
Abstract
Strong working relationships between infectious disease (ID) physicians and public health have resulted in the early detection of emerging infectious threats. From May 6 through June 5, 2015, we surveyed ID physicians in the Infectious Diseases Society of America’s Emerging Infections Network about communications with public health. A total of 688 of 1491 (46%) members completed the survey, 624 (91%) of whom knew how to reach their health department directly for an urgent issue. Only 38 (6%) described communications with their health department as poor. Interest in newer technologies (eg, mobile smartphone applications) showed mixed results. Interest in a smartphone application differed significantly by years of ID experience, with 81 of 146 (55%) respondents with <5 years of ID experience, 172 of 359 (48%) respondents with 5 to 24 years of ID experience, and 61 of 183 (33%) respondents with ≥25 years of ID experience in favor of a smartphone application (P < .001). As more physicians adopt newer communication technologies, health departments should be prepared to incorporate these tools to communicate with ID physicians.
Infectious disease (ID) physicians are often the first to see cases of emerging infections. 1,2 They need to know when to call and with whom to speak at the local or state health department when they see a clinical case with potential public health importance. Furthermore, public health practitioners need to be able to contact ID physicians to communicate concerns, ask questions, and provide information about emerging public health threats. We present findings from a survey about communication between public health and physicians from the Infectious Diseases Society of America’s (IDSA’s) Emerging Infections Network (EIN).
Methods
The IDSA EIN includes approximately 1500 practicing ID physicians from all 50 US states, the District of Columbia, Canada, and Puerto Rico (Canadian members were excluded from our survey). Membership is voluntary, and the network represents approximately 18% of IDSA physician members and 20% of US board-certified ID physicians. 3 Queries of the Emerging Infections Network are intended to gauge the current landscape of infectious disease practice and are designated as non-research as described in current Centers for Disease Control and Prevention (CDC) policy. As such, institutional review board review was not required.
We developed a 13-question survey with technical assistance from CDC, the Council of State and Territorial Epidemiologists, and the Association of State and Territorial Health Officials. Respondents could provide write-in comments. The EIN staff members sent the electronic survey to all EIN physicians for completion between May 6 and June 5, 2015. We obtained data on years of ID experience, geographic region, and employer from the EIN database. We determined population density using the 2014 population of the county of the member’s practice divided by the land area of that county. We used SAS® version 9.3 4 and Pearson’s χ2 test or Fisher’s exact test to compare categorical variables. We used Clopper-Pearson’s exact method to calculate 95% confidence intervals (CIs).
Study Sample
A total of 716 of 1491 (48%) physicians responded to the survey, generally reflecting the overall EIN membership except that respondents were more likely than nonrespondents to practice pediatric ID, have 15 to 24 years of experience since ID fellowship, or work in a university or medical school. Twenty-eight respondents replied that the survey was not applicable and that communication with public health departments was not relevant to their practices; they were excluded from subsequent analyses, leaving 688 respondents.
Results
Contacts Initiated by ID Physicians
Of 688 respondents, 624 (91%) said they knew how to reach their health department directly for an urgent issue, and 597 (87%) had contacted the state or local health department in the past 2 years. Of 594 respondents who indicated reasons for contacting the health department, 412 (69%) cited reporting a notifiable disease, 371 (63%) cited a possible infection of public health importance, 348 (59%) cited arranging for diagnostic testing, 193 (32%) cited concerns about sexually transmitted infections or human immunodeficiency virus contact tracing, 187 (32%) cited a possible outbreak (Table 1), and 151 (25%) cited other reasons. Findings did not differ by population density.
Issues for which infectious disease (ID) physicians had contacted their state or local health department in the past 2 years, by years of ID experience, survey of Emerging Infections Network physicians, United States, May-June 2015a
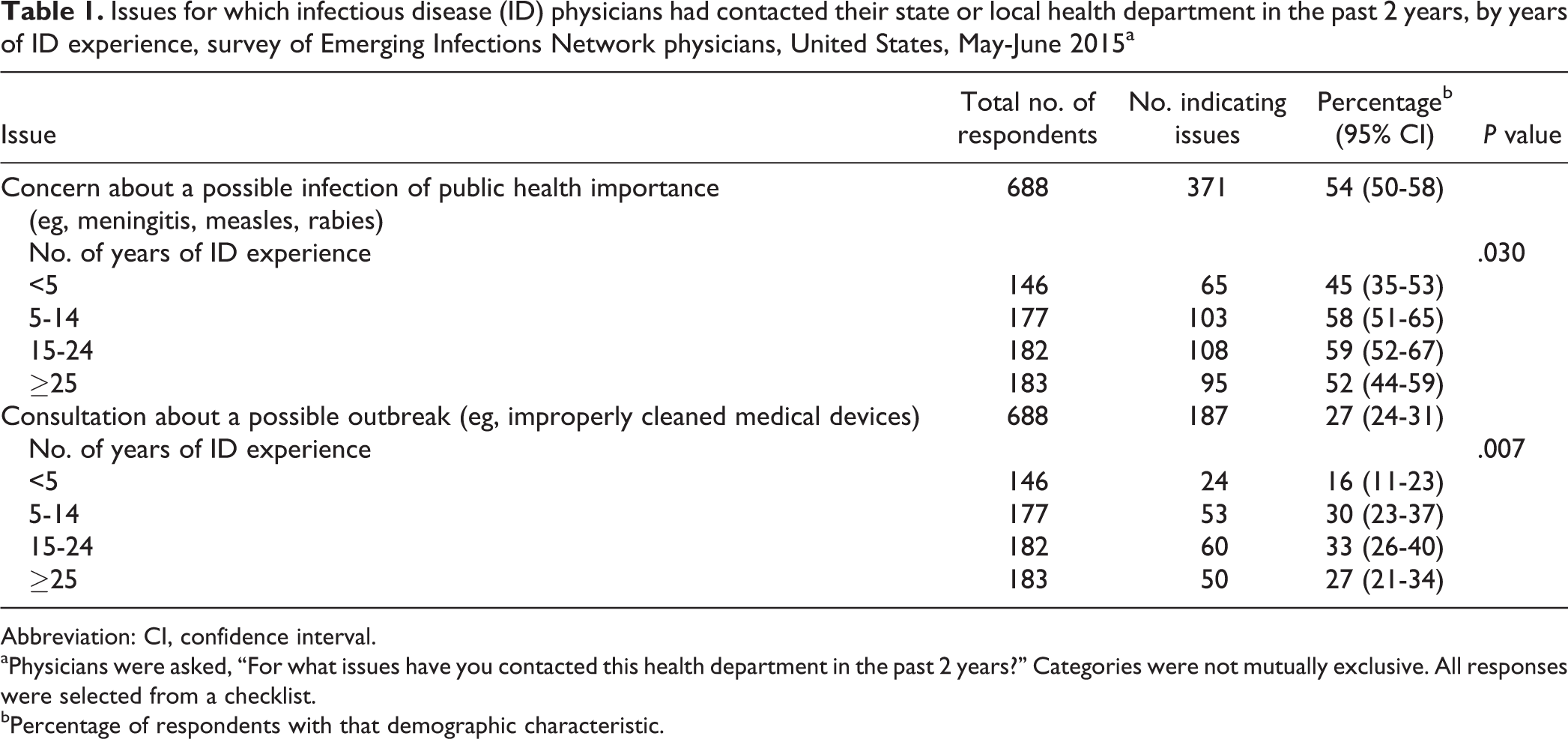
Abbreviation: CI, confidence interval. aPhysicians were asked, “For what issues have you contacted this health department in the past 2 years?” Categories were not mutually exclusive. All responses were selected from a checklist.
bPercentage of respondents with that demographic characteristic.
Contact Initiated by the State or Local Health Department
Of 688 respondents, 491 (71%) indicated being contacted by their health department in the past 2 years about an issue or case that the health department was investigating. Websites, email and fax health alerts, health information sent by postal mail, and presentations by public health staff members were generally available. Respondents reported health alerts sent by email, fax, or text to be particularly beneficial and health alerts sent by postal mail to be less beneficial (Table 2).
Infectious disease (ID) physician assessment of the usefulness of varying forms of communication from their state or local health department, by years of ID experience, survey of Emerging Infections Network physicians, United States, May-June 2015a
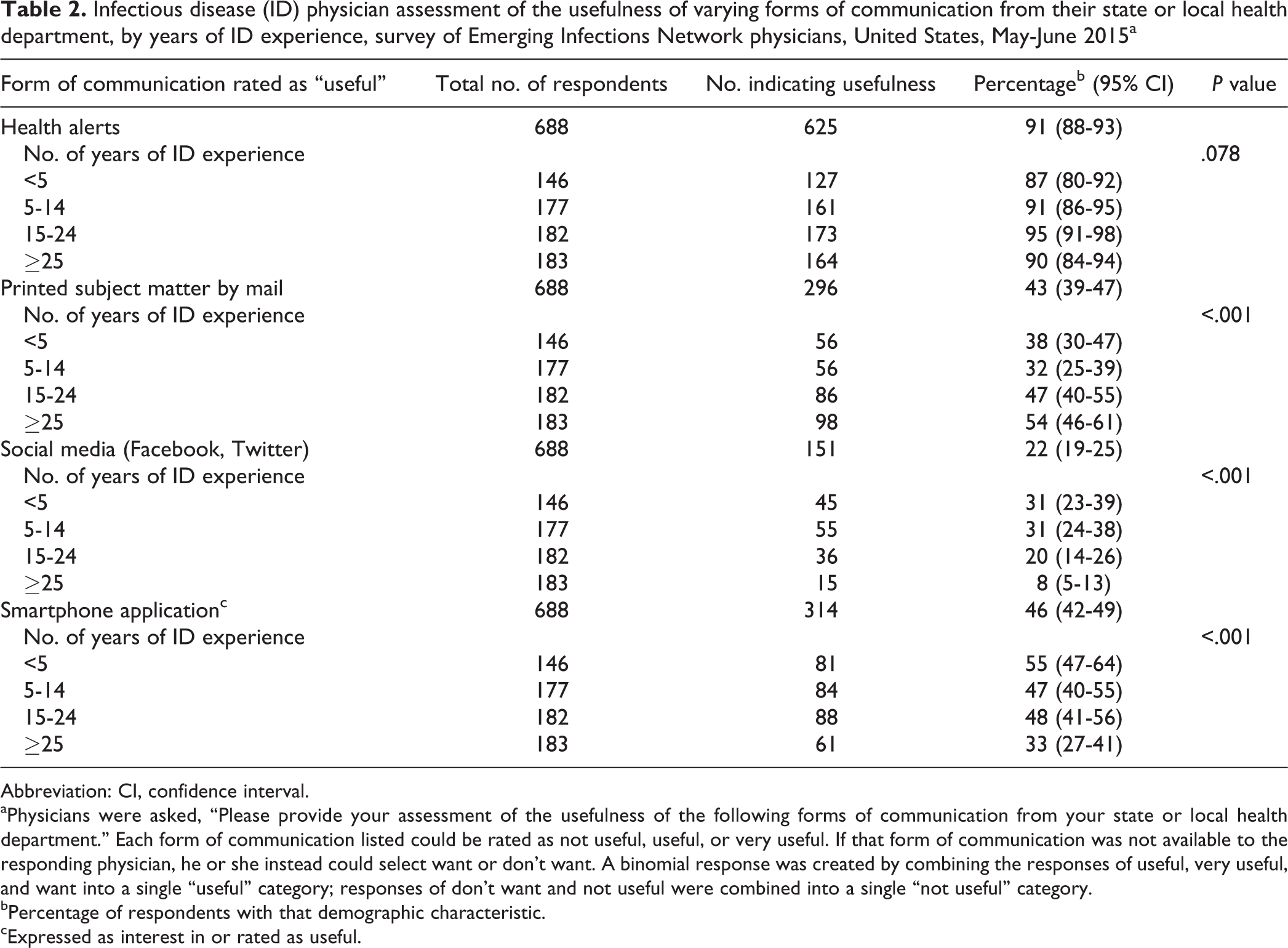
Abbreviation: CI, confidence interval. aPhysicians were asked, “Please provide your assessment of the usefulness of the following forms of communication from your state or local health department.” Each form of communication listed could be rated as not useful, useful, or very useful. If that form of communication was not available to the responding physician, he or she instead could select want or don’t want. A binomial response was created by combining the responses of useful, very useful, and want into a single “useful” category; responses of don’t want and not useful were combined into a single “not useful” category.
bPercentage of respondents with that demographic characteristic.
cExpressed as interest in or rated as useful.
Those interested in a smartphone application differed significantly from those with no interest in a smartphone application by years of ID experience. Eighty-one of 146 (55%) respondents with <5 years of experience, 172 of 359 (48%) respondents with 5 to 24 years of experience, and 61 of 183 (33%) respondents with ≥25 years of experience wanted a smartphone application (P < .001) (Table 2).
Regarding preferred sources for obtaining public health information, 675 (98%) respondents cited CDC, 633 (92%) respondents cited professional societies (eg, IDSA), 159 (23%) noted paid online medical resources (eg, ProMED mail), 149 (22%) cited publicly available websites (eg, WebMD, newspapers, blogs), and 34 (5%) cited social media (eg, Twitter) as preferred sources (Table 3). Respondents generally preferred CDC rather than state or local health departments as a source for information on emerging infections such as Ebola virus disease, Middle East Respiratory Syndrome Coronavirus, and Enterovirus D68. However, for more common infections (eg, measles and influenza), respondents considered both CDC and state or local health departments to be useful information sources.
Preferred sources for obtaining public health information, by years of infectious disease (ID) experience, survey of Emerging Infections Network physicians, United States, May-June 2015a
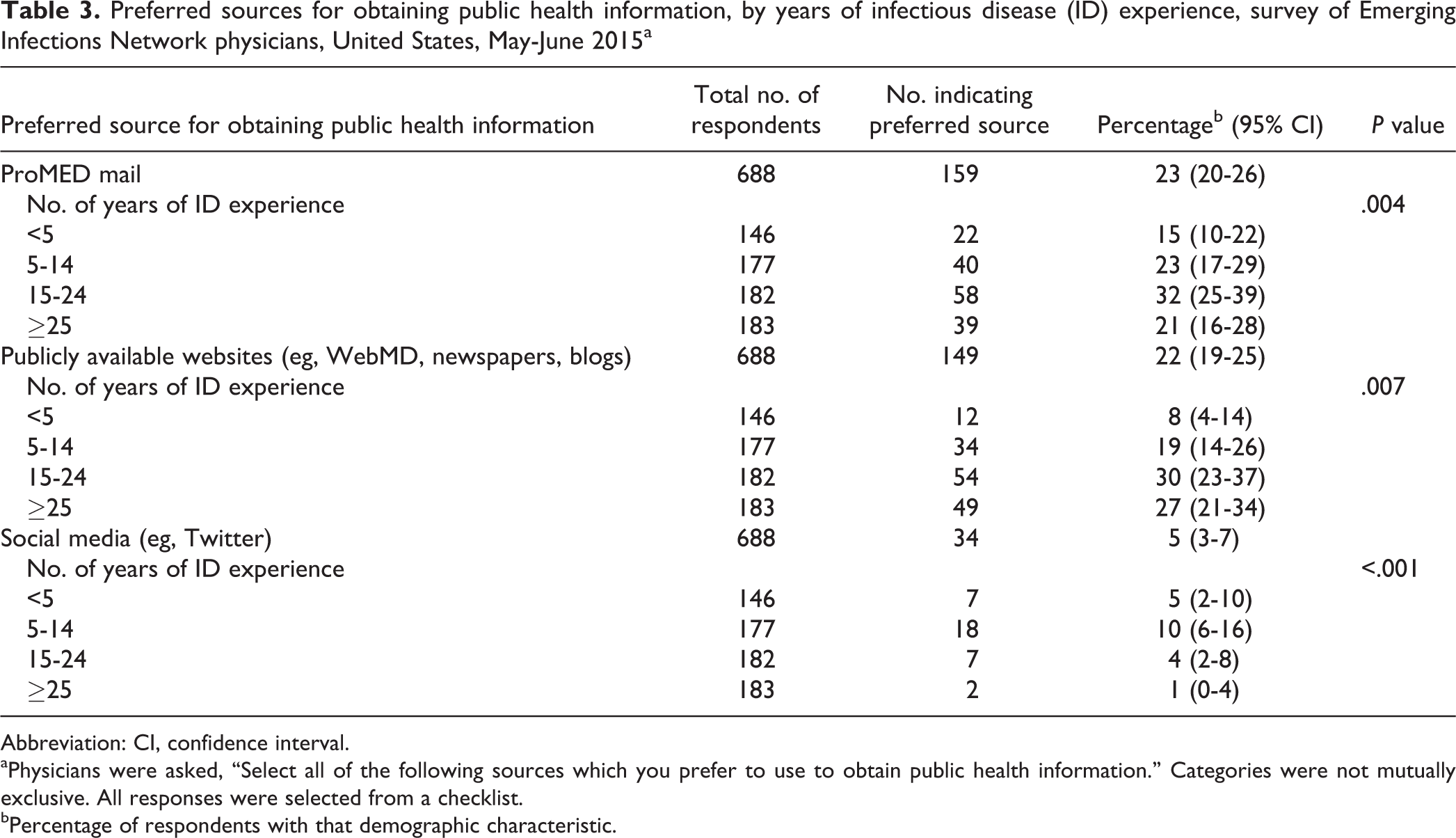
Abbreviation: CI, confidence interval. aPhysicians were asked, “Select all of the following sources which you prefer to use to obtain public health information.” Categories were not mutually exclusive. All responses were selected from a checklist.
bPercentage of respondents with that demographic characteristic.
A total of 323 (47%) respondents reported that they had modified their practice after communications with health departments. The most common reasons cited for changes in practice included Ebola, tuberculosis, measles, and sexually transmitted infections. Finally, 165 (24%) respondents described their communication with health departments as outstanding, 311 (45%) described it as good, 141 (21%) described it as adequate, and 38 (6%) described it as poor.
Responses to Open-ended Questions
Overall, 89 respondents said no barriers existed or indicated having a good relationship with their health department. A common challenge was knowing whom to contact at the health department and being able to connect with that person directly. Sixty-six respondents wanted telephone numbers or direct access to specific contacts. Multiple respondents indicated that an automated answering service was a disincentive to contacting the health department.
Twenty-nine respondents suggested ways to build relationships with health department staff members, including updates at division meetings or physicians’ offices, improved engagement with key local ID providers during outbreaks, joint ID/public health rounds using streaming media, joint journal clubs, and speaking at local ID society meetings to explain health department services and describe local epidemiology and disease surveillance.
Twelve respondents made suggestions about notifiable disease reporting. Several respondents requested easily found lists of reportable conditions on the health department website. A small number of respondents commented on newer technologies. Twenty respondents expressed a desire for email or text messaging; 19 respondents mentioned web-based communications, including a more user-friendly website and clear contact numbers or a physician-to-physician line listed on the website. Several respondents requested smartphone mobile applications. Other respondents indicated that the need to enter passwords for health alerts or notifications meant some physicians did not access those notifications.
Discussion
The ID physicians are a critically important constituency for health departments, as indicated by their knowledge of how to reach their health departments for an urgent issue and the high percentage who reported having contacted their health departments in the past 2 years. In a previous assessment by the New York City Department of Health and Mental Hygiene, 61% of respondents had contacted the health department in the past year. 5 Similarly, 76% of respondents to a survey by CDC and the American Academy of Pediatrics and 83% of respondents to a survey by CDC and the American Academy of Family Physicians knew a primary contact at the state health department, and 83% and 57% of respondents to the 2 surveys, respectively, had contacted that person in the previous 12 months. 6
The majority of ID physicians in our survey described communications with their health department as outstanding or good. Despite mostly positive interactions between ID physicans and public health, we identified opportunities for improvement. A common challenge was knowing whom to contact at the health department and being able to reach that person directly. Staffing limitations may prevent health department personnel from being available immediately, but all health departments typically have a staff member on call, although this person may not be a physician. It may be helpful for ID physicians to become familiar with the health department’s organizational structure to understand how the on-call individual reports to or relates to the usual health department contact. An emergency situation can sometimes serve as a catalyst for building trust between ID physicans and public health staff members who may not have an opportunity to interact with each other on a daily basis. For example, several respondents indicated that working together on Ebola preparedness resulted in improved contact with their health department overall. Receiving key information from a trusted source at the health department with whom the ID physician has worked closely in the past may be more important than receiving a large volume of material from health department personnel whom the physician does not know. 7
Numerous respondents commented on challenges in reporting notifiable diseases, including requests for lists of reportable conditions and the inability to report online. Many health departments already offer lists of reportable conditions and online reporting; thus, a simple solution to reporting challenges might be to inform ID physicians about such resources. In the future, notifiable disease surveillance could be improved by an informatics-driven approach. 8,9 Since 2010, CDC has provided annual resources via the Epidemiology and Laboratory Capacity for Infectious Diseases cooperative agreement to 57 state, local, and territorial health departments to improve electronic laboratory reporting. 8
Regarding recent changes in communications technology, responses were mixed. Those with less ID experience were more likely than those with more ID experience to want a smartphone application. Years of ID experience may be a surrogate for age. Many ID physicians described alerts via email, fax, or text to be useful. The CDC Health Alert Network (HAN) items disseminated via email are a relatively simple and rapid channel for information sharing. Most state-based HANs cover more than 90% of their population. 10 Another potential resource is IDSA’s Rapid Communications Task Force, which sends ID physicians succinct, urgent advisory emails with epidemiology updates, clinical aspects of diseases, diagnostics, case definitions, infection control, treatment, and exposure management information. 11
Limitations
This study had several limitations. First, the views of physicians in the EIN may not represent the views of all ID physicans. Thus, other ID physicians could have different experiences of communications with their health departments. Second, questions relied on physican recall, and physicians may have forgotten instances during which they interacted with public health. Third, it is possible that survey respondents have more familiarity or interaction with health departments than nonrespondents, resulting in overestimation of the strength of these communication channels. Fourth, we focused on ID physicans. However, patients with emerging infections might present to an urgent care or outpatient clinic rather than an ID physician. Future surveys could focus on primary care physicans, who might be the first to encounter emerging infections.
Conclusion
Strong working relationships between ID physicians and public health should be viewed as an asset in preparing for emerging infectious threats. Newer technologies such as social media and smartphone applications may not be the best way to communicate with middle-aged or older physicians. However, as more ID physicians adopt newer technologies, health departments should be prepared to make use of these tools.
Footnotes
Acknowledgments
The authors thank Robert Pinner, Satish Pillai, Susan Gantt, and Anne Wagstaff for their ongoing contributions to the Infectious Diseases Society of America’s Emerging Infections Network, assistance with literature reviews, survey input, and review of the article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This publication was supported by cooperative agreement #1U50CK000187 from the Centers for Disease Control and Prevention (CDC). Its contents are solely the responsibility of the authors and do not necessarily represent the official views of CDC.