
Abstract

In 2001, the Council on Linkages Between Academia and Public Health (hereinafter, Council on Linkages) adopted a set of core public health competencies that described the practical skills necessary for an effective public health workforce. 1 The Council on Education for Public Health requires that schools and programs of public health meet certain subject competencies for accreditation, such as those identified by the Council on Linkages. 2 For the subject of epidemiology, the Council on Linkages competencies include describing factors affecting the health of a community, assessing the validity and reliability of data, and collecting, analyzing, and interpreting quantitative and qualitative data that can be used to assess the health of a community. 1 Traditionally, epidemiology classes in master of public health (MPH) programs address these competencies through didactic lecture, example-based activities, and group discussion, all of which can be effective for introducing and explaining epidemiologic concepts. However, the bridge from the classroom to practice is not always achieved. MPH students have difficulty grasping methodologic concepts and how they apply to their future professions. 3,4 After taking epidemiology classes, students might understand epidemiologic theory and concepts but struggle with how to use epidemiology to solve real-world problems. 3,5
MPH programs can bridge that experiential gap through activities that allow students to apply public health concepts to community health issues. Although MPH programs often require students to undertake an internship or clerkship to gain experience in public health practice, experiential learning does not commonly take place in the classroom. 6 Academicians have called for an integration of experiential learning activities in epidemiology and other methods classes. 7 –9 Although the literature documents several successful practice-based applications of epidemiologic methods in the classroom, 10 –13 these examples are exceptions rather than the rule.
Studies show that experiential learning and service learning are successful in teaching public health, medicine, and other health-related disciplines. 6,11 –14 Experiential learning is a teaching approach that gives students an opportunity to apply theory and concepts learned in the classroom to a setting outside the classroom. Experiential learning activities connect students directly to the subject being studied rather than merely thinking about or reading about the actions of others. 15,16 This approach teaches through experience and reflection rather than through didactic information transfer from teacher to student. Decades of pedagogical theories by John Dewey, Kurt Hahn, and Paulo Freire support this model as an effective teaching technique. 16 Service learning is a type of experiential learning that not only engages students in a practical learning experience but also focuses students’ efforts on a community-based issue. 17 Service learning was identified as a promising learning technique that should be used more by programs of public health in the 21st century to teach students about real-world public health issues. 5 In the classroom, the service-learning model promotes application of information learned in the classroom to a community issue to obtain a deeper understanding of the learning objectives. 6
This article describes the Observed Smoking Behavior Project, which is an experiential service-learning project performed by students in the Advanced Epidemiology course in the Jefferson College of Population Health MPH program at Thomas Jefferson University. We provide an overview of the project, describe student feedback on the project, reflect on lessons learned, and offer suggestions for epidemiology instructors who are interested in incorporating an experiential data collection project in their classes.
Methods
The Observed Smoking Behavior Project
The Jefferson College of Population Health MPH program comprises about 90 students and has been accredited by the Council on Education for Public Health since 2009. To earn a degree in the program, students need to complete 45 credits of topical and methodologic classes, including Fundamentals of Epidemiology. Advanced Epidemiology is an elective course that expands on the epidemiologic theory, principles, and methods that are introduced in the Fundamentals course. In spring 2015, MPH program faculty decided that the Advanced Epidemiology course should teach students the practical skills of collecting and analyzing data to expand their public health skills, help prepare them to complete the program’s required capstone project, and make them more appealing to potential employers.
The design of the experiential project was inspired by the work of Smoke Free Philly, which is part of Get Healthy Philly, an initiative of the Philadelphia Department of Public Health. 18 Smoke Free Philly brings stakeholders together to plan, implement, and evaluate initiatives to reduce smoking in Philadelphia County, Pennsylvania, the county with the highest adult smoking rate among the 11 most populous US counties. 19 In early 2015, we met with the program manager of Smoke Free Philly and learned that the initiative could benefit from acquiring additional local data on the amount of smoking, secondhand smoke exposure, and tobacco-related litter in various settings. To meet this need and to address student pedagogical competencies, we created the Observed Smoking Behavior Project. For the project, we asked students to collect data on smoking behavior among people in 2 Philadelphia settings—parks and private vehicles—and use these data to quantify the proportion of people who smoke in these settings. Ultimately, the project was intended to support the tobacco control efforts of the Philadelphia Department of Public Health.
In April, May, and June 2015, we assigned 19 students enrolled in Advanced Epidemiology to 1 of 4 data collection roles to collect data on smoking behavior (Table). To assist data collection in parks, we created a mobile telephone application (app) called ObserveSmoking, which students downloaded onto their smartphones. This app provided students a way to discreetly collect data about public smoking behavior and efficiently and securely send the results electronically to the instructor. 20 Students assigned to the role of counter observed people entering 1 of 3 Philadelphia parks: Independence Square National Historical Park, Washington Square Park, and Louis Kahn Park (Figure). Using selection features on the ObserveSmoking app, the counters categorized each person entering their assigned park according to smoking status (smoking/not smoking), age (adult/child), and sex (male/female). Using a stopwatch feature on the app, the timers timed a sample of smokers who entered the parks to identify the duration of smoking in the parks. Litter auditors used paper data collection instruments to categorize the proportion of tobacco-related litter that they observed in parks. Students who were vehicle observers observed smoking among occupants of vehicles traveling through 1 of 4 intersections in downtown Philadelphia: 10th St and Chestnut St, 11th St and Walnut St, 12th St and Locust St, and 13th St and Spruce St (Figure). Vehicle observers used handheld electronic devices and the Advanced Tally Counter app 21 to categorize a sample of vehicles passing through intersections by occupant smoking status, number of occupants, and presence of child occupants. Smoke Free Philly advised the development of methods for collecting data in parks and shared Philadelphia Department of Public Health–developed instruments that had been used previously for smoking observations and litter audits in parks. 22
Data collection sites and tools and roles of MPH students in the Observed Smoking Behavior Project, Philadelphia, Pennsylvania, April to June 2015a
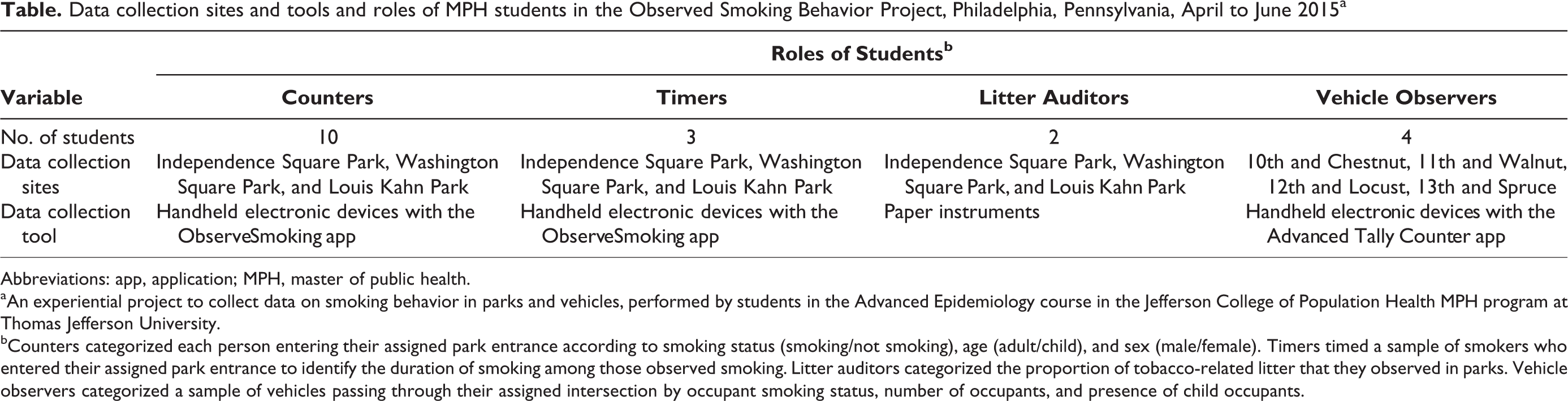
Abbreviations: app, application; MPH, master of public health.
aAn experiential project to collect data on smoking behavior in parks and vehicles, performed by students in the Advanced Epidemiology course in the Jefferson College of Population Health MPH program at Thomas Jefferson University.
bCounters categorized each person entering their assigned park entrance according to smoking status (smoking/not smoking), age (adult/child), and sex (male/female). Timers timed a sample of smokers who entered their assigned park entrance to identify the duration of smoking among those observed smoking. Litter auditors categorized the proportion of tobacco-related litter that they observed in parks. Vehicle observers categorized a sample of vehicles passing through their assigned intersection by occupant smoking status, number of occupants, and presence of child occupants.
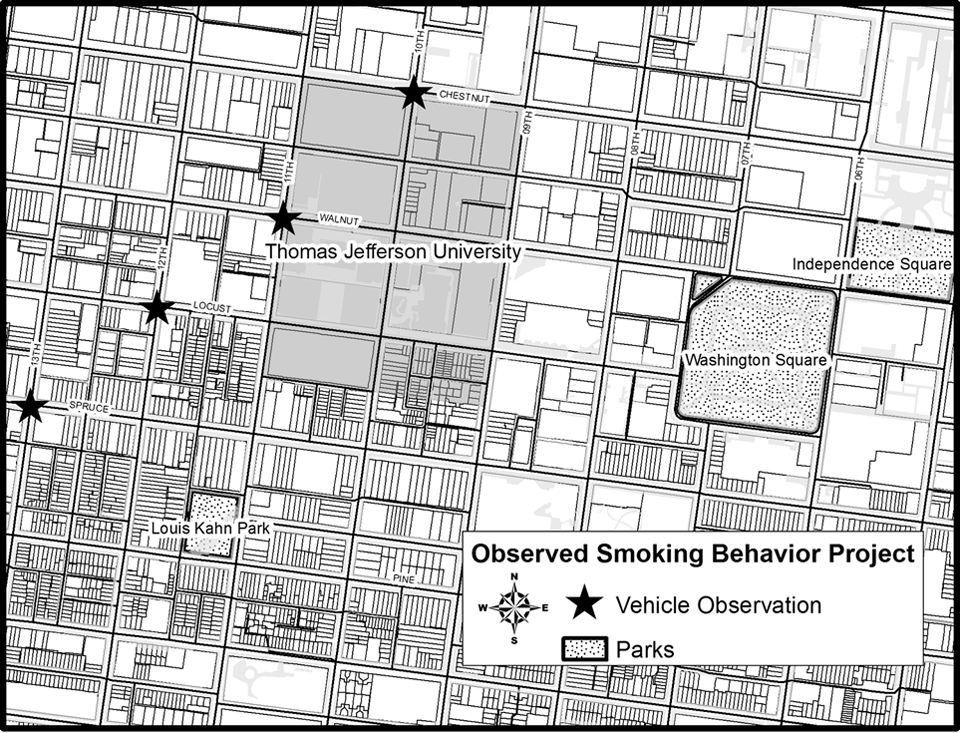
Data collection sites for the Observed Smoking Behavior Project, Philadelphia, Pennsylvania, April to June 2015. The Observed Smoking Behavior Project was an experiential project to collect data on smoking behavior in parks and vehicles performed by students in the Advanced Epidemiology course in the Jefferson College of Population Health master of public health program at Thomas Jefferson University.
Each student was trained on data collection protocols by the instructor during class time. The training included the processes that the counters, timers, litter auditors, and vehicle observers each needed to follow for collecting, saving, and submitting data by using the smartphone apps or paper instruments. In addition, the training included reviewing pictures of smoking products, definitions for how to define a smoker (someone who is in possession of a product meant to be smoked, whether or not it is lit), and methods to help distinguish between the study definition of adults (aged ≥13) and children (aged ≤12). After the trainings, students practiced collecting data and performed an activity that required those with similar data collection roles to observe the same park patrons, vehicles, or area for litter audits. During the next class, students completed an interrater reliability activity using these data to calculate how reliable they were at categorizing park patrons and vehicles using the data collection instruments. After training was completed, students collected data during the last 30 minutes of each weekly class from 4:15 to 4:45
Outcomes
Data Collection
During the course of five 30-minute observation periods in May and June 2015, counters observed 3179 adults and 257 children among the 3 parks; timers timed 20 smokers; litter auditors categorized 1469 pieces of litter; and vehicle observers categorized 4483 vehicles at the 4 intersections. During class time, students reflected on data collection from previous weeks, discussed instrumentation issues, and talked about methodological challenges with data collection. Twice during the 11-week class, we reviewed the counter results and discussed how they could be used to inform public health practice.
Reflection Paper
The students were required to complete a reflection paper on their experience collecting empirical research during the Observed Smoking Behavior Project. In addition to personal reflection, they were required to consider their data collection role, identify threats to validity and reliability, and suggest improvements for future data collection. The writing assignment encouraged students to consider how the experience affected the development of their epidemiologic skills and course competencies.
In their papers, students reported that the Observed Smoking Behavior Project helped them describe factors affecting the health of communities. Their comments included, “I think [results of the study] could be of interest to the public, especially to parent groups and parents of young children who frequent the park, as a few people (smokers) are severely polluting a space that is meant for everyone.” In reflecting on the validity and reliability of the study data, one student commented, “One of the strengths of this data collection method is that it utilizes direct observation. There is no ambiguity on whether or not the instrument is measuring false positives or negatives, since I can visually attest to if each person is physically smoking.” Overall, students saw the Observed Smoking Behavior Project as a link between epidemiologic theory and data collection in the real world. One student stated, “I found this data collection project very interesting because it put the epidemiology knowledge gained in the classroom into practice. I do believe that there could be some improvements to the data collection, but all in all, I enjoyed my experiences.”
Lessons Learned
This project is an example of an experiential learning activity that should be a component of epidemiology courses in MPH programs. Although it was difficult to isolate student learning outcomes attributable to the Observed Smoking Behavior Project, students reported that the project was interesting and enjoyable and reinforced course content, including some of the major Council on Linkages competencies for epidemiology. Students used the data that they collected to identify the proportion of smokers among those observed in parks and vehicles, and they acknowledged how the data described the epidemiologic characteristics of person, place, and time. 23 The data collection itself, analysis activities during class time, and reflection activities gave students a hands-on experiential way to hone important epidemiologic skills that can be used in their future occupations. Also, the reflection paper assignment required students to critically analyze the data collection methods, identify threats to data validity and reliability, suggest improvements for data collection methods, and describe how the results could inform public health interventions and improve the health of communities.
We have several suggestions for MPH programs that consider creating a student data collection project in epidemiology classes. First, the major challenge that we encountered was the amount of out-of-class time that was required to conduct this study. Four roles with 4 different training requirements, instruments, protocols, and analysis methods were required. It would not have been possible, in a 1-term class, for 1 instructor alone to plan and manage these 4 separate data collection roles while performing the other required instructional duties of the class (ie, preparing lessons, creating in-class activities, and preparing and grading assignments). Fortunately, Jefferson College of Population Health provided funding for a graduate assistant who managed the data collection for the Observed Smoking Behavior Project. Additionally, the ObserveSmoking app was designed and developed in collaboration with staff members from the Thomas Jefferson University Center for Teaching and Learning. Without their assistance, counters and timers would have used clipboards and paper instruments to collect data instead of the app on their smartphones. Subsequently, the time burden of entering and organizing timer and counter data from paper instruments may have been overwhelming. For instructors considering similar data collection and analyses for their epidemiology classes, we recommend exploring departmental or campus resources that might ease the administrative or time burden for such projects. Additionally, we recommend limiting the number of student data collection roles to 1 or 2, based on stakeholder, student, or instructor preference.
Second, student data collection and analysis should be built into the course requirements. We assigned one-fifth of the total points in the class (100 of 500) to assignments associated with the project, which we believe was adequate. Students received points for evaluating the training, collecting and analyzing the data, and completing the reflection paper. Point incentives helped ensure that students attended class, collected data according to protocol, performed analysis activities in class, and adequately reflected on the methods and results of the study.
Finally, care must be taken to consider how the data are used for analysis in and out of the classroom. In class, the students particularly enjoyed talking about the sources of bias and threats to validity that they identified while collecting data. This discourse served as a rich source for discussing epidemiologic concepts, such as validity and reliability, study design, and sampling. But, given time constraints, we could not designate equal amounts of class time to discuss each data collection role, and we largely focused our discussion on the role of the timers. This compromise was satisfying to students who were timers, but students who had other roles expressed disappointment that equivalent amounts of class time were not devoted to their roles. Also, students were very interested in performing their own analyses of class-collected data, but there was no opportunity to do so. For future data collection, we will consider creating a shared electronic space on the Blackboard class website whereby students could access the raw data and perform their own analyses outside of class.
Conclusion
The Observed Smoking Behavior Project gave Jefferson College of Population Health MPH students enrolled in Advanced Epidemiology an enjoyable and meaningful project in which they applied the epidemiologic information that they developed in the classroom. The project helped them gain practical methodological skills and experience in collecting and analyzing data that could inform local public health initiatives. Epidemiology instructors in schools and programs of public health should consider adopting experiential classroom projects to help students apply epidemiologic concepts to the real world, address course competencies, and prepare students for the public health workforce.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.