
Abstract
Objectives:
Work-related traumatic injury is a leading cause of death and disability among US workers. Occupational injury surveillance is necessary for effective prevention planning and assessing progress toward Healthy People 2020 objectives. Our objectives were to (1) describe the Washington State Trauma Registry (WTR) as a resource for occupational injury surveillance and research, (2) compare the WTR with 2 population-based data sources more widely used for these purposes, and (3) compare the number of injuries ascertained by the WTR with other data sources.
Methods:
We linked WTR records to hospital discharge records in the Comprehensive Hospital Abstract Reporting System for 2009 and to workers’ compensation claims from the Washington State Department of Labor and Industries for 1998 to 2008. We assessed the 3 data sources for overlap, concordance, and case ascertainment.
Results:
Of 9185 work-related injuries in the WTR, 3380 (37%) did not link to workers’ compensation claims. Use of payer information in hospital discharge records along with the WTR work-relatedness field identified 20% more linked injuries as work related (n = 720) than did use of payer information alone (n = 602). The WTR identified substantial numbers of work-related injuries that were not identified through workers’ compensation or hospital discharge records.
Conclusions:
Workers’ compensation and hospital discharge databases are important but incomplete data sources for work-related injuries; many work-related injuries are not billed to, reported to, or covered by workers’ compensation. Trauma registries are well positioned to capture severe work-related injuries and should be included in comprehensive injury surveillance efforts.
Occupational injuries and illnesses place a heavy burden on workers, employers, workers’ compensation systems, and society overall. The national medical and productivity cost for occupational injuries and illnesses has been estimated at $250 billion annually, higher than the $219 billion estimated for cancer. 1 Although preventable, work-related traumatic injury is a leading cause of death and disability among US workers. The National Institute for Occupational Safety and Health estimated that about 2.9 million workers were treated in emergency departments for occupational injuries and illnesses in 2011, about 150000 of whom were hospitalized. More than 4300 US workers died from occupational injuries in 2012. 2
Occupational injury surveillance is necessary for effective prevention planning, evaluation, and policy development. Numerous local, state, national, and private databases are used for this purpose, but all have limitations and gaps. 3 The exploration of new data sources is motivated by barriers to full ascertainment that differentially affect databases, such as reluctance by workers, employers, and/or health care providers to file a workers’ compensation claim; nonreporting by workers to avoid retaliation or stigma; work not being identified as the cause of injury; incomplete employer injury logs; and changing workers’ compensation coverage and reporting requirements. 4 Underreporting of work-related injuries is substantial and potentially on the rise. 5 –9
Occupational injury surveillance is also central to assessing progress related to Healthy People 2020 objectives. Workers spend one-quarter of their lifetime at work or commuting, and work is one of the most important determinants of health. 10 The Council of State and Territorial Epidemiologists has collaborated closely with the National Institute for Occupational Safety and Health to increase state-based surveillance capacity to address occupational injuries as a preventable public health problem, and it has promulgated occupational health indicators that rely on data available for most states, including hospital discharge and workers’ compensation databases. 11
We adapted the World Health Organization’s injury pyramid 12 to focus on occupational injuries and available data sources (Figure). No single data source covers all occupational injuries, and many are not covered by workers’ compensation.
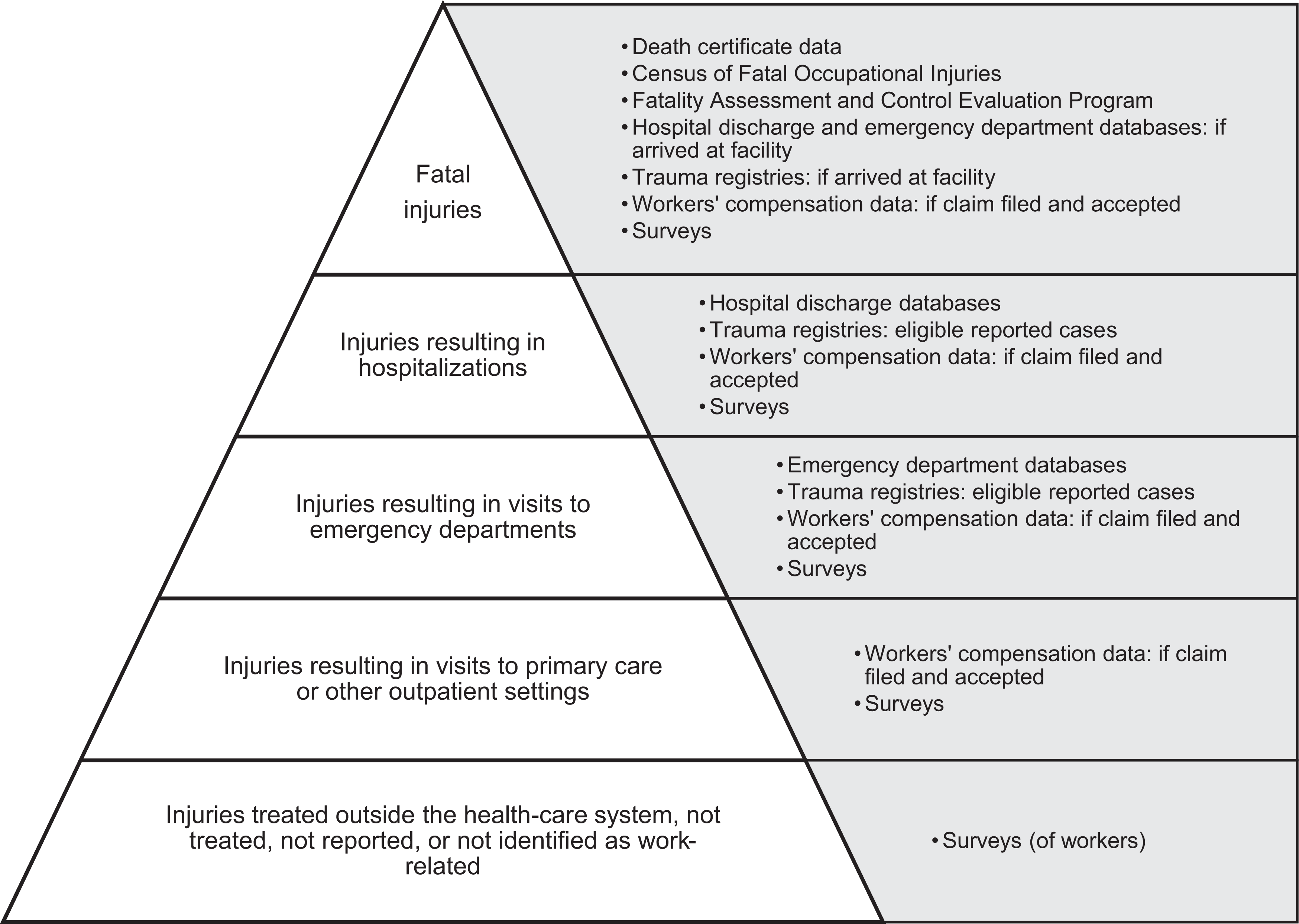
Occupational injury pyramid with examples of available data sources for each tier (adapted from the World Health Organization injury pyramid 12 ). “Surveys” may include those of health care settings and providers (eg, National Ambulatory Medical Care Survey, National Hospital Care Survey), employers (eg, Survey of Occupational Injuries and Illnesses), workers and family members (eg, Behavioral Risk Factor Surveillance System, National Health Interview Survey), or combinations of these (eg, Medical Expenditure Panel Survey).
Health care–based surveillance can avoid some reporting filters associated with workers’ compensation claims data or employer surveys. 4 However, use of hospital discharge databases requires reliance on payer fields (ie, billing to workers’ compensation) to identify work-related injuries. 11 Relying on payer information to estimate injury incidence and trends leads to numerous well-documented problems, including work injuries not reported as work related or not covered by workers’ compensation, cost shifting to other insurance coverage or to the worker, and temporal trends in health care billing practices. 7 –9,13,14
In contrast, many state trauma registries, including the Washington State Trauma Registry (WTR), include an indicator of work relatedness (distinct from payer). 14,15 Thus, trauma registries may be valuable for ascertaining serious work-related injuries not reported or billed to workers’ compensation. 4 Trauma registries also frequently include information about the use of protective devices (eg, helmets, safety restraints). 15 However, trauma registries are generally not considered population based for several reasons, which are detailed elsewhere. 16 Most important, not every health care facility that treats trauma is designated as a trauma center with mandatory reporting requirements; designation and reporting practices vary by state. 15,17 In addition, trauma registries may capture data on an increasing proportion of registry-eligible trauma cases as they evolve and mature. 15,18
Most states maintain trauma registries, but these are often untapped for occupational injury surveillance and research. Researchers in several states (eg, Alaska, Illinois, Iowa, Kentucky, Washington) are exploring these registries as a resource for occupational injury surveillance and related methodology research, 14,16,18 –22 as well as occupational injury–related research studies, including studies on racial/ethnic disparities, 23,24 nonfatal occupational injury outcomes, 25,26 and occupational health services research (eg, trauma center–based drug and alcohol screening of injured workers 27 and cost-shifting issues 13 ). In addition to state trauma registries, 2 US-based trauma registries have been used for occupational injury research: the Department of Defense Trauma Registry and the National Trauma Data Bank, a convenience sample of data submitted voluntarily by trauma centers and maintained by the American College of Surgeons. 28
Our objectives were to (1) describe the utility of the WTR as a resource for occupational injury surveillance and research, (2) compare the WTR with 2 population-based data sources that are more widely used for these purposes (ie, workers’ compensation and hospital discharge databases), and (3) compare the number of injuries ascertained by the WTR with that ascertained by other data sources, for several injury types.
Methods
Data Sources and Study Population
The 3 data sources used for this study were the WTR, the Comprehensive Hospital Abstract Reporting System (CHARS), and workers’ compensation data from the Washington State Department of Labor and Industries. The WTR and CHARS are both maintained by the Washington State Department of Health. To summarize data on overlap among the 3 data sources, we used linked data produced for 2 previous studies (the time frames of these 2 studies were contiguous but did not overlap). 14,21 The WTR and workers’ compensation data linkage covered the years 1998 through 2008, 14 and the WTR and CHARS data linkage was from 2009. 21 These studies were approved by the Washington State Institutional Review Board.
The WTR–workers’ compensation data linkage included all WTR cases (inpatient admissions and emergency department only) and compensable workers’ compensation claims (not limited to traumatic injury claims). Compensable workers’ compensation claims included accepted claims for fatalities, total permanent disability, and those involving compensation for work missed because of the injury. We excluded medical-only workers’ compensation claims.
The WTR-CHARS linkage included WTR inpatient stays and CHARS records from WTR-reporting hospitals with at least 1 International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) injury-related diagnosis (range: 800-959.9). 29 Both studies excluded patients aged younger than 16, non-Washington residents, and injuries occurring outside Washington State. Direct personal identifiers were available for linkage procedures. Records were linked and de-duplicated through The Link King, a public domain software program developed in Washington State for deterministic and probabilistic linkage of administrative records. 30 All nonexact matches were reviewed by the first author (J.M.S.) for plausibility. Further details about data linkage procedures can be found elsewhere. 14,21
Trauma Registry Data
The WTR contains mandatory reporting data for traumatic injuries that meet inclusion criteria from all state-designated trauma services (levels I-V). In 2004, the WTR trauma manager estimated that the WTR captured data on about 85% of trauma patients with injuries satisfying registry inclusion criteria. 17 The Washington State Department of Health designates trauma services as part of the comprehensive statewide emergency medical services and trauma care system. Mandatory reporting began in 1995, and trauma coverage increased as the trauma system added new hospitals. Although the WTR inclusion criteria have been refined over time, in general, reports were mandatory for adult patients who were discharged with ICD-9-CM diagnosis codes of 800-904 or 910-959 (injuries), 994.1 (drowning), 994.7 (asphyxiation), or 994.8 (electrocution) and who met at least 1 of the following criteria: trauma resuscitation team activation, dead on arrival, death during the emergency department visit or associated hospital stay, interfacility transfer by emergency medical services or ambulance, or inpatient admission of at least 48 hours. 31
The WTR conducts periodic validation studies assessing factors such as coding accuracy and completeness. The state-provided software used by the hospitals to collect and submit data to the registry contains logic and error checks that facilitate data quality and completeness. Reporting has improved over time: fewer than 5% of data were missing in the payer and work-relatedness data fields. The WTR is described in more detail elsewhere. 16,31
Workers’ Compensation Claims
Washington State has a single-payer workers’ compensation system (an exclusive State Fund) for about 70% of covered workers. Self-insured employers account for the remaining 30% of covered workers. We obtained population-based data for compensable State Fund and self-insured workers’ compensation claims from the Washington State Department of Labor and Industries, which performs the functions of an insurer for State Fund claims and administers the state workers’ compensation system for both State Fund and self-insured employers. The covered population does not include exempt/excluded employment (ie, sole proprietors, domestic workers) or workers covered by federal workers’ compensation programs.
Hospital Discharge Data
We obtained population-based data for traumatic injury-related inpatient hospital discharges from CHARS. CHARS contains inpatient hospital discharge information derived from billing records for nearly all Washington State community hospitals. 32
Work-Related Injuries
Both the WTR and CHARS have a payer category identifying the Washington State Department of Labor and Industries as a potential payer, which captures data on State Fund and self-insured workers’ compensation coverage. We used payer information to construct a binary payer variable (workers’ compensation/non–workers’ compensation). In a previous study, we found substantial concordance between WTR and CHARS records on whether the primary payer was workers’ compensation (κ = 0.79, observed agreement = 98%). 21 Using payer information is the most broadly feasible method to identify the bulk of work-related injuries in hospital discharge records. 11 In contrast to CHARS, the WTR contains a work-relatedness data field—distinct from payer—that can be used to identify work-related injuries. This work-related indicator has been shown to be highly sensitive (87%) and specific (97%) in identifying work-related injuries. 14
Analysis
We summarized the overlap in linked cases between the WTR and CHARS and between the WTR and compensable workers’ compensation claims. We compared the number of work-related cases involving fatalities, inpatient hospitalizations, burns, traumatic brain injury, and amputations in the WTR with the number of work-related cases reported by several other Washington State data sources, 16,26,33,34 matching case definitions and periods to the extent possible. For this comparison, we calculated a case ascertainment ratio, defined as the number obtained from the WTR divided by the number obtained from the comparator data source. We also summarized lessons learned from the literature and from our previous studies to present a side-by-side comparison of the attributes of these 3 data sources, as a reference for Washington State–based occupational injury surveillance and research.
Results
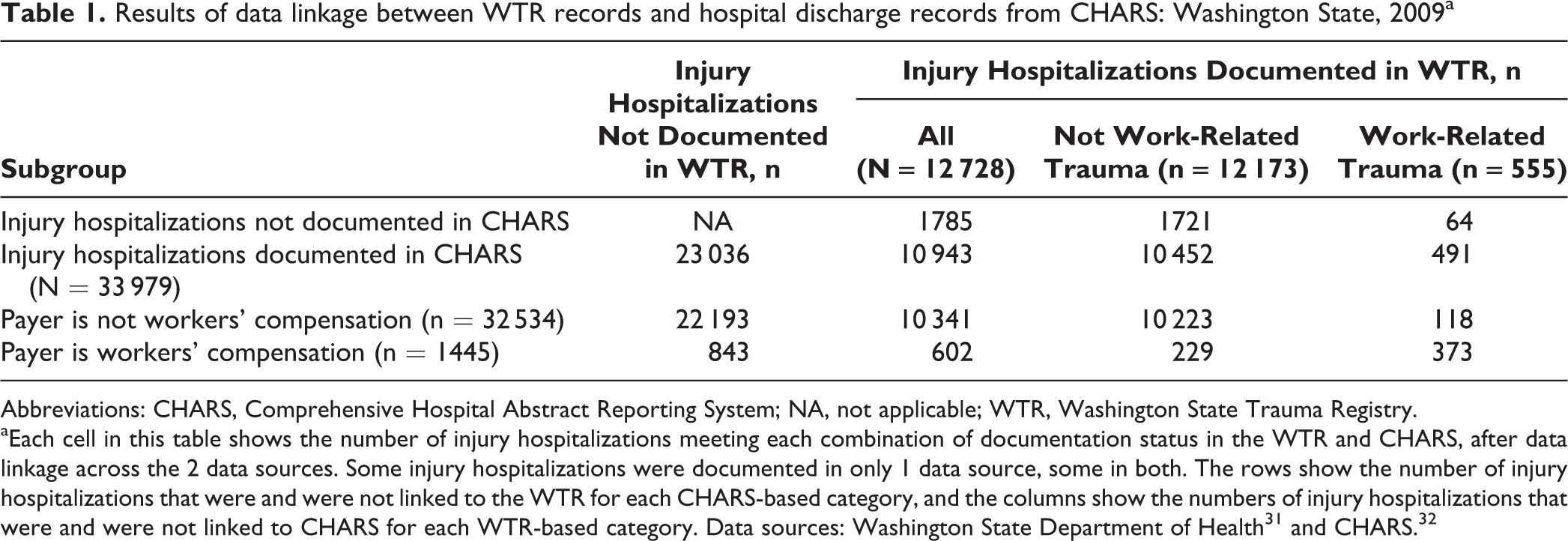
Of the 12728 eligible WTR hospitalized injury cases in 2009, 10943 (86.0%) were linked to an eligible CHARS discharge; conversely, 10943 of the 33979 eligible CHARS discharges (32.2%) linked to an eligible WTR hospitalized injury case (Table 1). Of the 720 linked WTR/CHARS discharges identified as work related by either source, 602 were identified as work related by the payer field in CHARS (373 of those 602 were identified as work related by both sources), and 118 additional discharges were identified solely by the WTR work-relatedness field (CHARS payer was not workers’ compensation). In other words, use of both the CHARS payer and the WTR work-relatedness field identified 19.6% more linked injury hospitalizations as work related than did CHARS payer alone (Table 1).
Results of data linkage between WTR records and hospital discharge records from CHARS: Washington State, 2009a
Abbreviations: CHARS, Comprehensive Hospital Abstract Reporting System; NA, not applicable; WTR, Washington State Trauma Registry.
aEach cell in this table shows the number of injury hospitalizations meeting each combination of documentation status in the WTR and CHARS, after data linkage across the 2 data sources. Some injury hospitalizations were documented in only 1 data source, some in both. The rows show the number of injury hospitalizations that were and were not linked to the WTR for each CHARS-based category, and the columns show the numbers of injury hospitalizations that were and were not linked to CHARS for each WTR-based category. Data sources: Washington State Department of Health 31 and CHARS. 32
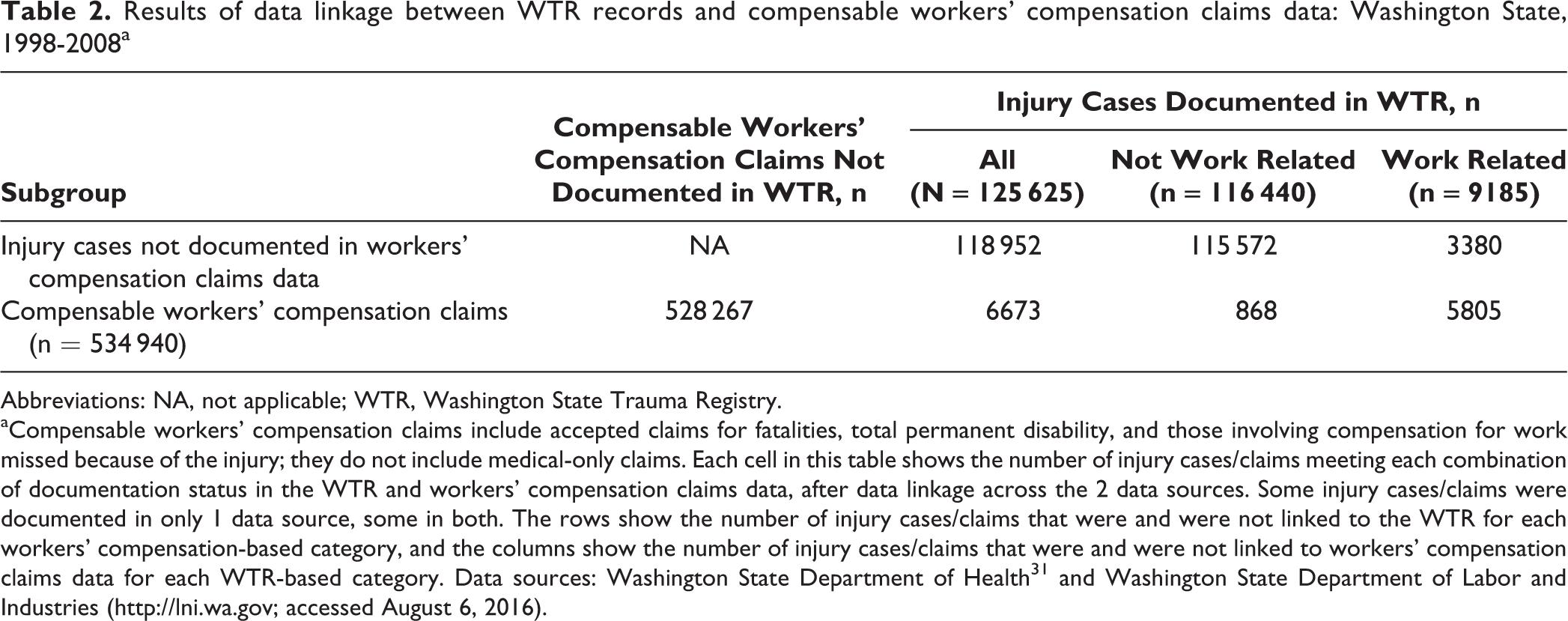
Of the 125625 eligible WTR cases from 1998 to 2008, 6673 (5.3%) were linked to a compensable workers’ compensation claim; conversely, 6673 of the 534940 compensable workers’ compensation claims (1.2%) were linked to an eligible WTR injury case. Of the 9185 work-related WTR injury cases, 63.2% (n = 5805) were linked to a compensable workers’ compensation claim, compared with 0.7% (868 of 116440) of non-work-related WTR injury cases (Table 2).
Results of data linkage between WTR records and compensable workers’ compensation claims data: Washington State, 1998-2008a
Abbreviations: NA, not applicable; WTR, Washington State Trauma Registry.
aCompensable workers’ compensation claims include accepted claims for fatalities, total permanent disability, and those involving compensation for work missed because of the injury; they do not include medical-only claims. Each cell in this table shows the number of injury cases/claims meeting each combination of documentation status in the WTR and workers’ compensation claims data, after data linkage across the 2 data sources. Some injury cases/claims were documented in only 1 data source, some in both. The rows show the number of injury cases/claims that were and were not linked to the WTR for each workers’ compensation-based category, and the columns show the number of injury cases/claims that were and were not linked to workers’ compensation claims data for each WTR-based category. Data sources: Washington State Department of Health 31 and Washington State Department of Labor and Industries (http://lni.wa.gov; accessed August 6, 2016).
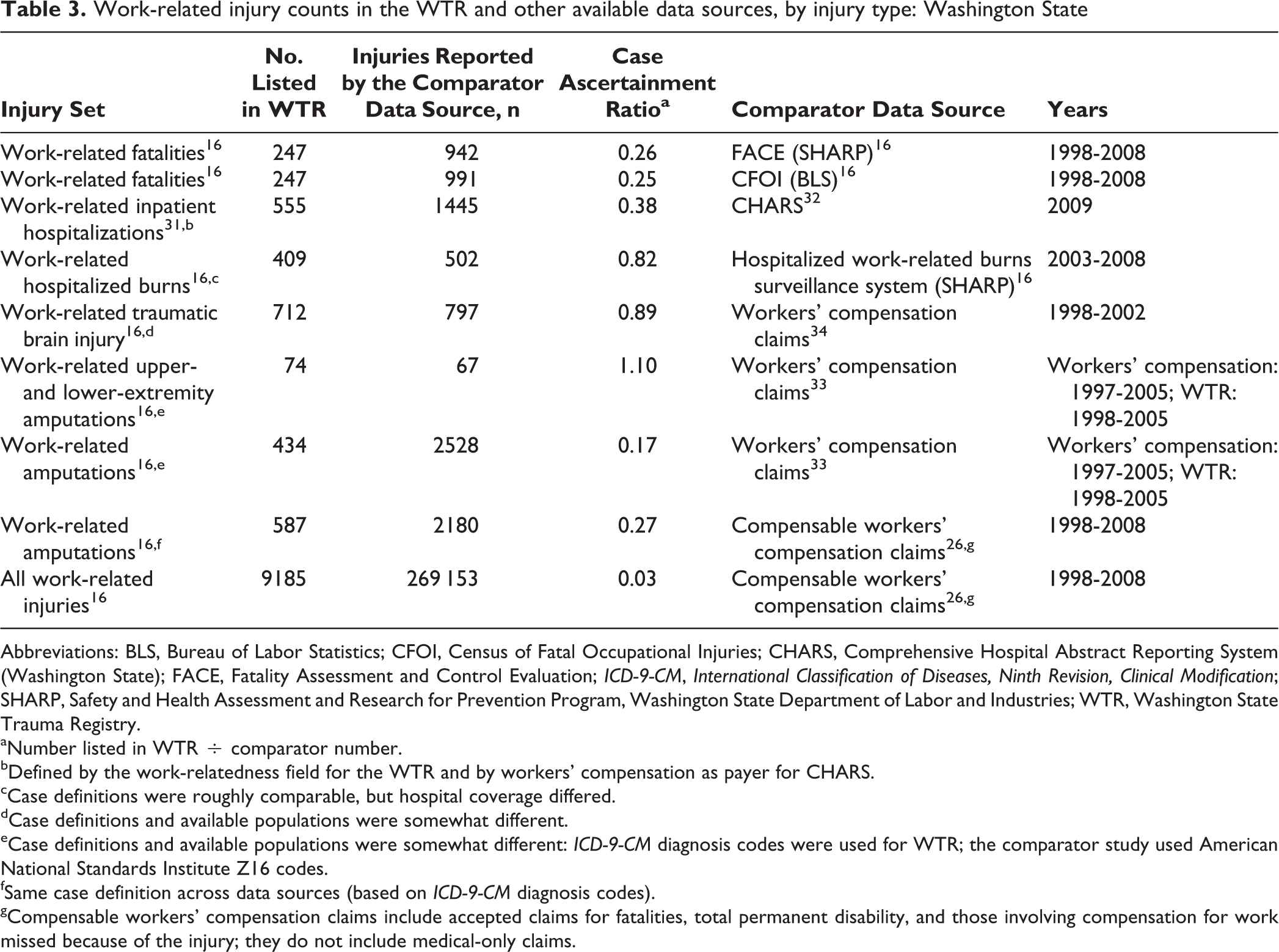
We compared the number of work-related injuries in the WTR with the number of work-related injuries in other available Washington State data sources. The WTR captured roughly 25% of occupational fatalities. Among nonfatal occupational injuries, the WTR had higher case ascertainment ratios for the more severe injury types (eg, hospitalized burns, traumatic brain injury, severe amputations of the upper and lower extremities; Table 3). The side-by-side comparison of important attributes of the WTR, CHARS, and workers’ compensation data sources revealed important similarities and differences among the 3 data sources. For example, the data generation purpose of CHARS and workers’ compensation claims data is tightly linked to billing and reimbursement, whereas the WTR is a clinical database developed for quality improvement purposes (Table 4).
Work-related injury counts in the WTR and other available data sources, by injury type: Washington State
Abbreviations: BLS, Bureau of Labor Statistics; CFOI, Census of Fatal Occupational Injuries; CHARS, Comprehensive Hospital Abstract Reporting System (Washington State); FACE, Fatality Assessment and Control Evaluation; ICD-9-CM, International Classification of Diseases, Ninth Revision, Clinical Modification; SHARP, Safety and Health Assessment and Research for Prevention Program, Washington State Department of Labor and Industries; WTR, Washington State Trauma Registry.
aNumber listed in WTR ÷ comparator number.
bDefined by the work-relatedness field for the WTR and by workers' compensation as payer for CHARS.
cCase definitions were roughly comparable, but hospital coverage differed.
dCase definitions and available populations were somewhat different.
eCase definitions and available populations were somewhat different: ICD-9-CM diagnosis codes were used for WTR; the comparator study used American National Standards Institute Z16 codes.
fSame case definition across data sources (based on ICD-9-CM diagnosis codes).
gCompensable workers’ compensation claims include accepted claims for fatalities, total permanent disability, and those involving compensation for work missed because of the injury; they do not include medical-only claims.
Key attributes of 3 occupational injury data sources: Washington State
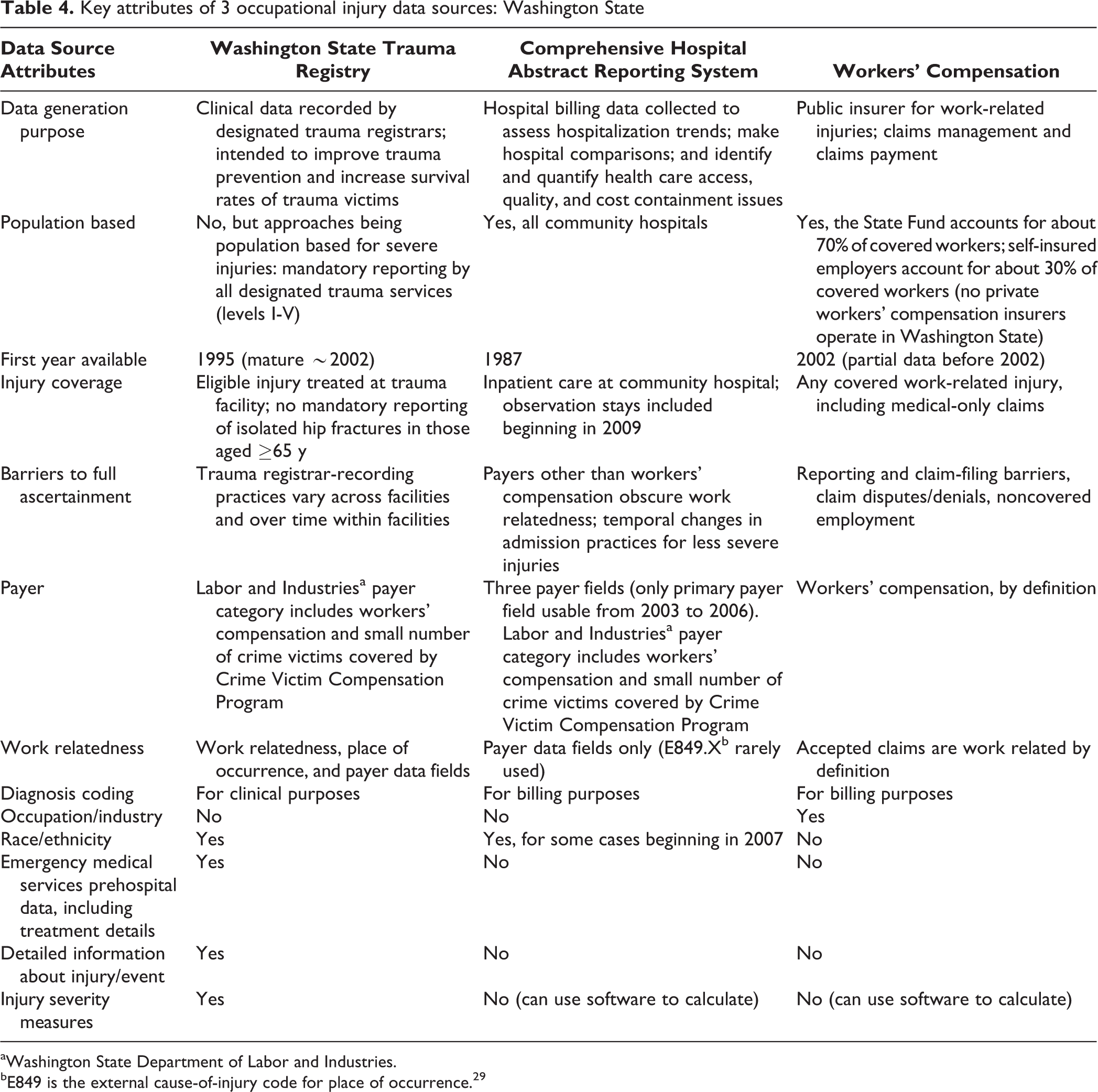
aWashington State Department of Labor and Industries.
bE849 is the external cause-of-injury code for place of occurrence. 29
Discussion
Findings from this study show that workers’ compensation and hospital discharge databases are important but incomplete data sources for work-related injuries. The WTR identified a substantial number of work-related injuries that could not be identified through workers’ compensation claims or the payer field in hospital discharge records. This finding corroborates previous research demonstrating that the payer field is an inadequate identifier of work-related injuries, primarily because many work-related injuries are not billed to, reported to, or covered by workers’ compensation. 4,5,7 –9,13,14,19 The Washington State Department of Health generally considers CHARS superior to the WTR for most surveillance purposes because of less variation in inclusion criteria and the inclusion of all hospitals regardless of trauma designation. However, the advantages of identifying work-related injuries via several data fields led to a closer look. Previous research has shown that using the work-relatedness field and/or place of occurrence data substantially augments the number of occupational injuries captured with use of payer alone. 13,14,21 In addition, having independent information about work relatedness and payer is critical for conducting research on workers’ compensation claim filing, workers’ compensation coverage, and cost shifting. 9,13 Although the WTR is technically not population based, we have found substantial similarities in occupational injury trends estimated with either trauma registry data or hospital discharge data (rate estimates were most similar when a severity threshold was applied). 18
Trauma registries capture a portion of the occupational injuries in the top 3 tiers of the injury pyramid, particularly severe nonfatal traumatic injuries. Severe nonfatal occupational injuries place a heavy and ongoing burden on workers and their families, on workers’ compensation and other insurers, and on public health and government disability systems, and they are an important public health priority. 1,2 Trauma registries—and hospital discharge databases—do not capture most occupational fatalities (top tier of the pyramid), because a substantial proportion of injury fatalities occur in the field and the worker may never arrive at a reporting hospital. The WTR captures about 25% of work-related fatalities, and the Illinois Trauma Registry captures about 20% of work-related fatalities. 22 This finding is consistent with other studies showing that a substantial proportion of injury fatalities occur on-scene before admission to a hospital (up to 72% depending on jurisdiction and setting). 35
Hospital discharge databases and trauma registries have contrasting strengths and limitations. Hospital discharge databases are typically population based and often publicly available, but they are constructed for billing and reimbursement. Greater resources are devoted to coding trauma registry records than hospital discharge records, including more input from clinical staff members, because injury-related diagnoses and severity measures are used to guide clinical management and evaluation. In addition, trauma charts are often abstracted concurrently (during the inpatient stay), providing more opportunity to correct e-codes and improve data quality before discharge. 36 Trauma registries with a work-relatedness data field and a distinct workers’ compensation payer category have the potential to minimize the proportion of severe injuries that fall into the bottom tier of the occupational injury pyramid because of their not being identified as work related, more so than hospital discharge databases. 14,21
State trauma registries vary considerably in reporting requirements, inclusion criteria, data elements, and coding conventions. 15,17 National surveys have provided comprehensive snapshots of trauma registry characteristics by state, 15,17 but data fields that are relevant to occupational injury research need to be enhanced. The list of attributes for each data source used in this study could serve as a checklist for researchers or public health personnel who are contemplating trauma registry–based occupational injury surveillance or research projects. Assessing some or all of these areas—particularly the extent to which a trauma registry is population based and mature—would be important before calculating injury rates or trends. Trauma registry–based injury rates and trends may more accurately reflect underlying injury incidence after registry maturity. 18
Strengths and Limitations
Washington State has a well-developed trauma registry and population-based hospital discharge database and is one of only 4 states with an exclusive State Fund. These features jointly facilitate the ability to conduct population-based occupational injury research. Leveraging this unusual combination of circumstances is a strength of this study.
However, the data linkage findings were based on previous research involving different time frames, and we did not have access to linked data for all 3 data sources during the same period. Although not ideal, the differing time frames allowed for a general portrayal of the overlap among these databases, which has not previously been reported.
Conclusion
Trauma registries could serve as a primary source of surveillance data to more fully describe severe occupational injuries (eg, improved case ascertainment, use of protective devices, identification of high-risk populations, and emerging injury patterns). They could also contribute valuable information to occupational injury prevention programs. Trauma registries are well positioned to capture several types of severe work-related injuries that are public health priorities, including motor vehicle crashes, falls, and traumatic brain injury.
State agencies maintain distinct silos of complementary data that could address public health policy and programmatic goals if linked or otherwise used synergistically. Trauma registries contain data fields that are not available from workers’ compensation claims (eg, race/ethnicity, injury severity measures). Data linkage has facilitated research combining the relatively rich demographic and injury data in the WTR with the relatively rich outcomes data (ie, disability, costs) from workers’ compensation claims. 26 Furthermore, trauma registries should be included in comprehensive multisource occupational injury surveillance efforts. Linking trauma registry, hospital discharge, and workers’ compensation data has increased case ascertainment and surveillance capacity, 19 and this approach broadens coverage of the occupational injury pyramid. Future research should continue to explore the use of state trauma registries around the country for occupational injury surveillance and research.
In health care databases, it is challenging to identify work-related injuries if workers’ compensation is not listed as a payer. The WTR work-relatedness field provides an unusual opportunity to overcome this barrier; however, the lack of occupation and industry information restricts what can be learned. The American College of Surgeons has made progress by developing the National Trauma Data Bank and issuing the National Trauma Data Standard, which specifies that participating trauma centers should collect occupation and occupational industry for all injuries flagged as work related. 28 However, the recent removal of workers’ compensation as a distinct payer category from the data standard will hamper occupational injury research based on the National Trauma Data Bank and may hinder surveillance efforts in those states that align their data collection efforts with the data standard. Place of occurrence e-codes and “civilian activity done for income or pay” (E000.0 in ICD-9-CM; Y99.0 in International Classification of Diseases, Tenth Revision, Clinical Modification) 37 are also valuable but underused resources for identifying occupational injuries. We recommend that those responsible for health care databases encourage full use of available work-related codes and that occupation, industry, and work status be added as required data fields to facilitate occupational injury surveillance and research that guides policy and prevention efforts.
Footnotes
Author Note
The contents of this article are solely the responsibility of the authors and do not necessarily represent the official views of the National Institute for Occupational Safety and Health.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded in part by the National Institute for Occupational Safety and Health, grants 1R03OH009883 and 1R21OH010307.