
Abstract
Objectives:
Little research has examined the long-term health consequences of gang affiliation among Mexican Americans. The objectives of this study were to (1) measure biological indicators of cardiovascular and metabolic risk, as well as prevalence of sexually transmitted infections (STIs), in a sample of Mexican American men aged 25-40 who were affiliated with gangs as adolescents and (2) compare those indicators with a comparable national sample of Latino men.
Methods:
Using bivariate analyses, we compared blood pressure, body mass index, 4 metabolic and cardiovascular indicators, and 4 infections for 179 Mexican American formerly gang-affiliated men in San Antonio, Texas, and 155 Mexican American men from the National Health and Nutrition Examination Survey. We used multivariate models to estimate adjusted risk scores for each sample controlling for age, marital status, and education.
Results:
Compared with men in the national sample, the unadjusted results showed that men in the gang-affiliated sample had significantly higher mean systolic blood pressure (125.6 vs 120.0 mm Hg, P = .001), diastolic blood pressure (81.4 vs 71.1 mm Hg, P < .001), and C-reactive protein (5.9 vs 3.6 mg/L, P = .04), and a significantly lower mean total cholesterol (164.2 vs 205.5 mg/dL, P < .001) and low-density lipoprotein cholesterol (91.1 vs 120.1 mg/dL, P < .001). Compared with men in the national sample, more men in the gang-affiliated sample had herpes simplex virus type 2 (64/174 [36.8%] vs 18/147 [12.2%], P < .001), chlamydia (10/176 [5.7%] vs 1/135 [0.7%], P = .02), and hepatitis C virus (85/173 [49.1%] vs 0, P < .001). The gang-affiliated sample had a significantly higher adjusted risk score than the national sample (1.5 vs 1.1, P = .003).
Conclusions:
Gang-affiliated Mexican American men had significant disparities in biological risk indicators and STIs, which can lead to long-term health implications and highlight the need for tailored prevention strategies. Long-term exposure to psychosocial stressors and subsequent systemic inflammation may also increase the risk for physiological and psychological dysregulation and detrimental chronic health conditions in this population.
Latino adolescents and young adults in low-income neighborhoods in the United States are disproportionately at risk for engaging in delinquency and crime-related gang activities. 1 Criminal justice data indicate that Latinos are overrepresented in gangs and may have a longer duration of gang membership than do those in other racial/ethnic minority groups. 1,2 Joining a gang typically occurs during early to mid-adolescence, and gang membership most often lasts no more than 1 or 2 years. 3 -5 However, the trajectories of those in gangs are heterogeneous, and a small subset of gang members maintain their affiliation for a much longer period of time. 4 The consequences of affiliation with a street gang, which include abusing drugs, dropping out of school, engaging in violence, and being involved with the criminal justice system, are well documented. 6,7 However, less is known about the cumulative, long-term physical health status of gang-affiliated men, especially those with prolonged gang affiliations.
Although Latinos in the United States have lower all-cause mortality rates than those of non-Latinos, Latinos do have higher mortality rates for particular causes of death, including homicide, diabetes, HIV, digestive cancers, 8 and cardiovascular disease. 9 People in the criminal justice system (including gang members) are often excluded from conventional school-based and household surveys because of residential mobility, stigma, incarceration, and/or homelessness. 10 For example, one study of adolescent gang members found that 55% had been expelled from school, 11 whereas another study found that black men who had been incarcerated had spent 13.4% of their working lives in prison 12 ; consequently, both of these groups were likely to be left out of survey sampling. These types of exclusions can affect the accuracy of population health statistics. For example, one study documented a 7% increase in overall sexually transmitted infection (STI) prevalence when the incarcerated population was included in population health statistics for black men. 13
To fully and accurately characterize the current health status of the broader non-immigrant Latino population, and to begin to document the long-term health consequences of gang membership, baseline objective health profiles of gang-affiliated Latino men, particularly in relation to the profiles of men in the general Latino population, are needed. This study provided a collection of objective health data for a sample of adult men who were initially recruited during adolescence into a longitudinal study on Mexican American street gangs. The objectives of our study were to (1) measure biological indicators of cardiovascular and metabolic risk, as well as prevalence of STIs, in this population and (2) compare them with data on a national household sample of Latino men. To our knowledge, this study is among the first to provide objective health information about this understudied, non-immigrant, gang-affiliated Latino population.
Methods
All research protocols were approved by the Institutional Review Board at the University of Southern California and by Executive Services at the Texas Department of Criminal Justice. For our study, we used the term “gang-affiliated men” to refer to young adult males with a history of adolescent gang involvement.
Gang-Affiliated Sample
We obtained sample data on gang-affiliated men from a 15-year longitudinal study of young adult Mexican American men in San Antonio, Texas. San Antonio has a population of more than 1.3 million people, more than half of whom are Latinos of Mexican origin. 14 The city ranks among the top 10 US cities with the largest numbers of people living in distressed ZIP codes (measured by low high school graduation rates, housing vacancy, adults not working, poverty rates, median income ratio, employment changes, and change in business establishments), and it has the highest level of economic spatial inequality (ie, unequal amount of economic qualities, resources, or services across geographic units within a country, city, or region) in the United States among its ZIP codes. 15
The men in the sample for the 15-year longitudinal study were recruited from San Antonio’s West Side, an area characterized by a high concentration of poverty, unemployment, criminality, drug trafficking, and Mexican American street gangs. 11,16,17 The men were originally identified and recruited in 1996 and 1997 as part of a study of adolescent gang members. At that time, the rosters of gang members were developed during one year by using gatekeepers, gang contacts, key informants, and field workers. All information about gang members was verified by a minimum of 3 of these sources. Subsequently, a multistage stratified design was applied to select a random sample of 160 men, representing 26 known Mexican American gangs in this urban area, from the rosters. A detailed description of the sampling design for the longitudinal study is available elsewhere. 17,18
From 2009 through 2012, we performed a follow-up study of the original men in the longitudinal study, locating 152 (95.0%) of the original 160 men. 17,18 Of those located, we enrolled 119 (78.3%) men, resulting in a final follow-up rate of 74.4%. We were also able to enroll 9 men who were incarcerated in the Bexar County Jail or the Texas Department of Criminal Justice in the follow-up study. Of the 33 men located but not enrolled in the follow-up study, 16 declined to participate, 6 were deceased, 2 were in federal prison, and 9 did not participate for unknown reasons. In addition, we recruited an additional 156 men from the original rosters, creating a final sample size of 275 men for the follow-up study.
Interviews for the follow-up study consisted of having the men complete standardized cross-sectional questionnaires and life history calendars. We had biological specimens collected from a representative subsample, which consisted of 179 men aged 25-40. We received funding for biological specimen collection after our study began, and the funding allowed only 179 men to be tested. No men refused to give a biological sample, although 8 men were unable to provide a sample because of collapsed veins or because they were incarcerated in Bexar County Jail, where blood samples could not be drawn. Blood and urine samples were tested by LabCorp, a nationally recognized laboratory company that provides medical testing and laboratory services. Trained phlebotomists performed all venipuncture procedures. Participants in the study were compensated $70.
Measures
We assessed indicators of cardiovascular and metabolic risk using biological data, collected as part of the follow-up study from the gang-affiliated men, that included anthropomorphic measurements as well as blood and urine test results. The anthropomorphic measurements included body mass index (BMI), which we calculated from measurements of height and weight (weight in kilograms divided by height in meters squared [kg/m2]), diastolic blood pressure (DBP), and systolic blood pressure (SBP).
We also assessed cardiovascular and metabolic risk by using data on lipid level indicators, including total, high-density lipoprotein (HDL), and low-density lipoprotein (LDL) cholesterol, which had been obtained from blood samples by using the enzymatic method (mg/dL). We used nonfasting blood because of difficulty in implementing fasting requirements, which could have potentially compromised recruiting efforts in this hard-to-reach population. We evaluated low-grade systemic inflammation by using C-reactive protein (CRP), a nonspecific biomarker that, when elevated, may suggest cardiovascular disease risk, inflammatory disease, infection, or injury. 19 We measured CRP (mg/L) by using an immunochemiluminometric assay that did not require fasting blood for an accurate measurement. 20
We assessed multiple indicators of infection. We determined herpes simplex virus type 2 infection status by using a type-specific immunoglobulin-G antibody blood test (HerpeSelect 2 ELISA IgG; Focus Technologies), with any index value >0.9 considered positive. We assessed hepatitis C virus (HCV) infection status with antibody assays of blood by using the Abbott HCV EIA 3.0 procedure for encoded antigens (recombinant c100-3, HC-31, and HC-34); when positive, it was confirmed by the hepatitis C recombinant immunoblot assay.
Screening for Neisseria gonorrhoeae (gonorrhea) and Chlamydia trachomatis (chlamydia) was performed with a polymerase chain reaction test technique for molecular detection of bacterial DNA, using 10 mL of urine. We tested for HIV infection by using enzyme-linked immunoassay for HIV antibody in blood; when positive, it was confirmed with a Western blot. Lastly, we assessed for the presence of opiate, cocaine, amphetamine, and marijuana metabolites with the 4 Panel Drug Test Strip urine test (Home Health Testing).
General Population Sample
We also obtained demographic (age, marital status, education), examination (blood pressure and BMI), and laboratory (total, HDL, and LDL cholesterol; CRP; HIV; HSV-2; HCV; chlamydia; and gonorrhea) data on a nationally representative sample of 155 Mexican American men aged 25-40 from the 2007-2008 National Health and Nutrition Examination Survey (NHANES), which we referred to as the general population sample. 21 NHANES assesses the health and nutritional status of adults and children in the United States through interviews and physical examinations. NHANES typically oversamples Mexican Americans to increase the reliability and precision of estimates of health status indicators for this population subgroup. Bilingual interviews and interpreters are provided to assist with the questionnaires, medical examinations, and collection of urine and fasting blood samples for laboratory analysis. Physical health indicators also included an average of 3 blood pressure measurements.
Analysis and Statistical Methods
We used established clinical thresholds 22 -24 for the biological indicators to identify high-risk cut points for cardiovascular and metabolic risk (Table 1). The standard CRP high-risk cut-off of 3.0 mg/L was used, 24 and the scale was changed to a multiple of 10. We constructed a risk summary scale of the 7 biological indicators, which included total cholesterol, LDL cholesterol, HDL cholesterol, CRP, BMI, DBP, and SBP, with a score that reflected the number of risk factors that were above the established clinical thresholds (range, 0-7). For both the gang-affiliated sample and the general population sample, we calculated means and standard deviations for each biological indicator and for the unadjusted summary scale scores. Because complete data were missing for a few men in the samples, we reported percentages with numerators and denominators rather than listwise deletion. We also calculated the relative risk between samples for these indicators and scores.
Clinical high-risk cut points for biological risk indicators used to evaluate Mexican American men aged 25-40 from a gang-affiliated sample in San Antonio, Texas (2009-2012), and a general population sample of Latino men from the National Health and Nutrition Examination Survey (2007-2008)a
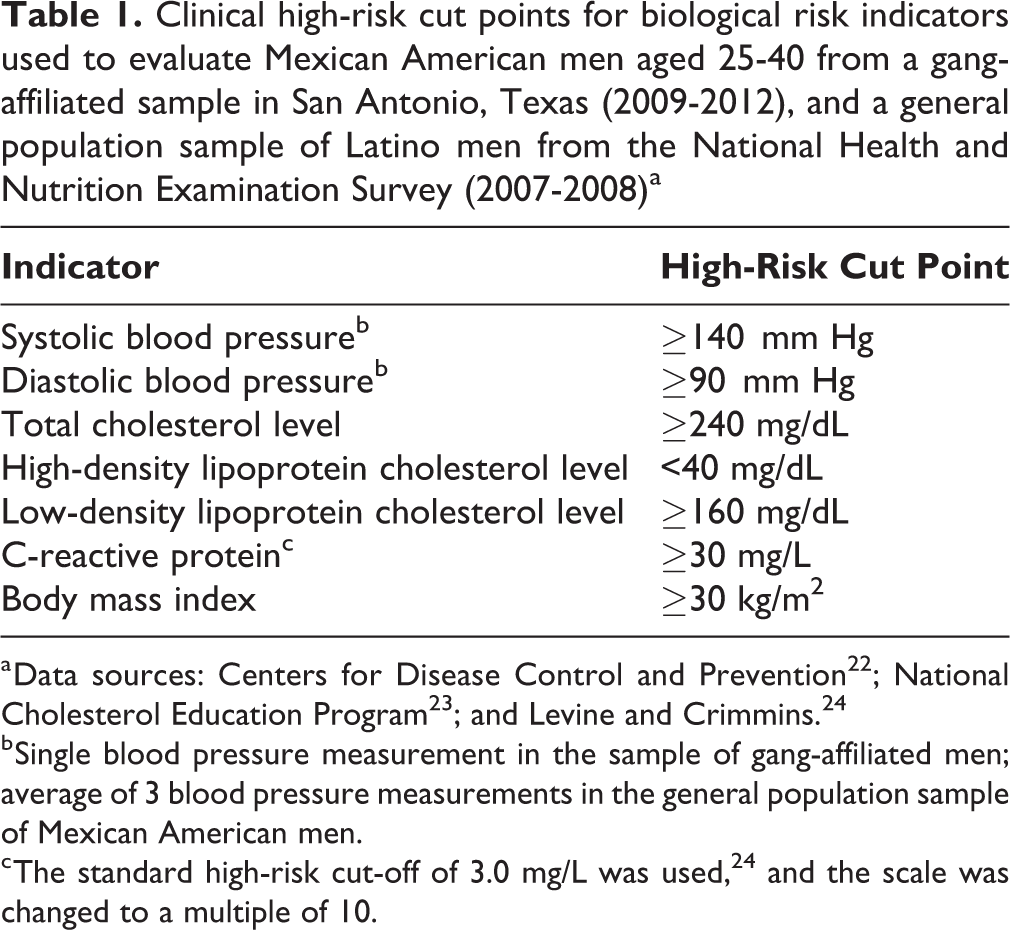
a Data sources: Centers for Disease Control and Prevention 22 ; National Cholesterol Education Program 23 ; and Levine and Crimmins. 24
b Single blood pressure measurement in the sample of gang-affiliated men; average of 3 blood pressure measurements in the general population sample of Mexican American men.
c The standard high-risk cut-off of 3.0 mg/L was used, 24 and the scale was changed to a multiple of 10.
We used paired t tests and Pearson χ2 tests to compare the means and prevalence of the biological indicators and risk summary scale scores of the gang-affiliated and general population groups. We estimated the adjusted risk of having high-risk biological indicators or scores for both the gang-affiliated and general population groups by using a negative binomial regression model with bootstrapped standard errors (SEs), controlling for age, education, and marital status. We used a postestimation command to estimate the predicted counts for each group based on the model, holding the control variables at their mean. We reported results as incidence risk ratios and provided β coefficients and SEs. We set significance at P < .05 for all comparisons, except for those pertaining to the risk summary scale scores, for which we defined it at P < .10. We performed all statistical analyses by using Stata release 14. 25
Results
A significantly smaller proportion of the 179 gang-affiliated men, compared with the sample of 155 men in the general population, were married (n = 66 [36.9%] vs n = 114 [73.6%], P < .001) or had a college degree (n = 0 vs n = 16 [10.3%], P < .001). Compared with the sample of men in the general population, the gang-affiliated sample was significantly younger (mean age, 31.7 vs 32.8, P = .01) and had a significantly lower proportion of men aged 35-40 (n = 36 [20.1%] vs n = 69 [44.5%], P < .001).
The gang-affiliated sample had low levels of education (mean, 9.4 y completed), a low proportion with health insurance (25/168, 14.9%), and a high proportion who were unemployed (96/179, 53.6%) or had at least 1 felony conviction (144/179, 80.4%). On average, these men reported not seeing a physician for the past 2.5 years (interquartile range, 0.17-6.42; median, 1.0). Their mean total time incarcerated was 5.3 years, and 81 of 179 (45.3%) men reported a current affiliation with an adult gang. On drug screening, of the 177 men in the gang-affiliated sample who were assessed, 80 (45.2%) tested positive for opiates, 88 (49.7%) for cocaine, 86 (48.6%) for marijuana, and 5 (2.8%) for methamphetamines. Although comparable indicators for the 155 men in the general population sample were not available, 12 (7.7%) reported any marijuana use, 6 (3.9%) reported any cocaine use, and none reported any heroin use, in the past 30 days.
Men in the gang-affiliated sample had significantly higher mean values for both SBP (125.6 vs 120.0 mm Hg, P = .001) and DBP (81.4 vs. 71.1 mm Hg, P < .001) compared with those in the general population sample (Table 2). The gang-affiliated sample of 179 men, compared with the general population sample of 155 men, had significantly higher proportions with high-risk values for SBP (n = 30 [16.8%] vs n = 9 [5.8%], P = .002) and DBP (n = 46 [25.7%] vs n = 4 [2.6%], P < .001) (Table 3). The relative risks of gang-affiliated men having SBP and DBP above the high-risk cut points were 2.9 and 10.0, respectively, indicating that those with a history of gang membership were 3 times more likely than those in the general population sample to have high SBP and 10 times more likely to have high DBP. Within the general population sample, 3 (1.9%) men used blood pressure medication, although the number of men in the gang-affiliated population who used blood pressure medication was unknown.
Biological risk indicators among Mexican American men aged 25-40 from a gang-affiliated sample in San Antonio, Texas (2009-2012), and a general population sample of Latino men from the National Health and Nutrition Examination Survey (2007-2008)a
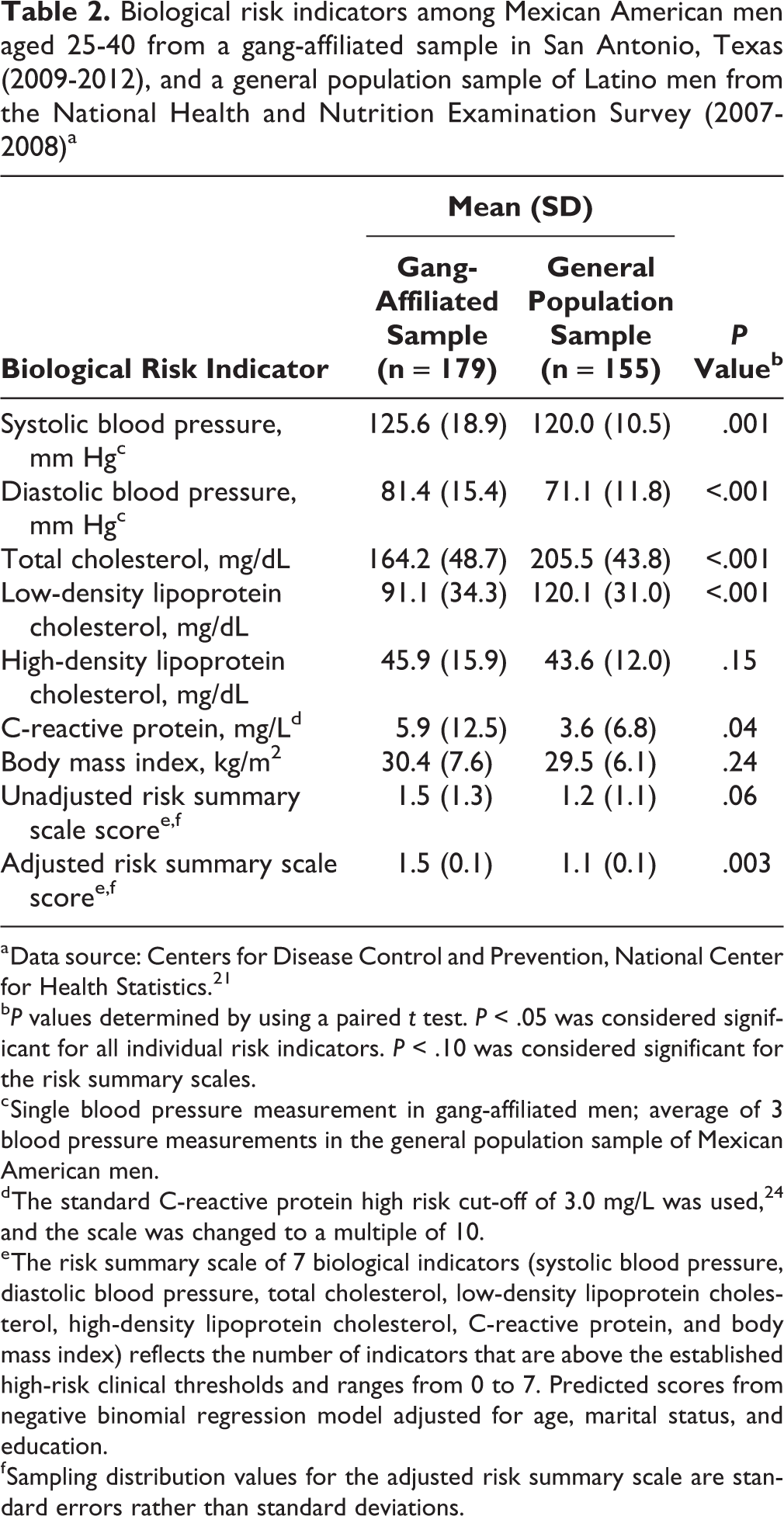
a Data source: Centers for Disease Control and Prevention, National Center for Health Statistics. 21
bP values determined by using a paired t test. P < .05 was considered significant for all individual risk indicators. P < .10 was considered significant for the risk summary scales.
c Single blood pressure measurement in gang-affiliated men; average of 3 blood pressure measurements in the general population sample of Mexican American men.
d The standard C-reactive protein high risk cut-off of 3.0 mg/L was used, 24 and the scale was changed to a multiple of 10.
e The risk summary scale of 7 biological indicators (systolic blood pressure, diastolic blood pressure, total cholesterol, low-density lipoprotein cholesterol, high-density lipoprotein cholesterol, C-reactive protein, and body mass index) reflects the number of indicators that are above the established high-risk clinical thresholds and ranges from 0 to 7. Predicted scores from negative binomial regression model adjusted for age, marital status, and education.
f Sampling distribution values for the adjusted risk summary scale are standard errors rather than standard deviations.
Mexican American men aged 25-40 with high-risk biological risk indicators and with active sexually transmitted infections, from a gang-affiliated sample in San Antonio, Texas (2009-2012), and a general population sample of Latino men from the National Health and Nutrition Examination Survey (2007-2008)a
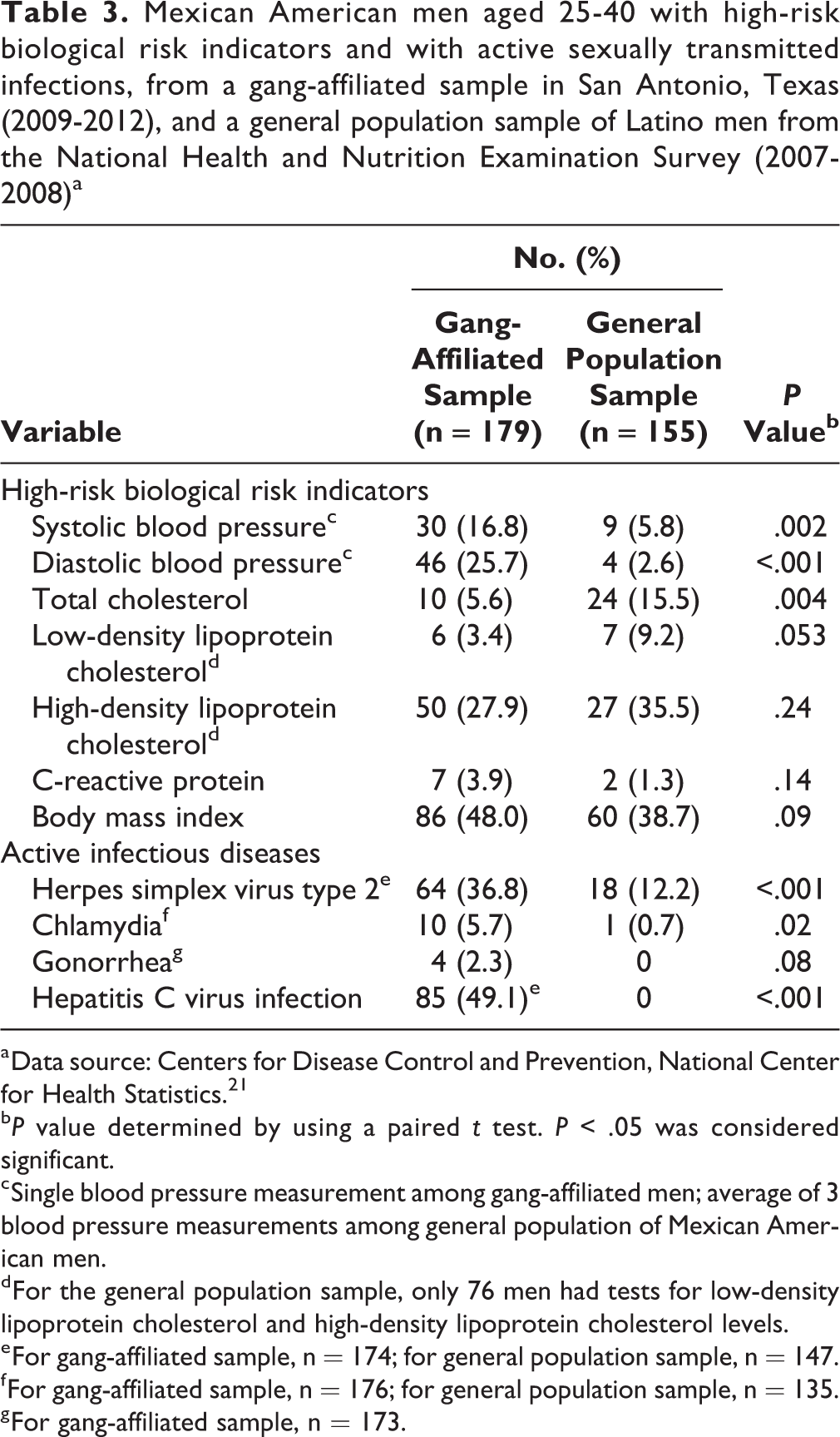
a Data source: Centers for Disease Control and Prevention, National Center for Health Statistics. 21
bP value determined by using a paired t test. P < .05 was considered significant.
c Single blood pressure measurement among gang-affiliated men; average of 3 blood pressure measurements among general population of Mexican American men.
d For the general population sample, only 76 men had tests for low-density lipoprotein cholesterol and high-density lipoprotein cholesterol levels.
e For gang-affiliated sample, n = 174; for general population sample, n = 147.
f For gang-affiliated sample, n = 176; for general population sample, n = 135.
g For gang-affiliated sample, n = 173.
Men in the general population sample, compared with men in the gang-affiliated sample, had significantly higher mean total cholesterol (205.5 vs 164.2 mg/dL, P < .001) and LDL cholesterol (120.1 vs 91.1 mg/dL, P < .001) levels, but the difference in mean HDL cholesterol levels between the 2 groups was not significant (P = .15) (Table 2). Also, men in the general population sample, compared with men in the gang-affiliated sample, had a significantly higher proportion with high-risk total cholesterol (24/161 [14.9%] vs 10/179 [5.6%], P = .004) (Table 3). The relative risks of men in the general population sample, compared with those in the gang-affiliated sample, having total and LDL cholesterol levels above the high-risk cut points were 2.7 and 2.8, respectively.
Men in the gang-affiliated sample, compared with men in the general population sample, had a significantly higher mean value for CRP (5.9 vs 3.6 mg/dL, P = .04) (Table 2). In addition, the mean BMI was close to the high-risk cut point for obesity for both samples.
The gang-affiliated group had a significantly higher average unadjusted risk summary scale score than the general population group (1.5 vs 1.2, P = .06) (Table 2). Using a negative binomial regression model on the 2 samples, adjusted for age, education, and marital status, we estimated an incidence risk ratio for the adjusted risk summary scale score of 1.30 (β = 0.32, SE = 0.11, P = .003), indicating that the mean risk summary score for gang-related men was significantly higher than that for men in the general population sample, even when other demographic factors were held constant (1.50 vs 1.15, P = .003).
Higher proportions of men in the gang-affiliated sample compared with the general population sample had herpes simplex virus type 2 (64/174 [36.8%] vs 18/147 [12.2%], P < .001), chlamydia (10/176 [5.7%] vs 1/135 [0.7%], P = .02), and HCV infection (85/173 [49.1%] vs 0, P < .001) (Table 3). Based on these findings, men in the gang-affiliated sample had a 3-fold higher risk of testing positive for herpes simplex virus type 2 and an 8.5-fold higher risk of testing positive for chlamydia than men in the general population sample.
Almost half (85/173 [49.1%]) of men in the gang-affiliated population tested positive for HCV infection (Table 3), but only 38 (44.7%) of those men were aware of their status. In the sample of gang-affiliated men, only 1 of the 10 men with chlamydia, none of the 4 men with gonorrhea, and 1 of the 64 men with herpes simplex virus type 2 self-reported their diagnoses. In the same sample, 20 men reported a previous diagnosis of chlamydia and 15 men reported a previous diagnosis of gonorrhea. Only 1 man in the gang-affiliated sample tested positive for HIV, and most (174/179 [97.2%]) reported having had at least 1 HIV test in their lifetime.
Discussion
Our study contributes to the growing body of literature on the long-term health consequences of gang membership. 5,26,27 It also adds to the knowledge base about biological risk indicators among sociodemographic subcategories of racial/ethnic minority groups in the United States. 28 -31
Our findings suggest an association between gang membership and elevated risks for cardiovascular, metabolic, and infectious diseases. Specifically, when compared with the general population sample, the gang-affiliated sample had higher blood pressure levels and CRP and a higher prevalence of STIs. The findings on blood pressure are important because high blood pressure is a risk factor for cardiovascular disease. The difference in prevalence of HCV infection between the samples is also concerning because of the relatively young age of the men in the gang-affiliated sample.
These poor health characteristics are further exacerbated by low levels of access to health care services, lack of health care resources, and relatively young age among the gang-affiliated population. An awareness of these characteristics is important when addressing both current and potentially long-term health conditions in this population. Most of the biological risk indicators and STIs that we assessed are treatable. Yet, if left undiagnosed and untreated, they can lead to early morbidity and mortality.
Our findings also contribute to an accurate portrayal of the health status of Mexican Americans, the largest subpopulation of Latinos in the United States. Members of this group are often at the nexus of high levels of social vulnerability, health risk, and health care costs. Furthermore, with the Affordable Care Act now providing health care to millions of low-income people, including those in the criminal justice–involved population, 32 -34 an in-depth understanding of the unique health risks borne by people previously excluded from health care services is of great value. Our findings provide insight into the health risks of Mexican Americans and gang-affiliated men, and they highlight the need for tailored prevention strategies to curtail potential health epidemics in racial/ethnic minority communities.
Our findings also point to the importance of understanding how adverse experiences among young people relate to adverse health outcomes during adulthood. Although our study did not focus on the effect of childhood trauma on health risk, others have found that adolescent gang membership is associated with poverty, violence victimization, and intergenerational drug use and criminality. 35 -38 In addition, studies of gang-involved populations found that they harbor high levels of childhood physical neglect, illicit drug use, and mental health conditions. 22,25,27 Further research is warranted to help understand how adverse experiences throughout the life course may affect adult health and well-being. Although the causes of health inequities are complex, future analyses could build on our findings to understand how various social determinants and trajectories of gang membership and incarceration influence adult health status.
Finally, our work contributes to mounting public health evidence on the consequences of long-term exposure to psychosocial stressors on dysregulation and detrimental health conditions. 39,40 Among other findings, we noted a higher proportion of men with elevated CRP levels and significantly higher mean CRP levels in the gang-affiliated sample compared with the general population sample. CRP is a marker for systemic inflammation. Future research might explore how the stress of everyday life associated with poverty, incarceration, trauma, and drug use, often experienced by disadvantaged racial/ethnic minority populations, may lead to high levels of distress and anxiety, which in turn may contribute to systemic inflammation and subsequent morbidity and mortality.
Limitations
Our study had several limitations. First, although we attempted to make comparisons across samples, we acknowledge that the samples may not be directly comparable. The NHANES sample, relative to the gang-affiliated sample, represented a more general population with a wider geographic distribution. Furthermore, comparison data were not available for the San Antonio area specifically. We should also note that because of the data available at the time of the analysis, there were differences in years between the studied gang group and the comparison group (2009-2012 vs 2007-2008). Also, the data obtained from the NHANES were based on blood samples taken during fasting and the average of 3 blood pressure measurements taken during fasting. In contrast, data for the gang-affiliated sample were obtained by using nonfasting blood samples, and blood pressure measurements were based on a single random measurement. Because blood pressure is affected by numerous factors and may vary by time of day, 41 these measures may not be directly comparable. Second, the high-sensitivity CRP test was not used for either sample. However, because the standard CRP test was used for both populations, the CRP data we used were likely comparable.
Third, the NHANES data that we used did not include any information about gang involvement. As a result, we were unable to purposefully exclude men with former or current gang involvement from the general population sample. However, research suggests that people who are long-term gang members and those involved in the criminal justice system are underrepresented in national household surveys such as NHANES. 10,12,13,42 Therefore, we believe that the risk of bias was small. Fourth, our study did not clarify whether the differences that we identified between the samples were attributable to gang membership, contact with the criminal justice system, poverty, discrimination, or other sources of disadvantage, all of which are possible given that these factors are intertwined. Finally, the generalizability of our results may be somewhat limited until comparable investigations are conducted with similar populations. Nonetheless, our findings likely represent the experiences of Latino adolescents and young adults living in low-income neighborhoods across the United States, who are disproportionately at risk for engaging in delinquency and crime-related gang activities and for exposure to the criminal justice system.
Conclusions
We identified important differences in the prevalence of biological risk factors associated with cardiovascular and metabolic diseases, and in the prevalence of infectious diseases, between a unique subgroup of gang-affiliated, high-risk, nonimmigrant, US Mexican American men and a group representing the general Mexican American male population. These disparities indicate substantial risk and long-term health implications for disadvantaged and gang-affiliated Mexican American men, highlighting the need to tailor prevention strategies to this population of men and collect biological measures for these populations. Our findings are important given the young age of these men and their lack of health care resources, which are needed to address current health issues and long-term health consequences. Our results also suggest the possibility that stress processes associated with the challenges that young racial/ethnic minority men in urban environments face may contribute to previously unappreciated systemic inflammation. Long-term exposure to psychosocial stressors and subsequent systemic inflammation may increase the risk for physiological and psychological dysregulation and detrimental chronic health conditions in this population.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for this study was provided by the National Institutes of Health, National Institute on Drug Abuse grant R01DA023857.