
Abstract
Objective.
Acute exposure to pesticides is associated with nausea, headaches, rashes, eye irritation, seizures, and, in severe cases, death. We characterized pesticide-related hospitalizations in Texas among children and teenagers for 2004–2013 to characterize exposures in this population, which is less well understood than pesticide exposure among adults.
Methods.
We abstracted information on pesticide-related hospitalizations from hospitalization data using pesticide-related International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) codes and E-codes. We calculated the prevalence of pesticide-related hospitalizations among children and teenagers aged ≤19 years for all hospitalizations, unintentional exposures, intentional exposures, pesticide classifications, and illness severity. We also calculated age- and sex-specific prevalence of pesticide-related hospitalizations among children.
Results.
The prevalence of pesticide-related hospitalizations among children and teenagers was 2.1 per 100,000 population. The prevalence of pesticide-related hospitalizations per 100,000 population was 2.7 for boys and 1.5 for girls. The age-specific prevalence per 100,000 population was 5.3 for children aged 0–4 years, 0.3 for children and teenagers aged 5–14 years, and 2.3 for teenagers aged 15–19 years. Children aged 0–4 years had the highest prevalence of unintentional exposures, whereas teenagers aged 15–19 years had the highest prevalence of intentional exposures. Commonly reported pesticide categories were organophosphates/carbamates, disinfectants, rodenticides, and other pesticides (e.g., pyrethrins, pyrethroids). Of the 158 pesticide-related hospitalizations, most were coded as having minor (n=86) or moderate (n=40) illness severity.
Conclusion.
Characterizing the prevalence of pesticide-related hospitalizations among children and teenagers leads to a better understanding of the burden of pesticide exposures, including the type of pesticides used and the severity of potential health effects. This study found differences in the frequency of pesticide-related hospitalizations by sex, age, and intent (e.g., unintentional vs. intentional).
Children and teenagers are susceptible to environmental health threats because of their behaviors, physiology, and windows of susceptibility (e.g., fetal development, puberty). 1 Children crawl and play close to the ground; put their hands or toys in their mouths; eat, breathe, and drink more per unit body weight than adults; and have greater surface area than adults compared with their weight. 1,2 These factors can increase childhood exposure to contaminants in food, air, water, and soil. 3
Pesticides are defined by the U.S. Environmental Protection Agency (EPA) as any substance that “prevents, destroys, repels, or mitigates a pest, or is a plant regulator, defoliant, desiccant, or nitrogen stabilizer.” 4 In 2007, approximately 66 million pounds of pesticides were applied to homes and gardens in the United States. Acute pesticide exposures typically occur once or during a short period of time and involve exposure to doses of pesticides that may result in the rapid onset of symptoms. Acute pesticide exposures are associated with many negative health effects, including nausea, headaches, rashes, eye irritation, seizures, and death. 6 Although chronic pesticide exposures occur during a longer time period, they typically do not involve exposure to doses of pesticides that would result in the rapid onset of symptoms; symptoms usually develop over time. Chronic pesticide exposures are associated with such negative health effects as cancers, birth defects, reproductive disorders, neurodegenerative diseases, cardiovascular disease, respiratory diseases, diabetes, chronic renal disease, and autoimmune disease. 6,7 Of U.S. poison center calls in 2014, pesticides were the eighth most common substance category involved in exposures among children aged ≤5 years. 8
The primary objective of this study was to quantify and characterize pesticide-related hospitalizations in Texas among children and teenagers. We analyzed hospitalizations by intent (unintentional or intentional), sex, age, severity of illness, and pesticide classification. A second objective was to assess the utility of International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) codes and E-codes for identifying cases. 9 –11 Hospitalization data have been used in the United States to examine pesticide-related hospitalizations, but, to our knowledge, our study is the first to examine pesticide-related hospitalizations among children and teenagers in Texas. 12,13
Methods
Data collection
We obtained data from the Texas Health Care Information Collection Texas Inpatient Public Use Data File for 2004–2013, which contains data on hospital discharges. 14,15 The dataset includes information on patient age, sex, race/ethnicity, length of hospital stay, admission status, severity of illness, patient’s county of residence, diagnoses codes, cost of hospitalization, and payer information. 14,15 Diagnoses are based on ICD-9-CM codes and E-codes.
We selected pesticide-related ICD-9-CM codes and E-codes based on the National Institute for Occupational Safety and Health Pesticide Program and scientific literature. ICD-9-CM codes assign codes for diagnoses in U.S. hospitals, whereas E-codes classify injury by intent (e.g., unintentional, homicide/assault, suicide/self-harm, undetermined) and mechanism (e.g., poisoning, motor vehicle) (Table 1). 12,13,16 We classified a case as a hospitalization resulting from unintentional pesticide exposure if the code was not for suicide or self-inflicted injury (e.g., E-codes 950.0–E950.9). We included E-code 861.4 (disinfectants) as a pesticide-related code because disinfectants are regulated under the Federal Insecticide, Fungicide, and Rodenticide Act as pesticides. 12 We defined hospitalizations resulting from intentional exposures in two ways: (1) records with E-code 950.6 (suicide or self-inflicted harm by agricultural and horticultural chemical and pharmaceutical preparations other than plant foods and fertilizers) and (2) records with codes for non-pesticide suicide or self-inflicted harm (E950.0–E950.5 and E950.7–E950.9) that were used with a pesticide-related ICD-9-CM code. 12,13,16 We first used E-codes to identify hospitalizations resulting from intentional pesticide exposures because they are used to classify injury by intent (unintentional or intentional).
Frequency of ICD-9-CM codes and E-codesa used to classify pesticide-related hospitalizations, by percentage of hospitalizations among children and teenagers aged <19 years, Texas, 2004-2013 (n=158)b
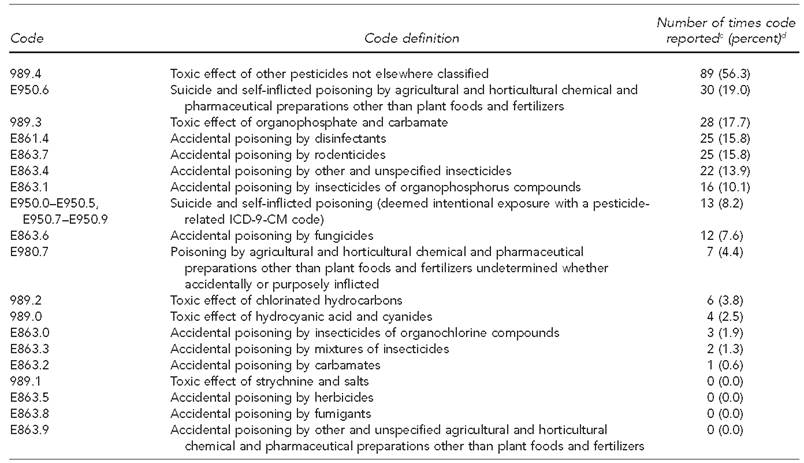
aData source: Centers for Medicare & Medicaid Services (US). ICD-9-CM diagnosis and procedure codes: abbreviated and full code titles [cited 2016 May 27]. Available from: https://www.cms.gov/Medicare/Coding/ICD9ProviderDiagnosticCodes/codes.html
bData source: Texas Department of State Health Services. Texas hospital inpatient discharge public use data file, 2004–2013. Austin: Texas Department of State Health Services, Center for Health Statistics; 2016.
cThe sum of the number of codes is greater than the number of cases because some cases included multiple pesticide-related ICD-9-CM codes and E-codes.
dPercentages total to more than 100 because some cases included multiple pesticide-related ICD-9-CM codes and E-codes.
ICD-9-CM = International Classification of Diseases, Ninth Revision, Clinical Modification
E-code = external cause of injury or poisoning code
Variables included year of hospitalization, patient demographic characteristics (age, sex, race/ethnicity), patient’s county of residence, principle diagnosis code, and 34 diagnostic codes (24 other diagnostic code fields and 10 E-code fields). In all cases, patients were defined as being aged ≤19 years (hereinafter referred to as children and teenagers). We grouped age into three categories: 0–4 years, 5–14 years, and 15–19 years. Next, we created a pesticide classification variable based on the most specific pesticide code reported, as described in previous research. 12 For example, if the ICD-9-CM code was 989.4 (other pesticide) and the E-code was E863.7 (rodenticide), the case was coded as rodenticide. We based categories used for classification on the chemical categories in the ICD-9-CM codes and E-codes, including disinfectants, fumigants, fungicides, herbicides, hydrocyanic acid and cyanides, rodenticides, chlorinated hydrocarbons, strychnine, and salts; organochlorines; organophosphates/carbamates; and other pesticides. Codes used to indicate other pesticides included 989.4, E863.3, E863.4, and E980.7. -Organochlorines and chlorinated hydrocarbons were both classified as organochlorines. E-codes were used first to identify hospitalizations resulting from intentional pesticide exposures because they are used to classify injury by intent (unintentional or intentional). We assessed severity of illness by using the All Patient Refined (APR) Diagnosis Related Group (DRG) from the 3M™ APR-DRG (3M Company, Salt Lake City, Utah). 15 APR-DRG classifies patients with multiple illnesses or issues that involve multiple organs as having higher severity of illness. Each patient is assigned a severity-of-illness score according to distinct patient attributes, such as comorbid or preexisting conditions (e.g., heart disease or diabetes). 17 We used 2010 decennial population data from the U.S. Census Bureau for children and teenagers. 18
Data analysis
We used SAS® version 9.4 for data management and descriptive statistics. 19 We used Microsoft® Excel 2013 to calculate (1) the frequency of ICD-9-CM codes and E-codes used for pesticide-related hospitalizations by percentage of hospitalizations and (2) the frequency and prevalence (and 95% confidence intervals [CIs]) of all pesticide-related hospitalizations, hospitalizations resulting from unintentional pesticide exposures, and hospitalizations resulting from intentional pesticide exposures. We further analyzed these data by sex, age category, severity of illness, and pesticide classification. We also assessed the utility of ICD-9-CM codes and E-codes for identifying cases.
Results
We identified 158 pesticide-related hospitalizations using ICD-9-CM codes and E-codes. The two most common ICD-9-CM codes were 989.4 (other pesticides, n=89, 56.3%) and 989.3 (organophosphates/carbamates, n=28, 17.7%). The four most common E-codes were E950.6 (suicide and self-inflicted poisoning associated with pesticides, n=30, 19.0%), E861.4 (disinfectants, n=25, 15.8%), E863.7 (rodenticides, n=25, 15.8%), and E863.4 (other pesticides, n=22, 13.9%) (Table 1).
Frequency and prevalence of pesticide-related hospitalizations
Of the 158 pesticide-related hospitalizations among children and teenagers in Texas during 2004–2013, the average annual number of hospitalizations was 15.8 (range: 8–23) (Figure). Boys accounted for 65.8% of pesticide-related hospitalizations, with a prevalence of 2.7 per 100,000 population (95% CI 2.2, 3.2). Overall, children aged 0–4 years had the highest prevalence of pesticide-related hospitalizations per 100,000 population (5.3) compared with children and teenagers aged 5–14 years (0.3) and teenagers aged 15–19 years (2.3) (Table 2).
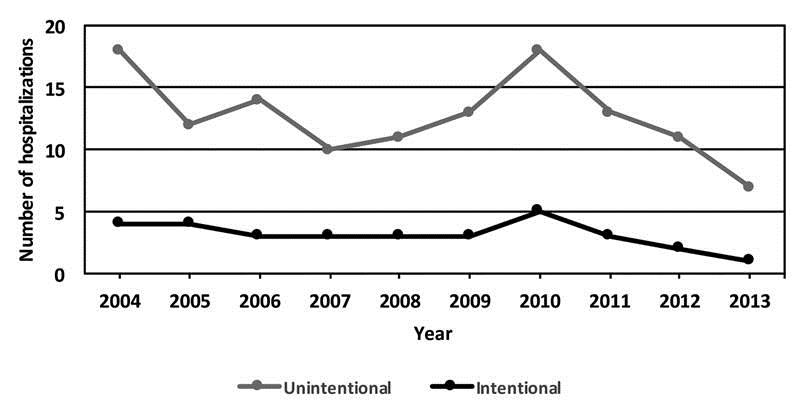
Number of hospitalizations for intentional and unintentionala pesticide exposure among children and teenagers aged ≤19 years, by year, Texas, 2004-2013b
Frequency and prevalence of pesticide-related hospitalizations among children and teenagers aged <19 years, by sex, age, and severity of illness, Texas, 2004-2013a
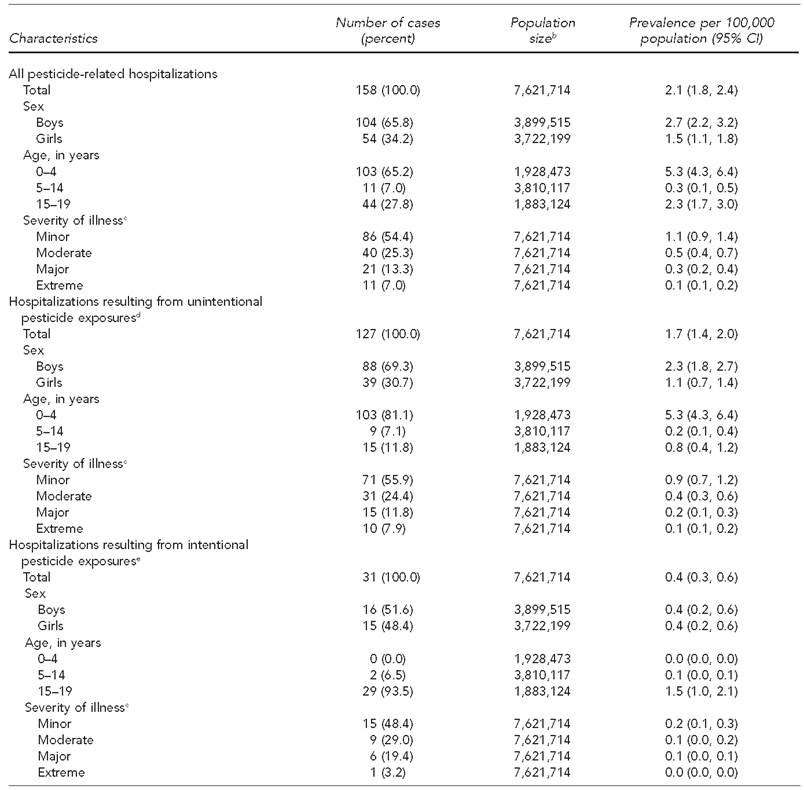
aData source: Texas Department of State Health Services. Texas hospital inpatient discharge public use data file, 2004-2013. Austin: Texas Department of State Health Services, Center for Health Statistics; 2016.
bData source: Census Bureau (US). American FactFinder: 2010 Census summary file 1, table PCT12 [cited 2016 Jan 9]. Available from: http://factfinder.census.gov/faces/nav/jsf/pages/index.xhtml
cIllness severity is based on the 3M™ All Patient Refined Diagnosis Related Group, which defines severity of illness into four categories based on the diagnosis, as well as age and presence of comorbid or preexisting conditions.
dUnintentional pesticide exposures are those that were deemed to occur without intent of harm or were not done on purpose. eIntentional pesticide exposures are those that were deemed to occur with intent of harm or were done on purpose.
CI = confidence interval
Hospitalizations resulting from unintentional pesticide exposures
From 2004 to 2013, 127 pesticide-related hospitalizations among children and teenagers resulted from unintentional pesticide exposures. The average number of hospitalizations resulting from unintentional pesticide exposures was 12.7 per year (range: 7–18) (Figure). The prevalence of hospitalizations resulting from unintentional pesticide exposures was 1.7 per 100,000 population (95% CI 1.4, 2.0) (Table 2). Overall, children aged 0–4 years had the highest prevalence of hospitalizations per 100,000 population resulting from unintentional pesticide exposure (5.3) compared with children and teenagers aged 5–14 years (0.2) and teenagers aged 15–19 years (0.8) (Table 2).
Hospitalizations resulting from intentional pesticide exposures
We identified 31 pesticide-related hospitalizations resulting from intentional exposures among children and teenagers. The average number of hospitalizations resulting from intentional pesticide exposures was 3.1 (range: 1–5) (Figure). The prevalence of hospitalizations per 100,000 population resulting from intentional pesticide exposures for children and teenagers was 0.4 (95% CI 0.3, 0.6). The sex-specific prevalence per 100,000 population was 0.4 (95% CI 0.2, 0.6) for both boys and girls. Teenagers aged 15–19 years had a higher prevalence per 100,000 population (1.5) compared with children and teenagers aged 5–14 years (0.1). No children aged 0–4 years were hospitalized for intentional pesticide exposures (Table 2).
Severity of illness
By severity, of the 158 pesticide-related hospitalizations, 86 (54.4%) were minor, 40 (25.3%) were moderate, 21 (13.3%) were major, and 11 (7.0%) were extreme. We found similar results for hospitalizations resulting from unintentional and intentional pesticide exposures (Table 2). We identified four deaths that were all determined to result from an unintentional pesticide-related exposure: three were girls, one was a boy, two were aged 5–14 years, and two were aged 15–19 years.
Pesticide classification
The most common categories of pesticide class based on the most specific pesticide ICD-9-CM and E-code available included other pesticides (n=58, 36.7%), organophosphates/carbamates (n=28, 17.7%), disinfectants (n=25, 15.8%), and rodenticides (n=25, 15.8%). The prevalence of pesticide-related hospitalizations per 100,000 population was 0.8 (95% CI 0.6, 1.0) for other pesticides, 0.4 (95% CI 0.2, 0.5) for organophosphates/carbamates, 0.3 (95% CI 0.2, 0.5) for disinfectants, and 0.3 (95% CI 0.2, 0.5) for rodenticides. For hospitalizations resulting from unintentional pesticide exposures, the most common categories were other pesticides (n=37, 29.1%), disinfectants (n=25, 19.7%), rodenticides (n=25, 19.7%), and organophosphates/carbamates (n=21, 16.5%). The most common categories for hospitalizations resulting from intentional pesticide exposures were other pesticides (n=21, 67.7%) and organophosphates/carbamates (n=7, 22.6%) (Table 3).
Frequency and prevalence of pesticide classifications for hospitalizations for intentional and unintentional pesticide exposure among children and teenagers aged <19 years, by pesticide classification, Texas, 2004–2013a
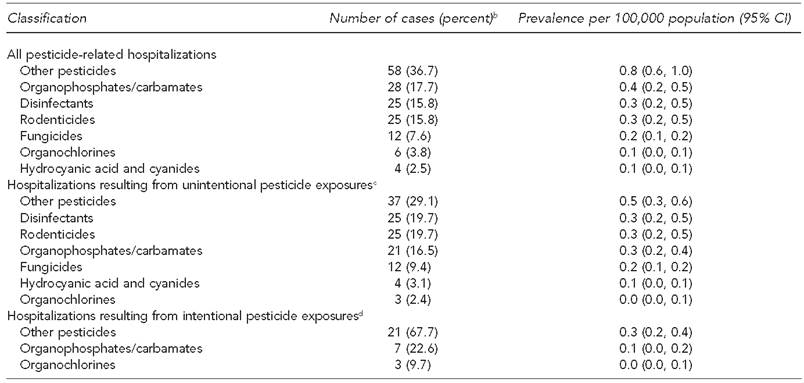
aData source: Texas Department of State Health Services. Texas hospital inpatient discharge public use data file, 2004-2013. Austin: Texas Department of State Health Services, Center for Health Statistics; 2016.
bSome percentages do not total to 100 because of rounding.
cUnintentional pesticide exposures are those that were deemed to occur without intent of harm or were not done on purpose.
dIntentional pesticide exposures are those that were deemed to occur with intent of harm or were done on purpose.
CI = confidence interval
Utility of ICD-9-CM codes and E-codes for identifying cases
Of the 127 unintentional pesticide exposures, we identified 96 (75.6%) hospitalizations resulting from unintentional pesticide exposures by using ICD-9-CM codes alone and 31 (24.4%) by using E-codes. A total of 110 (86.6%) hospitalizations resulting from unintentional pesticide exposures would have been identified by using E-codes alone, with an additional 17 (13.4%) identified using ICD-9-CM codes. Of the 31 intentional pesticide exposures, we identified 30 (96.8%) hospitalizations resulting from intentional pesticide exposures by using E-code 950.6. We identified the remaining hospitalizations resulting from intentional exposures by using E-codes 950.0–950.5 or 950.7–950.9 with a pesticide-related ICD-9-CM code.
Discussion
Of the 158 pesticide-related hospitalizations among children and teenagers, 127 (80.4%) resulted from unintentional exposures and 31 (19.6%) resulted from intentional exposures. This finding differs from national data in the American Association of Poison Control Centers’ National Poison Data System, which reports that 94% of all pesticide ingestions were unintentional. 20 Because there is no surveillance system to capture data on pesticide exposures, the total burden of pesticide exposures in Texas and the United States cannot be estimated. However, globally in 2002, pesticide ingestion resulted in 186,000 deaths. 21
We found that pesticide-related hospitalizations resulting from unintentional and intentional pesticide exposures decreased from 2004 to 2013. It is unclear why this decrease occurred or if it will continue. Additionally, the increase in both unintentional and intentional pesticide-related hospitalizations in 2010 cannot be explained. However, multiple factors (e.g., vector-borne disease outbreaks such as West Nile virus) could affect pesticide exposures and ultimately hospitalizations.
In our study, teenagers aged 15–19 years had the highest prevalence of intentional pesticide exposures compared with children aged 0–4 years and children and teenagers aged 5–14 years. In 2014, teenagers and young adults aged 15–24 years in the United States had a suicide rate of 11.6 per 100,000 population. 22 Additionally, 15.9% of all suicide deaths resulted from poisonings, including poisoning by pesticides. 22 Based on this study’s findings and known suicide statistics, future research should address intentional pesticide exposures among teens aged 15–19 years.
The findings of this study are supported by the scientific literature. At least two studies found that males of all ages had higher rates of pesticide-related hospitalizations than females in California and Louisiana. 12,13 In a 2010 study, Badakhsh et al. characterized pesticide-related hospitalizations for Louisiana from 1998–2007 for all populations and found that pesticide-related hospitalizations decreased during the time period. 12 In a 2006 study, Mehler et al. characterized pesticide-related illnesses and injuries for California from 1994–1996 using California Pesticide Illness Surveillance Program data, poison control data, hospitalization data, and death certificates. 13 Both studies found that intentional pesticide-related hospitalizations accounted for more than 25% of cases, 12,13 whereas we found that intentional pesticide-related hospitalizations accounted for about 18% of cases. This disparity could be caused by differences in study populations: we focused on children and teenagers, whereas both other studies focused on all age groups. 12,13 Badakhsh et al. calculated an average of 12 pesticide-related hospitalizations per year for children aged ≤18 years, whereas we calculated an average of 15.8 pesticide-related hospitalizations per year for children and teenagers aged ≤19 years. 12 Despite similar numbers of pesticide-related hospitalizations, the rates differed, perhaps because of differences in the definition of children or size of the state populations. 12
Our study found that the most common pesticide categories involved in pesticide-related hospitalizations were organophosphates/carbamates and other pesticides (e.g., herbicides, pyrethroids/pyrethrins) based on ICD-9-CM and E-code classifications. This finding is supported by existing literature, which found that 2,4-dichlorophenoxyacetic acid (2,4-D), glyphosate, mecoprop, pendimethalin, dicamba, trifluralin, and pelarganoc acid, malathion, carbaryl, and pyrethroids were the 10 most commonly used active ingredients in conventional pesticides in 2006–2007 for the home and garden market sector. 5 These ingredients fall into the pesticide categories of herbicides, organophosphates/carbamates, and pyrethroids. Additionally, a pesticide inventory conducted in Webb and Hidalgo counties in Texas found that pyrethroids were the most commonly reported pesticides. 23
Limitations
This study had several limitations. First, hospitalization data captured only data on acute exposures and did not capture data on chronic exposures or long-term consequences. Second, data on visits to urgent care, primary care physicians, and emergency departments were not included in the dataset; the dataset did not capture data on cases that did not require a -hospitalization. Third, some cases of pesticide-related hospitalization may have been missed by using the available ICD-9-CM codes and E-codes. Fourth, because of data collection and billing cycles, not all hospitalizations may have been included in the dataset. 15 Fifth, some cases may have been misclassified, because some of the pesticide-related categories can include substances other than pesticides. For example, formaldehyde is reported under E-code E861.4 (disinfectant), but it has many uses, such as in building materials, household products, and pesticides. 24 Lastly, the use of the APR-DRG for illness severity was a limitation because this classification is dependent on the underlying problem, which can be confounded by complicating or comorbid conditions. Illness severity is patient- and disease-specific; thus, interpretation of illness severity should be conducted with caution. 25 For example, a child with a preexisting condition may not have the same adverse health effects that a healthy child would have as a result of pesticide exposure.
Strengths
To our knowledge, this study is the first to use hospitalization data to identify pesticide-related hospitalizations in children and teenagers in Texas. In addition, we used both ICD-9-CM and E-codes for case definition, which allowed for more potential cases to be identified. We also analyzed all pesticide-related codes for each case to report the most specific pesticide code, which allowed for understanding of the most commonly reported pesticide categories along with the most common potential health effects. Although this study reported only a snapshot of pesticide exposures that resulted in hospitalizations in Texas, our findings are consistent with other state-level data, suggesting that similar patterns exist throughout the United States. Lastly, to account for the limited sample size and to capture data on other exposures, we are analyzing poison center data to describe exposures reported to poison centers; this dataset has approximately 61,000 exposures for children and teenagers from 2000–2013 in Texas. 26
Conclusion
Limited information is available on the prevalence of pesticide exposures among children and teenagers in Texas and the United States. We found that age was an important variable in determining the risk of hospitalization for both unintentional and intentional pesticide exposures. In addition, boys had a higher prevalence of pesticide-related hospitalizations than girls. These data can be used to develop tailored interventions to address the use of pesticides for self-harm among teenagers. The present study also supports the use of a surveillance program to address acute pesticide poisonings among children and teenagers, such as the Pesticide Exposure Surveillance in Texas program, which requires the reporting of known and suspected acute occupational pesticide poisonings. 27
The burden of pesticide exposures among children and teenagers in Texas and the United States can begin to be understood by analyzing Texas hospitalization data; however, additional studies using other state or national data (e.g., poison center data, mortality data, cancer registry data) should be conducted to capture data on pesticide-related exposures throughout the United States. Research is also needed to characterize risk factors for pesticide exposures to guide interventions.
Footnotes
This research was deemed exempt by the Texas A&M Institutional Review Board (study #2015-0563M).