
Abstract
Objective:
We estimated the reduction in number of hospitalizations for acute myocardial infarction and stroke as well as the associated health care costs resulting from reducing the number of smokers in the US federal workforce during a 5-year period.
Methods:
We developed a 5-year spreadsheet-based cohort model with parameter values from past literature and analysis of national survey data. We obtained 2015 data on the federal workforce population from the US Office of Personnel Management and data on smoking prevalence among federal workers from the 2013-2015 National Health Interview Survey. We adjusted medical costs and productivity losses for inflation to 2015 US dollars, and we updated future productivity losses for growth. Because of uncertainty about the achievable reduction in smoking prevalence and input values (eg, relative risk for acute myocardial infarction and stroke, medical costs, and absenteeism), we performed a Monte Carlo simulation and sensitivity analysis.
Results:
We estimated smoking prevalence in the federal workforce to be 13%. A 5 percentage-point reduction in smoking prevalence could result in 1106 fewer hospitalizations for acute myocardial infarction (range, 925-1293), 799 fewer hospitalizations for stroke (range, 530-1091), and 493 fewer deaths (range, 494-598) during a 5-year period. Similarly, estimated costs averted would be $59 million (range, $49-$63 million) for medical costs, $332 million (range, $173-$490 million) for absenteeism, and $117 million (range, $93-$142 million) for productivity.
Conclusion:
Reductions in the prevalence of smoking in the federal workforce could substantially reduce the number of hospitalizations for acute myocardial infarction and stroke, lower medical costs, and improve productivity.
Smoking is the leading preventable cause of death in the United States and is responsible for more than 480 000 deaths each year, including an estimated 41 000 deaths resulting from exposure to secondhand smoke. 1 Smoking costs the United States more than $300 billion per year, including almost $170 billion in direct medical care costs and more than $156 billion in lost productivity resulting from premature mortality and exposure to secondhand smoke. 1,2 Nationally, the prevalence of adult smokers declined from 20.9% in 2005 to 15.1% in 2015; despite this reduction, an estimated 40 million people were smokers in the United States in 2015. 3
Employers cover approximately half of employee medical costs. 4 Given the high medical and productivity costs associated with smoking, many employers are interested in encouraging their employees to quit. 5 The federal government, with more than 2 million employees, is the largest employer in the United States. 6 We estimated that 13.0% (95% confidence interval [CI], 11.5%-14.4%) of federal workers (or approximately 260 000 people) smoked cigarettes during 2013-2015. 7
Reducing smoking prevalence among federal workers could have positive health outcomes, reduce medical costs, and lower productivity losses, thereby benefiting insurers, the federal government, employees, and, ultimately, taxpayers. Although quitting smoking can lead to many health improvements, one of the immediate effects is a reduction in the risk of acute myocardial infarction and stroke and their associated hospitalizations and deaths. 8 Reductions in each of these adverse health outcomes can have economic impacts via medical costs averted and deaths prevented. Furthermore, people who quit smoking may also have higher productivity through fewer missed workdays. 5,9 To date, estimates of the short-term cardiovascular health and economic effects to employers from smoking cessation have not been calculated.
In this study, we used an evidence-based spreadsheet model to simulate the impact of 2 what-if scenarios: (1) a base-case scenario in which smoking prevalence stays the same and (2) an alternate scenario in which smoking is immediately reduced by 5 (range, 1-6) percentage points. We further estimated the reduction in hospitalizations for acute myocardial infarction and strokes and associated economic impacts.
Methods
Smoking Prevalence in the Federal Workforce
In 2015, among adults aged 20-64, the federal workforce consisted of 1.95 million nonseasonal, full-time and part-time employees. Because of data limitations, we excluded military, intelligence, and postal employees as well as contractors and non–full-time-equivalent fellows. 6 We estimated health impacts only for adults aged 35-64, because few cardiovascular events occur before age 35 and studies on acute myocardial infarction and stroke for recent quitters were limited to these age groups. 1,8,10 We estimated the prevalence of current smoking and former smoking in the federal workforce using data from the National Health Interview Survey (2013-2015). To determine the number of federal workers, we used the class of worker, which lists federal workers as a category, and we weighted our estimates using the adult final annual weights. 7 We defined current smokers as those who reported having smoked ≥100 cigarettes in their lifetime and indicated that they smoked every day or some days. We considered former smokers to be those who reported smoking ≥100 cigarettes in their lifetime and indicated they currently did not smoke.
Estimating the Incidence of Acute Myocardial Infarction and Stroke in the Base-Case and Reduced-Prevalence Scenarios
For those aged 18-34, we did not estimate reductions in acute myocardial infarction and stroke because the impact of smoking on cardiovascular disease is not distinguishable. Therefore, we accounted only for excess absenteeism in this age group. For those aged 35-64, we modeled cardiovascular disease outcomes (acute myocardial infarction and stroke) using a method first described for the US population in 1997 by Lightwood and Glantz. 8 This method was also used in later studies for the United Kingdom in 2000 and Australian populations in 2005. 11,12
To begin, Lightwood and Glantz obtained relative risks for acute myocardial infarction and stroke in current and former smokers from available studies that examined the impact of cessation on cardiovascular outcomes. Five publications met Lightwood and Glantz’s criteria for acute myocardial infarction 13 –17 and 2 met their criteria for stroke. 14,18 In a later study on the Australian population, 1 additional study was used for acute myocardial infarction. 19 Using the aforementioned studies, we followed Lightwood and Glantz by estimating a decline in the relative risk for acute myocardial infarction and stroke from time of quit using an exponential decay:

whereby RR(t) was the relative risk for a quitter to that of a nonsmoker, t months since quitting. RRs was the relative risk of current smokers to nonsmokers. RRf was the relative risk of a former smoker and represented the lowest relative risk possible for a quitter as compared with a nonsmoker, t was the time in months since quitting, and τ was the number of months it took for the relative risk to decrease by a log factor. In our model, all people quit at time zero. Then, we determined how quickly a quitter’s risk would decrease using LnRR(t). The minimum risk for a quitter was RRf . Both Lightwood and Glantz and Hurley fitted sex-specific exponential decay models for acute myocardial infarction. Following Lightwood and Glantz and Hurley, we used a pooled model for stroke (eg, males and females had the same risk of stroke).
To obtain hospitalization rates for recent quitters, we multiplied the relative risk by the current hospitalization rate of acute myocardial infarction and stroke for nonsmokers. Because we could observe only the hospitalization rate for the national population for acute myocardial infarction and stroke, we followed Lightwood and Glantz’s method for estimating the nonsmoker hospitalization rate (Rn ) using the following formula:

Ps and Pf were the proportions of smokers and former smokers in the population, and R 0 was the observed population hospitalization rate. We estimated R 0 for acute myocardial infarction and stroke using data from the 2010 National Hospital Discharge Survey. 20 We assumed that adults aged 35-54 and 55-64 had the same survival probability and that survival probabilities were comparable by smoking status. After estimating the nonsmoker hospitalization rate, we estimated population hospitalization rates of current smokers and recent quitters by multiplying the corresponding relative risk (current smoker, recent quitter) by Rn .
To obtain estimates of premature mortality from acute myocardial infarction and stroke, we applied survival rates from Lightwood and Glantz (Table 1). We assumed that adults aged 35-54 and 55-64 had the same survival probability and that survival probabilities were comparable by smoking status. We also assumed that deaths were evenly distributed over time. We calculated aggregate total reductions in hospitalizations, deaths, and costs as well as health outcomes per 10 000 employees and costs per employee.
Characteristics and epidemiological inputs used to estimate the impact of reducing smoking on cardiovascular disease outcomes among federal employees during a 5-year period
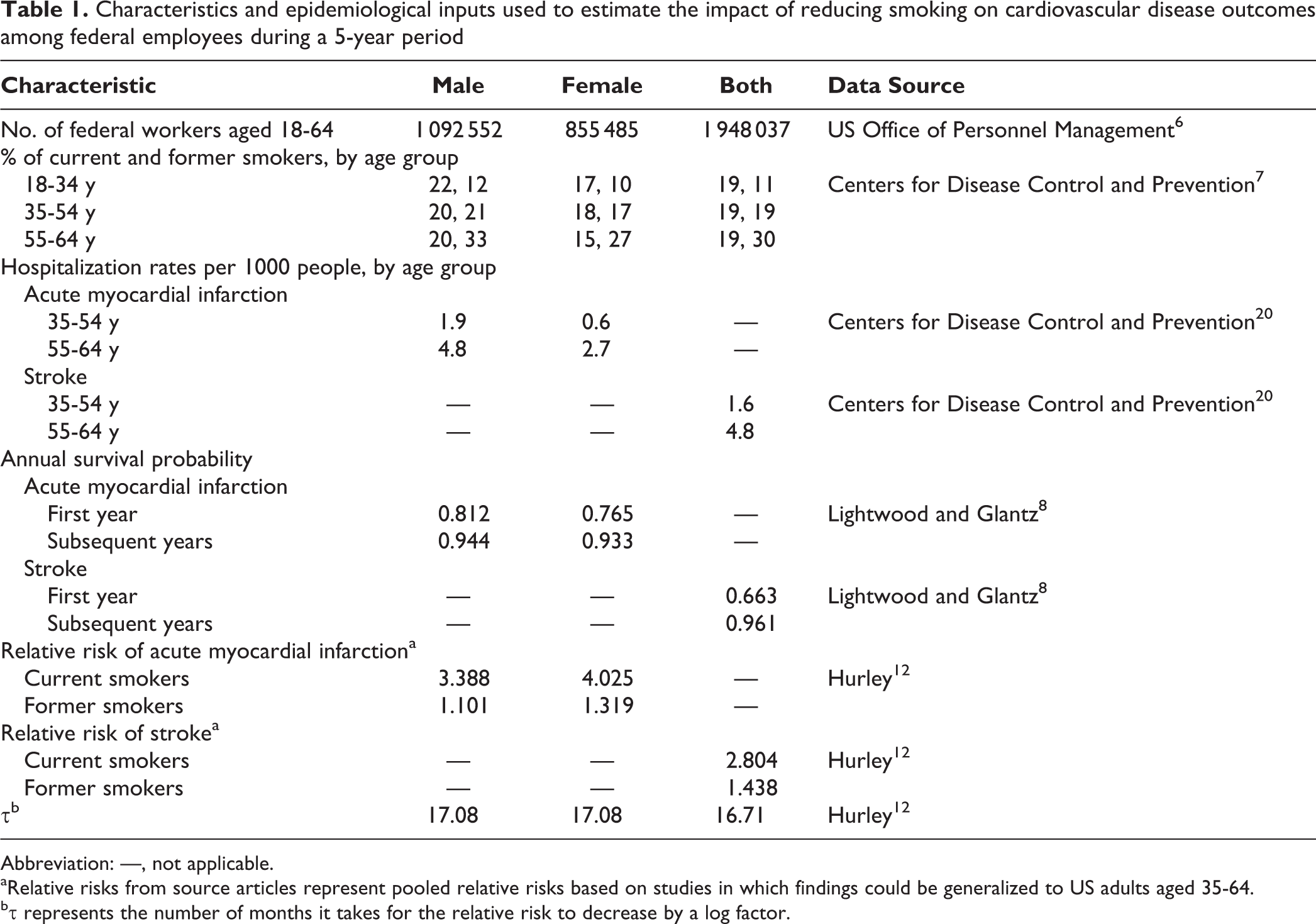
Abbreviation: —, not applicable.
aRelative risks from source articles represent pooled relative risks based on studies in which findings could be generalized to US adults aged 35-64.
bτ represents the number of months it takes for the relative risk to decrease by a log factor.
Medical Costs and Productivity Losses
We included costs for incident hospitalization and absenteeism, ongoing medical costs, and productivity losses associated with premature mortality. We obtained data on incident hospitalization costs associated with acute myocardial infarction and stroke from published studies that estimated costs from the privately insured, employed workforce (Table 2). 21,23 We obtained data on ongoing medical costs (ie, the additional medical costs associated with chronic care after a person has a stroke or acute myocardial infarction) from a published source using the Medical Expenditure Panel Survey. 22 We updated all medical costs to 2015 US dollars using the personal consumption expenditure index for health care. 30
Costs associated with acute myocardial infarction and stroke hospitalizations, productivity losses, absenteeism, and associated inflation and productivity adjustments used in a model estimating the impact of reducing smoking among the federal workforce during a 5-year period
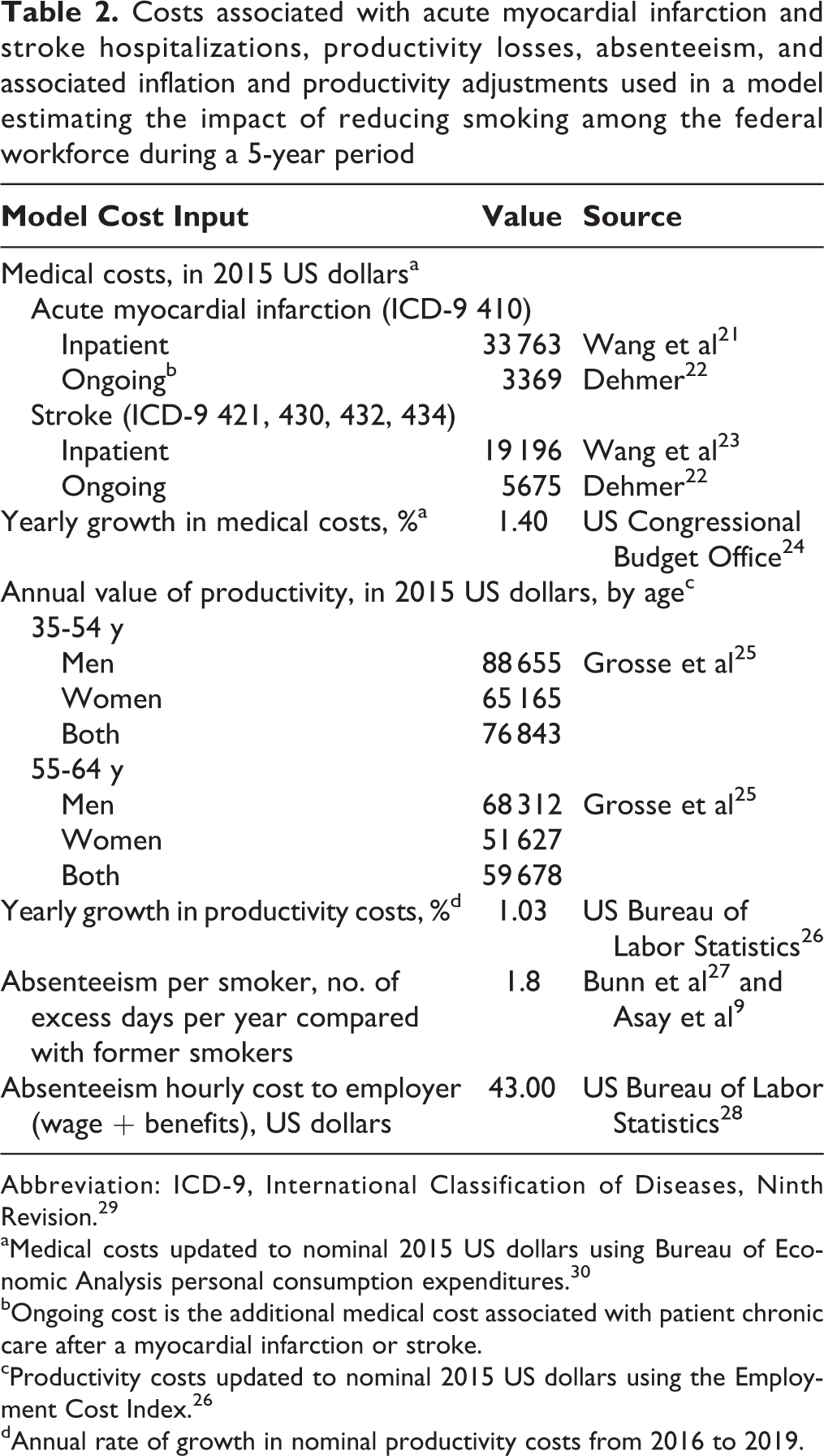
Abbreviation: ICD-9, International Classification of Diseases, Ninth Revision. 29
aMedical costs updated to nominal 2015 US dollars using Bureau of Economic Analysis personal consumption expenditures. 30
bOngoing cost is the additional medical cost associated with patient chronic care after a myocardial infarction or stroke.
cProductivity costs updated to nominal 2015 US dollars using the Employment Cost Index. 26
dAnnual rate of growth in nominal productivity costs from 2016 to 2019.
We assumed that medical costs would grow from 2015 for the next 4 years at the US Congressional Budget Office forecasted estimate of medical cost growth per capita (1.4%). 24 We computed ongoing costs by counting the number of people alive who had a stroke or acute myocardial infarction in current and all previous years and then multiplying by the respective yearly ongoing cost for a maximum of 5 years. A person who had more than 1 hospitalization would incur incident costs for each hospitalization. We conservatively assumed that people had the same ongoing cost regardless of the number of hospitalizations.
We measured the cost of premature mortality using a published study that provided the value of productivity (yearly compensation) by sex and age. 25 We based annual mortality on published survival rates that we incorporated as the percentage of people alive 1 year after an event (acute myocardial infarction or stroke) and then each year thereafter (Table 1). 8,31 We used sex-specific weighted averages of productivity across age groups to estimate the productivity for those aged 35-54 and 55-64. We updated yearly compensation to 2015 dollars using the employment cost index. 26 Furthermore, we adjusted productivity losses averted to reflect future productivity growth by multiplying by the difference between employment cost index and the consumer price index (1.37%). 32
For excess absenteeism, a previous study estimated the difference in absenteeism days between former smokers and current smokers as 1.8 days per year. 27 To compute the total value of days missed, we multiplied the number of people alive each year who smoked in both scenarios by 1.8, then by 8 hours, and finally by the US Bureau of Labor Statistics’ published employee compensation rate for public sector employees ($44.60 per hour). 28 We adjusted absenteeism costs to reflect future productivity growth using the same method as for productivity losses.
Monte Carlo Sensitivity Analysis
To account for uncertainty in the potential reduction in smoking prevalence, we analyzed 3 additional scenarios: a 1 percentage-point reduction (8.9% relative change), a 3 percentage-point reduction (26.5% relative change), and a 6 percentage-point reduction (53.0% relative change). Furthermore, because of the uncertainty of model parameters (eg, magnitude of ongoing medical costs and relative risks of acute myocardial infarction and stroke), we performed a Monte Carlo sensitivity analysis using @RISK 6.3 around each prevalence reduction. 33 To reflect uncertainty in ongoing medical costs, we used a uniform distribution 50% above and below the base-case ongoing cost values (acute myocardial infarction and stroke). We assumed that the relative risks of acute myocardial infarction and stroke followed a beta general distribution with mean equal to the base-case value. For acute myocardial infarction, the 5th and 95th percentiles of the relative risk beta distribution were 2.96 and 3.81 for men and 3.60 and 4.45 for women. For stroke, the 5th and 95th percentiles for the relative risk beta distribution were 2.47 and 3.14 for both men and women. 12 Finally, we varied the excess absenteeism associated with smoking between 0.6 and 2.3 days per year. 9 In our simulation, we conducted 5000 iterations and derived 95% credible regions for all outcomes, which we used as plausible upper and lower bounds for reductions in morbidity and mortality as well as averted costs. We evaluated outcomes as the mean and 95% credible region of the final distributions from the Monte Carlo sensitivity analysis.
Results
During a 5-year period, a 5 percentage-point reduction in smoking in the federal workforce with a population of 1.95 million workers (aged 20-64) would result in approximately 97 000 additional quitters, 1106 fewer hospitalizations for acute myocardial infarction (range, 925-1293), 799 fewer hospitalizations for stroke (range, 530-1091), and 493 fewer premature deaths (range, 494-598) (Table 3).
Total health and economic improvements from reducing the prevalence of smoking in the federal workforce during a 5-year perioda
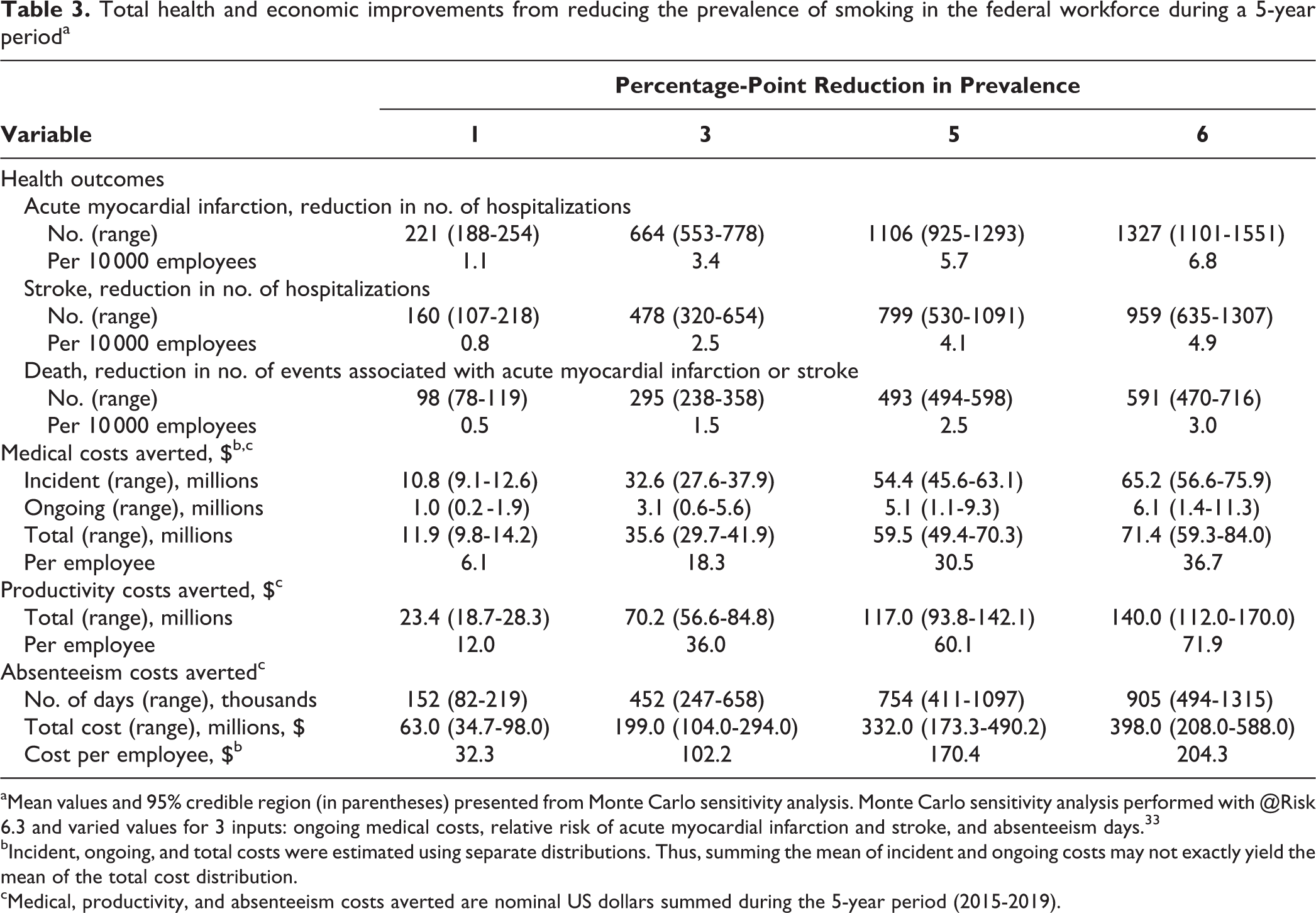
aMean values and 95% credible region (in parentheses) presented from Monte Carlo sensitivity analysis. Monte Carlo sensitivity analysis performed with @Risk 6.3 and varied values for 3 inputs: ongoing medical costs, relative risk of acute myocardial infarction and stroke, and absenteeism days. 33
bIncident, ongoing, and total costs were estimated using separate distributions. Thus, summing the mean of incident and ongoing costs may not exactly yield the mean of the total cost distribution.
cMedical, productivity, and absenteeism costs averted are nominal US dollars summed during the 5-year period (2015-2019).
Medical costs could be reduced by $59.4 million (range, $50.7-$68.8 million), absenteeism by 754 000 (range, 411 000-1 097 000) days, and absenteeism costs by $332.0 million (range, $173.3-$490.2 million). Finally, productivity costs averted from reduced premature mortality totaled $117.0 million (range, $93.8-$142.1 million). Because the relative risk of acute myocardial infarction and stroke decreases over time since quitting smoking, yearly estimated reductions in acute myocardial infarction, stroke, and deaths would increase over time (Figure 1). Similarly, medical costs and productivity losses averted would increase during a 5-year period (Figure 2).
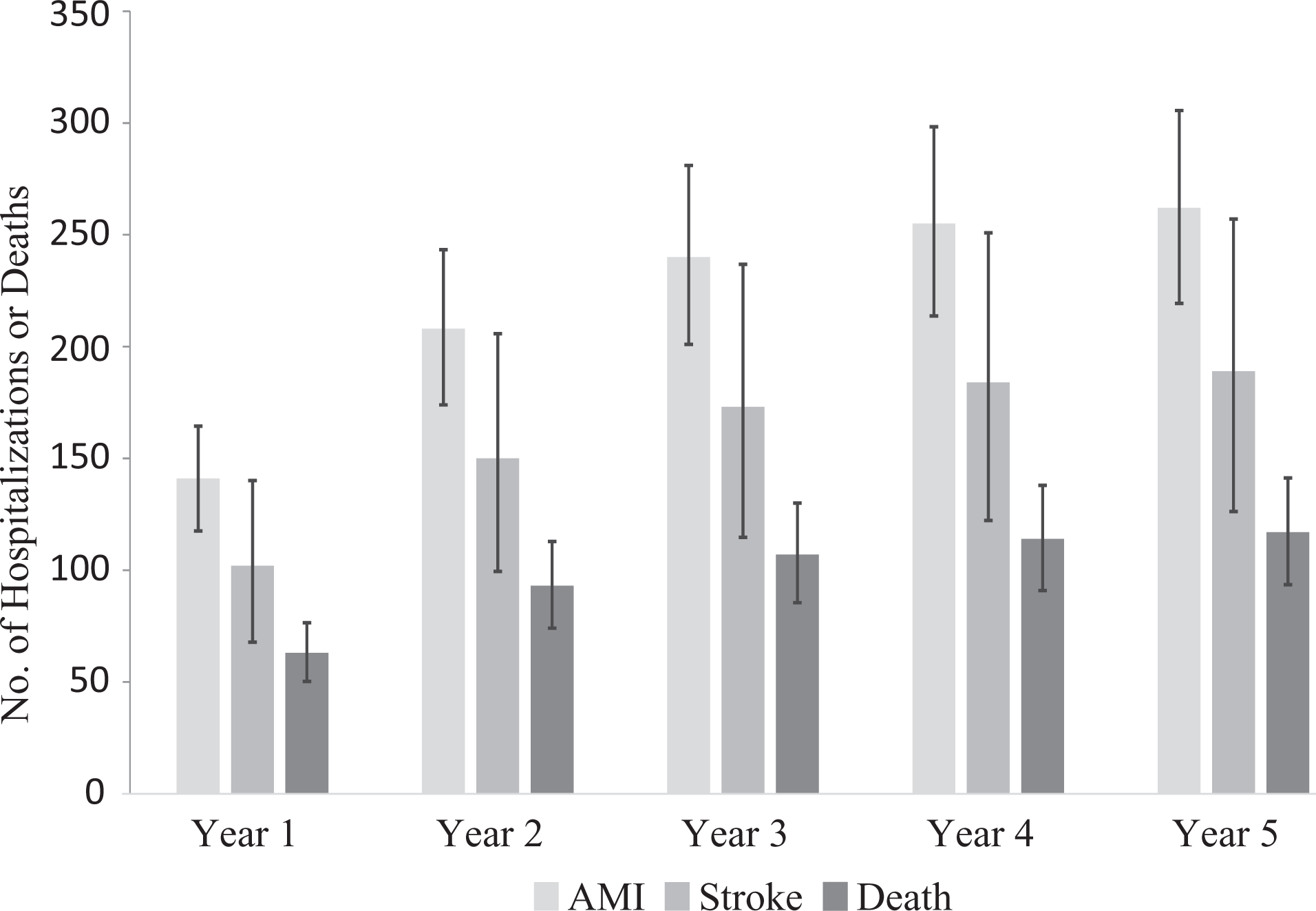
US federal workforce predicted reductions in the number of hospitalizations for acute myocardial infarction (AMI) and stroke and the number of deaths, after a 5 percentage-point reduction in smoking, 2015-2019. Error bars indicate 95% confidence intervals.
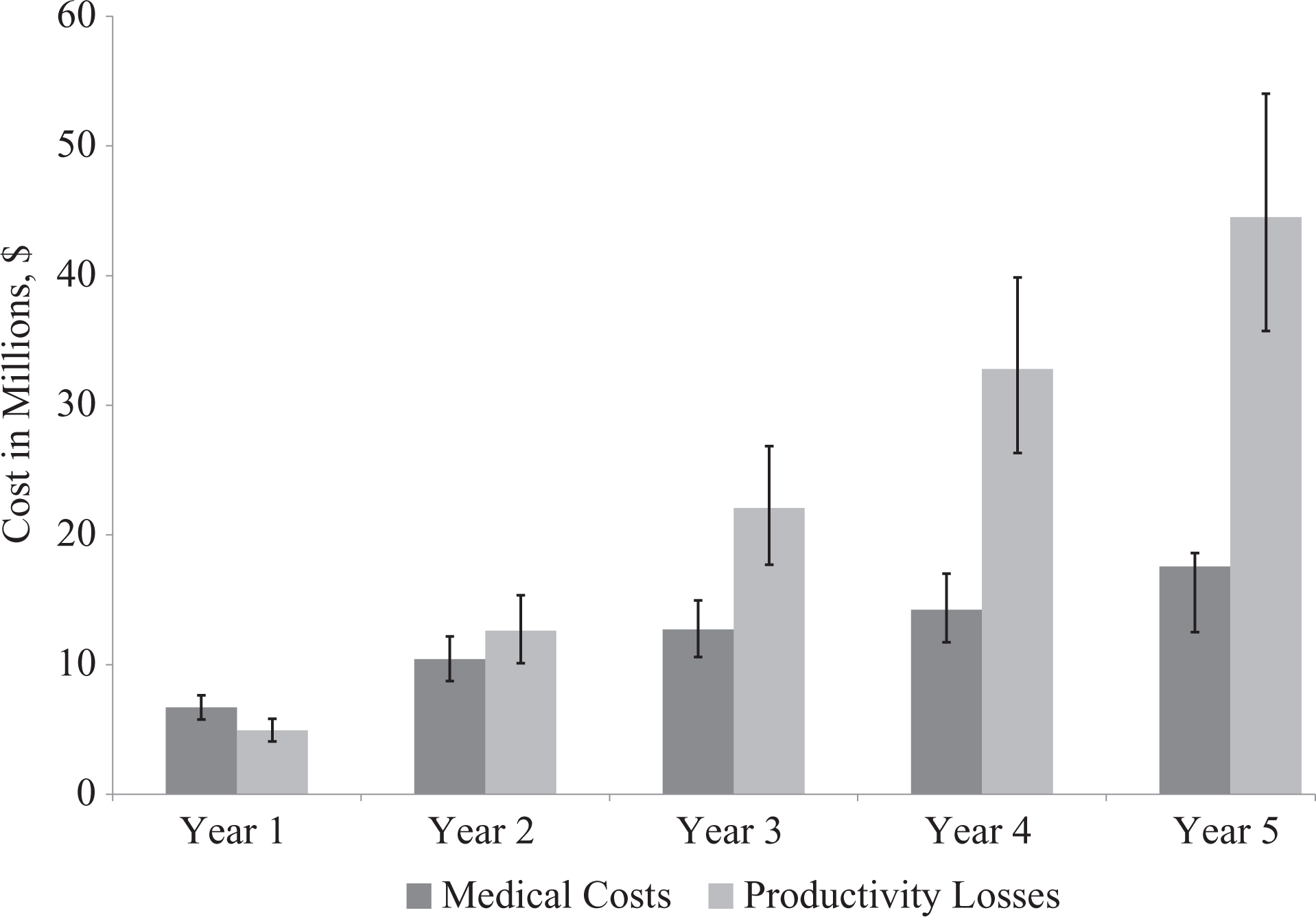
US federal workforce predicted averted medical costs and productivity losses, after a 5 percentage-point reduction in smoking, 2015-2019. Errors bars indicate 95% confidence intervals generated from a Monte Carlo sensitivity analysis.
When we varied the reduction in prevalence from 5 percentage points to a lower prevalence reduction (eg, 1 or 3 percentage points), our results declined in magnitude (Table 3). However, even a 1 percentage-point reduction in smoking prevalence would reduce the number of hospitalizations for acute myocardial infarction by 221 and strokes by 160; the number of deaths by 98; medical costs by $11.9 million; and productivity costs by $23.4 million. Per 10 000 employees, a 5 percentage-point reduction would result in approximately 5.7 fewer hospitalizations for acute myocardial infarction (range across all scenarios, 1.1-6.8), 4.1 fewer hospitalizations for stroke (range across all scenarios, 0.8-4.9), and 2.5 fewer deaths (range across all scenarios, 0.5-3.0). When we divided our costs by the number of federal employees, we found that medical costs could be reduced by $30.50 per employee (range across all scenarios, $6.10-$36.70), productivity costs could be reduced by $59.00 per employee (range across all scenarios, $12.00-$71.90), and absenteeism costs could be reduced by $170.40 (range across all scenarios, $32.30-$204.30).
Discussion
As the largest employer in the nation, the federal government has policies in place that can influence a large number of employees and potentially serve as an example for the nation. At a 5% reduction in smoking prevalence, our model predicted substantial reductions in myocardial infarction and stroke hospitalizations, deaths, and associated medical and productivity costs. Even at a 1% reduction in smoking prevalence (moving from 13% to 12% prevalence of smoking in the federal workforce), we estimated potential reductions per federal employee of $6.10 in medical costs, $12.00 in productivity costs, and $32.30 in absenteeism costs, yielding a potential total cost offset of $50.40 per employee during a 5-year period. These costs accrue to insurers and employees through fewer hospitalizations and to the federal government through fewer missed workdays. Two potential options for reducing federal workforce smoking rates are (1) increasing awareness of tobacco cessation benefits provided through federal health insurance and (2) implementing a federal campus-wide tobacco-free policy.
Since 2011, the US Office of Personnel Management has required insurance carriers in the Federal Employees’ Health Benefits Program to provide a comprehensive, evidence-based tobacco cessation package. Through this coverage, federal employees and their dependents receive individual, group, and telephone counseling and the 7 US Food and Drug Administration–approved cessation medications with no copay or co-insurance. The coverage includes at least 2 quit attempts per year, with a minimum of 4 counseling sessions of at least 30 minutes for each attempt. 34 Although federal employee health benefits provide a minimum of 4 counseling sessions, meta-analyses show a significant dose–response relationship, whereby people who have more sessions have better rates of abstinence. 35 According to a 2013 Office of Personnel Management survey, only 10% of federal employees who were current tobacco users were aware of this health insurance benefit. 34 Further promotion of this benefit could enhance awareness and uptake of cessation benefits among federal employees.
Implementing tobacco-free policies could encourage more smokers to quit and prevent secondhand aerosol exposure from electronic cigarettes (also known as electronic nicotine delivery systems). Secondhand aerosol exposure from electronic nicotine delivery systems can expose others to harmful constituents. 36 More than 475 colleges and universities have implemented tobacco-free policies. 37 Only 3 federal departments have a tobacco-free policy (ie, the US Department of Health and Human Services, the Federal Trade Commission, and the Department of Transportation). Most federal agencies have implemented a 1997 executive order that bans cigarette smoking within federally owned and operated facilities. 38 This policy was updated in 2009 by an additional General Services Administration policy that extended the smoking restrictions to eliminate all remaining indoor smoking areas and to prohibit smoking in courtyards and within 25 feet of doorways and air intake ducts on outdoor spaces under the jurisdiction, custody, or control of the General Services Administration. 39 However, smoke-free policies do not cover other forms of tobacco use and do not extend restrictions on tobacco use to entire campuses, including outdoor grounds. In 2012, the National Prevention Council, which comprises 20 federal departments and is chaired by the US Surgeon General, established a shared commitment to increase tobacco-free environments across the federal government. 40
Limitations
This study had several limitations. First, because of data limitations, we did not include the US Postal Service, military, intelligence services, contractors, and non–full-time-equivalent fellows. Inclusion of these groups would have increased the magnitude of our results. Second, although we did not model additional costs of diseases associated with smoking, such as cancers, chronic obstructive pulmonary disease, complications from pregnancy, and health impacts associated with exposure to secondhand smoke, adding these costs would have increased the magnitude of our results. Third, we were not able to distinguish smokers by duration of smoking. Duration of smoking would allow us to further estimate a smoker’s risk of acute myocardial infarction or stroke. Fourth, we did not model cost implications beyond 5 years, which would have increased potential averted productivity losses and medical costs. Fifth, although our model relative risks represented pooled risks from studies that included age groups outside the 35-64 age range, these studies could be generalized to US adults aged 35-64. Finally, we did not account for potential lower wages of smokers compared with nonsmokers; a lower wage would decrease averted productivity losses and absenteeism costs. Despite these limitations, our analyses showed impacts for different what-if scenarios, providing a range for potential reductions in smoking prevalence and corresponding health and economic benefits.
Conclusion
Reducing the number of smokers in the federal workforce would improve the cardiovascular health of employees through fewer hospitalizations and deaths attributed to myocardial infarction and stroke, as well as decrease medical costs, productivity losses from premature death, and missed workdays. The federal government can leverage tobacco-free policies and promote current federal employee tobacco cessation benefits to encourage employees to quit smoking.
Footnotes
Acknowledgments
The authors thank Kakoli Roy for technical guidance and input, Dawn Alley for advice on the initial conceptualization of the project, and Kristy Marynak and Stephen Babb for comments on a previous version of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Disclaimer
The findings and conclusions in this article are those of the authors and do not necessarily represent the views of the Centers for Disease Control and Prevention or the US Department of Health and Human Services.