
Abstract
Objectives:
Sodium reduction in restaurant foods is important because 77% of sodium in the United States is consumed by eating prepared and restaurant foods. We evaluated a sodium-reduction intervention, Healthy Chinese Take-Out Initiative, among Chinese take-out restaurants in low-income neighborhoods in Philadelphia, Pennsylvania. Our objectives were to (1) analyze changes in the sodium content of food samples and (2) collect data on changes in chefs’ and owners’ knowledge about the health risks of sodium overconsumption, perceptions of the need for sodium reduction, self-efficacy for lowering sodium use, and perceptions of training needs for sodium-reduction strategies.
Methods:
The initiative trained chefs from 206 Chinese take-out restaurants on strategies to reduce sodium in prepared dishes. We analyzed changes in the sodium content of the 3 most frequently ordered dishes—shrimp and broccoli, chicken lo mein, and General Tso’s chicken—from baseline (July-September 2012) to 36 months after baseline (July-September 2015) among 40 restaurants. We conducted a survey to examine the changes in chefs’ and owners’ knowledge, perceptions, and self-efficacy of sodium reduction. We used multilevel analysis and repeated-measures analysis of variance to examine effects of the intervention on various outcomes.
Results:
We found significant reductions in the sodium content of all 3 dishes 36 months after a low-sodium cooking training intervention (coefficients range, –1.06 to –1.69, P < .001 for all). Mean knowledge (range, 9.2-11.1), perceptions (range, 4.6-6.0), and self-efficacy (range, 4.2-5.9) (P < .001 for all) of sodium reduction improved significantly from baseline (August 2012) to posttraining (also August 2012), but perceptions of the need for sodium reduction and self-efficacy for lowering sodium use returned to baseline levels 36 months later (August 2015).
Conclusions:
The intervention was a useful population health approach that led to engaging restaurants in sodium-reduction practices. Local public health agencies and professionals could partner with independent restaurants to introduce environmental changes that can affect population health on a broad scale, particularly for vulnerable populations.
Keywords
Cardiovascular disease (CVD) caused 1 of 3 deaths in the United States during 2012-2013 and led to health care, medication, and socioeconomic costs of more than $300 billion that same year. 1 Excess sodium consumption contributes to CVD risks. According to the Dietary Guidelines for Americans published by the US Department of Health and Human Services (HHS) and the US Department of Agriculture (USDA), the recommended sodium consumption is <2300 mg of sodium daily, which is about 800 mg per meal. The guidelines also recommend that people who have hypertension, who are middle-aged and older, or who are African American consume no more than 1500 mg of sodium per day. 2 However, the average sodium intake in the United States far exceeds the recommended amount. In the typical American diet, 77% of sodium intake comes from processed and restaurant foods. 3 Sodium content in restaurant foods can be extremely high, averaging 1512 mg in a main entrée 4 and up to 3200 mg for meals consisting of an entrée, a side dish, and shared appetizers. 5 This finding is particularly concerning for people in low-income racial/ethnic minority groups, including Hispanic, Asian, and African American people, who have high levels of dietary sodium intake, 6 eat restaurant meals more often, 7 and have a higher risk of developing and dying of hypertension and heart disease compared with non-Hispanic white people. 8 –10
Even modest decreases in sodium intake could yield substantial reductions in CVD-related morbidity, mortality, and medical costs. 11,12 Public health authorities worldwide are seeking population-level public health interventions for dietary sodium reduction. 13 –15 Suggested strategies include public-private partnerships, food and menu labeling, public education, product reformulation, and community action. 16 –18 According to a 2010 Institute of Medicine report, multiple public health efforts have attempted to reduce sodium intake, including encouraging food manufacturers and chain restaurants to reduce levels of sodium in the food supply voluntarily. 19 The results, however, have been less than ideal; several studies found consistently high levels of sodium intake from fast-food restaurant meals. 20 –22 Furthermore, sodium-reduction efforts in all settings at the local level—particularly those targeting high-risk populations—have been limited. Although the literature suggests that menu-labeling interventions promoting healthier options in restaurants in low-income communities are feasible and effective, 23 –25 research showing the effect of targeted sodium-reduction practices in large-scale restaurant interventions is scarce.
A study of take-out meals in the United Kingdom found that Chinese dishes had the highest sodium density of all meal categories examined. 26 To reduce sodium in foods, one approach is to use substitutes for sodium, including other spices, low- or no-sodium sauces such as fish sauce, or other types of sauce containing calcium or potassium. 27,28 These substitutes can be made with little or no substantial loss of taste. The main barriers to maintaining a low-sodium diet are taste, lack of initial acceptability of reduced-sodium foods, and lack of control of food preparation in meals. However, studies have not tested culturally appropriate interventions to reach chefs and owners of Chinese take-out restaurants in overcoming these barriers on a large scale.
Using a population health approach, 29 we conducted a large-scale, culturally sensitive intervention, the Healthy Chinese Take-Out Initiative (HCTI), to reduce the sodium content of dishes prepared by Chinese take-out restaurants in low-income urban communities in Philadelphia, Pennsylvania. We evaluated the changes in (1) laboratory-analyzed sodium content in 3 of the most popular dishes in Chinese take-out restaurants in a subset of HCTI participating restaurants and (2) sodium-related knowledge, perceptions, self-efficacy, and training needs of chefs.
Methods
HCTI Intervention
HCTI was a unique citywide effort to prevent and mitigate CVD among racial/ethnic minority groups in Philadelphia by decreasing the sodium content in meals served at 206 Chinese take-out restaurants. Established in 2012, the HCTI is a partnership among Temple University’s Center for Asian Health, Asian Community Health Coalition, Greater Philadelphia Chinese Restaurant Association, and Philadelphia Department of Public Health. Philadelphia has the highest prevalence of hypertension among the 10 largest US cities: 48% among African Americans and 32% among Hispanic Americans. 30 Chinese take-out restaurants are located predominantly in low-income neighborhoods with large racial/ethnic minority populations. Philadelphia has more than 400 independently owned and operated Chinese take-out restaurants that serve 6 million customers annually. 29
All HCTI partners were involved in project planning, development, implementation, and evaluation. The HCTI intervention consisted of (1) professionally led, culturally tailored training on healthy low-sodium cooking training; (2) distribution of low-sodium cooking materials, including low-sodium recipes, cooking utensils, and standard measuring spoons; (3) a citywide sodium-reduction mass-media campaign; and (4) annual one-on-one booster trainings and compliance checks with chefs. The training sessions on low-sodium cooking included (1) information on sodium intake and the benefits of reduced sodium intake on health improvement and disease prevention, (2) sodium intake guidelines, (3) strategies to reduce the use of sodium during food preparation and the availability of sodium to consumers, (4) cooking demonstration by culinary and nutrition experts, and (5) hands-on practice for all training attendees, including restaurant owners and chefs.
Our research team from Temple University’s Center for Asian Health conducted annual booster training at each participating restaurant to reinforce what attendees had learned at the initial interactive low-sodium cooking training session. Booster training began after the follow-up assessment. Project staff members offered additional resources and technical assistance during site visits. Participating restaurants implemented various sodium-reduction strategies, including using low-sodium ingredients, reducing the amount of sauce or soy sauce added to dishes, using fresh vegetables instead of canned vegetables, cooking with additional herbs and spices (eg, garlic, ginger, and chilies), and limiting distribution of soy sauce packets. Center for Asian Health research staff members conducted compliance checks in 2013, 1 year after baseline, to monitor the changes owners and chefs made in their food preparation and cooking practices and to assess customer response. All trainings, materials, and compliance checks were conducted in Chinese. The study was reviewed and considered exempt by the Temple University Institutional Review Board (IRB) and the Philadelphia Department of Public Health IRB.
Participants and Project Design
Of 450 Chinese take-out restaurants in Philadelphia, we contacted 250 restaurants in low-income neighborhoods. Of those, we identified 206 restaurants that were eligible and had owners who agreed to participate in the HCTI. To be eligible, a restaurant had to (1) be located in high-poverty ZIP codes in Philadelphia (≥20% of residents at or below the federal poverty level according to the American Community Survey 31 ), (2) serve solely as a take-out establishment, and (3) have owners or chefs who self-identified as Chinese Americans (the chefs could also be the owners).
Data Collection and Measurement for Food Sodium Content
To ensure equal representation geographically, we divided Philadelphia into 5 areas: north, south, east, west, and central. We then used stratified sampling to select 40 participating restaurants in the HCTI initiative to conduct sodium content analysis in their dishes during a 3-year period at 4 assessment points: baseline (July-September 2012), 6 months after baseline (January-March 2013), 24 months after baseline (July-September 2014), and 36 months after baseline (July-September 2015). We selected the 3 most frequently ordered dishes—shrimp and broccoli, chicken lo mein, and General Tso’s chicken—for sodium content analysis. The food samples were collected in a double-blind approach from the restaurants. Food orders were placed by volunteers of the research center who were not involved in the project and whose identity and affiliation were not revealed to the restaurants. Volunteers picked up the orders from the restaurants, collected food samples, and packaged and shipped them to Eurofins Scientific, Inc laboratories for sodium content analysis. For shrimp and broccoli and chicken lo mein, samples were collected at all 4 points (baseline, 6 months after baseline, 24 months after baseline, and 36 months after baseline). For General Tso’s chicken, measures were collected at 3 time points (6 months after baseline, 24 months after baseline, and 36 months after baseline); data were not collected at baseline because the funder requested it be added after baseline. We assigned each sample a unique identification linked to the restaurant to match the sodium results over time. We measured the total weight of each dish and the sodium content of each dish (in mg) per gram of food (mg/g).
Measuring Knowledge and Attitudes About Excess Sodium Consumption
We assessed restaurant owners’ and chefs’ knowledge and attitudes toward health consequences of sodium overconsumption at 3 points: baseline (August 2012), immediately after the chef training on the same day as baseline (posttraining, August 2012), and 36 months after baseline (August 2015). Of the 206 participating restaurants, 199 completed both baseline and posttraining assessments (97% response rate), and 166 restaurants completed the follow-up survey 36 months after baseline (83% response rate). We conducted all surveys through in-person interviews.
Using in-person interviews, we pilot-tested all instruments with 10 owners and chefs, revised the instruments based on feedback, and then translated the instruments into Chinese. Staff members at the Center for Asian Health, Temple University, and partnership organizations conducted in-person interviews. Measurement items and their reliability and validity are previously described. 29
The knowledge scale consisted of 13 items that measured chefs’ and owners’ knowledge of the health effects of excessive sodium consumption and the main source of sodium in diet. Chefs and owners responded to statements such as “consuming too much salt in the diet is harmful or very harmful,” “high blood pressure is associated with consuming too much salt,” and “salt added in processed food is the main source of salt in our diet.” The knowledge scale had moderate reliability at baseline (α = 0.50), posttraining (α = 0.65), and 36 months after baseline (α = 0.50). The original response options were on a 5-point Likert scale ranging from 1 (strongly disagree) to 5 (strongly agree). We then dichotomized answers, with 1 to 2 recoded as 1 (high level of knowledge) and 3 to 5 recoded as 0 (low level of knowledge). We summed answers for the 13 items to compute the knowledge score, which ranged from 0 to 13.
We used 7 items to compute a scale of perceptions of the need for preparing and offering low-sodium dishes. We asked participants their opinion about statements such as “There should be a reduction in the amount of salt in restaurant foods,” “Reducing the amount of salt in the menu options will benefit the restaurant,” and “More customers will be attracted by offering low-salt options on the menu.” The original response options were on a 5-point Likert scale ranging from 1 (strongly agree) to 5 (strongly disagree). We dichotomized the responses, with 1 to 2 recoded as 1 (high perception) and 3 to 5 recoded as 0 (low perception). Then we summed the answers to comprise the perception scores, which ranged from 0 to 7. The perception scale had moderate to high reliability at baseline (α = 0.85), posttraining (α = 0.82), and 36 months after baseline (α = 0.65).
We measured chefs’ and owners’ perceived self-efficacy to lower sodium use in restaurant food by using 7 items, including “confidence in reformulating recipes” and “confidence in cooking low-salt food.” We dichotomized responses on a 4-point Likert scale (1 = not at all confident to 4 = very confident) at the midpoint, with 1 to 2 recoded as 0 (low self-efficacy) and 3 to 4 recoded as 1 (high self-efficacy). Then we summed the scores to comprise the training needs scale, which ranged from 0 to 7. The self-efficacy scale had high reliability at baseline (α = 0.91), posttraining (α = 0.87), and 36 months after baseline (α = 0.78).
To measure chefs’ and owners’ perceptions of training needs for sodium-reduction strategies, we asked them about their level of training needs in 7 areas, including reformulating recipes and purchasing low-sodium food items from distributors. The original answers were on a 4-point Likert scale (1 = no need to 4 = high need). We dichotomized responses at the midpoint, with 1 to 2 recoded as 0 (no or low need) and 3 to 4 recoded as 1 (moderate or high need). Then we summed them to comprise the training needs scale, which ranged from 0 to 7, with a higher numeric value indicating a higher training need. The scale had high reliability at baseline (α = 0.83) and posttraining (α = 0.98) but low internal reliability at 36 months after baseline (α = 0.36).
Statistical Analysis
Sodium content analysis
We conducted 3 multilevel models, one for each dish, with sodium content (mg of sodium per gram of food [mg/g]) as the outcome variable and time point as a predictor. We used this multilevel procedure to account for the inherent dependency of the repeated-measures design, 32 and we used maximum likelihood estimation to account for missing data. Time (a level 1 measure) was nested within restaurants (a level 2 measure), with intercepts allowed to vary by restaurant. We contrast-coded time such that the time parameter measured change or difference in sodium content between baseline and 36 months after baseline for shrimp and broccoli and chicken lo mein and between 6 months after baseline and 36 months after baseline for General Tso’s chicken. Because no samples of General Tso’s chicken were collected at baseline, the results of this model could not be directly compared with results of the other 2 models. We calculated observed means of sodium content for all dishes at all time points. To compare the sodium content of these 3 dishes at 36 months after baseline with the USDA/HHS sodium intake guidelines, 2 we multiplied the dish weight (g) by sodium content (mg Na/g of food) to obtain the estimated total amount of sodium content in each dish. We analyzed the sodium content data using R version 3.3.2. 33
Secondary outcome analysis
We conducted individual repeated-measures analysis of variance models to examine the change in knowledge, perception, self-efficacy, and training needs from baseline to posttraining to 36 months after baseline. Huynh-Feldt test 34 and Greenhouse-Geisser test 35 results found no violation of sphericity in all repeated-measures analysis of variance analyses. We used the Tukey honest significant difference test for post hoc comparisons. We considered P < .05 to be significant. We performed statistical analyses for the knowledge and perception data with Stata version 14. 36
Results
The multilevel models (Table 1) showed a significant reduction in the sodium content of shrimp and broccoli (β = –1.69, P < .001) and chicken lo mein (β = –1.40, P < .001) from baseline to 36 months after baseline. The sodium content of General Tso’s chicken dropped significantly (β = –1.06, P < .001) from 6 months after baseline to 36 months after baseline. Intraclass correlation coefficients indicate the proportion of variance in the outcome variable—sodium content—that is explained by the time variable: 36% of the variation in sodium content in shrimp and broccoli can be attributed to the varying time periods of data collection, 41% of the variation in chicken lo mein, and 54% of the variation in General Tso’s chicken.
Multilevel model results for sodium content analysis of 3 mealsa at Chinese take-out restaurants in low-income neighborhoods (n = 40), Healthy Chinese Take-Out Initiative (HCTI),b Philadelphia, Pennsylvania, 2012-2015
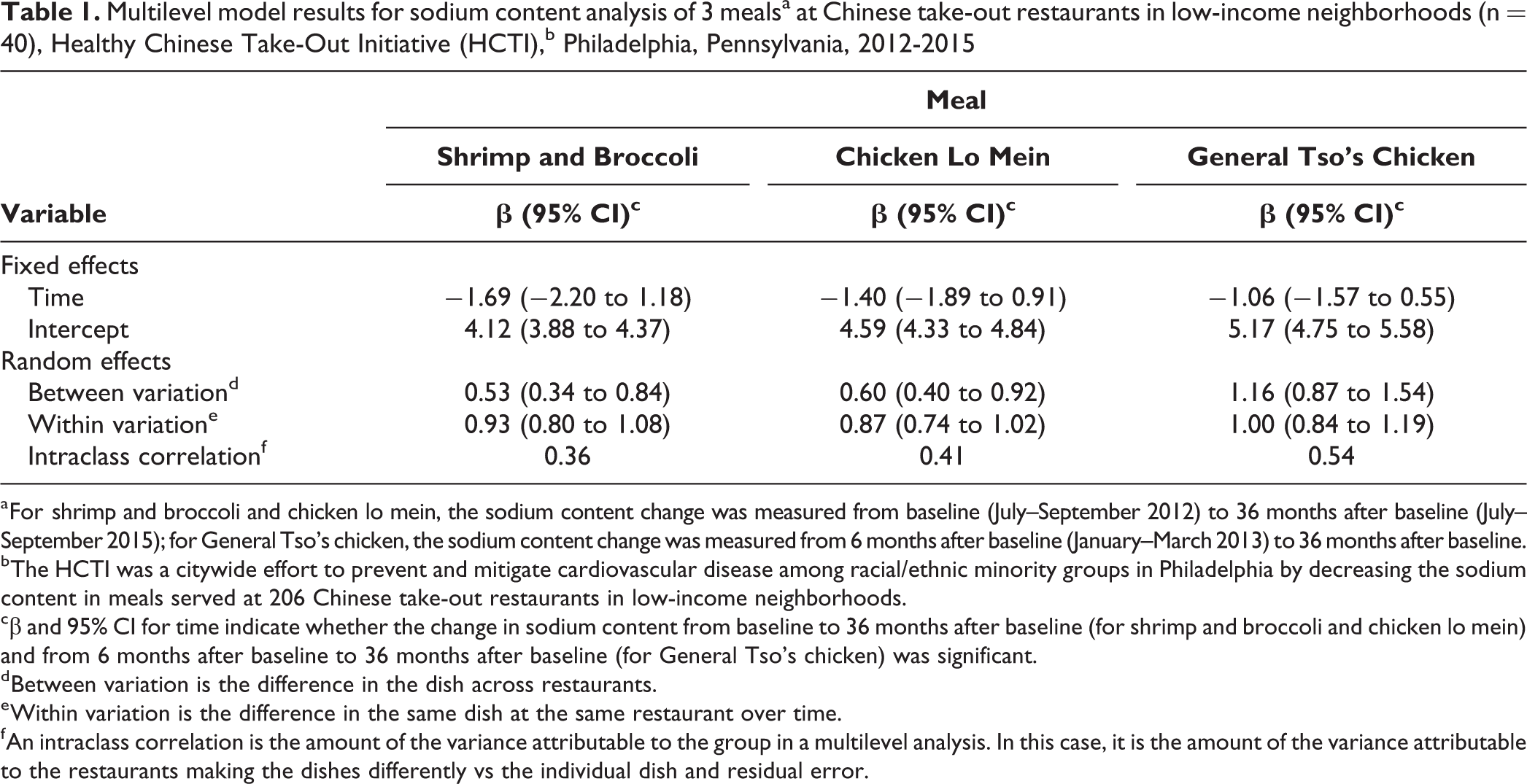
a For shrimp and broccoli and chicken lo mein, the sodium content change was measured from baseline (July–September 2012) to 36 months after baseline (July–September 2015); for General Tso’s chicken, the sodium content change was measured from 6 months after baseline (January–March 2013) to 36 months after baseline.
b The HCTI was a citywide effort to prevent and mitigate cardiovascular disease among racial/ethnic minority groups in Philadelphia by decreasing the sodium content in meals served at 206 Chinese take-out restaurants in low-income neighborhoods.
cβ and 95% CI for time indicate whether the change in sodium content from baseline to 36 months after baseline (for shrimp and broccoli and chicken lo mein) and from 6 months after baseline to 36 months after baseline (for General Tso’s chicken) was significant.
d Between variation is the difference in the dish across restaurants.
e Within variation is the difference in the same dish at the same restaurant over time.
f An intraclass correlation is the amount of the variance attributable to the group in a multilevel analysis. In this case, it is the amount of the variance attributable to the restaurants making the dishes differently vs the individual dish and residual error.
Sodium content was highest in General Tso’s chicken and lowest in shrimp and broccoli at all points. The reduction in sodium content was largest in shrimp and broccoli during the study period: a 36% relative reduction (from 5.5 to 3.5 mg/g). The relative reduction was 28% for chicken lo mein (from 5.7 to 4.1 mg/g), and from 6 months after baseline to 36 months after baseline, the sodium content of General Tso’s chicken dropped 19% (from 5.9 to 4.8 mg/g) (Figure). On average, all 3 dishes exceeded the maximum amount of sodium recommended by the USDA/HHS sodium intake guideline 2 for a single meal (lunch or dinner) at baseline and 36-month follow-up. The mean sodium content for shrimp and broccoli 36 months after baseline was 1508 mg and for General Tso’s chicken was 2004 mg, both of which exceeded the HHS/USDA guidelines 2 for a single meal (lunch or dinner). The mean sodium content for chicken lo mein was 2346 mg, which slightly exceeded the maximum daily sodium guideline (Table 2).
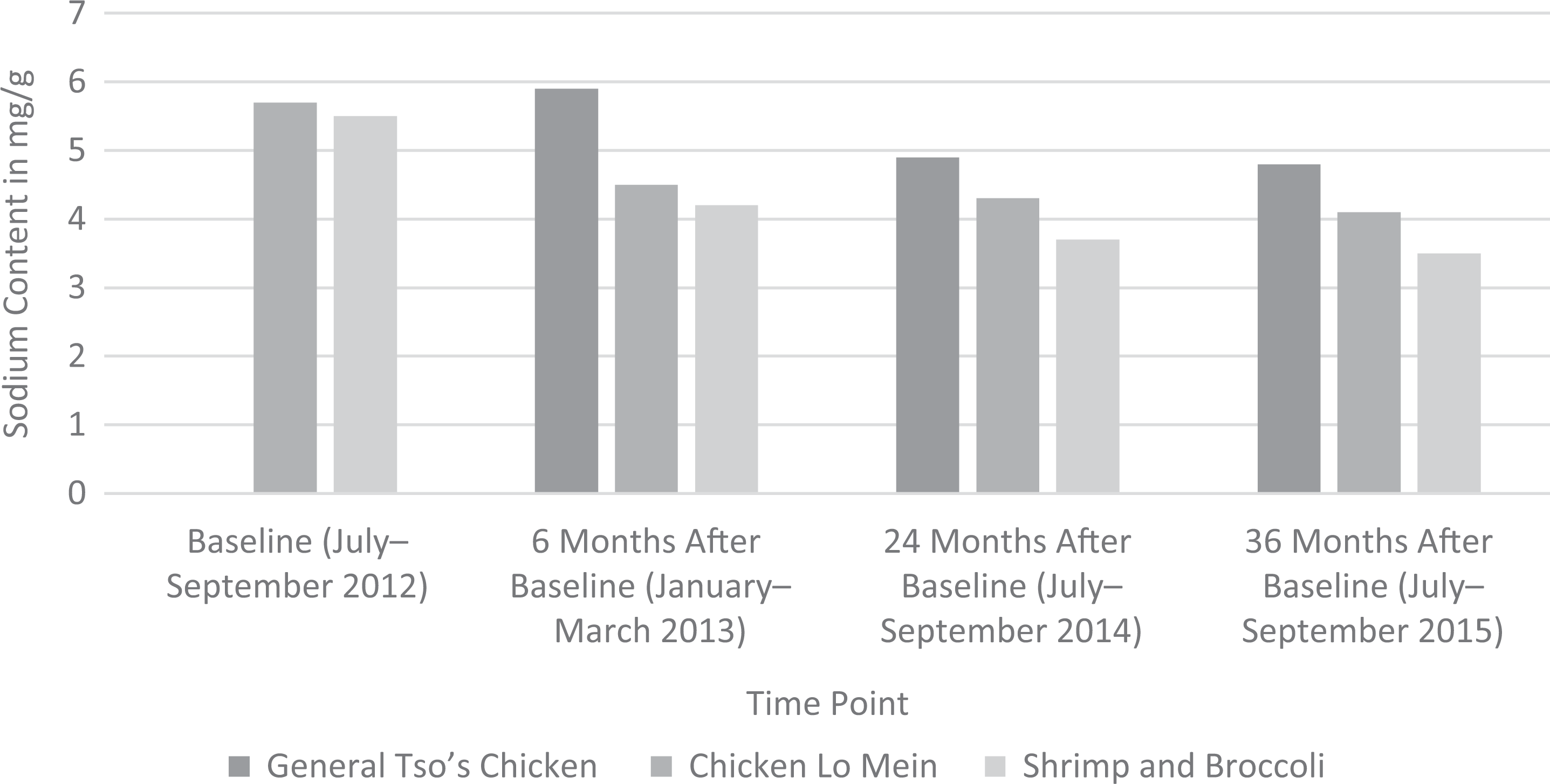
Mean sodium content of 3 Chinese take-out dishes at Chinese take-out restaurants in low-income neighborhoods (n = 166), Healthy Chinese Take-Out Initiative (HCTI), Philadelphia, Pennsylvania, 2012-2015. The HCTI was a citywide effort to prevent and mitigate cardiovascular disease among racial/ethnic minority groups in Philadelphia by decreasing the sodium content in meals served at 206 Chinese take-out restaurants in low-income neighborhoods. Data were not collected at baseline for General Tso’s chicken. Sodium content in milligrams per gram of food.
Total weight and sodium content per dish at 36 months after baseline in an analysis of 3 mealsa at Chinese take-out restaurants in low-income neighborhoods (n = 40), Healthy Chinese Take-Out Initiative (HCTI),b Philadelphia, Pennsylvania, 2012-2015
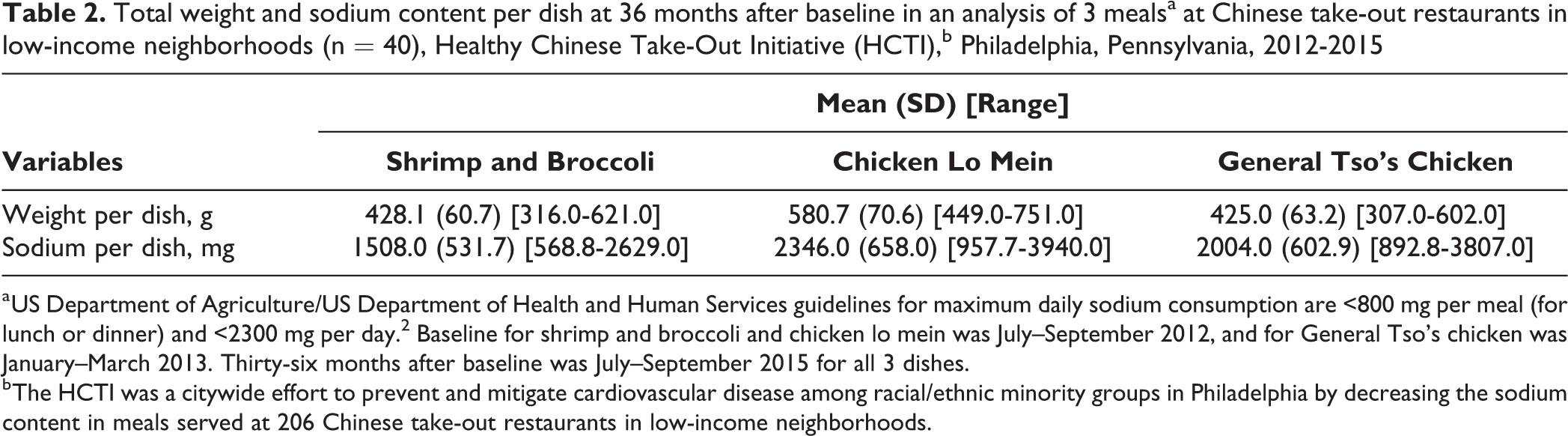
a US Department of Agriculture/US Department of Health and Human Services guidelines for maximum daily sodium consumption are <800 mg per meal (for lunch or dinner) and <2300 mg per day. 2 Baseline for shrimp and broccoli and chicken lo mein was July–September 2012, and for General Tso’s chicken was January–March 2013. Thirty-six months after baseline was July–September 2015 for all 3 dishes.
b The HCTI was a citywide effort to prevent and mitigate cardiovascular disease among racial/ethnic minority groups in Philadelphia by decreasing the sodium content in meals served at 206 Chinese take-out restaurants in low-income neighborhoods.
Post hoc tests indicated that knowledge increased significantly from baseline to posttraining and was maintained from posttraining to 36 months after baseline (Table 3). Perceptions of the need for preparing and offering low-sodium dishes and self-efficacy increased significantly from baseline to posttraining (P < .001) and then returned to baseline levels at 36 months after baseline. Perceptions of the need for training did not change significantly from baseline to posttraining and returned to baseline levels at 36 months after baseline.
Results of repeated-measures analysis of variance for differences in knowledge, self-efficacy, and training needs of sodium content among owners and chefs of Chinese take-out restaurants in low-income neighborhoods (n = 166), Healthy Chinese Take-Out Initiative (HCTI),a Philadelphia, Pennsylvania, 2012-2015
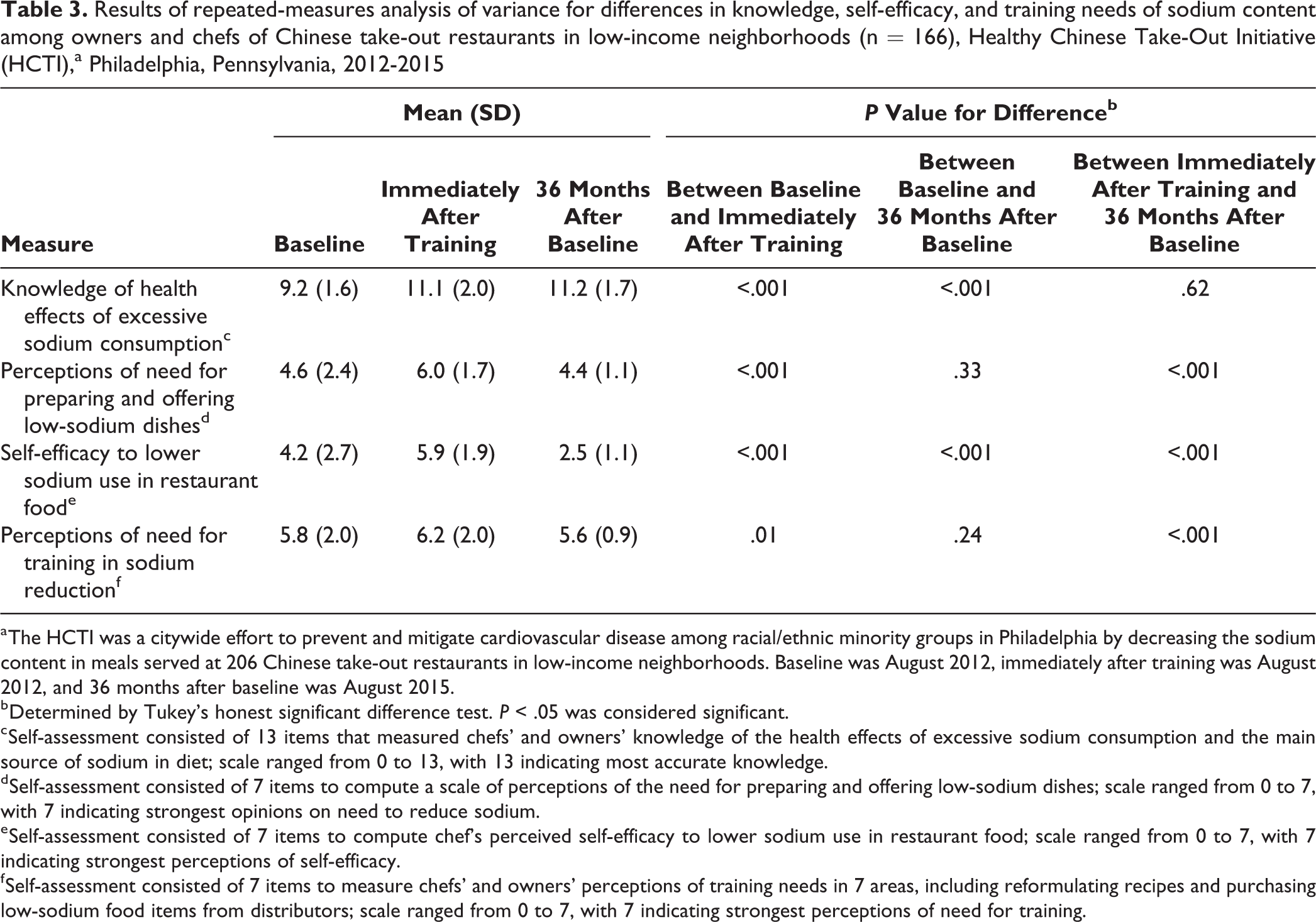
a The HCTI was a citywide effort to prevent and mitigate cardiovascular disease among racial/ethnic minority groups in Philadelphia by decreasing the sodium content in meals served at 206 Chinese take-out restaurants in low-income neighborhoods. Baseline was August 2012, immediately after training was August 2012, and 36 months after baseline was August 2015.
b Determined by Tukey’s honest significant difference test. P < .05 was considered significant.
c Self-assessment consisted of 13 items that measured chefs’ and owners’ knowledge of the health effects of excessive sodium consumption and the main source of sodium in diet; scale ranged from 0 to 13, with 13 indicating most accurate knowledge.
d Self-assessment consisted of 7 items to compute a scale of perceptions of the need for preparing and offering low-sodium dishes; scale ranged from 0 to 7, with 7 indicating strongest opinions on need to reduce sodium.
e Self-assessment consisted of 7 items to compute chef’s perceived self-efficacy to lower sodium use in restaurant food; scale ranged from 0 to 7, with 7 indicating strongest perceptions of self-efficacy.
f Self-assessment consisted of 7 items to measure chefs’ and owners’ perceptions of training needs in 7 areas, including reformulating recipes and purchasing low-sodium food items from distributors; scale ranged from 0 to 7, with 7 indicating strongest perceptions of need for training.
Discussion
To our knowledge, the HCTI intervention was the largest initiative in the United States to engage independent Chinese take-out restaurant chefs and owners in a coordinated sodium-reduction intervention. The results of this study lend support to population-level interventions to reduce sodium content in restaurant-prepared foods.
We found significant and sustained sodium reduction in participating restaurants during a 3-year period. The reductions were in line with the Institute of Medicine’s recommendations of small gradual declines in sodium content over time. 19 These gradual changes can have a large effect; a 600- to 900-mg reduction in sodium can lead to a 1.5- to 3-point decrease in blood pressure, which can substantially improve cardiovascular health for restaurant customers in the United States. Our results suggest that the training, low-sodium recipes, healthier cooking methods, and booster sessions provided to the chefs and owners were effective and, more important, sustainable. Because Chinese take-out restaurants are prevalent in low-income African American and Hispanic neighborhoods, reducing the sodium content could be a valuable approach to addressing health disparities and the high burden of CVD, hypertension, and other chronic diseases that disproportionally affect these racial/ethnic minority populations. 8,37 Previous research used laboratory analysis to assess the nutritional quality of restaurant foods, evaluate the practicality of voluntary menu-labeling strategies, or assess the accuracy of restaurant’s healthy meal claims, 38 but few studies used laboratory analysis to evaluate the effect of an intervention on sodium reduction. Future research should expand the intervention to other restaurants, such as restaurants serving pizza, delis, or buffets.
Knowledge of the health effects of excessive sodium consumption, perceptions about preparing and offering low-sodium meals, and self-efficacy to lower sodium use improved significantly from baseline to posttraining, which is consistent with findings from community-level interventions. 39 –42 Interestingly, the improvements in perceptions and self-efficacy were not sustained at 36 months after baseline, and for self-efficacy, levels dropped significantly below baseline levels. This finding indicates that knowledge may be associated more with the sustained reductions in sodium content than were perceptions and self-efficacy. Another cause of these changes in knowledge, perception, and self-efficacy may have been change of ownership in more than 2 dozen restaurants, which might have affected the continuity of the intervention effect. The relatively high turnover rate in ownership and chef positions at Chinese take-out restaurants should be considered in the study design and data analysis of future studies of this industry. Future research should explore mechanisms behind changes in knowledge and perception, cooking and food preparation methods, and food sodium content.
Our findings indicate that sodium-reduction initiatives targeting food cooking and preparation in community-based settings are feasible and can sustainably reduce sodium content in food. National efforts are underway to conduct population-level sodium-reduction interventions in restaurants and institutional settings, such as school districts, hospitals, government facilities, and senior centers. 43 However, research on the availability and feasibility of healthier food options in restaurants and take-out venues in low-income urban areas is still limited. 44 Because restaurant food is a major contributor of sodium in the food supply, more approaches that involve working with restaurants and chefs to reduce the amount of sodium in restaurant food are needed. Independent restaurants may be easier to work with than chain restaurants because they have more flexibility in menu planning and decision making. However, independent restaurants may have more challenges than chain restaurants with purchasing and sourcing low-sodium products because of limited resources. 45 Furthermore, an intervention might be more scalable among chain restaurants than among independent restaurants because chain restaurants have established management channels that would better facilitate the distribution and use of standardized tools and measures.
Local public health agencies and professionals could partner with independent restaurants to introduce environmental changes that can affect population health on a broad scale, particularly for vulnerable populations. Food service training and education are recommended strategies to support sodium-reduction efforts in restaurants 46 and institutional settings. 47,48 Our study demonstrated the importance of incorporating behavioral strategies (eg, distributing standard spoon sizes and new recipes for low-sodium dishes), culturally appropriate training, and ongoing support.
Another accomplishment of the HCTI intervention was the development and maintenance of a unique partnership among government, academia, industry, and the community. Each partner contributed substantially to initiative development and implementation, creating a robust intervention with tangible results to the health of Philadelphians. The Greater Philadelphia Chinese Restaurant Association was particularly strategic in helping to recruit restaurants, create support at the leadership level, and recognize the valuable role that take-out restaurants could play in improving the community’s health.
Limitations
This study had several limitations. First, because of limited resources, only a small subset of restaurants was included in the laboratory sodium content analysis. Second, although patterns from 6 months after baseline to 36 months after baseline showed similarities between shrimp and broccoli and chicken lo mein, we lacked a baseline assessment of General Tso’s chicken, and the true magnitude of reduction from baseline to 36 months was unknown for this dish. Third, because of multiple opportunities for training, education, and technical assistance (cooking trainings, follow-up trainings, educational resources and tools, annual compliance checks) for restaurant owners and chefs, it was difficult to identify which intervention component had the greatest effect on sodium reduction. The comprehensiveness of the intervention may have contributed to its effectiveness and maintenance. Fourth, the study did not have a control group. Further testing through a cluster randomized controlled trial is needed. Future research could also examine sales and acceptance of sodium-reduced versions of prepared food. Health outcomes of the target population could also be studied as a result of this type of intervention. Finally, the time intervals between assessment points (18 months between 6 months and 24 months after baseline, 12 months between 24 months and 36 months after baseline) were long and might have introduced 2 intervening factors. First, the intervention effects might have been more likely to wane. In this sense, our findings of consistent and significant reduction in sodium content would be a conservative estimate of our intervention effects. Second, participating restaurants could have been exposed to other sodium-reduction campaigns or policies. Future studies should distinguish and examine the effects of population-level interventions at shorter intervals (eg, 3-month intervals) and longer intervals (eg, 12-month intervals for a prolonged period of 5 years).
Conclusions
This study showed that comprehensive training with Chinese take-out chefs and owners resulted in short-term improvements to attitudes and sustained, meaningful reductions in the sodium content of food from 2012 to 2015. These findings demonstrate the feasibility and potential benefits to population health of a coordinated partnership among public health agencies, academic institutions, and community businesses and organizations to reduce sodium in restaurants.
Footnotes
Acknowledgments
The authors thank volunteers and partners of Temple University’s Center for Asian Health, Asian Community Health Coalition, and Greater Philadelphia Chinese Restaurant Association for their contributions to the initiative. The views expressed in this article do not necessarily reflect the official policies of the US Department of Health and Human Services nor does mention of trade names, commercial practices, or organizations imply endorsement by the US government.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for this project was made possible in part by cooperative agreement no. 1U58DP003557 from the Centers for Disease Control and Prevention, US Department of Health and Human Services, and Get Healthy Philly, an initiative of the Philadelphia Department of Public Health.