
Abstract
Objective.
We investigated the incidence of first-onset psychiatric disorders among Ohio Army National Guard members and the sociodemographic and military factors associated with these incident disorders. We aimed to identify potential risk factors and mitigating factors for a range of psychiatric disorders in a representative military sample.
Methods.
We analyzed data on a representative sample of 528 Ohio Army National Guard members who were assessed in person annually for first-onset psychiatric disorders from 2008 through 2012 using structured clinical interviews. We used a multivariable discrete-time Cox proportional hazard model to determine risk factors of first-onset anxiety or mood disorders.
Results.
The annualized incidence rate of any first-onset psychiatric disorder was 9.8 per 100 person-years at risk. Alcohol use disorder and major depressive disorder had the highest incidence rates among the unique disorders under study (5.0 and 4.2 per 100 person-years at risk, respectively). We found an association between respondents endorsing past-year deployment and a 29% increase in the risk of incident anxiety or mood disorder, whereas the past-year experience of any non-deployment traumatic event was associated with a 32% increase in risk of incident anxiety or mood disorder.
Conclusion.
Soldiers experience a substantial burden of first-onset alcohol use disorder and major depressive disorder annually; the experience of non-deployment–related traumatic events contributes substantially to increasing risk, suggesting that any effort aimed at mitigating mood and anxiety disorders in this population must consider the soldier’s life experience and military experience.
Since 2001, the U.S. military has deployed more than 2.6 million service members to support the longest sustained ground combat operation in the nation’s history. These operations require lengthy, often repetitive, and demanding deployments by both active-duty and National Guard and Reserve (reserve component) forces. 1 As the military increased occupational and personal demands on soldiers, the percentage of service members diagnosed with psychiatric disorders increased by 65% between 2001 and 2011 (2001: 5,387.1 cases per 100,000 person-years; 2011: 8,900.5 cases per 100,000 person-years), 2 the hospital rate and number of ambulatory visits caused by mental disorders doubled between 2006 and 2010, 3 and the civilian-adjusted suicide incidence rate was surpassed for the first time in 2008 (active-duty Army personnel rate in 2008: 20.2 suicides per 100,000 population; civilian-adjusted rate in 2005: 19.5 suicides per 100,000 population). 4 The simultaneous increase in military demands and psychiatric burden led to a scientific and public discourse on aspects of military service (e.g., deployment) and health policy changes (e.g., increased awareness of psychiatric disorder) that caused the increase in psychopathology among service members. 5,6 However, much of the research that supports this association between aspects of military service and psychiatric disorders is based on prevalence studies; these studies assess disease burden but not disease risk. 7 –9
Historically, the burden of mental illness has been lower for military and veteran populations than for civilians; however, recent evidence suggests this difference has reversed. 4 In 2014, Kessler and colleagues 10 showed that the prevalence of 30-day psychiatric disorders is higher among U.S. service members than among sociodemographically matched civilians. This finding fits with the contemporary understanding that military experiences may lead to an increased psychiatric burden. However, this same report indicated that most service members with disorders reported that their symptoms began before enlistment. 10 Furthermore, a population-based study published in 2014 documented that service members are more likely than non-military civilians to report adverse childhood experiences. 11 These two studies suggest an alternative mechanism for the military’s psychiatric burden that is driven by chronic, cyclical, or re-aggravated pre-military psychiatric symptomology.
Although prior research provides insight into the burden of mental illness in the military, at least three gaps in the literature limit our knowledge about its risk. First, although one in three service members has never been deployed, 12 most studies restrict analysis to deploying populations, limiting inferences about the risk associated with the more general military experience. 13 Second, previous military studies have reported either the cross-sectional prevalence or proportion of “new-onset” psychiatric disorder cases. New-onset cases are qualified only by the absence of a disorder at the baseline interview and disorder diagnosis at a later interview, rather than the absence of a lifetime history of disorder at baseline. Because a substantial proportion of psychiatric disorders begin before military service, 10 analyses of first-onset disorders is likely to overestimate the incidence rate of first-onset psychiatric disorders during service. Third, previous studies have focused on only three disorders (alcohol use disorder [AUD], major depressive disorder [MDD], and posttraumatic stress disorder [PTSD]), leading to a deficiency of data on the risk and burden of several less prevalent psychiatric disorders (e.g., phobias, dysthymia).
To address these limitations, we investigated sociodemographic and military predictors of first incidence of psychiatric disorders in a representative sample of military personnel followed during four annual study waves. We describe the first incidence estimates of the rates of psychiatric disorders in a reservist population and investigate sociodemographic and military factors that may increase the risk of anxiety or mood disorders.
Methods
Participants
The Ohio Army National Guard (OHARNG) Mental Health Initiative is an ongoing, population-based, open, prospective study that has enrolled OHARNG service members annually since 2008. We chose the OHARNG for this study because of its similarities in several key demographic and social factors to U.S. populations (e.g., proportion of high school graduates, per-capita income) and National Guard populations (e.g., age, sex, rank). 14,15 We conducted this analysis among respondents completing the in-person interview component of the larger prospective telephone survey 16 that assessed resilience and risk factors for psychiatric disorders. The validity of the data collected by telephone was assessed by comparing them with data collected through clinical psychiatric interviews, which are considered the gold standard for psychiatric assessment. 17
We used data collected from 2008 through February 2012. Sample selection occurred in three phases. First, as described elsewhere, 16 the telephone survey randomly selected currently serving OHARNG members aged ≥17 years (n=2,616). Using American Association for Public Opinion Research definitions, 18 the overall cooperation rate (defined as number of OHARNG members who consented [n=2,834] divided by number of successfully contacted people with working telephone numbers [n=4,198]) was 67.5%, and the response rate (defined as OHARNG members who completed the survey [n=2,616] plus those who consented but were ineligible [n=187] divided by the number of working telephone numbers [n=6,154] minus those disqualified [n=31]) was 43.2%; both rates were similar to other population-based military cohort studies, such as Army Study to Assess Risk and Resilience in Servicemembers (65.1% cooperation rate and 49.8% response rate). Second, we randomly invited 1,046 (40%) individuals completing the telephone survey to receive more information by postal mail and participate in the clinical interview; 952 (91%) agreed to the clinical interview. Of these 952 service members, 452 (47.5%) were not contacted before the targeted number of OHARNG service members (n=500) provided written informed consent and were enrolled in the study. Third, in 2010, 105 new service members were added to the sample using the same protocols used for the baseline sample (n=605). We excluded 77 respondents who were assessed only at baseline, leaving a final analytical sample of 528 respondents.
Measures
Diagnostic assessment
Trained doctoral- or masters-level clinicians administered the Structured Clinical Interview for DSM-IV (SCID) 19 and Clinician-Administered PTSD Scale (CAPS) 20 annually from June 2008 through February 2012 in a neutral, private location (e.g., private library room, participant’s home) to assess first incidence of Diagnostic and Statistical Manual of Mental Disorders, 4th Edition (DSM-IV) psychiatric disorders. 21 The baseline interview assessed respondents’ military, mental health, and treatment history, and social and economic circumstances, while annual follow-up assessments focused on interim mental health risk factors and diagnostic symptomology.
The SCID assesses Axis I disorders, 19 which we categorized into three classes: anxiety disorder (panic disorder, agoraphobia without panic disorder, specific phobia, social phobia, and PTSD), mood disorders (MDD, dysthymia, and bipolar disorder I/II), and substance use disorders (alcohol and/or drug abuse and/or dependence). All diagnoses were based on DSM-IV criteria, and a decision tree approach was used to record the presence or absence of each disorder for current and lifetime occurrences. We did not include sub-threshold disorders.
The CAPS was administered twice during each assessment to assess PTSD symptoms: once to assess symptoms caused by an event described by the participant as the worst event (hereinafter referred to as “potentially traumatic event”) to occur during his or her most recent deployment and a second time to assess symptoms caused by an event described by the participant as the worst event to occur outside his or her most recent deployment. 22 We defined a case of PTSD by using the frequency ≥1 and intensity ≥2 method, which is the most sensitive and the original scoring rule. 20,23 Frequency ratings of symptoms are made on a five-point scale, from 0 (never or none of the time) to 5 (daily or almost every day), and intensity symptoms are also made on a five-point scale, from 0 (none or no problem with symptom) to 5 (extreme, incapacitating). Thus, symptoms with frequency ≥1 and intensity ≥2 suggest that the person is experiencing the symptom with at least mild intensity some of the time. Participants meeting diagnostic criteria for PTSD on either CAPS were classified as having PTSD. We found monthly interrater reliability for the SCID and CAPS showed good concordance between interviewers and diagnostic assessment methods for our study (free-marginal multirater κ>0.85). 24
Potentially traumatic events
We assessed potentially traumatic events using the 16-item Life Events Checklist. The Life Events Checklist and CAPS were developed concurrently with the intent that the Life Events Checklist would screen for potentially traumatic events for the CAPS. We selected the original 16 Life Events Checklist items because of their association with PTSD symptomology. 25 In our study, participants were asked about lifetime potentially traumatic events at the baseline interview and past-year potentially traumatic events during follow-up interviews.
Sociodemographic and military characteristics
Baseline sociodemographic risk factors included cohort (baseline, dynamic cohort [i.e., the 105 people who were added after the baseline cohort, during wave 3]), age at enrollment, race (non-Hispanic white, non-Hispanic black, other), and sex. Additional baseline military risk factors included age at joining the military and lifetime deployment (yes/no). Potential time-varying risk factors included marital status (single/never married, married, previously married [separated, divorced, widowed]), education (≤high school, some college, ≥college degree), pay grade (enlisted [E1–E9], officer [warrant officer 1–5, officer 1–10]), and deployment (yes/no) since the respondent’s last interview. We also adjusted the model of mood and anxiety disorder for AUD (never, ever but not last year, last year) and drug use disorder (never/ever).
Statistical analyses
We used sequential regression multiple imputation to impute the interval censoring of disorder symptoms and missing covariates. 26 We generated five imputations. Interval censoring occurred after baseline when a respondent reported the onset of disorder symptoms at a follow-up interview but did not participate in one or more intermediate interviews. With interval censoring, it is unclear if the respondent developed the disorder at the time of interview or at an earlier time point. The timing of disorder onset mattered when we calculated the person-years at risk to estimate incident rates and the time to event in survival data analysis.
We calculated the number of service members at risk, new cases, and person-years at risk of developing each psychiatric disorder. We calculated number of service members at risk as the number of respondents who were disorder-free during their lifetime at baseline (i.e., who did not ever have a diagnosis of a disorder). New cases were respondents who did not have a diagnosis of a disorder at baseline and who received a diagnosis of the disorder during follow-up. We calculated person-years at risk of developing each psychiatric disorder from the baseline survey date to either the date of disorder onset, loss to follow-up, or end of the study period. We estimated the incidence rate of each disorder by using intercept-only Poisson regression, in which the number of new cases was the outcome and the person-years at risk was the offset. We calculated the incidence rate for an aggregate category as the first onset of any unique disorder among formerly disorder-free respondents for all unique disorders in the category at baseline. We calculated incidence rates for each unique disorder irrespective of the other disorders in the category.
We estimated the odds ratios of risk factors associated with the prevalence of mood or anxiety disorder at baseline using logistic regression. We conducted bivariate and multivariable logistic regression estimates with 95% confidence intervals (CIs) of the prevalence of mood or anxiety disorder at baseline. Among the respondents who were disorder-free at baseline and had at least one follow-up interview, we estimated hazard ratios of incidence using unadjusted and adjusted discrete-time Cox proportional hazard models. We obtained estimates and standard errors by fitting the models separately in each of the imputed datasets first and then combining the results across the five imputed datasets using Rubin’s rule. 27,28 We conducted all statistical analyses using R. 29
Results
Of the 528 study participants, most were aged 17–34 years (70.9%), male (87.7%), non-Hispanic white (88.4%), enlisted personnel (88.6%), and previously deployed (57.5%). The demographic and military characteristics of study participants and the OHARNG population were similar, except for marital status: 44.8% of study participants were single and 44.6% were married, whereas 55.4% of the OHARNG population were single and 38.5% were married (Table 1).
Characteristics of Ohio Army National Guard (OHARNG) members and a sample of the OHARNG population, United States, 2008 through 2012
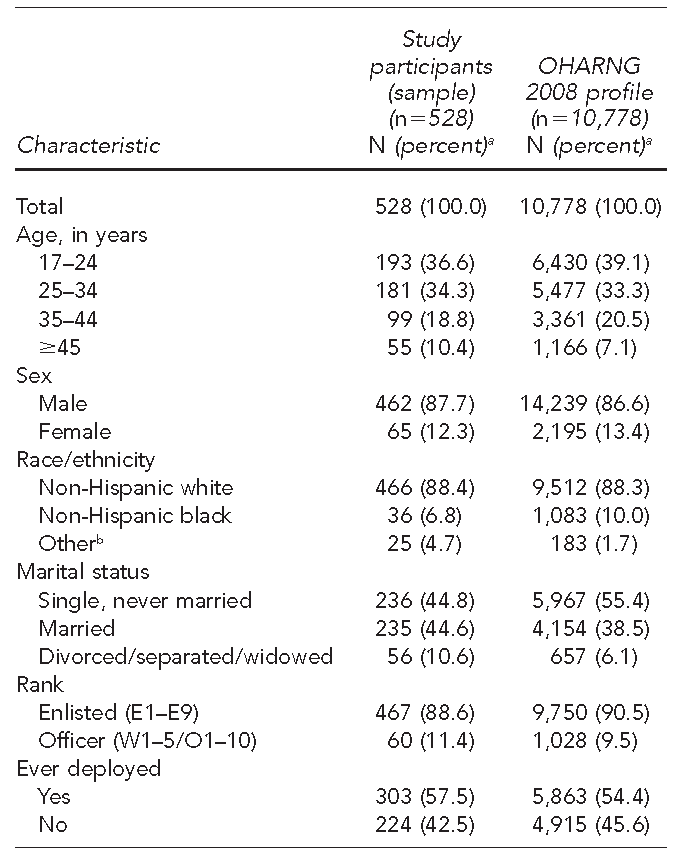
aNot all percentages total to 100 because of rounding.
bIncludes American Indian/Alaska Native, Asian American/Pacific Islander, or Hispanic
E = enlisted
W = warrant officer
O = officer
At baseline, 336 respondents met diagnostic criteria for one or more psychiatric disorders. The unadjusted and adjusted models for baseline disorders were similar for most characteristics, with the exception of education and marital status, where the bivariate association was significant and the multivariable association was not. Respondents with an anxiety or mood disorder at baseline were more likely to be female than male (adjusted odds ratio [AOR] = 1.91, 95% CI 1.12, 3.25), to have more potentially traumatic events (AOR=1.56, 95% CI 1.12, 2.16), and to meet diagnostic criteria for lifetime AUD (AOR=1.71, 95% CI 1.18, 2.49) or drug use disorder (AOR=1.65, 95% CI 1.00, 2.73). We found no association between lifetime deployment and baseline disorder (Table 2).
Bivariable and multivariable logistic regression models for lifetime prevalence of anxiety or mood disorders at baseline in a sample of Ohio Army National Guard members (n=528), United States, 2008 through 2012
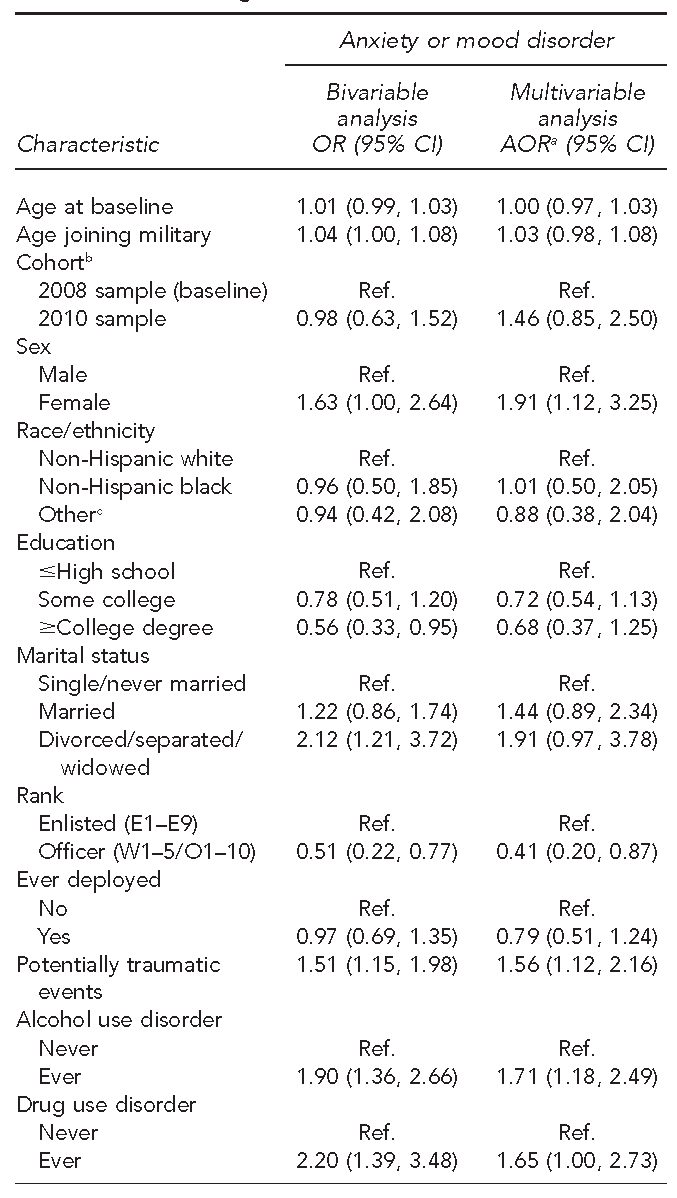
aAdjusted for all other variables in the table
bThe study sample comprised 500 people who were recruited in 2008 and 105 people who were recruited in 2010.
cIncludes American Indian/Alaska Native, Asian American/Pacific Islander, or Hispanic
OR = odds ratio
CI = confidence interval
AOR = adjusted odds ratio
Ref. = reference group
E = enlisted
W = warrant officer
O = officer
Among the 192 respondents who were disorder-free at baseline, 41 respondents were diagnosed with a first-onset psychiatric disorder during the 417 person-years of follow-up, for an incidence rate of 9.8 individuals per 100 person-years, or 9.8% per year (Figure). Although average incidence rates across the aggregate categories (i.e., anxiety disorders, mood disorders, substance use disorders) differed by <1 percentage point (range: 3.8%–4.6%), the incidence rates across component categories of mood disorders and substance use disorders were heterogeneous. The two highest incident rates for any category were for AUD (5.0%, 95% CI 3.5, 7.0) and MDD (4.2%, 95% CI 3.0, 5.7) and the two lowest rates were for drug use disorder (0.6%, 95% CI 0.3, 1.3) and bipolar II (0.5%, 95% CI 0.2, 1.1). In contrast, the incidence rates for anxiety disorders were homogenous, ranging from 0.7% (obsessive-compulsive disorder) to 1.8% (specific phobia).
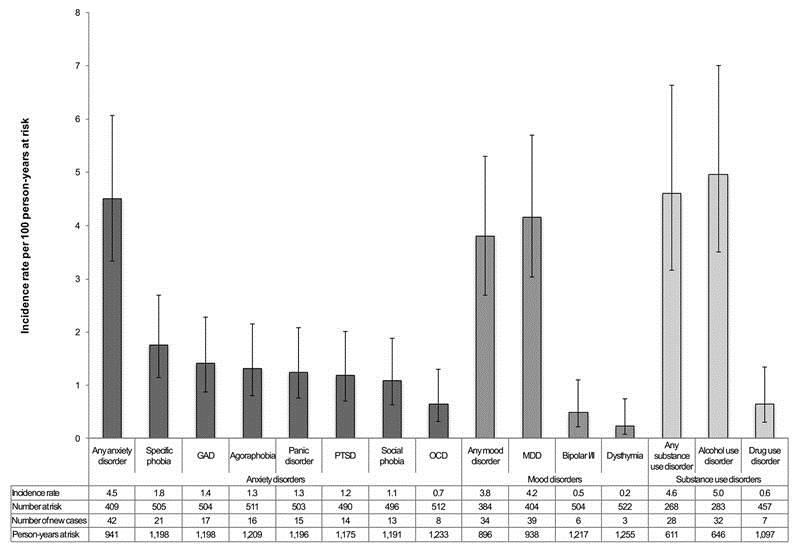
Incidence rates and 95% confidence intervals of anxiety, mood, and substance use disorders per 100 person-years at risk, Ohio Army National Guard (n=528), 2008 through 2012a
Incident anxiety or mood disorder was modestly associated with past-year deployment (adjusted hazard ratio [AHR] = 1.29, 95% CI 1.00, 1.66), non--deployment–related traumatic event in past year (AHR=1.32, 95% CI 1.10, 1.59), and lifetime potentially traumatic events (AHR=2.25, 95% CI 1.11, 4.55). Although lifetime AUD was not associated with incident risk of anxiety or mood disorder, past-year AUD was associated with a moderate increase in risk (AHR=1.68, 95% CI 1.35, 2.08). Finally, previously married respondents were 3.73 (95% CI 1.47, 9.48) times more likely than those who were single or never married to be diagnosed with an incident anxiety or mood disorder during follow-up (Table 3).
Bivariable and multivariable Cox proportional hazard models for incident anxiety or mood disorders in a sample of Ohio Army National Guard members (n=528), United States, 2008 through 2012
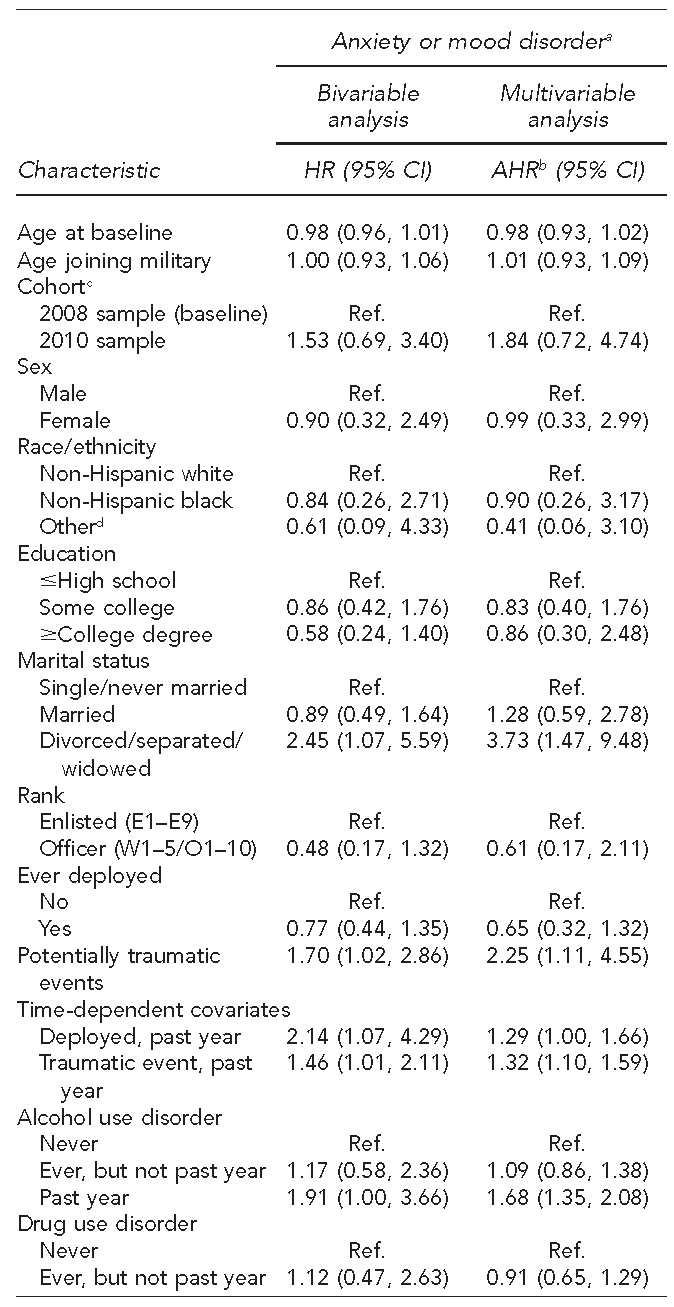
aA total of 89 episodes; 889 person-years at risk
bAdjusted for all other variables in the table
cThe study sample comprised 500 people who were recruited in 2008 and 105 people who were recruited in 2010.
dIncludes American Indian/Alaska Native, Asian American/Pacific Islander, or Hispanic
HR = hazard ratio
CI = confidence interval
AHR = adjusted hazard ratio
Ref. = reference group
E = enlisted
W = warrant officer
Discussion
In a representative sample of OHARNG members, we documented 9.8 new cases of any first incidence of DSM-IV disorder per 100 person-years at risk. Our analyses produced four major findings. First, we found that the incidence rates for disorders in this study were considerably higher than the U.S. civilian rates for AUD (5.0% vs. 1.7%) 30 and MDD (4.2% vs. 1.5%). 30,31 The higher rates reported for these two disorders could be attributed to sociodemographic differences between the military and civilian samples; military populations are predominantly younger (75% are ≤35 years of age) and male (>80%) compared with the U.S. population, which is on average 35 years of age and 51% female. Both disorders are commonly associated with younger age, 30 –32 and male sex is commonly associated with AUD. 32,33 Discrepancies in incidence rates among studies may also reflect differential exposure to predictors of mental illness. Military personnel are twice as likely as civilians to have adverse childhood experiences, including household substance abuse, physical abuse, and sexual abuse, 11 which have been documented to increase the risk of AUD and MDD. 34 –36
Second, the incidence rates for AUD, MDD, and PTSD in our study were consistent with previously published military rates. Two previous studies, the Millennium Cohort Study and the Readiness and Resilience in National Guard Soldiers study, documented first-onset psychiatric disorders in the reserve component and provide a useful comparison. Consistent with previous studies, 58% of our sample had ever deployed. 12 Insofar as deployment is a risk factor for psychiatric disorders, the incidence of AUD (5.0%) and MDD (4.2%) in our study was similar to the incidence in a non-deployed subsample of the Millennium Cohort Study but lower than the incidence in a deployed subsample reporting combat exposure in the Millennium Cohort Study 37,38 and Readiness and Resilience in National Guard Soldiers study. 39 That our incidence estimates were between those of deployed personnel with combat exposure (6.0% for AUD and 8.2% for MDD) and without combat exposure (2.8% for AUD and 2.8% for MDD) 37,38 could be attributed, in part, to the healthy warrior effect, which proposes that the military is more likely to deploy healthier personnel. 40,41 Furthermore, differences may also be associated with the increased risk of mental illness after stressful combat experiences. 42,43
Third, our observation that the incidence rate of first-onset PTSD was 1.2% per year was substantially lower than previously documented rates of first-onset PTSD among soldiers (2.9%–11.3%). 44 –46 The lower rates reported for PTSD could be attributed to the different case definitions used by studies. Among the reserve component, all previous prospective -studies assessed first-onset disorder, which is a measure combining data on disorders that were not present at baseline but were re-aggravated during a follow-up interval with data on first-incidence disorders. Because about one in three PTSD cases begin before military service, 10 and because PTSD has been documented to be cyclical in more than 25% of cases, 47,48 the higher rates documented in previous studies could be due to re-aggravated disorders.
Fourth, our finding that previously married respondents and respondents reporting exposure to a traumatic lifetime event or past-year event had the highest incidence of anxiety or mood disorder is consistent with existing literature. 49 –52 Relationship issues are common among military personnel. 53,54 Although literature examining the association among military stressors, mental health, and relationship issues 55 exists, the association between these stressors and the rising rates of divorce in military marriages is unclear. 56,57 Recent studies proposed a mediation model whereby the association between combat deployment and relationship/marital satisfaction is mediated by screening positive for PTSD. 39,58 Other studies provided evidence on the interactive effect of PTSD, alcohol misuse, intimate partner violence, and relationship issues among civilians and combat veterans. 59,60 Future analyses are needed to investigate these two hypotheses explaining the interrelationships among trauma, marital disruption, and mental illness in military personnel.
Limitations
This study had several limitations. First, the data were susceptible to information bias. Although a bias against reporting embarrassing behaviors 61 and the perception of psychiatric illness stigma are prevalent in the military, 62 we compensated for this concern by assuring participants’ confidentiality, both verbally and in writing, before volunteering for this study and by conducting all assessments in neutral locations using civilian clinicians and no military personnel. Second, these findings may not be generalizable to other reservists (e.g., Navy Reserve) from other states or active-duty military personnel. Although the OHARNG population is similar in several key demographic and social factors to the U.S. population (e.g., proportion of high school graduates, per-capita income) 14 and National Guard population (e.g., age, sex, rank), 15 our study sample had a higher proportion of respondents who were divorced, separated, or widowed, a group shown to be at increased risk for mood or anxiety disorder. The higher number of divorced, separated, and widowed respondents may have resulted in increased incidence rates. Future replication of findings in other states and components would improve confidence in our findings.
Conclusion
This study is the first to prospectively estimate first incidence of several psychiatric disorders using gold-standard clinical interviews in a representative sample of U.S. armed services members, OHARNG members. Our study advances the literature on military psychiatric epidemiology by overcoming limitations of previous studies that examined disorder prevalence or first-onset disorders or restricted analyses to deployed service members. The greater incidence of anxiety and mood disorders among previously married respondents and people experiencing lifetime and past-year potentially traumatic events underscores the need for heightened vigilance in identifying and monitoring service members who are experiencing marital disruptions, particularly in relation to other potentially traumatic experiences. The marginal association between past-year deployment and first incidence of anxiety or mood disorder suggests that studies selecting respondents on deployment status limit knowledge about the causal mechanisms that contribute to mental illness burden in the military. Therefore, future studies should consider deployment experiences as part of a broader set of life-course risk factors that can affect the psychopathology of mental illness among service members.
This article was supported by National Institute on Drug Abuse grant #T32DA031099 [DSF]. This work was supported by the Office of the Assistant Secretary of Defense for Health Affairs through the Joint Warfighter Medical Research Program under Award No. W81XWH-15-1-0080, W81XWH-07-1-0409, and W81XWH-10-1-0579 [DSF, MTB, IL, PC, GHC, LS, ES, TG, ND, TF, PLR, JRC, SG]. The U.S. Army Medical Research Acquisition Activity, 820 Chandler Street, Fort Detrick MD 21702-5014, is the awarding and administering acquisition office. Opinions, interpretations, conclusions, and recommendations are those of the authors and are not necessarily endorsed by the Department of Defense. The funding organization reviewed and approved the study but had no role in the design and conduct of the study; collection, management, analysis, or interpretation of the data; or preparation of the article.
Footnotes
The informatics support for this research was provided by the Michigan State University Clinical and Translation Sciences Institute, through its Biomedical Research Informatics Core. The Institutional Review Boards at the University Hospitals Case Medical Center and University of Toledo approved all study methods.