
Abstract
This study examined the frequency of screening-positive symptom levels for depression, anxiety, attention deficit hyperactivity disorder (ADHD), and internet use, as well as factors independently associated with these outcomes among university students. We aimed to clarify interrelationships among these conditions and various sociodemographic variables, using a large sample of 4,556 students. Participants completed a web-based survey, including a sociodemographic questionnaire, the Adult ADHD Self-Report Screening Scale for DSM-5, Beck Anxiety and Depression Inventories, and Internet Addiction Test. Based on established cut-off scores, the proportions of participants screening positive were 39.8% for depression, 37.7% for anxiety, 35.5% for ADHD, and 9.1% for elevated internet use symptoms. Furthermore, 6.2% of participants reported a history of suicide attempts. In multivariable logistic regression models, screening positive for depression was independently associated with younger age, not living with family, lower family income, a history of psychiatric disorders or suicide attempts, as well as co-occurring elevated symptom levels above the established cut-offs for anxiety, ADHD, and elevated internet use. Screening positive for anxiety was independently associated with female sex, a family history of domestic migration, being in a romantic relationship, and a history of psychiatric disorder or suicide attempt, as well as co-occurring elevated symptom levels above the established cut-offs for depression, ADHD, and elevated internet use symptoms. Screening positive for elevated internet use symptoms was independently associated with male sex, a family history of international migration, suicide attempt history, and co-occurring elevated symptom levels above the established cut-offs for depression, anxiety, and ADHD. These findings indicate a high burden of elevated symptoms in university students and underscore the urgent need for accessible mental health support systems, targeted screening, and referral pathways within universities.
Introduction
The college years are a transition period in which individuals face academic and social pressures while gaining autonomy and undergoing essential mental development (Pedrelli et al., 2015). Recent studies have shown a nearly 50% increase in mental health problems among college students from 2013 to 2021 (Lipson et al., 2022). There has also been a significant rise in suicidal thoughts and behaviors, a particularly concerning mental health issue (Duffy et al., 2019). A World Health Organization study on first-year college students in eight countries found lifetime prevalence rates of anxiety, mood, or substance abuse disorders at 35.3% and 12-month prevalence rates at 31.4%. These rates vary by region; for instance, Belgium reported a lifetime prevalence of 22.4%, while Australia reported 48.3% (Auerbach et al., 2018). In Türkiye, where our study was conducted, research often focuses on individual mental health disorders rather than comprehensive studies examining multiple disorders, their comorbidity, and common risk factors. Previous studies in Türkiye reported the prevalence of depression at 26.2% (Bostanci et al., 2005), generalized anxiety disorder at 25.2% (Cengiz & Topuzoğlu, 2022), attention deficit and hyperactivity disorder (ADHD) at 15.5% (Kılıçoğlu et al., 2009), and pathological internet use at 11.4% (Aslan et al., 2021).
Mental health issues during college can negatively impact problems with academic performance, leading to decreased success and increased dropout rates (Eisenberg et al., 2009). They also affect satisfaction with university life (Liu & Wang, 2024), can cause sleep problems (Dinis & Bragança, 2018), and heighten suicidal behaviors (Garcia-Williams et al., 2014). These problems extend beyond the individual, affecting their social environment and having broader societal impacts.
Various factors were linked to mental health problems in college students, including low income (Said et al., 2013), social support, health problems (Lei et al., 2021), and living alone (Tran et al., 2017). Research on risk factors in middle-income countries such as Türkiye seems to be limited. In Türkiye, issues with friends (Bostanci et al., 2005) and immigration (Cengiz & Topuzoğlu, 2022) were associated with depressive symptoms, while anxiety was linked with difficulties understanding lessons, chronic disease (Ozen et al., 2009), being female, and living in dormitories (Cengiz & Topuzoğlu, 2022). Understanding the risk factors for mental health disorders is vital to prevent them and provide appropriate support. Schools play an essential role in students’ lives, and offering support can enhance well-being and protect against mental health problems (Romeo et al., 2024).
This study examined the elevated symptom levels of anxiety, depression, ADHD, internet use and their sociodemographic and clinical correlates in a large university sample. The results aimed to improve understanding of these disorders in middle-income countries like Türkiye and identify areas requiring intervention. By addressing these disorders together, this study offers a holistic view of common mental health disorders among college students, providing critical data for developing effective interventions.
Methods
Participants and Procedure
This research was conducted at Pamukkale University, a large institution located in Denizli, southwest of Türkiye. The university comprises 48 schools, including institutes, faculties, and vocational schools, and had 47,806 students enrolled during the 2023-2024 academic year. The research was planned as a project of the Pamukkale University Student Support Unit (SSU), which offers support to students in various aspects of their university life, including academic, social, psychological, economic, and career-related matters.
The research aimed to identify psychological issues that could impair the academic and social functionality of students. Before starting the research, permission was obtained from the Pamukkale University Non-Interventional Clinical Research Ethics Committee on 05.03.2024, with the approval number E-60116787-020-508607. Following the approval, a face-to-face meeting was held with SSU members in each school to introduce the research. Online survey forms were distributed to students via SSU members. Information about the research was provided in the survey forms, and only students who agreed to participate and provided consent were able to see the questionnaire.
Given the sensitive nature of the survey items, particularly those related to suicide attempts, we implemented specific ethical safeguards. The survey included a clear statement that participation was voluntary and that respondents could withdraw at any time. Because the study was conducted through the Student Support Unit, which provides psychological support to students, the participants were informed that support was available if they felt they needed it. To protect privacy and encourage candid responses, data were collected anonymously.
The research utilized various assessment tools, including a sociodemographic data form, the Adult ADHD Self-Report Screening Scale for DSM-5, the Beck Anxiety Inventory, the Beck Depression Inventory, and the Internet Addiction Test. The data collection took place between 15.04.2024 and 05.06.2024. The goal was to distribute the survey to all students. Therefore, the research universe consisted of 47,806 students; out of these, 5,781 responded, 5,512 of these students consented to participate, and 4,556 completed all forms.
Measures
Sociodemographic data questionnaire
This form collected information on housing type (living at home vs. living in a dormitory), household composition (living with family, living with friends, or living alone), family income (below vs. above the minimum wage), parents’ marital status (separated vs. together), family migration history (yes/no), relationship status (partner: yes/no), disability (yes/no), presence of any psychiatric disorders (yes/no), and history of suicide attempts (yes/no). All items were single-response and coded as mutually exclusive categories (i.e., no multiple-response items).
Adult ADHD Self-Report Screening Scale for DSM-5 (ASRS-5)
Developed by the World Health Organization, this is a 5-point Likert-type scale with 6 questions designed for adult ADHD self-report screening based on DSM-5 criteria. The scale’s validity was established by Üstün et al. (Ustun et al., 2017), and the Turkish version was validated by Aslan-Genç et al. A score of 10 or above indicates screening positivity/elevated ADHD symptom levels (Aslan Genç et al., 2021).
Beck Anxiety Inventory (BAI)
Created by Beck et al., this scale measures anxiety severity. It consists of 21 items rated on a 4-point Likert scale ranging from 0 (not at all) to 3 (severe), with a total score ranging from 0 to 63 (Beck et al., 1988). Higher scores indicate greater anxiety levels, categorized as mild (8-15), moderate (16-25), and severe (26-63). The Turkish version was validated by Ulusoy et al. (Ulusoy et al., 1998).
Beck Depression Inventory (BDI)
This scale assesses emotional, vegetative, cognitive, and motivational symptoms of depression through 21 questions, each scored between 0 and 3, with scores ranging from 0 to 63 (Beck et al., 1961). The severity levels are minimal (0-9), mild (10-16), moderate (17–29), and severe (30–63). The Turkish version was validated by Hisli (Hisli, 1989).
Internet Addiction Test (IAT)
Developed by Young (Young, 1998), this test includes 20 questions rated on a 5-point Likert scale. Scores of 50-79 indicate moderate internet addiction, and scores of 80-100 indicate severe internet addiction (Kaya et al., 2015). The Turkish validation was confirmed by multiple studies (Balta & Horzum, 2008; Bayraktar, 2001).
In the present study, Cronbach’s alpha was 0.92 for BDI, 0.94 for BAI, 0.79 for ASRS-5, and 0.93 for IAT.
It is important to note that the self-report instruments used in this study (ASRS-5, BAI, BDI, and IAT) are designed for screening purposes. While scores above the established cut-offs indicate elevated symptom levels or a high risk for the respective conditions, they do not constitute a formal clinical diagnosis. Therefore, terms such as “depression,” “anxiety,” “ADHD,” or “elevated internet use symptoms” used throughout the results refer to individuals screening positive for these symptom domains rather than those with a confirmed clinical diagnosis.
Data Analysis
Data were analyzed using SPSS 25.0 (IBM SPSS Statistics 25 software (Armonk, NY: IBM Corp.)). Continuous variables were presented as mean ± standard deviation, while categorical variables were shown as numbers and percentages. The Chi-square test was used to compare categorical variables, and the Kolmogorov-Smirnov test assessed the normality of continuous variables. Given that parametric test assumptions were met, Student’s t-test or One-way ANOVA was used for comparing continuous variables. Pearson correlation coefficients evaluated relationships among the total scores of the BDI, BAI, ASRS-5, and IAT.
Participants were categorized into screen-positive and screen-negative groups based on established cut-off scores: Depression (BDI ≥17), Anxiety (BAI ≥16), ADHD (ASRS-5 ≥ 10), and elevated internet use symptoms (IAT ≥50). Binary logistic regression analyses were conducted using theory-driven forced-entry models. Two sets of models were estimated for each outcome. Primary models (Model (1) included sociodemographic and clinical history variables, while extended models (Model (2) additionally included other symptom groups to account for comorbid psychopathology. Regression results are presented as regression coefficients (B), standard errors, and Wald statistics. Model performance was evaluated using Nagelkerke R2, omnibus likelihood ratio tests, and discrimination indices (ROC/AUC). Model calibration was assessed using the Brier score calculated from predicted probabilities. Hosmer–Lemeshow goodness-of-fit test results are reported for completeness but were interpreted cautiously and not emphasized, as this statistic is known to be overly sensitive in large samples. For regression analyses, household composition was dichotomized to reflect living with family versus not living with family (including living with friends and living alone) to improve model parsimony and interpretability.
Results
The sociodemographic characteristics of 4556 participants were examined, revealing the following findings. 71.1% of the participants were female. The mean age was 21.47 years (SD = 4.32; Median = 21.0; range = 18–68). Regarding housing type, 42.4% of the participants reported living at home, while 57.6% reported living in dormitories. In terms of household composition, 32.6% reported living with family, 45.1% living with friends, and 22.3% living alone. In terms of family background, 12.1% had separated parents, 31.3% had a family income below the minimum wage, 4.1% had a family history of international migration, and 21.7% had a family history of domestic migration. Personal characteristics showed that 26.6% had a partner, 1.1% had a disability, 8.0% had a history of psychiatric illness, and 6.2% had a history of suicide attempt.
The Correlations Between Beck Depression Inventory (BDI), Beck Anxiety Inventory (Bai), Adult ADHD Self-Report Screening Scale (ASRS-5), and Internet Addiction Test (IAT) Scores
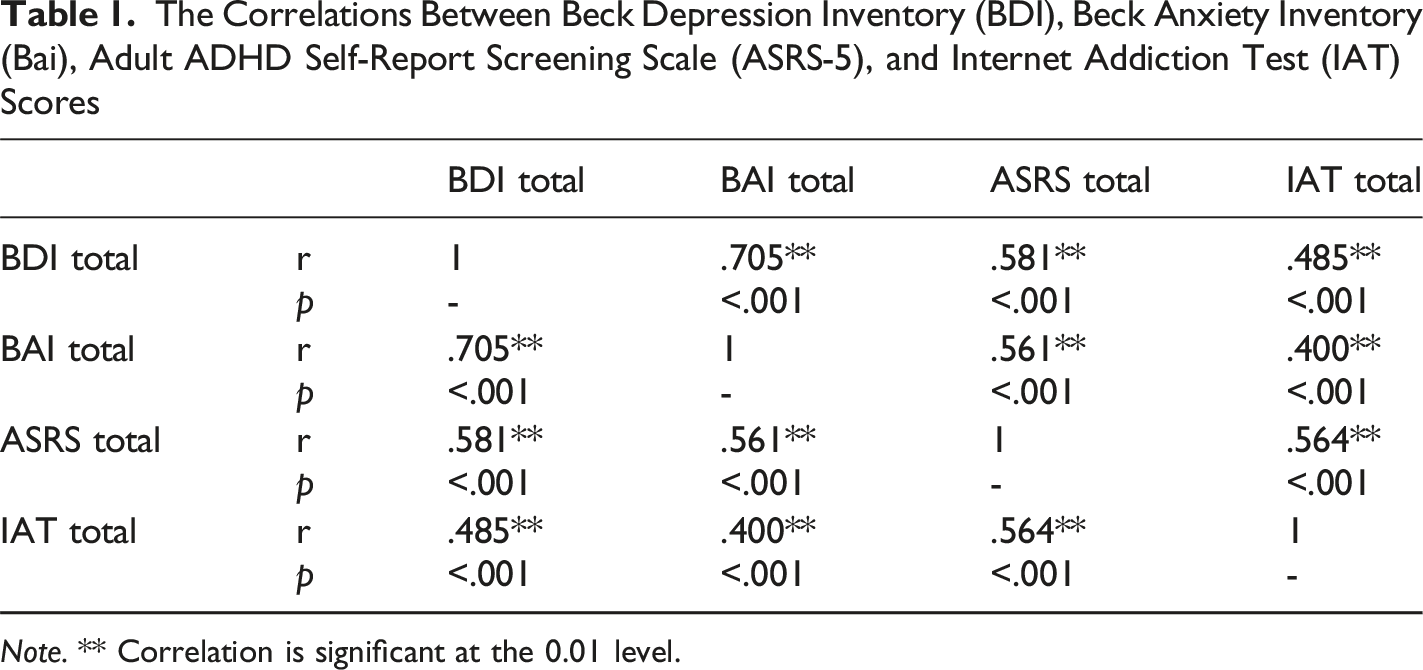
Note. ** Correlation is significant at the 0.01 level.
Sociodemographic Variables Comparisons
Comparisons of BDI, Bai, ASRS-5, and IAT Scores by Sociodemographic and Clinical Variables
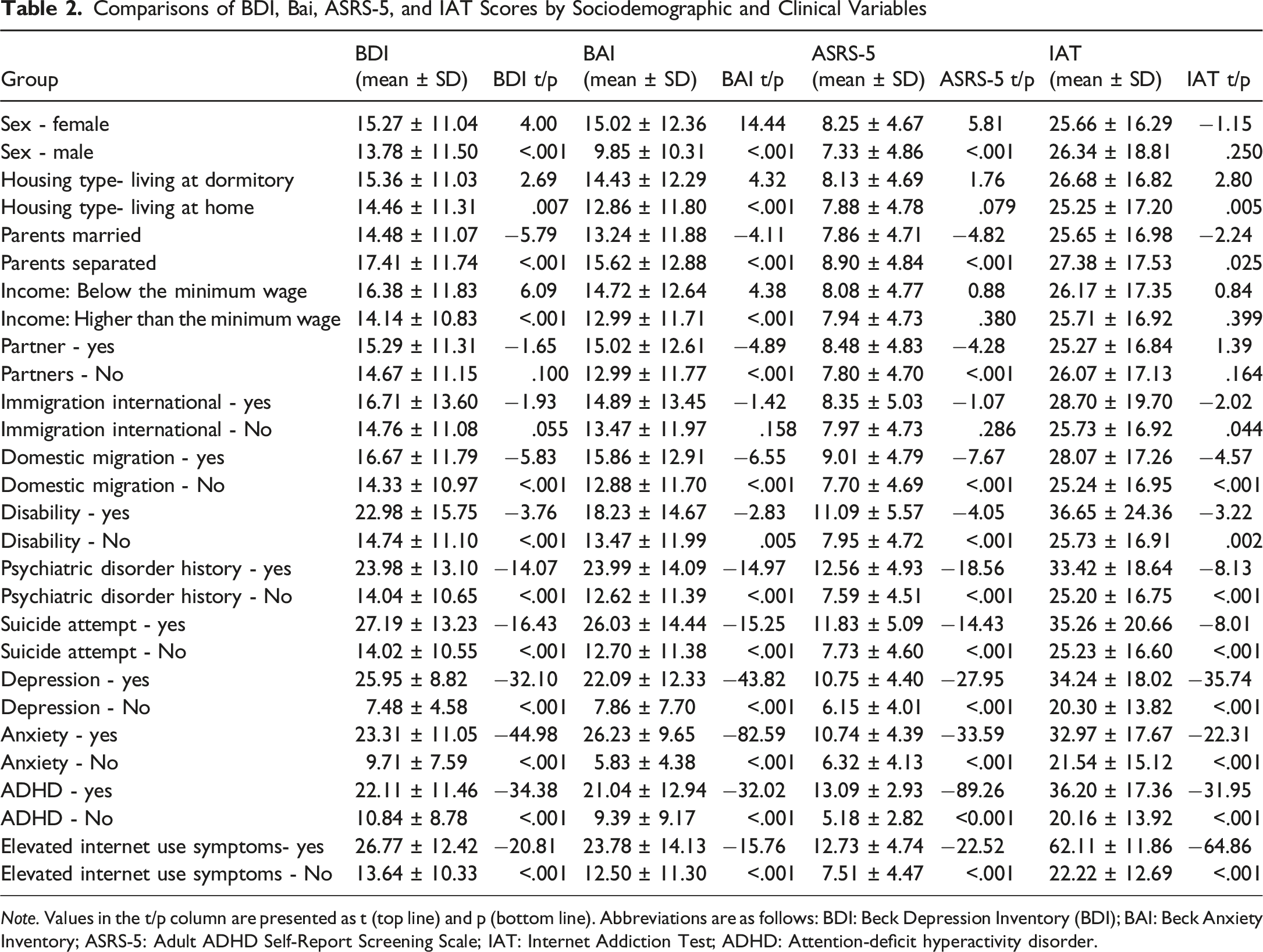
Note. Values in the t/p column are presented as t (top line) and p (bottom line). Abbreviations are as follows: BDI: Beck Depression Inventory (BDI); BAI: Beck Anxiety Inventory; ASRS-5: Adult ADHD Self-Report Screening Scale; IAT: Internet Addiction Test; ADHD: Attention-deficit hyperactivity disorder.
Sex: While IAT scores were similar across genders, females had higher BDI, BAI, and ASRS-5 scores. Also, females had a higher frequency of psychiatric disorder history (Chi-square: 5.284, p = .022), but history of suicide attempt did not differ significantly between sexes.
Living arrangements: Participants living in dormitories had higher BDI, BAI, and IAT scores compared to participants who were living at home. However, participants who were living at home had a higher history of psychiatric disorders than dormitory residents (Chi-square: 6.759, p = .009). Post hoc comparisons using the Tukey HSD test indicated that participants living with family had significantly lower BDI (vs. friends: p < .001; vs. alone: p < .001), BAI (vs. friends: p < .001; vs. alone: p = .020), ASRS-5 (vs. friends: p = .004; vs. alone: p < .001), and IAT (vs. friends: p < .001; vs. alone: p = .005) scores compared to those living with friends or living alone.
Family background: Participants with separated parents had higher BDI, BAI, ASRS-5, and IAT scores. They also had higher rates of suicide attempts (Chi-square: 44.447, p < .001) and psychiatric disorder history (Chi-square: 30.154, p < .001). Participants with income levels below the minimum wage had higher BDI and BAI scores. Participants with a domestic migration history had higher BDI, BAI, ASRS-5, and IAT scores, as well as higher rates of psychiatric disorders (Chi-square: 8.423, p = .004) and suicide attempt history (Chi-square: 8.214, p = .004). Participants with an international migration history had higher IAT scores.
Personal characteristics: Participants with partners had higher BAI and ASRS-5 scores, along with more frequent psychiatric disorders (Chi-square: 24.562, p < .001) and suicide attempt history (Chi-square: 17.749, p < .001). Participants with disabilities had higher BDI, BAI, ASRS-5, and IAT scores, as well as more frequent psychiatric disorders (Chi-square: 43.664, p < .001) and suicide attempt history (Chi-square: 25.531, p < .001). Participants with a history of psychiatric disorder or suicide attempt had higher BDI, BAI, ASRS, and IAT scores. A history of psychiatric disorder is more frequent in participants with suicide attempt history (Chi-square: 259.764, p < .001).
Logistic Regression Analysis
Logistic Regression Analysis Results: Independently Associated Variables for Screening Positive for Depression
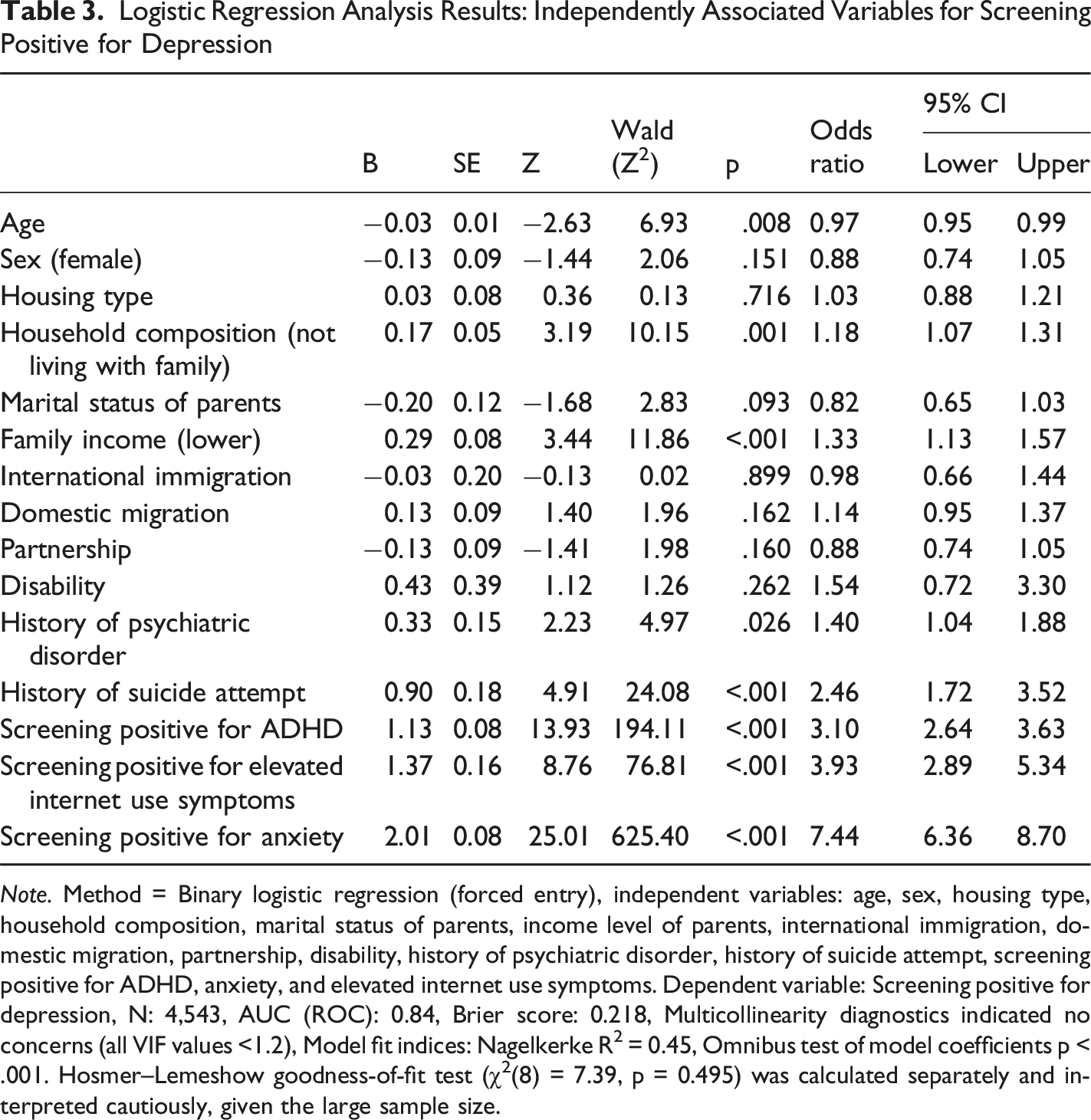
Note. Method = Binary logistic regression (forced entry), independent variables: age, sex, housing type, household composition, marital status of parents, income level of parents, international immigration, domestic migration, partnership, disability, history of psychiatric disorder, history of suicide attempt, screening positive for ADHD, anxiety, and elevated internet use symptoms. Dependent variable: Screening positive for depression, N: 4,543, AUC (ROC): 0.84, Brier score: 0.218, Multicollinearity diagnostics indicated no concerns (all VIF values <1.2), Model fit indices: Nagelkerke R2 = 0.45, Omnibus test of model coefficients p < .001. Hosmer–Lemeshow goodness-of-fit test (χ2(8) = 7.39, p = 0.495) was calculated separately and interpreted cautiously, given the large sample size.
Logistic Regression Analysis Results: Independently Associated Variables for Screening Positive for Anxiety
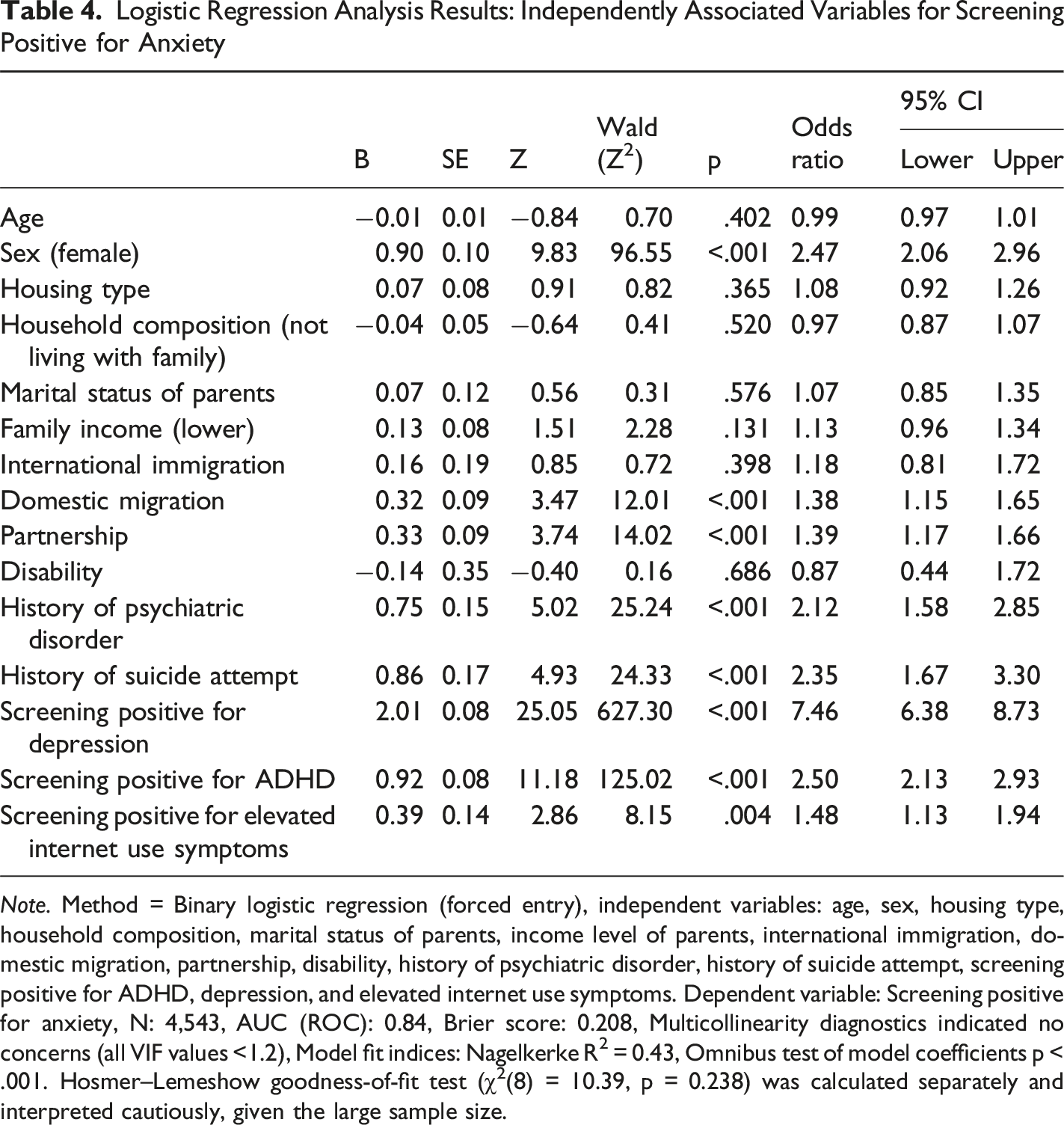
Note. Method = Binary logistic regression (forced entry), independent variables: age, sex, housing type, household composition, marital status of parents, income level of parents, international immigration, domestic migration, partnership, disability, history of psychiatric disorder, history of suicide attempt, screening positive for ADHD, depression, and elevated internet use symptoms. Dependent variable: Screening positive for anxiety, N: 4,543, AUC (ROC): 0.84, Brier score: 0.208, Multicollinearity diagnostics indicated no concerns (all VIF values <1.2), Model fit indices: Nagelkerke R2 = 0.43, Omnibus test of model coefficients p < .001. Hosmer–Lemeshow goodness-of-fit test (χ2(8) = 10.39, p = 0.238) was calculated separately and interpreted cautiously, given the large sample size.
Logistic Regression Analysis Results: Independently Associated Variables for Screening Positive for Elevated Internet Use Symptoms
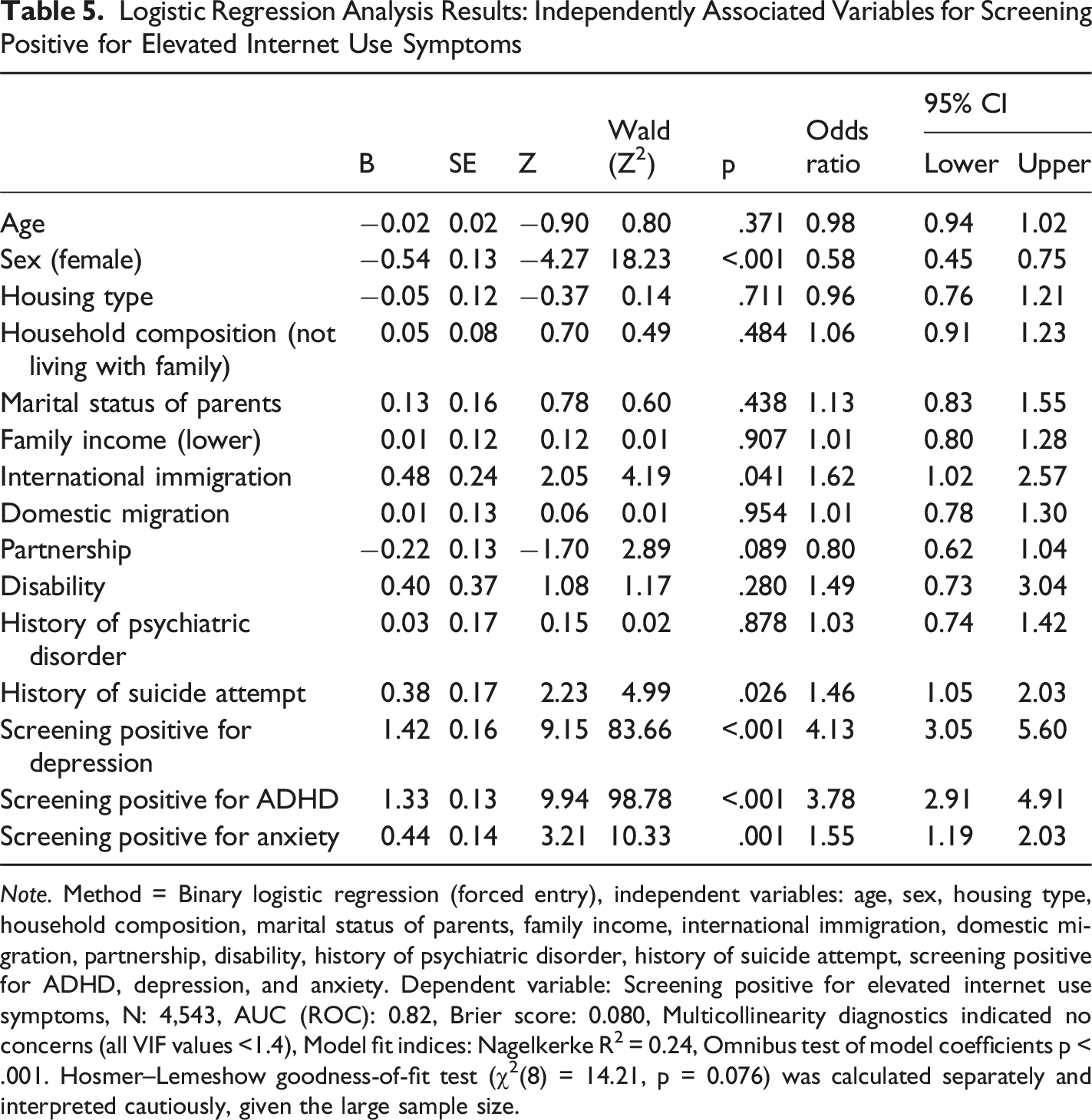
Note. Method = Binary logistic regression (forced entry), independent variables: age, sex, housing type, household composition, marital status of parents, family income, international immigration, domestic migration, partnership, disability, history of psychiatric disorder, history of suicide attempt, screening positive for ADHD, depression, and anxiety. Dependent variable: Screening positive for elevated internet use symptoms, N: 4,543, AUC (ROC): 0.82, Brier score: 0.080, Multicollinearity diagnostics indicated no concerns (all VIF values <1.4), Model fit indices: Nagelkerke R2 = 0.24, Omnibus test of model coefficients p < .001. Hosmer–Lemeshow goodness-of-fit test (χ2(8) = 14.21, p = 0.076) was calculated separately and interpreted cautiously, given the large sample size.
Discussion
This study examined the frequency of screening positive symptom levels for depression, anxiety, ADHD, and elevated internet use, as well as factors independently associated with these outcomes among university students. Our findings indicate a substantial burden of screening positive symptom levels across these domains, with observed associations involving sociodemographic characteristics and co-occurring symptom burden. Specifically, the proportions of participants screening positive were 39.8% for depression, 37.7% for anxiety, 35.5% for ADHD, and 9.1% for elevated internet use symptoms. These rates are broadly consistent with global and local prevalence estimates. However, the proportion screening positive for ADHD in our sample was higher than in many international studies, which may reflect regional contextual factors or methodological differences related to the screening instruments and cut-off thresholds used.
For depressive symptoms, 39.8% of students scored above the established cut-off. A recent global review and meta-analysis identified a 33.6% prevalence of depressive symptoms in university students (Li et al., 2022), indicating that our findings are slightly above this global average. Within Türkiye, previous studies reported a prevalence of 26.2% in 2000 (Bostanci et al., 2005) and 38.3% in 2013 (Ulaş et al., 2015) among university students. This suggests a potential increase in depressive symptoms over time.
In our study, 37.7% of students scored above the established cut-off for anxiety, which is broadly consistent with the approximately 39% global prevalence reported by Li et al. (Li et al., 2022). In Türkiye, a 36.7% prevalence of trait anxiety has been observed among university students (Ozen et al., 2009). This similarity suggests that anxiety is a prevalent issue for university students both locally and globally, warranting attention and intervention.
Our results indicated that 35.5% of the students screened positive for ADHD symptoms. This is significantly higher than international screening rates, with studies from the United States and Korea reporting positive screening rates for ADHD of 12.3% (Garnier-Dykstra et al., 2010) and 7.6% (Kwak et al., 2015) among college students. This discrepancy may reflect higher reported ADHD symptom levels in Türkiye or methodological differences related to screening tools and cut-off thresholds. Within Türkiye, the rate of ADHD without functional impairment was reported at 21.8% among primary school students (Ercan et al., 2015), substantially higher than the global rate of 7.6% for the same age group (Salari et al., 2023).
Our study found that 9.1% of the students exhibited elevated internet use symptoms above the cut-off point. A meta-analysis in China reported an 11% prevalence of internet addiction among college students (Shao et al., 2018), while another study in Asia documented a 24.3% prevalence (Duc et al., 2024). Previous Turkish research found an 8.6% prevalence among university students (Alaçam, 2012). Our findings align with the local rates but fall below the higher rates observed in other Asian regions, illustrating the potential impact of regional, social, and cultural differences on internet use behaviors.
We found that 6.2% of the students reported a history of suicide attempts. A review and meta-analysis study reported a 5.2% lifetime prevalence among students in Southeast Asia (Arafat et al., 2024). In Türkiye, previous data indicated a 7.1% prevalence among college students, with higher rates in rural areas (7.8%) compared to metropolitan areas (2.3%) (Toprak et al., 2011). Our finding is slightly higher compared to the global rates but lower than previous Turkish findings. This discrepancy might be due to the location of our study. The study’s location is a large city but not considered metropolitan.
In multivariable analyses, several sociodemographic and clinical variables were independently associated with screening positive for depression. Younger age was associated with higher odds of depressive symptoms above the established cut-off, consistent with U.S. data indicating that depression prevalence is highest among individuals aged 18–24 years and declines with increasing age (Lee et al., 2023). This trend was also seen in Korea, where individuals in their twenties exhibited the highest rate of depressive symptoms (Cho et al., 1998). Our study participants, mostly aged between 18 and 24, may face significant academic, career, and social pressures, contributing to these findings. Not living with family emerged as another associated variable. Prior research indicated that university students living alone had higher depression (Jang et al., 2021). Family support could be a protective factor against depression in university students. Additionally, a low family income level was identified as an associated variable, with studies from China (L. Chen et al., 2013) and Türkiye (Bostanci et al., 2005) finding a link between low socioeconomic status and depressive symptoms. This economic strain could negatively impact students’ social and academic lives, predisposing them to depression. A history of psychiatric disorders was also associated with depression. A review highlighted that existing mental health disorder was a risk factor for depression (Sheldon et al., 2021). Having a mental health problem might create a vulnerability to depression. Furthermore, a history of suicide attempts was associated with screening positive for depression, aligning with the finding that past suicidal ideation or suicide attempts in college students was a significant risk factor for depression. (Ebert et al., 2019). For these reasons, depression should not be overlooked in students with a history of suicide attempts. ADHD symptoms were also associated with screening positive for depression. ADHD symptoms were found to be a stressor for depressive symptoms in university students (Sahmurova et al., 2022). ADHD symptoms might impact academic and social areas, facilitating depression in university students. Elevated internet use symptoms were another associated variable, as they may be associated with loneliness and decreased social interactions; however, directionality cannot be inferred. Finally, anxiety was associated with screening positive for depression, supporting the bidirectional relationship between these two conditions (Jacobson & Newman, 2017).
We found female sex as an associated variable with screening positive for anxiety. Gao et al. found that anxiety was more common in women than in men among Chinese university students (Gao et al., 2020). Further studies would be beneficial to understand the causes of anxiety in women, specific to university times. The history of domestic migration was linked to anxiety, possibly due to stress and loss associated with migration (Essayagh et al., 2023). Having a partner was also associated with anxiety, with the possible dual impact of support and stress from the relationship. A history of psychiatric illness and past suicide attempts were also linked to anxiety, consistent with a USA college student study showing past mental illness as a predictor of anxiety symptoms (Bloomfield et al., 2024) and a study on Chinese college students showing suicidal thoughts as a predictor of possible anxiety (Ge et al., 2020). ADHD was again identified as an associated variable for anxiety. O’Rourke et al. found that college students with ADHD are more likely to have anxiety disorders and have lifelong anxiety symptoms (O’Rourke et al., 2017). A study on Chinese medical school students identified attention deficit and hyperactivity as an anxiety-associated factor (Shen et al., 2020). One possible interpretation is that higher ADHD symptom burden may be linked to elevated anxiety symptoms through academic, social, and functional stressors; however, this interpretation is hypothesis-generating and cannot be tested in the present cross-sectional design. Elevated internet use symptoms were similarly associated with anxiety, corroborating the findings from the meta-analysis (Li et al., 2022).
Male sex was one of the associated variables with screening positive for elevated internet use symptoms. Although literature shows mixed results regarding sex and elevated internet use symptoms (Balcı & Gülnar, 2013; Shan et al., 2021; Swain et al., 2024), this highlights the need for sex-specific investigations, especially regarding gaming disorder and social media addiction. An international migration history was also associated with elevated internet use symptoms, likely due to acculturative stress associated with adapting to new societies (J. Li & Liu, 2021). A history of suicide attempts was associated with elevated internet use symptoms, supported by a meta-analysis showing a link between internet addiction and suicidality (Cheng et al., 2018). This relationship might stem from high psychiatric comorbidity in both conditions and their associations with impulsive/aggressive behaviors (Peng et al., 2021). ADHD symptoms were also associated with elevated internet use symptoms, aligning with a meta-analysis that showed a connection between ADHD symptoms and problematic internet use (Augner et al., 2023). The immediate rewards of internet use may appeal to individuals with ADHD, who may struggle to regulate their use (Augner et al., 2023). Finally, we found anxiety as an associated variable with elevated internet use symptoms, consistent with recent literature showing anxiety as a predictor of internet addiction (M. Chen & Zhang, 2024; Xie et al., 2023).
Although we used the Internet Addiction Test (IAT) - a widely used, valid, and reliable measure-the scale was developed before the current dominance of social media and short-form video platforms, which may limit its sensitivity to contemporary, platform-specific problematic usage patterns. Problematic engagement with short-form video and social media content (e.g., TikTok/Reels-like feeds) may have been captured under the broader construct of elevated internet use symptoms and could not be distinguished at the modality or platform level. Notably, many current platforms are designed to sustain engagement through continuous feeds, algorithmically curated content, rapid feedback loops, and endless scrolling, features that are intended to sustain engagement and may reinforce repetitive use cycles via algorithmic reinforcement.
Within this context, the observed associations of ADHD symptoms, depressive symptoms, and anxiety symptoms with elevated internet use symptoms may be difficult to attribute solely to elevated use of the internet. ADHD-related vulnerabilities-especially executive function difficulties and a stronger preference for immediate over delayed rewards-may increase the appeal of fast-paced digital environments that deliver immediate reinforcement, thereby elevating susceptibility to problematic engagement (Dekkers & van Hoorn, 2022). Similarly, individuals with anxiety symptoms and depressive symptoms may increasingly rely on social media or short-form video content for coping and/or emotion regulation, which may further contribute to problematic use (Zhan & Zhu, 2025; Zubair et al., 2023). Accordingly, our findings on elevated internet use should be interpreted considering the current digital ecosystem, where problematic use of short-form video and social media platforms may represent an increasingly salient risk factor for student mental health.
Patterns of problematic use may also vary by gender. Prior studies suggest that gaming and gaming-related applications may be more prominent among men (Kim et al., 2022), whereas social media-based problematic use was more frequently reported in women (Mari et al., 2023). However, because the IAT does not differentiate modality or platform-specific subtypes of problematic use, future research would benefit from a more fine-grained assessment of not only overall use but also the mode of use (e.g., gaming, short-form video, social media) and preferred platforms.
Limitations
Despite a large sample size, several limitations should be considered when interpreting the findings. First, data were collected through self-report scales without clinical interviews, limiting the confirmation of diagnostic accuracy. The cross-sectional and single-center design restricts the ability to infer causality and generalize the results to the broader university student population. In addition, we were unable to benchmark our sample against institutional demographics (e.g., sex, age, faculty/department distribution); therefore, the representativeness of the sample cannot be confirmed. Accordingly, findings should not be interpreted as population estimates for the broader university student body, and generalization beyond the participating students should be made cautiously. A longitudinal design would have been more effective in determining causal relationships and clarifying temporal dynamics among the identified factors. Crucially, the rates reported in this study represent screening-positive status based on self-report scales, not clinical diagnoses confirmed by psychiatric interviews. Self-report measures can be susceptible to response bias and may overestimate the prevalence of disorders compared to structured clinical assessments. Consequently, our findings should be interpreted as reflecting the burden of symptoms within the student population rather than the true epidemiological prevalence of these psychiatric disorders.
In the regression models, co-occurring symptom domains were included to account for substantial comorbidity and shared symptom burden and to evaluate whether sociodemographic variables remained independently associated after adjustment. Consequently, variables identified in these models should be interpreted as independently associated correlates of screening-positive status rather than predictors of incident disorder. Finally, the strong associations among symptom domains likely reflect co-occurrence or shared variance rather than causal relationships and should be viewed as hypothesis-generating.
Conclusions
Our findings revealed a high burden of elevated symptom levels for depression, anxiety, and ADHD, as well as internet use among university students, underscoring the urgent need for robust mental health support systems within academic institutions. These services must be both accessible and actively promoted, ensuring students can seek help, receive appropriate interventions, or be referred to specialized care when necessary. Particular attention should be given to vulnerable subgroups, such as students with a history of migration and those from low-income backgrounds, to ensure effective mental health promotion and protection within the university population.
In conclusion, this study highlights the pressing need for comprehensive mental health services tailored to the unique needs of university students. By addressing the specific associations identified, institutions can better support the mental well-being of their students, fostering a healthier academic environment.
Footnotes
Acknowledgments
The authors wish to thank Pamukkale University Student Support Unit members and all students who participated.
Ethical Consideration
This study was performed in line with the principles of the Declaration of Helsinki. Approval was granted by the Pamukkale University Non-Interventional Clinical Research Ethics Committee, dated 05.03.2024, and numbered E-60116787-020-508607.
Consent to Participate
Those who provided their consent to participate in the study were included in the study.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets of the current study are available from the corresponding author upon reasonable request.