
Abstract
Objectives:
Female family members affect both the likelihood of adolescent pregnancy and the outcome of that pregnancy. We examined the degree to which an older sister’s adolescent reproductive outcomes affect her younger sister’s reproductive behavior, and whether relationships in adolescent pregnancy among sisters born to adolescent mothers differ from those born to nonadolescent mothers.
Methods:
We followed a birth cohort in Manitoba, Ontario, Canada, to age 20 using linkable administrative databases housed at the Manitoba Centre for Health Policy. The cohort consisted of 12 391 girls born in Manitoba between April 1, 1984, and March 31, 1996, who had 1 older sister. We used logistic regression models to examine the relationships among familial adolescent pregnancy outcomes.
Results:
Compared with adolescent girls whose older sister did not have an adolescent pregnancy, adolescent girls whose older sister had an adolescent pregnancy were more likely to have a pregnancy (adjusted odds ratio [aOR] = 2.57), regardless of whether that pregnancy was completed (aOR = 2.56) or terminated (aOR = 2.59). Relationships in adolescent pregnancy among sisters were much stronger for those born to nonadolescent mothers (aOR = 3.16 [older sister completed adolescent pregnancy] and 3.18 [older sister terminated adolescent pregnancy]) than to adolescent mothers (aOR = 1.65 [older sister completed adolescent pregnancy] and 1.77 [older sister terminated adolescent pregnancy]). For younger sisters having an adolescent pregnancy, the odds of her completing the pregnancy were reduced if her older sister had terminated an adolescent pregnancy and her mother had not been an adolescent mother (aOR = 0.38).
Conclusions:
Younger sisters of adolescents who had a pregnancy may benefit from targeted interventions to reduce their likelihood of adolescent pregnancies.
An adolescent girl’s socioeconomic environment plays a substantial role in her chances of pregnancy. Living in low-income neighborhoods or having a friend or family member with an adolescent pregnancy increases the risk of pregnancy. 1,2 Adolescent motherhood has health and social consequences for both mother and child. Young mothers have higher rates of postpartum depression than older mothers, and their children are more likely to be born preterm and have a lower birth weight than children born to older mothers. 3,4 Compared with older mothers and their children, adolescent mothers and their offspring tend to have lower levels of education and lower rates of employment. 5,6 Studies of pregnant adolescent girls in Brazil and New Zealand found that those who ended their pregnancies were more likely to graduate from high school and to be better off economically than those who completed their pregnancies. 7,8 Additionally, in Sweden, social norms and attitudes of family members about adolescent pregnancy were found to strongly influence adolescent girls’ decision to become an adolescent mother. 9
Female family members affect both the likelihood of adolescent pregnancy and the outcome of that pregnancy. The likelihood of adolescent pregnancy increases when an adolescent has both (1) a mother who was an adolescent mother and (2) an older sister who had an adolescent pregnancy; however, the latter is the stronger influence. 10 This influence is attributable to social learning, shared parenting influences, and shared societal risk. 11 Adolescent mothers often raise their children in lower-income neighborhoods, which is also associated with early childbearing. 12
We examined the odds of pregnancy and pregnancy completion during adolescence among younger sisters by posing the following questions: (1) Are younger sisters more likely to have an adolescent pregnancy if their older sister had an adolescent pregnancy or if they were born to adolescent mothers? (2) Do the odds of adolescent pregnancy in the younger sister differ by whether the older sister’s adolescent pregnancy was terminated or resulted in a birth? (3) Does an older sister’s adolescent pregnancy outcome affect the younger sister’s odds of becoming an adolescent mother (as opposed to terminating that pregnancy)? and (4) Do these relationships differ among sisters born to mothers who had their first child as an adolescent compared with those born to mothers who had their first child at age ≥20? We used a population-based cohort to examine these questions and contribute to the literature on adolescent reproduction.
Methods
Setting
The rate of adolescent pregnancy (ie, girls aged 15-19) in the Canadian province of Manitoba, Ontario, exceeds the national Canadian average. In 2010, the adolescent pregnancy rate in Canada was 28.2 per 1000 adolescent girls; in Manitoba, the rate was 48.7 per 1000 adolescent girls. The adolescent pregnancy termination rate was also higher in Manitoba (19.1 per 1000 adolescent girls) than in Canada overall (14.7 per 1000 adolescent girls). 13 Globally, the teen pregnancy rate per 1000 adolescent girls in 2010 was slightly lower in Manitoba than in the United States (57.4) and in England and Wales (54.6) but higher than in Australia (34.0). 14 –16 In Manitoba, females of all ages have legal, safe, and free access to pregnancy termination; girls aged <18 do not require consent from a parent or guardian to terminate their pregnancy. 17 Although abortions are legal, access to abortions in Manitoba is limited, particularly in rural areas. 18 The rate of adolescent pregnancy termination per 1000 adolescent girls was higher in Manitoba than in the United States (15 in 2010) and similar to the rates in England and Wales (20 in 2011) and Australia (19 in 2010). 16,19
Data
The Manitoba Population Research Data Repository (hereinafter, the Repository) contains province-wide, routinely collected data on all people who are insured by the provincial government. 20 Health variables are measured continually from physician claims and hospital abstracts (as long as an individual remains in Manitoba). Among the data sets within the Repository, we linked data from the provincial health registry, physician claims, hospital discharge abstracts, educational achievement, child protective services (ie, Child and Family Services), and area-level income measures. 21 We identified sisters using their mother’s health registration number.
Aside from residents insured by the federal government (eg, military personnel and federal inmates, which account for <0.5% of the provincial population), the Manitoba Research Registry identifies all provincial residents. 22 Approximately 16 000 children are born annually, making follow-up in the Repository (about 74% during 20 years) comparable with that of the largest birth cohort studies based on primary data. Data linkage, confidentiality and privacy, and validity are described elsewhere. 23
Cohort Formation
Our analysis included women born between April 1, 1984, and March 31, 1996 (n = 129 085). This period provided a cohort of young women who stayed in the province until at least their 20th birthday, had 1 older sister, and had no missing values for mother’s age at birth and neighborhood income quintile. We included only women who had pregnancies when they were aged 12-19. We were interested in pregnancies that were completed (ie, live or still birth) or terminated; we excluded families in which 1 sister had an adolescent pregnancy that was ectopic or resulted in a miscarriage or intrauterine birth. A total of 12 391 young women remained in the cohort (Figure).
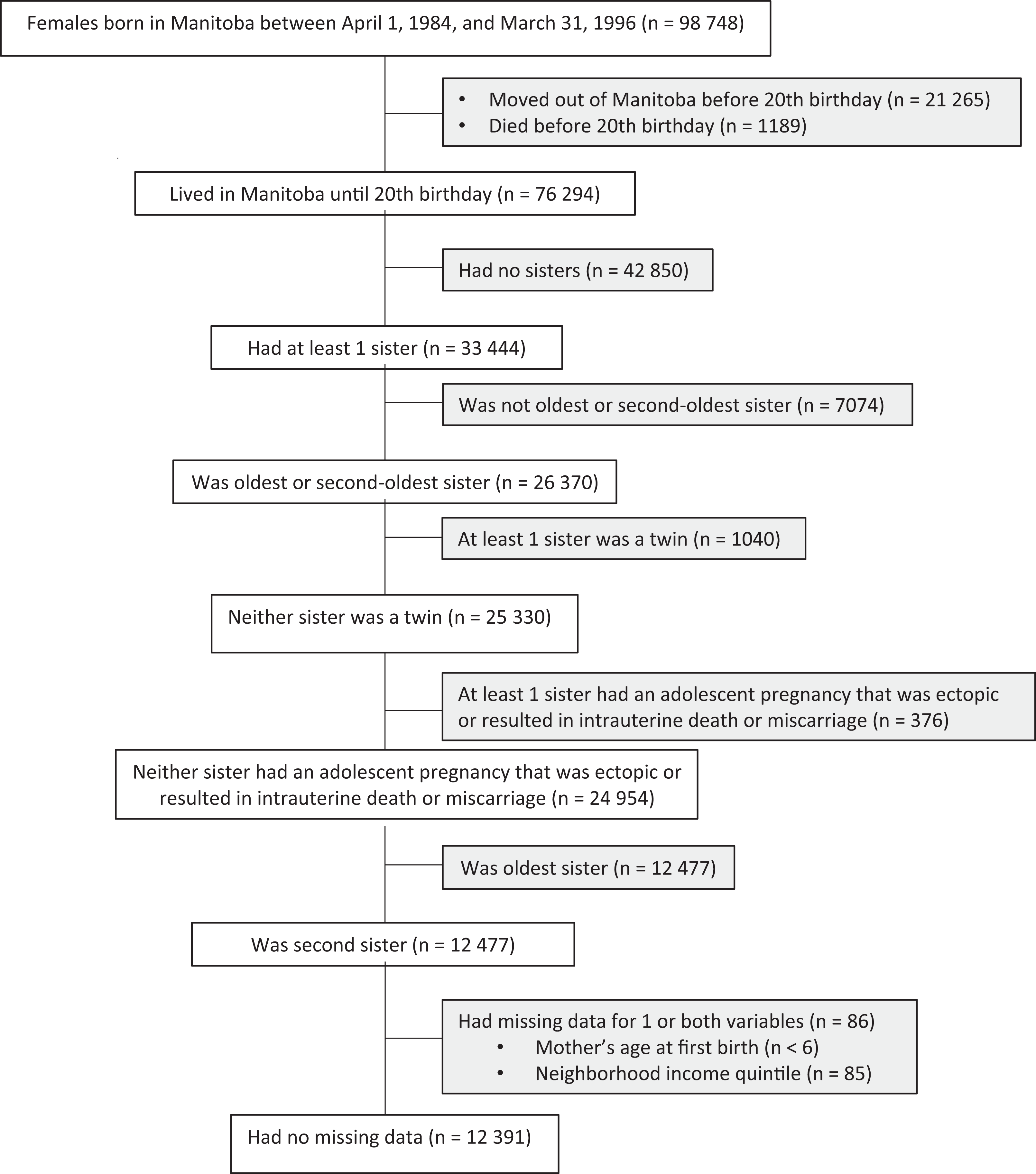
Selection of adolescent girls in a study of adolescent pregnancy among girls aged 12-19, older sisters, and mothers, Manitoba, Canada, 1996-2016. Shaded boxes indicate excluded data.
Variables
Outcome
We determined pregnancy status by using International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) codes (for pregnancies before April 1, 2004) and International Statistical Classification of Diseases and Related Health Problems, Tenth Revision, Canada (ICD-10-CA) and Canadian Classification of Health Intervention (CCI) codes (for pregnancies on or after April 1, 2004) in the hospital discharge abstract database. 24 –26 The ICD-10-CA and CCI codes for pregnancy-related diagnoses are more specific than the ICD-9-CM codes (eg, the trimester of a diagnosis is indicated) but are comparable with ICD-9-CM codes for our purposes. 27 We examined only the first pregnancy in adolescents aged 12-19, and we classified them as either completed (ie, live or still birth) or terminated.
Independent variables
The independent variables of interest were (1) whether the oldest sister had an adolescent pregnancy, (2) the outcome of that pregnancy (completed or terminated), and (3) the age of the mother at the time of her first birth (age <20 [adolescent mother] or age ≥20 [nonadolescent mother]).
Covariates
Based on a review of the literature and the availability of variables in the database, we included several key variables describing neighborhood, maternal, and individual characteristics. 2,28 –30 Neighborhood variables were (1) income quintiles (from 1 = lowest income [<$30 308/year] to 5 = highest income [>$55 910/year]) for the younger sister’s neighborhood of residence at birth and on her 12th birthday (with different sets of quintiles for urban and rural populations) and (2) geographic region (urban, rural south, and rural mid/north) of the neighborhood at both dates. In Manitoba, the geographic regions refer to neighborhoods that are urban (>10 people/km2), rural south (1-9 people/km2), or rural mid/north (<1 person/km2). The models also adjusted for mother’s marital status at the time of the younger sister’s birth. We collected data on the following characteristics of the younger sister: whether she had ≥2 mental health diagnoses, moved ≥2 times, or had a change in family structure (ie, parental divorce, death, marriage, remarriage) before her 12th birthday. Mental health diagnoses were defined by ICD-9-CM codes (290-319) before April 1, 2004, and ICD-10-CA codes (F01-F99) after April 1, 2004. For the purposes of this study, ≥2 mental health diagnoses indicated a mental health condition, ≥2 moves (a change in 6-digit postal code) indicated residential mobility, and a change in family structure between birth and her 12th birthday indicated a change in family structure. Because the birth of this cohort spanned 11 years, we included the birth year of the younger sister to account for changes in social norms or perceptions among adolescents toward sexual relationships and reproductive health. In analyzing outcomes among those who had an adolescent pregnancy, we also included the age of the younger sister at the time of pregnancy.
Young women in the care of Child and Family Services are more likely to become pregnant than young women not in the care of Child and Family Services. 31 The recent linkage of Child and Family Services data (starting in 1992) to the Manitoba Research Registry limits the time frame and birth cohorts in which this measure can be observed; this variable is available for all girls starting at age 8. With adolescent pregnancy being examined between ages 12 and 19, we measured the variable for being in Child and Family Services care between a girl’s 8th and 12th birthdays.
Analysis
We studied the association between a younger sister’s adolescent pregnancy and the adolescent reproductive outcomes of older female family members by using 3 logistic regression models. The first model examined the association between a younger sister having an adolescent pregnancy and her older sister having an adolescent pregnancy. The second model analyzed the association between a younger sister having an adolescent pregnancy and her older sister’s adolescent reproductive outcome (ie, no pregnancy, terminated pregnancy, completed pregnancy). The third model analyzed the relationship between a younger sister having an adolescent pregnancy and her mother having been an adolescent mother.
A second set of analyses examined the odds of pregnancy completion and included only younger sisters who had an adolescent pregnancy. Again, we examined the associations of this outcome with her older sister having had an adolescent pregnancy, her older sister’s adolescent reproductive outcome, and her mother having been an adolescent mother.
Next, we studied the possible interaction between the older sister’s reproductive outcome and the mother’s adolescent motherhood status vis-a-vis the adolescent reproductive outcomes of the younger sister (first pregnancy, then pregnancy completion). We first obtained odds ratios from each logistic regression without covariates (unadjusted odds ratio), and then we adjusted the model for all covariates (adjusted odds ratio [aOR]). We used the Wald χ2 test and considered P < .05 to be significant. We performed all data management, programming, and analyses using SAS version 9.4. 32
Results
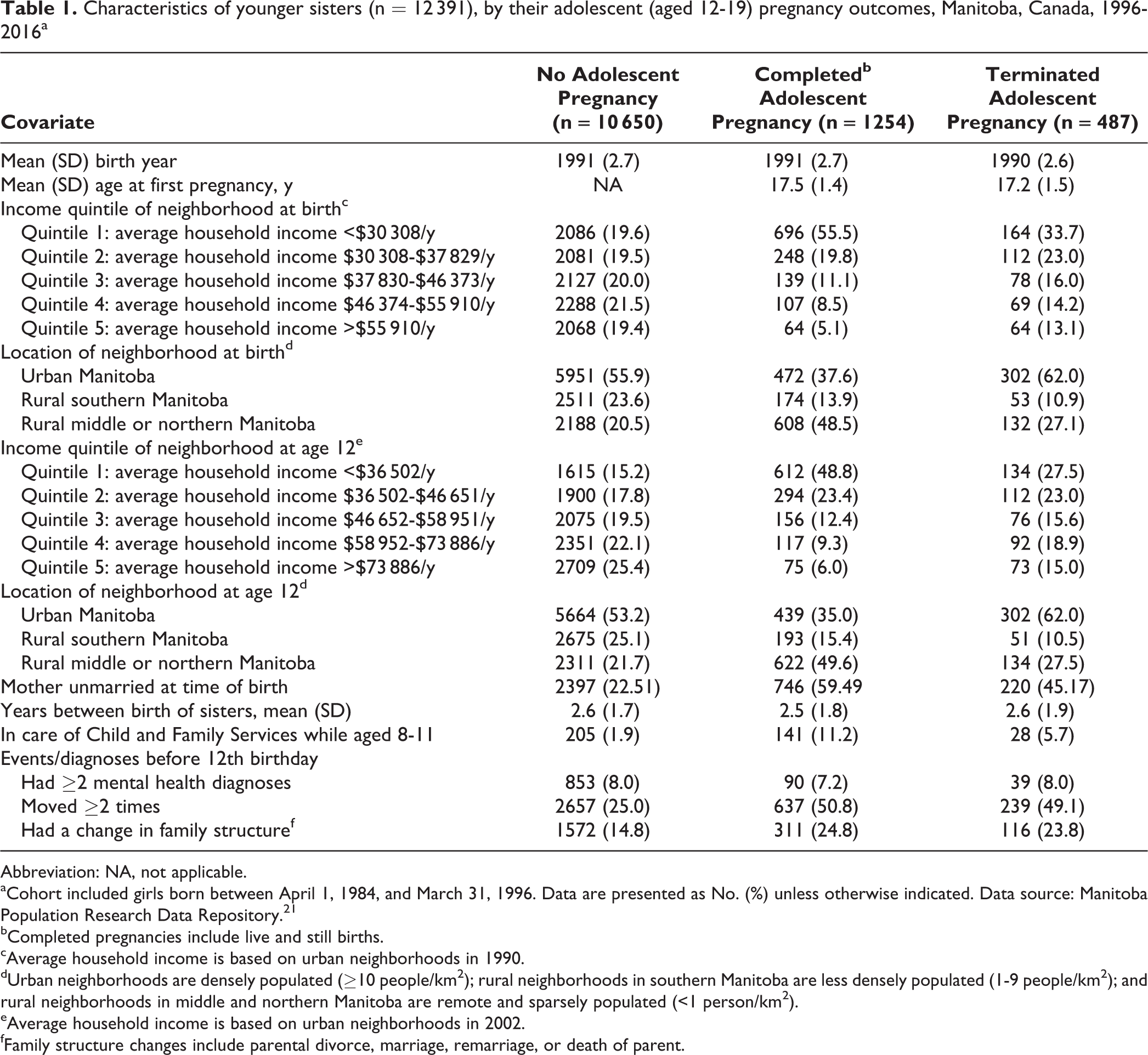
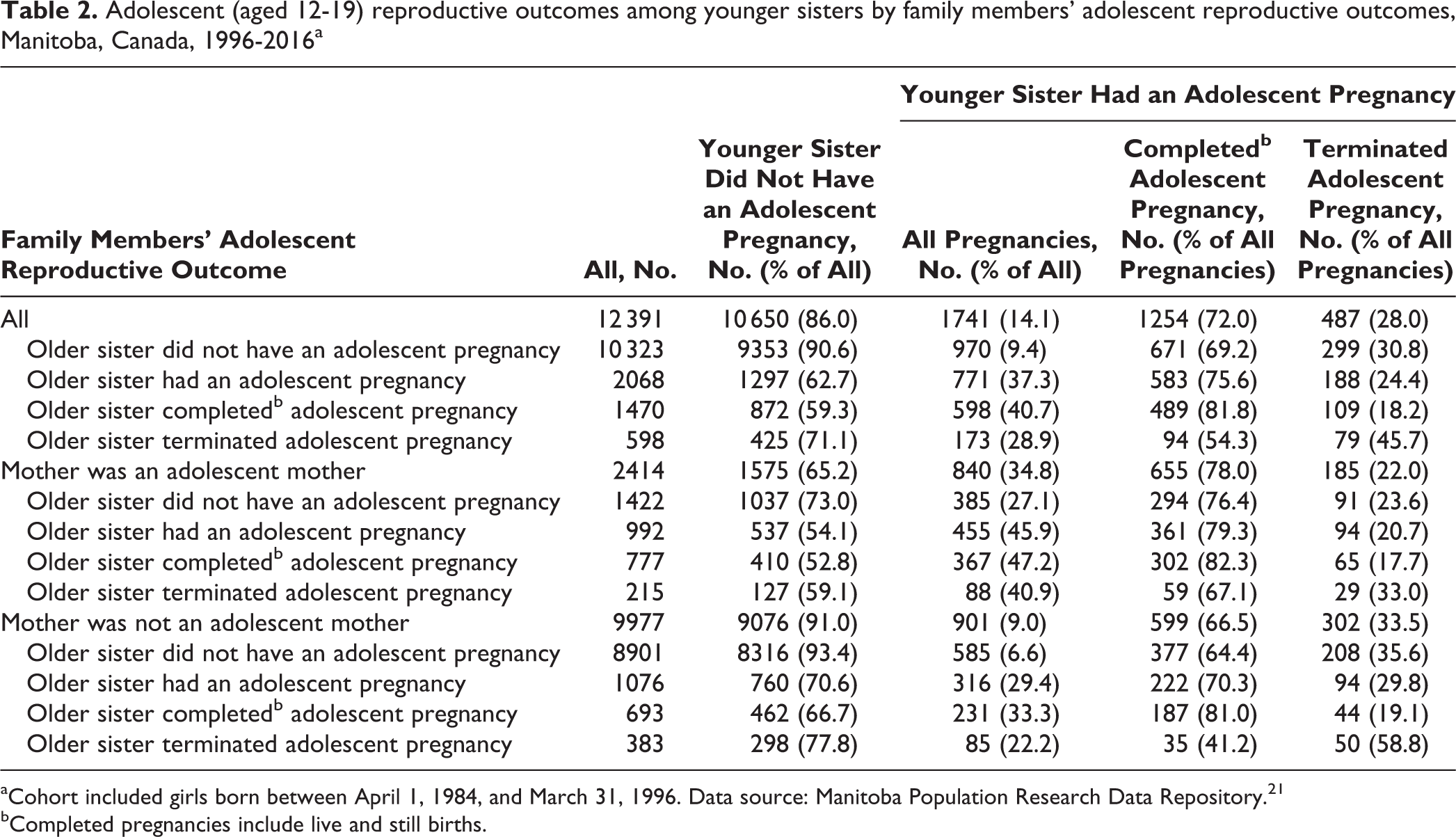
Of 12 391 younger sisters in the cohort, 1741 (14.1%) had a pregnancy, of which 1254 (72.0%) were completed (Table 1). Among younger sisters, adolescent pregnancy was more common among those born to adolescent mothers (840/2414, 34.8%) than to nonadolescent mothers (901/9977, 9.0%). Younger sisters had higher rates of adolescent pregnancy if their older sisters had an adolescent pregnancy (771/2068, 37.3%) than if their older sisters did not have an adolescent pregnancy (970/10 323, 9.4%) (Table 2). Pregnancy completion among younger sisters who had an adolescent pregnancy occurred more often among those with adolescent mothers (655/840, 78.0%) than among those with nonadolescent mothers (599/901, 66.5%). Among younger sisters who had an adolescent pregnancy, more pregnancies were completed if their older sisters completed an adolescent pregnancy (489/598, 81.8%) or did not have an adolescent pregnancy (671/970, 69.2%) than if their older sister terminated an adolescent pregnancy (94/173, 54.3%).
Characteristics of younger sisters (n = 12 391), by their adolescent (aged 12-19) pregnancy outcomes, Manitoba, Canada, 1996-2016a
Abbreviation: NA, not applicable.
aCohort included girls born between April 1, 1984, and March 31, 1996. Data are presented as No. (%) unless otherwise indicated. Data source: Manitoba Population Research Data Repository. 21
bCompleted pregnancies include live and still births.
cAverage household income is based on urban neighborhoods in 1990.
dUrban neighborhoods are densely populated (≥10 people/km2); rural neighborhoods in southern Manitoba are less densely populated (1-9 people/km2); and rural neighborhoods in middle and northern Manitoba are remote and sparsely populated (<1 person/km2).
eAverage household income is based on urban neighborhoods in 2002.
fFamily structure changes include parental divorce, marriage, remarriage, or death of parent.
Adolescent (aged 12-19) reproductive outcomes among younger sisters by family members’ adolescent reproductive outcomes, Manitoba, Canada, 1996-2016a
aCohort included girls born between April 1, 1984, and March 31, 1996. Data source: Manitoba Population Research Data Repository. 21
bCompleted pregnancies include live and still births.
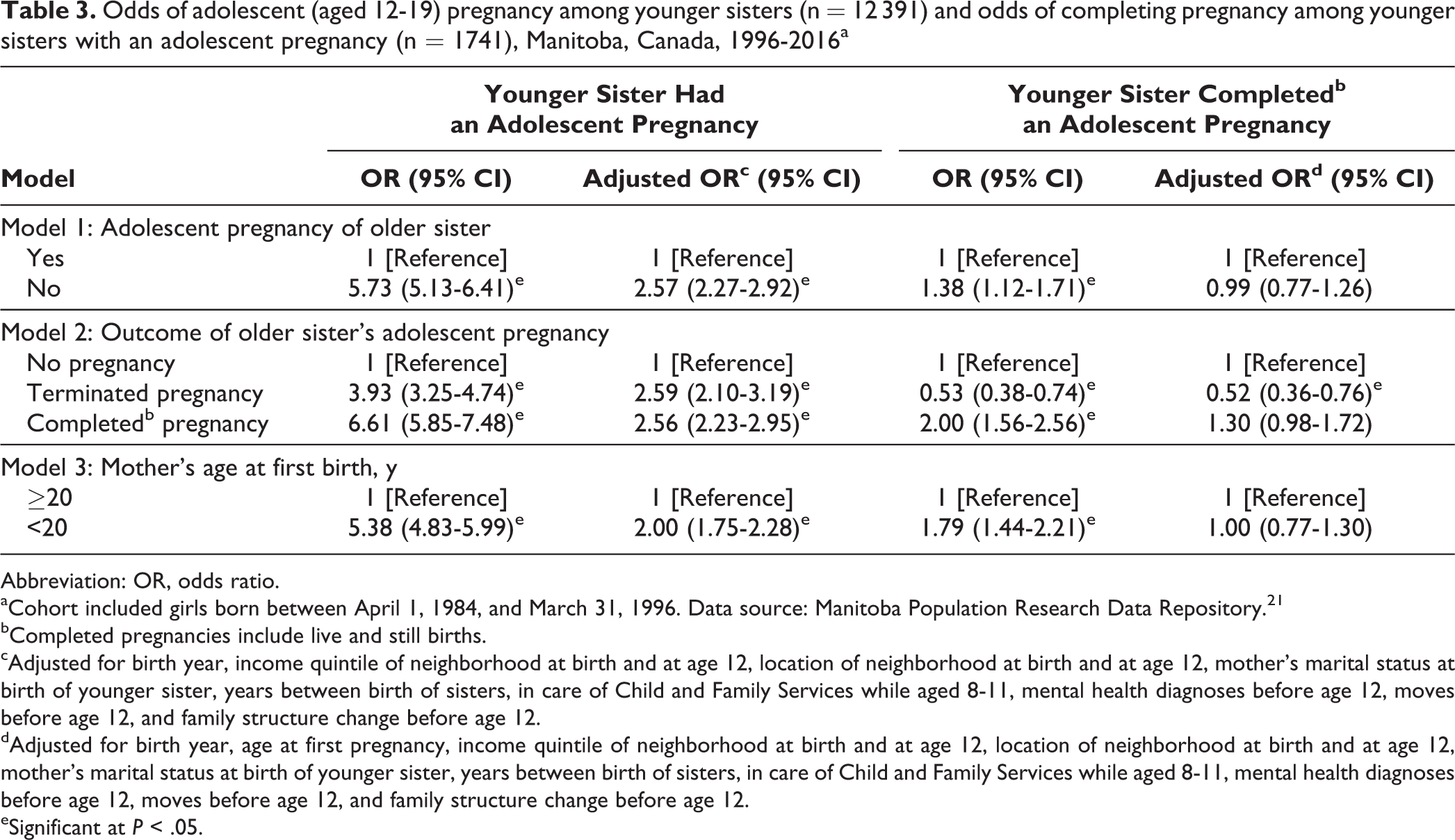
The odds of a younger sister having an adolescent pregnancy were significantly higher if her older sister had an adolescent pregnancy (aOR = 2.57; 95% confidence interval [CI], 2.27-2.92) than if her older sister did not have an adolescent pregnancy. This finding was true whether that pregnancy was completed (aOR = 2.56; 95% CI, 2.23-2.95) or terminated (aOR = 2.59; 95% CI, 2.10-3.19) (Table 3). A younger sister was also twice as likely to have an adolescent pregnancy if born to an adolescent mother compared with a nonadolescent mother (aOR = 2.00; 95% CI, 1.75-2.28). Among younger sisters who had an adolescent pregnancy, having an older sister who terminated an adolescent pregnancy decreased their likelihood of completing that pregnancy (aOR = 0.52; 95% CI, 0.36-0.76).
Odds of adolescent (aged 12-19) pregnancy among younger sisters (n = 12 391) and odds of completing pregnancy among younger sisters with an adolescent pregnancy (n = 1741), Manitoba, Canada, 1996-2016a
Abbreviation: OR, odds ratio.
aCohort included girls born between April 1, 1984, and March 31, 1996. Data source: Manitoba Population Research Data Repository. 21
bCompleted pregnancies include live and still births.
cAdjusted for birth year, income quintile of neighborhood at birth and at age 12, location of neighborhood at birth and at age 12, mother’s marital status at birth of younger sister, years between birth of sisters, in care of Child and Family Services while aged 8-11, mental health diagnoses before age 12, moves before age 12, and family structure change before age 12.
dAdjusted for birth year, age at first pregnancy, income quintile of neighborhood at birth and at age 12, location of neighborhood at birth and at age 12, mother’s marital status at birth of younger sister, years between birth of sisters, in care of Child and Family Services while aged 8-11, mental health diagnoses before age 12, moves before age 12, and family structure change before age 12.
eSignificant at P < .05.
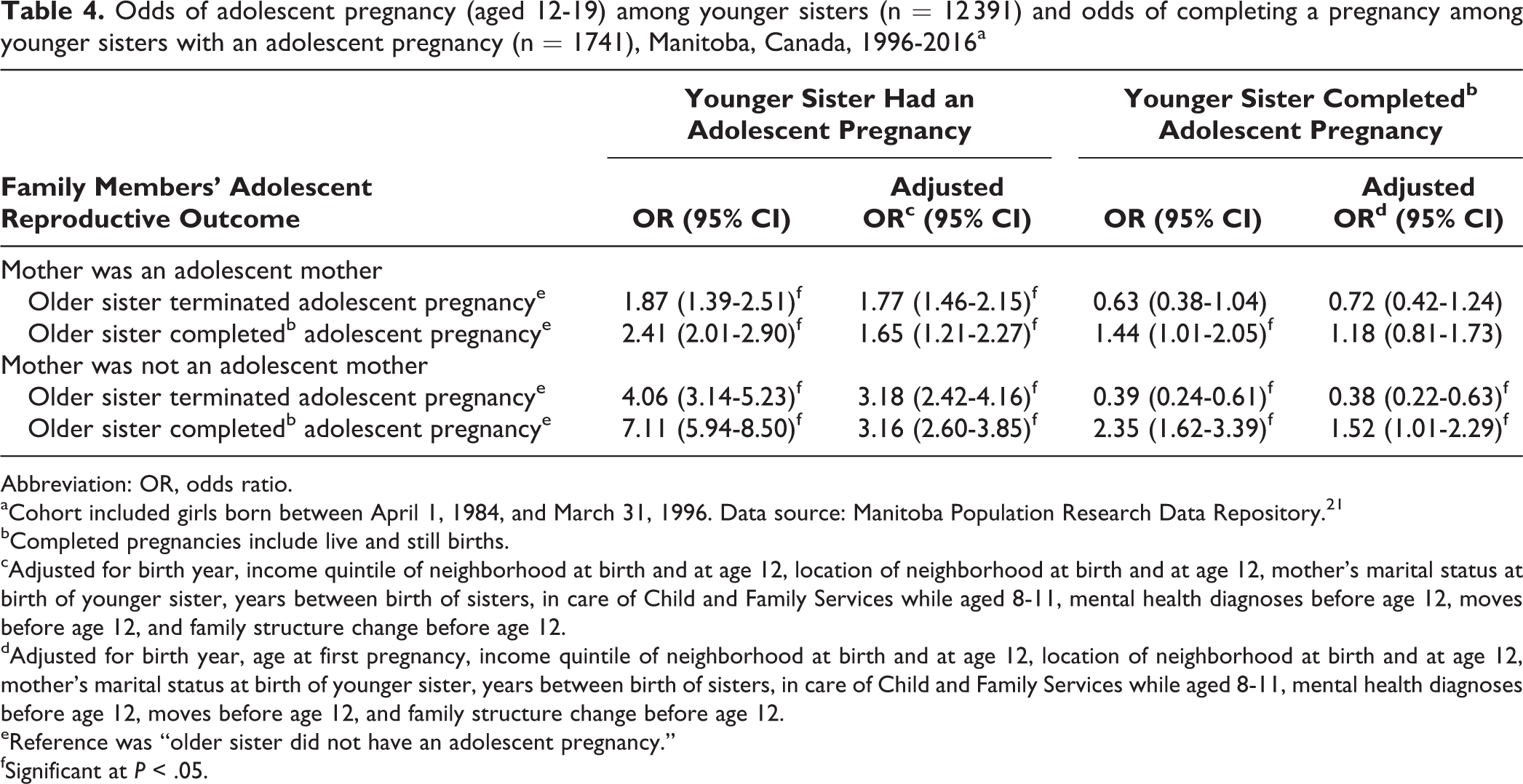
Adding the interaction term tested whether maternal age at first birth moderated the relationship between sisters’ adolescent pregnancies and pregnancy outcomes. Among younger sisters born to nonadolescent mothers, having an older sister with an adolescent pregnancy significantly increased the odds of the younger sister’s adolescent pregnancy regardless of whether that pregnancy was completed (aOR = 3.16; 95% CI, 2.60-3.85) or terminated (aOR = 3.18; 95% CI, 2.42-4.16). For sisters born to adolescent mothers, having an older sister who had an adolescent pregnancy also increased the likelihood of the younger sister having an adolescent pregnancy, regardless of whether the older sister terminated her pregnancy (aOR = 1.65; 95% CI, 1.21-2.27) or completed it (aOR = 1.77; 95% CI, 1.46-2.15). The relationships between sisters’ adolescent pregnancy outcomes were not as strong for sisters born to adolescent mothers as for sisters born to nonadolescent mothers (Table 4).
Odds of adolescent pregnancy (aged 12-19) among younger sisters (n = 12 391) and odds of completing a pregnancy among younger sisters with an adolescent pregnancy (n = 1741), Manitoba, Canada, 1996-2016a
Abbreviation: OR, odds ratio.
aCohort included girls born between April 1, 1984, and March 31, 1996. Data source: Manitoba Population Research Data Repository. 21
bCompleted pregnancies include live and still births.
cAdjusted for birth year, income quintile of neighborhood at birth and at age 12, location of neighborhood at birth and at age 12, mother’s marital status at birth of younger sister, years between birth of sisters, in care of Child and Family Services while aged 8-11, mental health diagnoses before age 12, moves before age 12, and family structure change before age 12.
dAdjusted for birth year, age at first pregnancy, income quintile of neighborhood at birth and at age 12, location of neighborhood at birth and at age 12, mother’s marital status at birth of younger sister, years between birth of sisters, in care of Child and Family Services while aged 8-11, mental health diagnoses before age 12, moves before age 12, and family structure change before age 12.
eReference was “older sister did not have an adolescent pregnancy.”
fSignificant at P < .05.
For younger sisters who had an adolescent pregnancy, their odds of completing that pregnancy were affected by their older sister’s adolescent reproductive outcome only when they were born to nonadolescent mothers. When born to nonadolescent mothers, younger sisters who had an adolescent pregnancy were less likely to complete their pregnancy if their older sister had terminated such a pregnancy (aOR = 0.38; 95% CI, 0.22-0.63) and more likely to complete their pregnancy if their older sister had completed such a pregnancy (aOR = 1.52; 95% CI, 1.01-2.29) (Table 4).
Discussion
Sisters and daughters of adolescent mothers are at greater risk for adolescent pregnancy than those who did not have female family members with adolescent pregnancies. 10,11,33 Social learning and modeling theories suggest that younger sisters are more likely to become pregnant if their older sister was an adolescent mother and are more likely to “(a) accept premarital sexual intercourse as the norm and (b) accept single parenthood as a way to achieve adult status” than if their older sister was not an adolescent mother. 11
In our study, pregnancy rates were highest when both mother and older sister had completed an adolescent pregnancy and lowest when neither the mother nor the older sister had been adolescent mothers. A smaller Australian study found that of adolescent girls who terminated their pregnancy, 15.0% had a sister who terminated her pregnancy, whereas only 10.8% of those who completed their pregnancy had a sister who had terminated a pregnancy. Additionally, daughters born to adolescent mothers were less likely than daughters born to nonadolescent mothers to terminate their adolescent pregnancy. 34
In our study, adolescent pregnancy completion among younger sisters was affected by the older sisters’ adolescent pregnancy outcomes only if the sisters were born to nonadolescent mothers. This finding could be explained by the fact that sisters born to nonadolescent mothers are more likely to live in neighborhoods with higher socioeconomic status, where adolescent pregnancies are uncommon, whereas sisters born to adolescent mothers are more likely to live in neighborhoods with lower socioeconomic status, where adolescent pregnancies are more common. For younger sisters who have less exposure to adolescent pregnancies in their neighborhood, the adolescent pregnancy of an older sister may be more influential for younger sisters born to nonadolescent mothers than for younger sisters born to adolescent mothers.
Strengths and Limitations
This study had several strengths. First, our use of linkable administrative data allowed us to follow a large birth cohort, with outcomes that were free from measurement biases often associated with survey data. 35 Another strength was our use of 2 waves of measurement for important covariates (region and urban/rural residence, neighborhood income quintile) to provide pretest information. 36
This study also had several limitations. First, data on certain covariates and mediating effects, such as measures associated with the decision to terminate a pregnancy (eg, personality, attitudes of people around them, culture, public policy, and partner violence), were unavailable in administrative data. Failing to adjust for these confounders may have inflated the association between exposure and outcome. 37 Second, our primary measure of socioeconomic status (neighborhood-level income) is associated with the adolescent’s environment but does not perfectly measure it. Finally, some of the pregnancy and pregnancy termination risk associated with an older sister’s adolescent reproductive outcome may be related to their shared environments (eg, socioeconomic status of their neighborhood, exposure to adolescent pregnancies) rather than to the behavior itself, which is referred to as misidentification. 37,38
Conclusions
Our findings suggest that family modeling is important. Having an older sister who had an adolescent pregnancy increased the likelihood of a younger sister having an adolescent pregnancy. This finding was true among younger sisters of adolescent mothers and nonadolescent mothers. For younger sisters who had an adolescent pregnancy, modeling of older sisters was seen only among sisters born to nonadolescent mothers. This finding suggests that the social factors associated with being born to an adolescent mother may outweigh the influence of an older sister’s pregnancy outcome. Given the challenges associated with adolescent motherhood, younger sisters whose older sisters had a pregnancy may benefit from targeted interventions to reduce their likelihood of adolescent pregnancy.
Footnotes
Acknowledgments
Data used in this study were from the Population Health Research Data Repository housed at the Manitoba Centre for Health Policy at the University of Manitoba and were derived from data provided by Manitoba Health, Seniors and Active Living, Manitoba Families, and Manitoba Education and Training under project #2013/2014-04. The results and conclusions of this article are those of the authors and do not imply any official endorsement by the Manitoba Centre for Health Policy, Manitoba Health, Seniors and Active Living, or other data providers.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by a Manitoba Training Program in Health Services Research graduate studentship. The funding source had no role in the design and conduct of the study; the collection, management, analysis, and interpretation of data; and the preparation, review, and approval of the manuscript.