused on eliminating major infectious diseases. Efforts to improve sanitation, treatment of drinking water, food inspections, and vector control led to major progress in health and the quality of the environment. 1 In the 1970s, major episodes of air and water pollution led to the establishment of the US Environmental Protection Agency (EPA) and the adoption of national laws focused on air, water, and soil pollution control and remediation. An unintended consequence of creation of the EPA was the disengagement of traditional public health agencies from environmental protection. 2
Now, the broad environmental and public health effects of air pollution, the built environment, and global climate change are becoming increasingly evident, 3 -6 and our understanding of the relationship between the environment and human health is evolving. Whereas environmental health once focused on infectious disease prevention, now the environmental health challenges have shifted toward the prevention of chronic disease. Cardiovascular disease is the leading cause of mortality in the United States. 7 Important risk factors for cardiovascular disease include environmental risks (eg, exposure to air pollution 8 ) and local built environment factors that discourage physical activity. 9 Reducing risks of chronic disease will require the reengagement of the public health community in environmental decision making. 10
Achieving a healthy environment will require a more holistic view than that behind current regulatory approaches. We must move beyond regulating smokestacks and discharge pipes toward an inclusive consideration of the role of the built environment in environmental quality and public health. The built environment is the human-made or modified structures where we live, work, and play, from the large scale of metropolitan areas to the small scale of individual buildings. It includes neighborhoods, roads, utility systems, and transportation systems. 11 In this article, we examine the relationship between the built environment and health and present a conceptual framework for building healthier communities.
The Relationship Between Environment and Health
The quality of the environment is a powerful determinant of human health. The World Health Organization (WHO) estimated that 22% of the total global burden of disease in 2012, including 12.6 million deaths each year, was due to environmental risks, including exposure to air pollution, chemicals, or radiation; inadequate water quality; and poor sanitation. 12 The effects on children are even greater; 26% of all deaths worldwide among children aged <5 in 2012 were attributable to environmental risks. 13
The environmental burden of disease is an estimate of the proportion of the global burden of disease that could be prevented by changes to the environment. The United States has the highest environmental burden of disease among comparably high-income countries. 14 Today, most diseases caused by environmental factors in the United States are highly prevalent chronic illnesses with broad effects on mortality and disability across all age groups. In 2012, the US burden of chronic disease attributable to environmental risks amounted to 8.8 million disability-adjusted life years, a measure of overall disease burden expressed as the number of life years lost to illness, disability, and early death. 15 These estimates are dominated by cardiovascular disease, neuropsychiatric disorders, cancer, asthma, and chronic obstructive pulmonary disease. 16 According to WHO, environmental risks related to these diseases include air, water, and soil pollution; ultraviolet and ionizing radiation; the built environment; electromagnetic fields; occupational risks; anthropogenic climate change; ecosystem degradation; noise; and not washing hands or contaminating food with unsafe water or dirty hands. These estimates do not include injury due to road traffic (responsible for an estimated 34 000 fatalities in the United States in 2013) 17 and other factors that can be influenced by the built environment.
Despite major improvements in air quality since the 1970s, air pollution is the largest environmental health risk in the United States. 18 Exposure to particulate matter air pollution was the sixth-leading risk factor for death in the United States in 2015, contributing to approximately 88 000 deaths per year. Ozone exposure contributes to an additional 9000 deaths per year. 19 These figures underestimate the full disease and quality-of-life effects of exposure to poor air quality. This underestimation is due to the fact that the recent estimates of the global burden of disease do not include the evolving research on cognitive, metabolic, and mental health outcomes associated with exposure to air pollution. 20
The built environment has an effect on many factors related to public health, including obesity, physical activity, 21 and mental health. 22 Air quality, which is associated with many health outcomes, is strongly influenced by the built environment. Car-centered development adopted since the 1950s required more roads, highways, and parking lots, leading to less green space, less availability of public transit or walkable/bikable transport, more traffic-related air pollution, and more injuries. Vehicles have a major effect on air quality, including a 17.5% contribution to fine particles (PM2.5) emissions in New York City. 23 Improvements in the built environment can result in substantial improvements to both ambient and indoor air quality. 24 The 1990 Clean Air Act Amendments brought about many policy changes relevant to the built environment, including vehicle emissions standards, promotion of low sulfur fuels for power generation, and energy conservation. These changes not only are cost effective but also greatly improve health: a prospective study of the Clean Air Act Amendments of 1990 found that their benefits will outweigh the costs of compliance by about 30:1 and will save 230 000 lives annually by 2020. 25 Furthermore, improvements to the built environment frequently are associated with other co-benefits, including reducing greenhouse gas emissions. 26
Environment-related disease has enormous economic effects. In 2008, the annual US cost of environment-related pediatric disease (including lead poisoning, asthma, childhood cancer, and neurobehavioral disorders) was estimated to be $76.6 billion, representing 3.5% of total health care costs. 27 State studies have shown similar effects on health care costs. 28,29
Not all populations are affected equally by environmental risks. A 2018 study found that population-weighted exposures to air pollution in Massachusetts were highest among urban non-Hispanic black populations and that the inequities, particularly for NO2 exposures in urban areas, increased from 2005 to 2010. 30 Nationally, population-weighted exposures of NO2 for nonwhite people were 4.6 parts per billion higher than for white people in 2006, and reducing the exposure levels of nonwhite people to the exposure levels of white people would save 7000 lives per year that are lost due to ischemic heart disease. 31 The environmental justice movement has increased the public’s awareness of the combination of increased exposures to environmental risks and social inequities that result in more disease related to such exposures in disadvantaged communities compared with wealthier, less exposed areas. 32 The increased environmental exposures faced by disadvantaged communities are due, in large part, to decisions made around the built environment, including industrial siting, roadway locations, and resulting traffic; pollution and toxic emissions; lack of accessible green space; and poor building and housing conditions. 33 Reducing the burden of environmental disease depends on identification of the most vulnerable populations and reducing disparities in exposure, disease outcomes, and disease prevalence.
The Public Health Approach
Today, the increasing proportion of disease burden caused by chronic diseases, coupled with a recognition of the role of the environment in these diseases, requires an inclusive, cross-sector approach to improving the built environment for healthier communities. The public health approach to solving environmental health problems is a stepwise process that includes: Defining the public health problem (identifying health risks of concern) Measuring the magnitude (understanding measures of disease or exposure in the population) Identifying key determinants of risk (including epidemiologic, social, and political factors) Developing and recommending policies (ways to reduce risk and promote health) Assessing health effects of policy options (eg, Health Impact Assessment [HIA]) Implementing and evaluating policy choices (tracking changes in community health)
34
This approach is built on epidemiologic evidence on health outcomes and risk; it integrates social considerations into policy recommendations and includes monitoring and health surveillance to evaluate policy impacts.
Numerous emerging tools and information resources are helping to advance the public health approach and offering new ways to inform environmental decision making. Some of these tools provide a new lens for examining the health implications of all policies (eg, the Health in All Policies 35 approach, a collaborative approach that incorporates health considerations into architecture, urban planning, transportation, energy systems, and all policy decisions). For example, an HIA uses a systems approach to integrate social, economic, environmental, and health data and stakeholder input and to characterize the potential health consequences of a proposed action or policy. 36,37 Leischow and Milstein 38 define the systems approach as “a paradigm or perspective that considers connections among different components, plans for the implications of their interaction, and requires transdisciplinary thinking as well as active engagement of those who have a stake in the outcome to govern the course of change.”
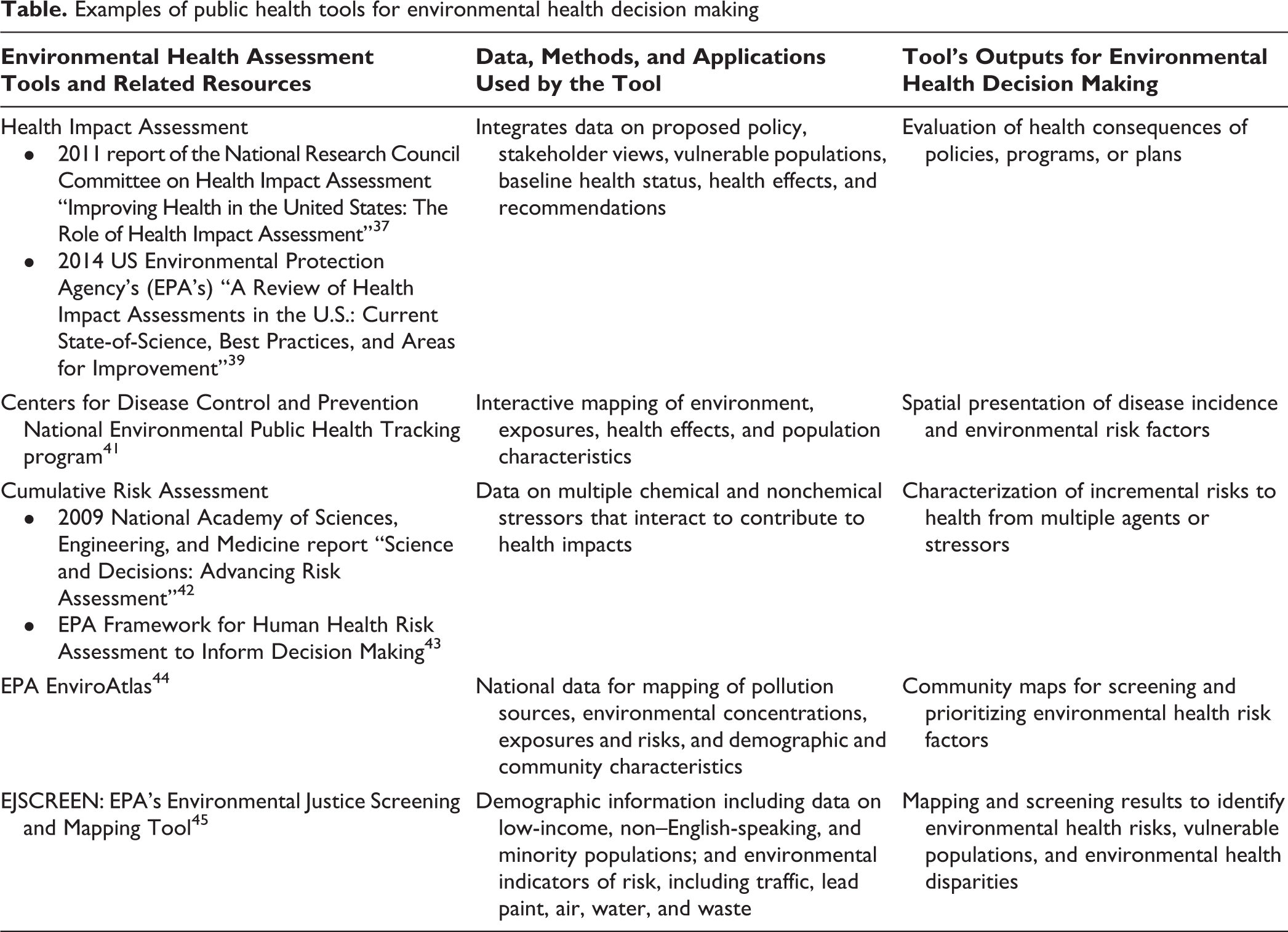
HIA complements other existing environmental health assessment processes, including environmental impact assessments. HIA is increasingly being applied by states, counties, local communities, and nongovernmental organizations throughout the United States to inform a range of decisions, including zoning, energy exploration, redevelopment, housing, industrial siting, mass transit, and road construction. 39,40 Other tools that support environmental health decision making include quantitative and qualitative risk assessment tools, mapping tools, and baseline data on environmental factors and health status (Table). These tools are useful not only for the design of new communities or cities but also for the redevelopment of existing neighborhoods or cities.
Examples of public health tools for environmental health decision making
A Framework for Healthy Communities
We propose a framework for building healthy communities that applies the aforementioned public health tools and approaches to strengthen the connections between public health and the built environment (Figure). The framework is adapted from WHO’s proposed road map for a global response to the health effects of air pollution. 46 Our framework is intended as a road map for reducing the adverse effects of the environment on communities. In the current state, it encourages cities to use baseline health and environmental risk factors to define challenges related to the built environment. The desired state presents public health and environmental goals for a healthy community. The framework includes needed public health tools and guidance and suggests cross-sector collaborators. It presents examples of health-informed practice (policies and investments) and identifies research and education needs. Finally, and most importantly, the approach includes ongoing health tracking and environmental monitoring activities (evaluation metrics) to evaluate the effect of improvements in the built environment and associated trends in the burden of environmental disease.
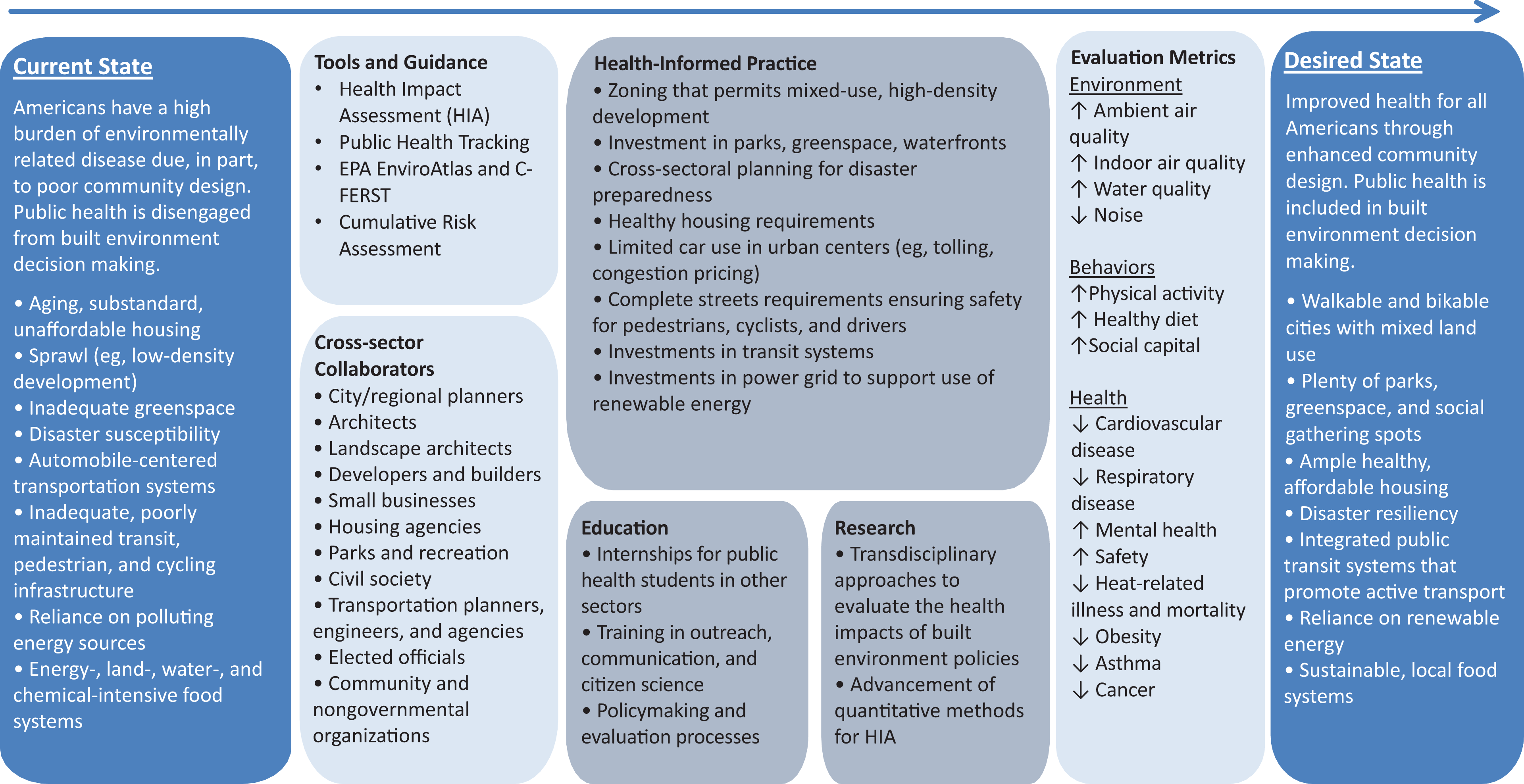
A framework for improving community health through better environment decision making. The current state presents baseline health and defines built environmental challenges. The desired state presents public health and environmental goals for a healthy community. The core components of the public health approach are shown indicating the path toward the desired state. Adapted from the World Health Organization. 46 Bulleted items may differ for various communities and applications. Abbreviations: EPA, US Environmental Protection Agency; C-FERST, Community-Focused Exposure and Risk Screening Tool.
Examples of Incorporating Health Into the Built Environment
The following are examples of improvement decisions in the built environment that affect health and quality of life and underscore the possibilities for broad stakeholder inclusion in community development decision making.
Urban Planning
Multisectoral planning can help cities address existing and anticipated environmental health threats. 47,48 Regions with urban sprawl have a higher carbon footprint, increased air pollution emissions, an increased reliance on cars, reduced ability to walk or bicycle, and decreased community cohesion compared with areas that have higher density development. 24 Oklahoma City provides an example of how cities can address these problems. With the participation of multiple city departments, the city government developed comprehensive development plans that include an HIA 49,50 to support urban infrastructure development ranging from increasing opportunities for walking and cycling, to providing access to healthy food, to building recreational facilities and improving the riverfront. The result has been an update of all zoning and planning codes, relocation of a major highway, creation of a large downtown park in a former industrial area, and development of trails to promote active recreation. 44 Such improvements can lead to more active lifestyles for residents, improved safety, strengthened community bonds, and improved air quality, 24 and they may have economic and climate benefits.
Housing
Substandard housing and homelessness are risk factors for poor health. 51 -53 Racial/ethnic and economic segregation is also associated with poor health outcomes for racial/ethnic minority groups. 54 Some housing authorities have combined healthy housing features, such as asthma-free housing and low-allergen housing. A leading example is the Mariposa Healthy Living Initiative, a 900-unit mixed-income development near downtown Denver. 55 In addition to healthy housing units, the Mariposa Healthy Living Initiative features “campaigns for action” that focus on social connectedness, physical activity promotion, healthy eating, health care access, and educational programs.
Green Space and Blue Space
Parks and green space offer a range of health benefits, some of which are direct (eg, stress reduction, improved birth outcomes) and some of which are indirect (eg, reduced crime rates 56 and reduced mortality during heat waves due to the urban heat island effect, which is the buildup of heat in urban areas compared with surrounding rural areas because of human activities 57 -59 ). The aesthetic appeal of water—coastal and riverfront areas sometimes called “blue space”— draws people to congregate, exercise, and relax near such areas. 60,61 Many cities are enhancing their green and blue spaces. For example, areas such as the Baltimore Inner Harbor and San Antonio River Walk feature broad walkways and have become centerpieces of each city’s economic development, its commercial and social life, and its tourist appeal. Targeted tree planting, focusing on areas with low tree coverage, 62 increases green space and may improve health through direct pathways (eg, trees filter out air pollutants, reduce the urban heat island effect) and indirect pathways (eg, aesthetic improvements that encourage walking and viewing vegetation for a restorative effect that improves mental health). 63
Public Transit, Walking, and Bicycling
Public transit ridership continues to grow in the United States; 10.5 billion public transportation trips were reported in 2015, an increase of 30% from 1995. 64 The greater Seattle area has invested in bus and light rail systems, resulting in a nearly 6% increase in ridership from 2016 to 2017, to a record 122 million riders in 2017. 65 Cities that make bicycling safe and convenient help promote this healthy and sustainable form of transportation while minimizing the risk of injuries. 66,67 Programs such as Safe Routes to School 68 encourage students to use active transport by ensuring that safe places are available for children to walk and bike. In a case study of 6 schools during a 3-year period (2007-2009), schools that implemented the Safe Routes to School program saw the percentage of students who walked or biked to school in the morning or afternoon roughly double from 8% to 16%. 69 Transit and cycling both reduce air pollution emissions and provide exercise opportunities, such as walking to and from transit stations or riding a bicycle. 70,71
Renewable Energy
Some towns have committed to being powered completely by renewable electric energy (excluding transportation). From 2008 to 2015, Aspen, Colorado; Burlington, Vermont; Greensburg, Kansas; and Rock Port, Missouri, achieved 100% renewable electricity sourcing, primarily in the form of wind and hydroelectric energy. 72 In 2008, Rock Port became the first US city to achieve this goal, and it now produces more electricity than it uses. A 2018 study found that if 17% of the electricity production in the eastern United States during summer 2006 were replaced with solar photovoltaics, PM2.5 would be cut by almost 5%, saving more than 1400 lives and $13 billion. 73
Recommendations for Practice, Research, and Education
Enabling public health practitioners to promote and support innovative collaborations for a healthy built environment will require changes to public health practice, research, and education. HIAs should be adopted as a core tool and competency for environmental health practitioners. HIAs should be increasingly quantitative, both in terms of health consequences and benefits and in terms of economic costs and benefits. Informed by these tools, public health officials must be prepared to engage with cross-agency, cross-sector, and community stakeholders from the early stages of problem formulation through evaluation of policy decisions. Accomplishing these goals will require (1) an examination of current organizational structure and support, (2) capacity building for managing information technology, and (3) cross-agency workforce training. Political and agency leaders at the federal, state, and local levels should reward cross-cutting solutions that encourage collaboration among officials from various sectors. Partnerships among researchers, public health practitioners, and public health associations should lead to the creation of technical assistance teams that can boost the capacity of practitioners, conduct HIAs, and integrate data on health with data on the environment. Finally, technological innovations should be adapted to promote public health. For example, emerging smart cities use digital technology and design to ensure that cities provide healthy living conditions, have infrastructure needed for high-quality jobs, and are sustainable (smartcitiescouncil.org). Similarly, expanded data, information, and communication tools (ie, Twitter, Facebook) will drive the evolving public health communication landscape.
Researchers should develop partnerships with communities across multiple disciplines, agencies, and sectors so that their research aligns with community needs. Cross-disciplinary research teams should aim to fill critical gaps in the data to assess the links between environment and health, improve the quantitative measures of HIAs, advance exposure science, identify vulnerable populations, and integrate social and behavioral influences on health risks. Research should document the economic effects of the built environment’s influence on health outcomes to provide a sound basis for balancing costs and benefits of improvements in the built environment. Researchers should integrate citizen science, whereby the public participates voluntarily in the scientific process to address real-world problems, into the evidence base (citizenscience.gov). Research should prioritize evaluation of citizen science tools that allow citizens to collect, analyze, and interpret data to ensure their quality and applicability, develop best practices for the use of these tools, and ensure comparability with current monitoring and surveillance programs. Systems-based research can provide an upstream perspective, moving from individual pollutants and pathways to integrated prevention strategies. Policy and implementation research should include longitudinal evaluation of the health effects of environmental policies.
With respect to education, discipline-based siloes in environmental health education must give way to cross-disciplinary skills and systems approach methodologies. Universities should support and incentivize the involvement of faculty, staff members, and students in practice, community engagement, and the local political environment. Environmental health programs should strengthen curricula and electives in disciplines relevant to upstream influences on health, such as planning, transportation, and energy, and develop interdisciplinary courses that link public health with aspects of the built environment. Similarly, public health content should be incorporated into planning and engineering training, as well as government and public policy training. Such training should include nontraditional approaches, including short courses, certificates, web-based learning, and online information resources to reach citizen scientists, businesses, agencies, and elected officials. Finally, communication should be a core competency for the training of future leaders, expanding beyond the peer-reviewed literature to emphasizing translation of science for diverse audiences and communicating uncertainty and risk.
This is a time of transition for environmental health. The changing global environment presents an opportunity and urgent need for public health leadership to move beyond traditional roles and reduce the burden of disease in the United States as we build healthy community environments.
Footnotes
Acknowledgments
The authors acknowledge the following people: Shelley Hearne, Big Cities Health Coalition; Jennifer Orme-Zavaleta, US Environmental Protection Agency (EPA); Gina Solomon, University of California, San Francisco; Clifford Mitchell, Maryland Department of Health; Jim Dwyer, Department of Transportation Port Administration; Emily Fisher, Johns Hopkins University (JHU); Jerry Taylor, Niskanen Center; Tim Whitehouse, Chesapeake Physicians for Social Responsibility; Suzanne Condon, Massachusetts Department of Health (retired); Jon Links, JHU; Keshia Pollack Porter, JHU; Dan Costa, EPA; Pat Breysse, Centers for Disease Control and Prevention; and Sarah Vogel, Environmental Defense Fund.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This article was produced with the support of the Bloomberg American Health Initiative, which is funded by a grant from the Bloomberg Philanthropies. Partial support for Koehler and Hobbs also provided by an Air Climate & Energy (ACE) Center Grant funded by US Environmental Protection Agency Assistance Agreement No. RD835871.