
Abstract
Exposure to explosive armaments during Operation Iraqi Freedom and Operation Enduring Freedom contributed to approximately 14% of the 352 612 traumatic brain injury (TBI) diagnoses in the US military between 2000 and 2016. The US Department of Defense issued guidelines in 2009 to (1) standardize TBI diagnostic criteria; (2) classify TBI according to mechanism and severity; (3) categorize TBI symptoms as somatic, psychological, or cognitive; and (4) systematize types of care given during the acute and rehabilitation stages of TBI treatment. Polytrauma and associated psychological and neurologic conditions may create barriers to optimal rehabilitation from TBI. Given the completion of recent combat operations and the transition of TBI patients into long-term care within the US Department of Veterans Affairs system, a review of the literature concerning TBI is timely. Long-term follow-up care for patients who have sustained TBI will remain a critical issue for the US military.
Traumatic brain injury (TBI) is defined as a traumatically induced structural injury of the brain or physiologic disruption of normal brain function resulting from an external force. Patients with TBI may show a combination of symptoms and signs, including periods of lost or altered levels of consciousness and amnesia, as well as neurologic deficits and/or intracranial lesions on imaging. 1 An estimated 1.7 million people in the general US population sustain mild, moderate, or severe TBIs each year: of these, approximately 1.4 million people seek care in emergency departments or other acute medical facilities, 275 000 require hospitalization, and 52 000 die from their injuries. 2
The high incidence of TBI in military members has caused it to be dubbed the signature wound of service members returning from Operation Iraqi Freedom (OIF) and Operation Enduring Freedom (OEF). 3 It may also have played a role in the US Department of Defense issuing guidelines in 2009 to (1) standardize TBI diagnostic criteria; (2) classify TBI according to mechanism and severity; (3) categorize TBI symptoms as somatic, psychological, or cognitive; and (4) systematize types of care given during the acute and rehabilitation stages of TBI treatment. 1
Recently, military databases have reported substantially fewer traumatic thoracic injuries and gunshot wounds in US service members during OIF and OEF than during previous wars, but they have also noted substantially more head and neck injuries, including TBIs. 4 Improvements in body armor, tactical training, and safety precautions have likely contributed to the lower number of non–head and neck wounds 5 as well as to a 92% survival rate for injured service members during OIF and OEF. 6,7
Yet, despite these relatively high survival rates, the fact that such a large proportion of recent military service members has sustained a TBI underscores the importance of a deeper understanding of and ongoing research into the epidemiology, classification, evaluation, and treatment of TBI. 2,4,8 We performed a literature review and synthesis referencing information from peer-reviewed and government sources to provide an overview of incidence, clinical approach, and policies relating to TBI within the US Military Health System from 2000 to the present.
TBI Incidence
TBI incidence statistics are often disputed. Indeed, estimates of TBI incidence based on patient self-reports or extrapolations of data sets differ widely, possibly obscuring the actual frequency of TBI in the military population. 9 For example, some studies have calculated TBI incidence based on regional injury casualty reports and excluded service members who returned to duty within 72 hours of injury. With such an approach, cases of mild TBI, often not accompanied by visible wounds, may be substantially underreported. 10 As another example, in a 2008 random survey of prior OIF and OEF service members, an estimated 19.5% of respondents sustained a TBI during deployment. Based on this proportion and by extrapolating across all military branches during the same period, 320 000 cases of TBI were estimated to have occurred during the Iraq and Afghanistan conflicts. 11 However, a separate Armed Forces Health Surveillance Center report covering a similar period identified only 130 000 clinically confirmed cases of TBI. 9 Based on a different approach, a survey of 3973 army unit members in 2009 suggested that about 23% of US service members were returning from OIF and OEF with a TBI. 3
Although there continues to be some debate about how the incidence of TBI in the military is calculated, it appears that it is reasonable to estimate that about 20% of US service members involved in OIF and OEF may have sustained TBIs. This prediction is consistent with US Department of Defense reports that 352 612 service members had TBIs between 2000 and 2016, the period that includes both OIF and OEF. 8
TBI Diagnosis and Classification
TBI is difficult to diagnose because it requires careful assessment of patients not only at the time of their injury but also during the acute period after the injury. Many of these injuries are not directly observed by clinicians during these important time points. Consequently, the details contained in witness accounts and self-reporting by those injured can provide important information. The fact that clinicians are often not involved at the time of or immediately after these injuries has contributed to substantial challenges implementing service-wide standardized protocols for TBI diagnosis and screening.
TBIs can be broadly classified by neurologic damage (diffuse, focal, or both), degree of penetration of the injury, and severity (mild, moderate, or severe). Also, because of the high prevalence in military populations, blast injuries can be subclassified through a mechanism-specific approach—as primary, secondary, tertiary, or quaternary (Table 1). 12 Tertiary blast injury is the principal mechanism of TBI among injured service members. 13
Centers for Disease Control and Prevention classification criteriaa for blast-injured military service members, according to mechanism of injury and result
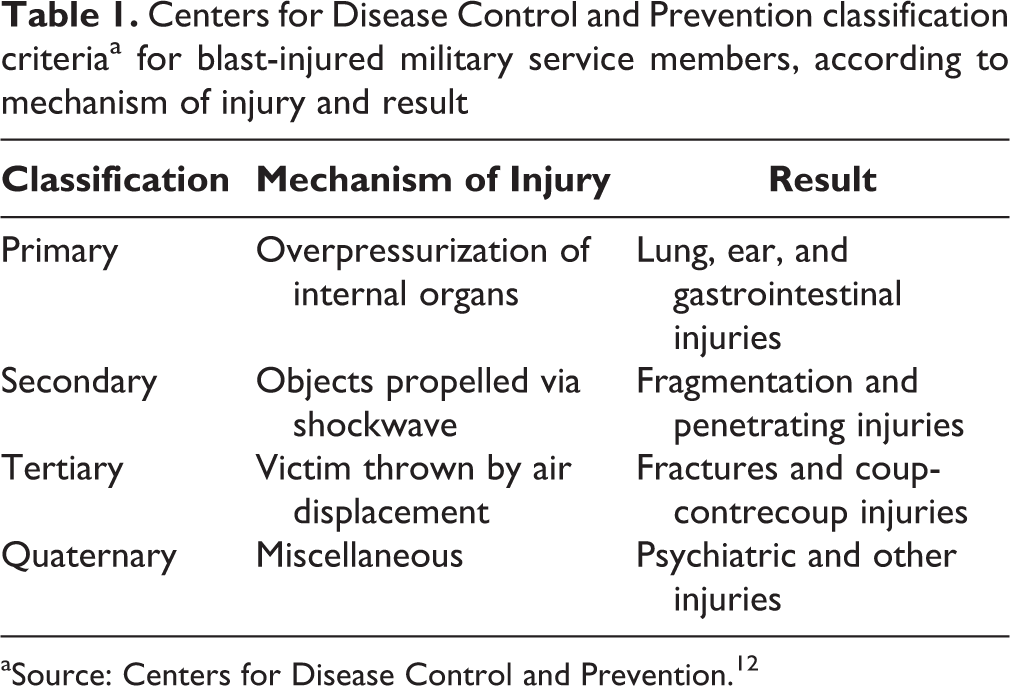
aSource: Centers for Disease Control and Prevention. 12
The most commonly employed classifications systems, however, focus on severity of injury. The Glasgow Coma Scale (GCS) is the most common scoring system used to describe the level of consciousness in a person following a TBI, and it is used to help gauge the severity of an acute brain injury. 1,2,14,15 Observations of verbal response, motor response, and eye-opening abilities are used to calculate a score that classifies the severity of TBI as mild (GCS score, 13-15), moderate (9-12), or severe (3-8). However, although valuable for early assessment, GCS has limited prognostic ability because patient performance may be affected by other factors, such as shock or low blood oxygen levels. 16 The highest GCS score obtained within the first 24 hours after injury is generally used as the reference point for subsequent rehabilitation and testing. 1,14
The US Department of Defense has adopted the use of a severity-based diagnostic classification system that includes the GCS with several other clinical criteria. In this classification system, the severity categories of TBI—which are based on the status of the patient at the time of the incident—are mild, moderate, and severe (Table 2). 1 Mild TBI, the most frequent form of brain injury, is commonly known as a concussion, 8,15 and it is diagnosed when there is normal neuroimaging, loss of consciousness for <30 minutes, alteration of consciousness from a moment up to 24 hours, posttraumatic amnesia for up to 24 hours, and a GCS score ranging from 13 to 15. However, severe TBI is diagnosed when there is normal or abnormal neuroimaging, loss or alteration of consciousness ≥24 hours, posttraumatic amnesia for ≥7 days, and a GCS score 3-8. TBI severity typically correlates with functional and rehabilitative outcomes. 1,9 However, some patients with severe injuries may have positive outcomes, whereas others with mild TBI may have long-term functional impairments.
Diagnostic criteriaa for determination of traumatic brain injury severity among military service members
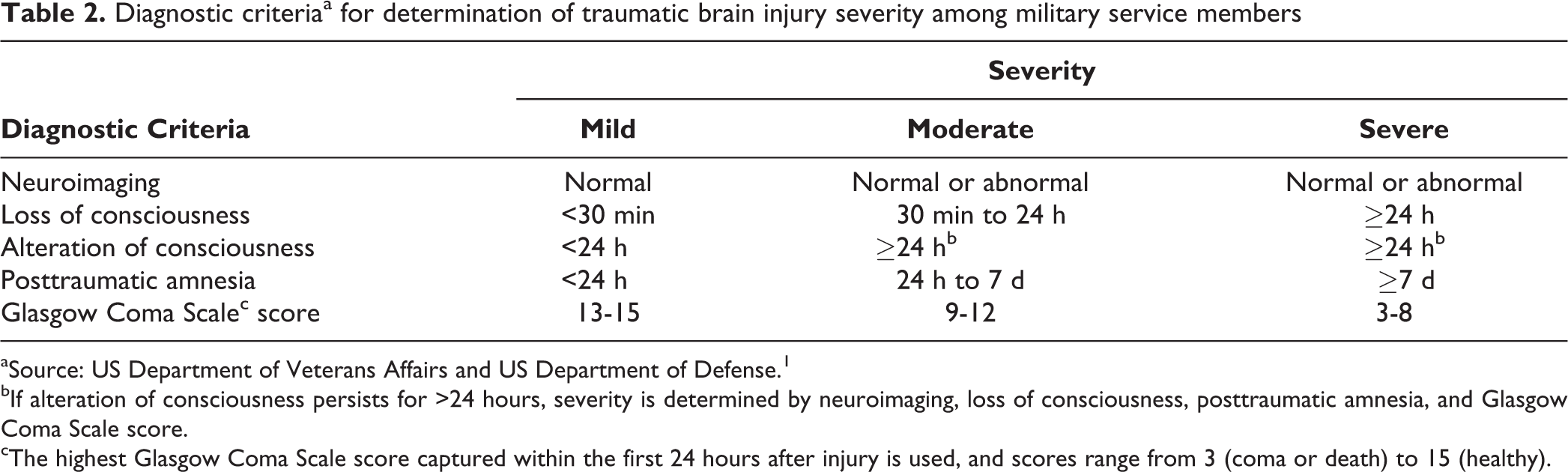
aSource: US Department of Veterans Affairs and US Department of Defense. 1
bIf alteration of consciousness persists for >24 hours, severity is determined by neuroimaging, loss of consciousness, posttraumatic amnesia, and Glasgow Coma Scale score.
cThe highest Glasgow Coma Scale score captured within the first 24 hours after injury is used, and scores range from 3 (coma or death) to 15 (healthy).
In a report of 907 TBIs in a single army unit, the injuries were classified as mild (82.5%), moderate (8.3%), severe (1.0%), or either complex or undiagnosed (8.2%). 3 In the 2009 US Department of Defense report of 28 958 TBIs in 2009, based on a classification system combining severity and mechanism, 83.0% were classified as mild, 6.8% as moderate, 1.2% as severe, and 1.8% as penetrating, with 7.2% not classifiable. 8
TBI Symptoms
The US Military Health System guidelines suggest that symptoms of mild TBI be thought of as somatic, psychological, or cognitive. 1 Examples of somatic symptoms that may occur with mild TBI include headache, drowsiness or fatigue, phonophobia, photophobia, insomnia, dizziness or difficulty balancing, nausea, and vomiting. Psychological symptoms associated with mild TBI may include irritability, anxiety, and depression. Cognitive symptoms that may occur after mild TBI include memory impairment, confusion, impulsiveness, difficulty concentrating, and problems with language or speed of processing. Various other more critical symptoms that may be associated with moderate to severe TBI include the following: diminished sensation (gustatory, olfactory, auditory, or visual), impaired depth perception, nystagmus, epileptic seizures, tinnitus, dementia, dysarthria, aphasia, peripheral neuropathy, and aggression. 1,17 –19 In addition, in a general population evaluated up to 10 years postinjury, patients with moderate or severe TBI had a substantially higher risk of developing and sustaining additional symptoms, such as abnormal social behaviors, 17 abnormal executive functioning, 18 increased aggression, 19 and alexithymia. 20
TBI Neuroimaging
Conventional imaging technologies often lack sensitivity for detecting mild TBI. For example, although computed tomography is useful for diagnosing gross injury or intracranial blood, it lacks the necessary resolution to detect subtle changes in neurocircuitry and cannot explain or predict postinjury behavioral deficits. However, in patients with moderate to severe TBI, newer high-resolution neuroimaging has shown extensive changes in white matter organization during stages of acute and chronic rehabilitation. 21,22
Diffusion tensor imaging, a form of diffusion magnetic resonance imaging, is capable of revealing white matter fiber-derived brain neurocircuitry maps and microstructural changes in the brain. 23 In a trial with severe TBI patients who had diffusion tensor imaging on 3 occasions after injury (<6 weeks, 2 years, and 5 years), fractional anisotropy, a measure of connectivity in the brain, was significantly lower (P < .05) in the genu and body of the corpus callosum and bilateral corona radiata regions of the brain. 21 However, radial diffusivity, a measure of degenerative pathology, was significantly (P < .05) higher in those regions. The changes in fractional anisotropy and radial diffusivity were particularly pronounced 2 years postinjury as compared with controls and were significantly (P < .05) associated 5 years postinjury with neurocognitive sequelae such as aphasia, dyspraxia, and amnesia.
In another study, diffusion tensor imaging was used to examine cortical thickness, white matter connectivity, and regional volume differences in patients after severe TBI, and testing revealed widespread atrophy in the prefrontal, parietal, and precuneus regions of the brain. 24 These changes were associated with diminished declarative memory. Declarative memory impairment is a well-documented effect of moderate and severe TBI and is hypothesized to be mediated and accompanied by changes in hippocampal white matter tracts. 22 In the study, although observed hippocampal volume was lower in patients with TBI than in controls, only decreases in fractional anisotropy successfully predicted declarative memory deficits. 24 Similarly, in a meta-analysis of 13 diffusion tensor imaging studies of patients with mild TBI, random-effect models showed significant reductions (P < .025) in fractional anisotropy and increases in mean radial diffusivity (P = .013) in the splenium of the corpus callosum. 25 These findings may explain the persistence and longevity of TBI symptoms seen in many injured service members. Although promising, the actual practical use of diffusion tensor imaging is currently limited because of its expense and the time required to perform serial imaging. 26,27
Initial TBI Prognosis
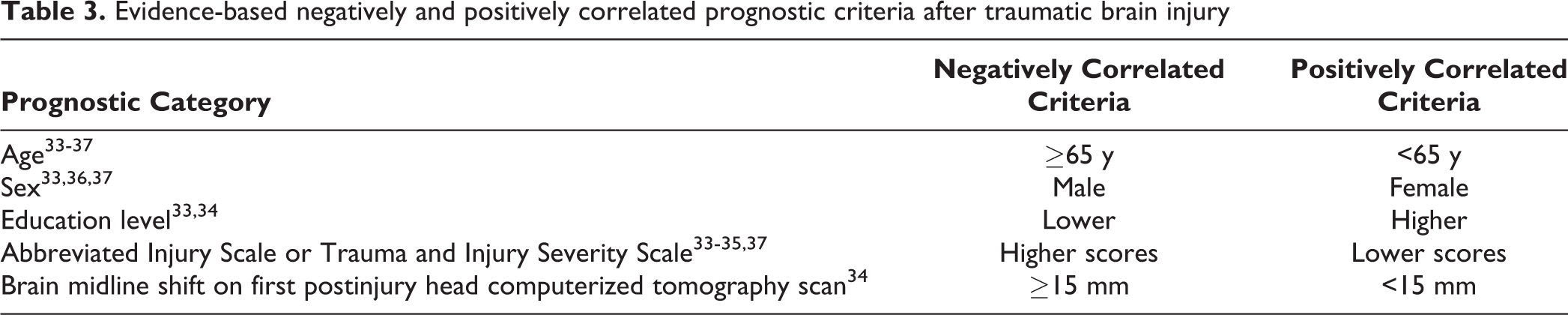
To determine the initial prognosis and establish a framework for rehabilitation for a patient after TBI, health care providers use information about the durations of loss of consciousness, coma, and posttraumatic amnesia in addition to the inability to follow commands. An extended duration of loss of consciousness immediately after injury is negatively correlated with long-term rehabilitative potential. 28,29 Determining the duration of loss of consciousness is challenging as this requires an external witness, because the patient is typically unaware of how long he or she was unconscious. Also, in combat situations it can be difficult to obtain accurate information about the duration of loss of consciousness. In addition to loss of consciousness, alterations in consciousness manifesting in acute cognitive-behavioral changes (eg, disorientation, confusion, delayed thinking) are frequently reported and may be used to help determine prognosis. 30,31 The initial prognosis may also be affected by the duration of posttraumatic amnesia. Posttraumatic amnesia is a state of disorientation and confusion that may occur immediately after initial TBI, is characterized by an inability to form new memories or recall older memories, and is considered resolved when clear, continuous memory returns. 32 Because of the shortcomings of prognostic variables when interpreted in isolation, practitioners may also use an aggregate system, combining a variety of evidence-based demographic and clinical components that correlate with prognosis (Table 3). Nevertheless, at the present time there is still no universally accepted consensus or standard prognostic scale for TBI.
Evidence-based negatively and positively correlated prognostic criteria after traumatic brain injury
TBI Treatment
Acute Management
The management of TBI in the acute setting is based on a combination of factors, including severity of injury, mechanism of injury, and time from injury. The general goal of acute treatment is homeostatic stabilization and prevention of secondary injuries. 38 The early management of moderate, severe, and penetrating TBI is particularly complex, with priority placed on maintaining appropriate cerebral blood flow and intracranial pressure. 39 These injuries may result in crushing or shifting of brain matter as well as intracranial hypertension and edema. 40 Elevated intracranial pressure can be detected by neuroimaging and actively monitored through intraventricular catheterization. 41,42 High intracranial pressures may be managed with pharmacologics, controlled hyperventilation, decompressive craniectomy, and/or simple manipulation of the patient’s skull. 43 –46 Endotracheal intubation and mechanical ventilation are frequently used in the acute setting of these severe injuries to ensure proper brain oxygenation, whereas blood pressure is strictly controlled through the use of intravenous fluids and medications. 39 Additionally, body temperature is tightly regulated to ensure that the brain’s metabolic resources are constant. 47 In cases of moderate, severe, or penetrating TBI, urgent neurologic surgery may be performed to remove foreign matter or to drain contusions and hematomas that are causing intracranial structure shifting. 39,47 Because there is a high risk of vasospasm and pseudoaneurysm formation between 2 and 14 days after blast-related injuries, intensive care monitoring is particularly important during this period. 48,49
The approach to early management of service members with mild TBI is different but no less important, given the high prevalence of mild TBI. Clinical recommendations for early treatment of mild TBI include rest and limited physical and cognitive exertion, followed by a gradual, clinician-supervised reintroduction to normal activities for up to 3 days after injury. 50 For cases of mild TBI in which symptoms persist beyond several days, monitoring is continued for up to 6 weeks before intervention is mandated. 51 At that time, if symptomatic treatment has not yet been implemented or has not improved the patient’s functional status, the clinician should reassess the patient for potential alternative explanations. In addition, because many experts consider chronic behavioral sequelae an exclusionary criterion for mild TBI, patients unresponsive to treatment for extended periods are frequently reclassified as having moderate or severe TBI. 1,5 It is also important to identify service members who have sustained multiple mild TBIs. For those who have had ≥3 TBIs during their lives and have impaired neurocognitive performance on simple tasks as well as increased symptoms of distress, it is recommended that they not be sent on any future deployments. 1,52
Rehabilitation
Rehabilitation of the patient with TBI begins after he or she is stabilized, with the aims of improving independent functioning, social integration, and disability adaptation. 53 Because TBI produces highly varied symptoms and because confounding behavioral health and psychiatric disorders may occur, misdiagnosis and ineffective treatment can result. As such, after identification and remediation of confounding conditions, clinicians should reevaluate patients for chronic symptoms of TBI and reassess treatment strategies. Routine follow-up evaluations and reassessments are recommended at 4-month intervals. 51 Depending on the complexity of the condition, some patients may require comprehensive rehabilitation regimens based on a range of therapeutic providers. 53,54 Patients who remain incapable of independent living despite rehabilitation efforts may need to be monitored in supported living facilities or vocational programs. 53 Psychiatric comorbidities such as dysthymia (also known as chronic depression), posttraumatic stress disorder (PTSD), and generalized anxiety disorder are not unusual and may require pharmacologic treatment on acute and long-term bases to decrease social impairment. 55 –57 Additional psychiatric services are often used in TBI cases related to combat or violence. 57,58
Outcomes
Psychological and neurologic impediments may create barriers to optimal rehabilitation from TBI during the acute and chronic phases of recovery. 59 The successful treatment of TBI patients with accompanying polytrauma generally requires lengthy physical rehabilitation, high levels of self-motivation, and a strong psychological foundation. Nevertheless, results from comprehensive treatment approaches to TBI in military populations have been encouraging. For example, community-integrated rehabilitation programs involving a mean treatment time of 190 days showed marked improvements in psychosocial impairment at a mean of 5 years postinjury for service members with mild to moderate TBI. 60 Additionally, in another study, neuropsychological functioning improved dramatically after 4 months of intensive neurocognitive rehabilitation therapy among service members who were followed for an average of 34 months after a mild to moderate TBI. 61
Indeed, the outcomes after mild TBI are generally positive, and mortality rates are low. 62,63 Most symptoms of mild TBI resolve days or weeks after the injury. 63 Persistent deficits are seldom reported, although complete recovery may be impeded by negative coping strategies, financial and family circumstances, intellectual disabilities, and older age. 64,65 Underlying psychiatric and behavioral problems, such as substance abuse, dysthymia, and poor general health, are also associated with longer periods of recovery, and those service members with a history of substance abuse are at increased risk for relapse. 65 –67
Although controversial, some research suggests that mild TBI may have long-term consequences on quality of life, cognition, and emotional functioning. 68 –70 A study of returning OIF and OEF service members with mild TBI from the US Department of Veterans Affairs Medical Center in Palo Alto, California, reported substantial cognitive and emotional barriers that could preclude successful community reintegration at initial and 2-year follow-ups. 71 Another investigation of post-TBI quality-of-life and neurocognitive outcomes in the general population reported incremental declines in clinical outcomes and decreased life satisfaction over time, with only 62.8% of the population being within the normal range for these measures 10 years postinjury. 72 Furthermore, 9.3% of the population in that study reported a loss of employment because of persistent difficulties related to mild TBI (eg, fatigue, insomnia) 10 years postinjury. Similarly, in a retrospective study of service members who sustained combat-related injuries during the Vietnam War, those with mild TBI were at increased risk of chronic dysthymia, psychosocial deficits, and subtle neurologic and neuropsychological conditions. 73,74
Research into the relationship between mild TBI and persistent symptoms must take into account the potentially confounding influence of multiple comorbidities, particularly for service members, among whom psychiatric and psychosomatic conditions frequently coexist with mild TBI. 31 For example, PTSD, of which 118 829 cases were reported among postdeployment service members between 2001 and 2014, 75 often co-occurs with TBI and has overlapping symptoms. 31 A survey of army infantry returning from Iraq indicated that 54 of 123 (43.9%) of those with confirmed mild TBI had PTSD, whereas only 155 of 1701 (9.1%) of those without TBI had PTSD. The survey also reported that those with mild TBI were more likely to report poor general health, more absences on workdays, increased somatic symptoms, and more frequent medical visits after returning from deployment than service members who sustained unrelated injuries or no injuries. Yet, when the analysis was adjusted to control for symptoms of PTSD and dysthymia, the only persistent symptom associated with mild TBI was headache. 31 Likewise, dysthymia and depression may be confounding influences on persistent symptoms after mild TBI. 76 One study found that although depression occurs most often in the first year after TBI, the risk of developing depression is elevated for decades. 57 However, as with PTSD, the actual link between depression and mild TBI is unclear, with one meta-analysis reporting concurrent incidence rates ranging widely, from 10% to 77%. 2,57,77 Some have suggested that PTSD and dysthymia may simply mediate the reporting of persistent symptoms by patients with mild TBI. 31,76,78
As a result of the overlap in the symptoms of TBI and other psychiatric and psychosomatic conditions that can occur postdeployment, these conditions and their symptoms are now collectively referred to as postdeployment syndrome. Postdeployment syndrome may include a combination of TBI, dysthymia, PTSD, chronic pain, and generalized anxiety. In general, patients identified as having postdeployment syndrome have multiple persistent and substantially impairing symptoms that continue for at least 3 months after all physical injuries have healed. Treatment of postdeployment syndrome emphasizes state-of-the-art traditional diagnostic and psychiatric medicine, careful regulation of sleep and environmental stressors, and a return to normalcy after combat. 79 Additional research involving the use of this new diagnostic and therapeutic umbrella term will be needed to help develop consensus on optimal long-term treatment and to more accurately determine outcome benchmarks for TBI. Nonetheless, patients should be made aware that most of those experiencing mild TBI make full recoveries hours or days after injury. 1,68
Although nongovernmental health care organizations and health insurance companies have historically considered TBI to be a onetime isolated event, others argue that TBI should more appropriately be thought of as a disease process. 80 The choice of perspective is important because extended clinical observation and long-term follow-up care are more likely to occur for a disease process than for an isolated event. Retrospective research supports the need for changes in health policy on the need for a longer-term approach to TBI care. One group of investigators found that TBI patients were 4 times more likely than the general population to die from pneumonia 1 year and 40 years after injury. The investigators also found a 22- to 37-fold higher risk of death attributable to epileptic seizures in TBI patients compared with their healthy peers. 81,82 Among patients with moderate to severe TBI evaluated months or years postinjury, 21% to 35% were found to have severely impaired production of endogenous growth hormone, raising the possibility of cascading hormonal changes after TBI. 83 –85 These investigations emphasize the value of considering TBI to be a disease process and the importance of long-term patient monitoring. Fortunately, comprehensive evaluation and treatment opportunities have been available for military service members with TBI, and the US Department of Defense has been funding research into the long-term consequences of and care for TBI. 1,5
Conclusion
An estimated 20% of US service members involved in OIF and OEF may have sustained TBIs. Substantial challenges remain for the service-wide implementation of standardized protocols for TBI diagnosis. Severity- and mechanism-based TBI classification systems that include GCS, with several other clinical criteria, are helpful to establish initial prognosis, focus acute management, and guide long-term rehabilitation strategies. For mild TBIs, survival rates are high, but there may be long-term consequences on quality of life, cognition, and emotional functioning. Retrospective research supports the need for health policy changes that address the need for a longer-term approach to TBI care, and the US Military Health System has already begun implementing those changes. Additional research is needed to better understand the pathophysiologic mechanisms of TBI and to come closer to consensus on optimal treatment strategies. In the meantime, long-term follow-up care for service members who have sustained TBI will be a critical issue for the US military.
Footnotes
Authors’ Note
The opinions or assertions contained in this article are the private views of the authors and are not to be construed as official or as reflecting the views of the Department of the US Army, the US Department of Defense, or the US government.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This work is supported by the Center for Rehabilitation Science Research, Department of Physical Medicine and Rehabilitation, Uniformed Services University of the Health Sciences, Bethesda, MD, USA, awards HU0001-11-1-0004 and HU0001-15-2-0003.