
Abstract
Objective.
Necrotizing fasciitis (NF) is a severe manifestation of invasive group A streptococcal (iGAS) infection. NF is a rapidly progressive infection of the subcutaneous tissues, including the fascia, and accurate diagnosis and prompt treatment are critical. Population-based surveillance is conducted for iGAS, including the severe manifestations of NF, by the federally funded Active Bacterial Core surveillance (ABCs) program.
Methods.
We used administrative claims data from a large managed care organization in Tennessee to enhance the public health surveillance for NF iGAS. For the period 2003–2012, we identified cases of NF in Tennessee by searching the claims database for diagnostic codes indicating the diagnosis of NF. We compared these cases with cases detected in selected Tennessee counties by ABCs.
Results.
Of 356 managed care patients with a diagnostic code indicating NF, we determined that 20 (6%) patients had been hospitalized with iGAS infection and, therefore, were likely to be true NF cases. Of these 20 patients, only 11 matched with patients identified by ABCs; nine patients had not been previously identified by ABCs. During the same time period, 54 patients with NF were ascertained by ABCs.
Conclusion.
Administrative claims data have the potential to augment disease surveillance but require a large investment in resources compared with the few NF cases identified.
Invasive infections caused by group A Streptococcus (GAS) or Streptococcus pyogenes include sepsis, bacteremic pneumonia, necrotizing fasciitis (NF), and streptococcal toxic shock syndrome, which cause substantial morbidity and mortality. In 2013, an estimated 11,500 cases and 1,100 deaths resulting from invasive GAS (iGAS) infection occurred in the United States. iGAS infections result in hospitalization for 92% of cases. 1 –3 Although iGAS NF is relatively uncommon (accounting for 6.7% of the estimated 10,700–13,400 cases of iGAS each year in the United States), prompt diagnosis and appropriate treatment is critically important because of the speed with which the infection can progress. The case fatality rate of NF as detected in the Active Bacterial Core surveillance (ABCs) program is approximately 29%. 1
Complete and timely reporting of these events is an important attribute of population-based public health surveillance. The Centers for Disease Control and Prevention began active surveillance for iGAS infections, including NF, in 1995 as part of the ABCs program of the Emerging Infections Program. Since then, the surveillance network has grown to 10 U.S. sites and includes surveillance of more than 32 million people in California, Colorado, Connecticut, Georgia, Maryland, Minnesota, New Mexico, New York, Oregon, and Tennessee. In Tennessee, five core metropolitan regional areas, covering 20 counties (approximately 3.7 million people), are included in the surveillance population.
In the United States, case ascertainment for surveillance traditionally comes from multiple sources, including hospitals, emergency rooms, and physicians’ offices. The use of administrative data for surveillance may improve case identification and determination of disease burden. In Tennessee, health insurance plans could supplement surveillance activities through submission of administrative medical claims data to enhance reporting, because approximately 85% of Tennessee residents have health insurance. 4 –10 To examine the utility of administrative medical claims data for iGAS surveillance activities, we assessed medical claims data from BlueCross BlueShield of Tennessee (BCBST) members and compared them with Tennessee ABCs data.
Methods
BCBST is a managed care organization in Tennessee that serves about half of Tennessee residents. The organization’s administrative claims system captures data from medical encounters that insured members have with the health-care system, including hospitalizations, outpatient visits, medical procedures, and laboratory testing. Data collected include member-specific information (e.g., ZIP code of the member’s residence at the time of service), International Classification of Diseases, Ninth Revision (ICD-9) codes indicating diagnoses and Current Procedural Terminology codes indicating procedures, dates of services, the medical provider rendering the service, and information about the facility where the service occurred. 11,12
We searched for the ICD-9 code for NF (728.86) among primary and admitting diagnoses, along with eight additional diagnoses on a given inpatient stay claim. By using these 10 diagnosis codes (i.e., admitting diagnosis, primary diagnosis, and up to eight additional diagnoses from the inpatient stay) from each medical service rendered, we were able to gather a larger collection of possible NF cases for review. We collected data retrospectively for services rendered from January 1, 2003, through December 31, 2012. To increase specificity, we also searched BCBST claims data for visits where both a diagnosis of NF (ICD-9 code 728.86) and a diagnosis of GAS (ICD-9 code 041.01) appeared. We included cases occurring only in residents of the 20 ABCs counties (which expanded from 11 counties prior to 2010 to 20 counties in 2010). An administrative claim for a service rendered can contain multiple lines representing different facets of the patient encounter (i.e., different diagnoses or procedures). For this reason, only a single entry was kept per claim number, indicating that single point of service to prevent duplication. We collected additional claims information for 30 days before and after an indicated NF diagnosis, which allowed medical records to be reviewed at other possible health-care facilities to help identify the correct facility where NF was first diagnosed.
ABCs program
We identified iGAS cases through active population- and laboratory-based surveillance of ABCs covering a surveillance catchment area of 11 Tennessee counties from 2003 through 2009 (i.e., Shelby, Davidson, Robertson, Sumner, Cheatham, Dickson, Williamson, Rutherford, Wilson, Knox, and Hamilton counties) and an additional nine counties in 2010 (i.e., Madison, Union, Anderson, Roane, Loudon, Blount, Sevier, Jefferson, and Grainger counties). ABCs defined a case of iGAS NF infection as a resident of the surveillance catchment population during the study period (January 2003 through December 2012) from whom GAS was isolated from a normally sterile site (e.g., blood, cerebrospinal fluid) or from a wound culture (e.g., muscle, fascia) accompanied by the diagnosis of NF. As part of the ABCs program, active surveillance for positive blood cultures and by infection-control nurses for NF is conducted in Tennessee, but routine active surveillance of wound cultures is not conducted. Medical records are reviewed by surveillance staff members for each suspected case of NF. Based on medical record review, we documented whether or not NF was confirmed by reviewing surgical and pathology reports.
We used a matching algorithm to compare patients identified by ABCs with patients found in BCBST records. 7 We compared the first and third characters of the first names of potential matching patients, as well as the first and third characters of their last names. We also compared the month, day, and year of the patient’s date of birth and sex. If all these comparisons yielded positive results, we declared a match. A match was also declared for reversal of first and last names, match of everything but first names, match of everything but year of birth, match of everything but sex, and match of everything but day of birth. The datasets were small enough to allow visual inspection for false matches. One such erroneous match was removed. We performed analyses using SAS® version 9.4, 13 Stata®/IC 13, 14 and Microsoft® Excel 2013 to calculate rates, run descriptive analyses, and conduct t-tests and Pearson’s χ2 determinations.
Results
During the study period, 17,417 claims in the BCBST database had the ICD-9 diagnosis code of 728.86 (NF) from patients who resided in ABCs counties (Figure 1). Of these 17,417 claims, 15,464 were unduplicated claims representing 356 unique patients, of whom 114 had no inpatient hospital claims, making the diagnosis of NF likely erroneous or misdiagnosed because NF is a severe disease requiring hospitalization. Of the 242 patients with hospital claims, charts were not available to review for 20 patients.
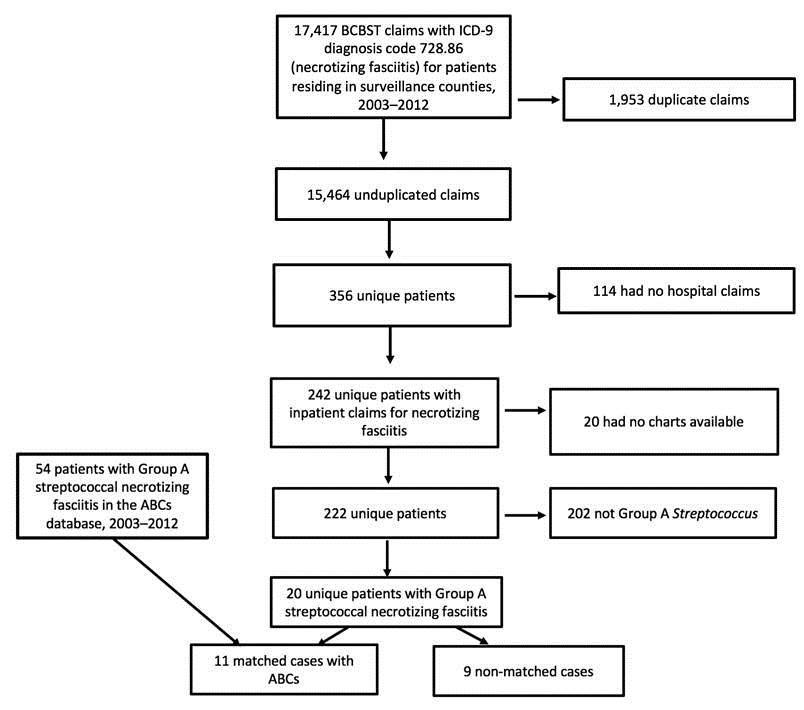
BlueCross BlueShield of Tennessee (BCBST) and Tennessee Emerging Infections Program Active Bacterial Core surveillance (ABCs) necrotizing fasciitis cases, Tennessee, 2003–2012
We performed medical record review for 222 patients: 20 (9%) had culture-positive GAS and 202 (91%) did not have any positive cultures from sterile sites or from a wound for GAS. During the same time period, 54 cases of GAS NF were identified within the Tennessee ABCs catchment area. This review provided a sensitivity of 20% (11/54) and positive predictive value (PPV) of 55% (11/20) for BCBST NF patients compared with ABCs NF patients. Of the 20 BCBST patients who were confirmed by medical record review, 11 matched with those in the ABCs database and nine did not. None of the unmatched patients had positive iGAS blood cultures, compared with eight of 11 matched patients. All of the unmatched patients had a confirmed diagnosis of iGAS by either wound (n=6) or abscess/tissue culture (n=3); three of the matched patients were confirmed by a wound/tissue or abscess culture positive for GAS (Figure 2). NF was specified in the operative note in nine of 11 matched patients and in all nine unmatched patients, and was specified in the pathology report of six matched patients and two unmatched patients.
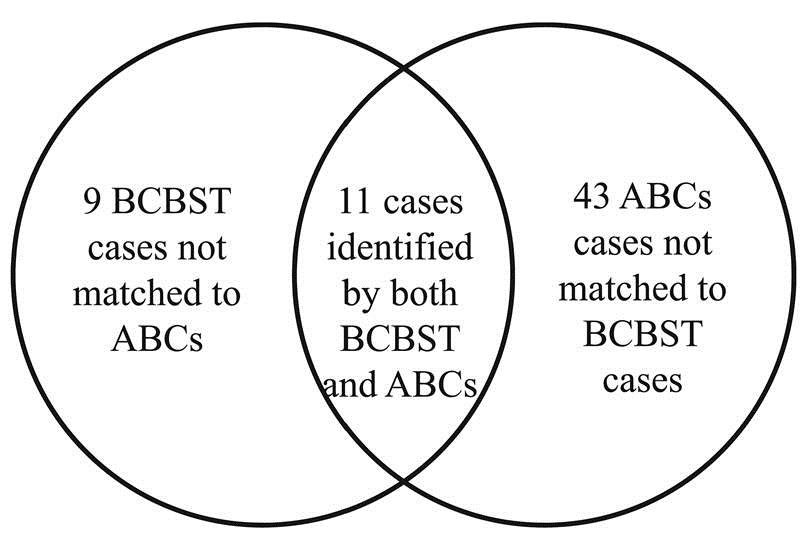
Overlap of BlueCross BlueShield of Tennessee (BCBST) and Tennessee Emerging Infections Program Active Bacterial Core surveillance (ABCs) necrotizing fasciitis cases, Tennessee, 2003–2012
The mean annual incidence of iGAS NF in the Tennessee ABCs data was 0.17 per 100,000 population (ranging by year from 0.03 to 0.31 per 100,000 population) compared with 0.06 per 100,000 population in the BCBST data (ranging by year from 0.00 to 0.19 per 100,000 population) (Figure 3).
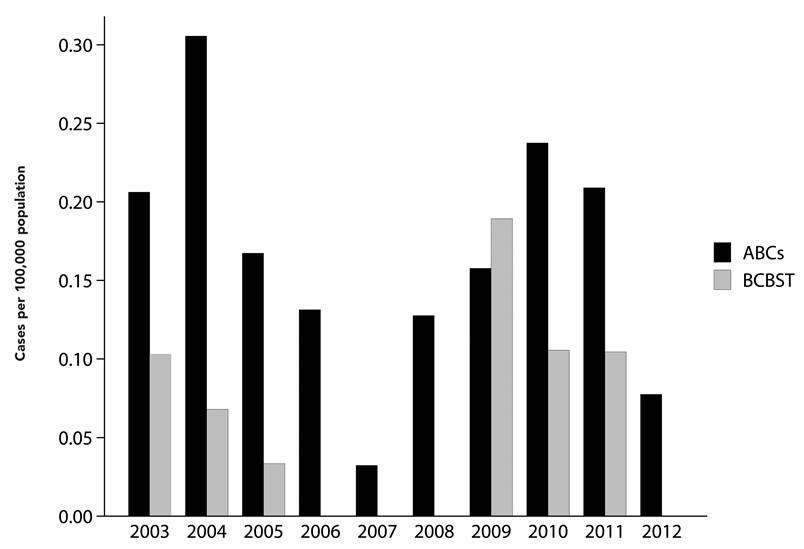
Annual incidence rate of Active Bacterial Core surveillance (ABCs) and BlueCross BlueShield of Tennessee (BCBST) necrotizing fasciitis cases per 100,000 population, Tennessee, 2003–2012a
A total of 12 unique patients in the BCBST had an ICD-9 diagnosis of both NF (728.86) and GAS (041.01), of whom nine had inpatient hospital claims. Of these nine patients, we could not locate records for one patient. We performed medical record review for the remaining eight patients: seven were verified to have both GAS and NF and one had neither GAS nor NF. Of these seven patients, five matched to the ABCs database and two did not (sensitivity: 9.3%, 5/54; PPV: 71%, 5/7).
Discussion
Only 20 (6%) of more than 350 patients in the managed care organization’s claims database with an ICD-9 diagnosis of NF were hospitalized with GAS cultured as the etiologic agent. Of the 20 iGAS NF patients identified through BCBST data, 11 had been previously detected by ABCs. Through this intensified effort to ascertain true cases of iGAS NF, we found only nine new cases during a 10-year period. The ICD-9 diagnosis code of NF in the claims database was neither sensitive nor predictive of iGAS NF. We found very few patients in BCBST data with an ICD-9 diagnosis of both NF (728.86) and GAS (041.01), and almost all had been previously found by ABCs, giving a lower sensitivity for the claims search. Using administrative claims data, we found no new cases with positive blood cultures, which is the principal means of identifying iGAS NF cases in the ABCs system. Expanding active surveillance in ABCs counties to include wound and tissue culture may have captured these new cases, but such an extension would far exceed the ability, funding, and resources of the current ABCs project.
During our medical record review, most patients with NF did not have GAS as an invasive pathogen; this finding is consistent with the literature indicating that GAS is one of several pathogens responsible for NF. 1 Including the ICD-9 code for GAS in addition to the ICD-9 code for NF did not help either sensitivity or PPV for BCBST GAS NF claims patients. Each medical record had to be reviewed thoroughly, including surgery, pathology, and radiology reports, to confirm the diagnosis of NF. Of the 20 patients identified through the administrative claims database search, two did not have supportive surgical or pathologic reports. Laboratory records had to be reviewed to document iGAS as the pathogen, because administrative claims data did not have laboratory test results. Additionally, using 10 diagnosis codes from each medical service may have contributed to a larger number of possible cases for review.
We first explored using a more sensitive, less precise claims algorithm (i.e., using NF diagnosis only) to see if we could enhance NF iGAS surveillance. Because claims information is collected strictly for billing and recordkeeping purposes, a substantial effort was needed to extract cases from claims data and format them for surveillance purposes. Substantial time, effort, and medical record review were needed to identify the true NF cases (i.e., those in ABCs and those that met the case definition but were not in ABCs), yet we found only a few true cases, which was likely a result of the low sensitivity of using the NF code alone. -Additionally, we found many cases reported in outpatient settings, which are likely false diagnoses because the severity of true NF would necessitate hospitalization. When we combined the ICD-9 codes for NF along with iGAS, the effort became more manageable because there were fewer cases to review; however, we found only two new cases not detected by routine ABCs during a 10-year period. When compared with state-reported data for some reportable conditions, combining health plan data with the state public health surveillance system could provide a comprehensive view of certain reportable conditions, such as infectious zoonotic disease clusters; however, in Tennessee, this approach is not a viable mechanism for other reportable conditions, such as iGAS NF, Salmonella, or Lyme disease. 5 –7,9 Given that the administrative claims data used in this study captured data on only about half of residents in the active surveillance areas, the true incidence of GAS NF is likely to be underestimated by much more than the 17% we reported.
Limitations
Limitations of this analysis included the use of administrative codes for NF, which identified many patients reported in outpatient settings, indicating an accuracy problem with the codes. Additionally, the coding algorithm may not have been specific enough to identify true matches. However, this matching algorithm has been used with other surveillance database comparisons with BCBST, and we were able to visually inspect for false positives.
Conclusion
Although we identified additional iGAS NF cases using administrative claims data, substantial resources were required to identify these few additional cases, which is not sustainable long-term and has minimal benefit for enhancing population-based surveillance in Tennessee.
Footnotes
Acknowledgements
The authors thank Ellyn Marder, Tennessee Department of Health, for her assistance with the matching algorithm; and Chris Van Beneden and Gayle Langley, Centers for Disease Control and Prevention, for their review of the article. The study protocol was approved by the Tennessee Department of Health, Vanderbilt, and BlueCross BlueShield of Tennessee institutional review boards.