
Abstract
Sexual and gender minority (SGM) populations include individuals who identify as non-heterosexual and/or whose gender identity does not align with their sex assigned at birth. SGM populations experience higher rates of social deprivation—disadvantages in socioeconomic factors and living conditions—compared to non-SGM groups. While current research highlights the negative health impacts of social deprivation, no work has assessed whether SGM identity moderates associations between social deprivation and mental health symptoms. Further, it is unknown whether specific measures of social deprivation are more strongly associated with mental health. This study aimed to fill these gaps by examining associations between social deprivation and mental health symptoms, as well as whether these relationships vary between SGM and non-SGM groups. Participants (N = 450) recruited from Prolific completed measures of anxiety, depression, schizotypy, and paranoia. The Social Deprivation Index and Social Vulnerability Index were derived from participants’ zip codes. Neither social deprivation measure was significantly associated with mental health symptoms. SGM status did not moderate associations between social deprivation and mental health symptoms, though the SGM group reported lower income levels, higher rates of social deprivation, and were more likely to have previously received mental health diagnoses and treatment compared to the non-SGM group. Results contribute to our understanding of socioeconomic factors related to mental health symptoms, particularly among minoritized groups. Future work should analyze interactions between individual-level and community-level factors on SGM mental health.
Keywords
Introduction
Social factors can have significant and profound effects on overall well-being and quality of life (Office of the Surgeon General, 2021). Populations living in environments with lower resource access may experience social deprivation, defined as poorer quality social health related to a lack of resources (Wright et al., 2019). Research has measured social deprivation using various facets (e.g., socioeconomic status, household characteristics; Agency for Toxic Substances and Disease Registry, 2024; Robert Graham Center - Policy Studies in Family Medicine & Primary Care, 2021), but it is not yet understood whether some measures of social deprivation are more strongly associated with mental health outcomes. Further, measures of social deprivation often neglect the role of individualized experiences, such as minoritized identities. While research has been conducted on the negative mental health effects of social deprivation, the associations between these for marginalized groups, such as sexual and gender minorities (SGM), are poorly understood. This gap is particularly pronounced for mental health symptoms akin to subclinical schizophrenia-like experiences, such as paranoia and schizotypy. This study sought to fill this gap and add to a growing field of research on the impact of social factors on mental health.
In the general population, social deprivation has been associated with physical and mental health (Bevan et al., 2022; Griggs et al., 2022; Liaw et al., 2018). For example, residing in a socially deprived area is related to greater risk of cardiovascular events (Algren et al., 2015; Bevan et al., 2022), cancer diagnoses (Barnard et al., 2015), and maternity-related complications (Haelterman et al., 2003; Patel et al., 2021). These difficulties are compounded by lower access to poorer quality of healthcare in socially deprived areas (Wright et al., 2019). Residing in a socially deprived area has further been correlated with worse well-being (Astell-Burt et al., 2012; Barr, 2018; Ribeiro et al., 2018) and greater anxiety and depression (Wright et al., 2019). Moreover, some work has investigated connections to subclinical symptoms aligned with schizophrenia. McElroy and colleagues (2019) recruited participants primarily from areas with prominent economic disadvantage to assess the relationships between mental health symptoms (i.e., paranoia, auditory hallucinations, concentration difficulties) and environmental factors (e.g., social cohesion and disorder). Socially deprived participants reported experiencing paranoia at a significantly higher rate than those not socially deprived (McElroy et al., 2019). Further, those who are socially deprived may have fewer resources available to effectively cope with mental health symptoms (Palermos et al., 2024) and may be at risk for using maladaptive strategies, such as smoking or unhealthy diet (Algren et al., 2015; Ribeiro et al., 2018). Lack of access to care coupled with higher tendencies to engage in unhealthy coping suggest a high likelihood of poorer mental health in areas of high social deprivation.
Yet, while some studies have found significant associations between social deprivation and mental health (e.g., Wright et al., 2019), other studies have not (e.g., Dunn et al., 2015). One explanation for these disparate findings may be the approach to measuring social deprivation. Often, measures of social deprivation are based on individual-level factors (e.g., socioeconomic status, income, housing quality; Hatzenbuehler et al., 2024; Lee et al., 2018). A relatively recent body of work has begun to examine area-level social deprivation. One metric of area-level deprivation is the Social Deprivation Index (SDI; Butler et al., 2012), a composite of neighborhood-level social and economic factors, including seven variables indicative of community deprivation (e.g., neighborhood poverty rates, education level). The SDI is derived from participants’ residential zip codes (Robert Graham Center - Policy Studies in Family Medicine & Primary Care, 2021). The composite nature of the data allows for neighborhood disadvantages to be quantified without relying on a single-item or self-report measure (Butler et al., 2012; Robert Graham Center - Policy Studies in Family Medicine & Primary Care, 2021). A second metric, the Social Vulnerability Index (SVI), was designed by the Agency for Toxic Substances and Diseases Registry and also measures community deprivation through zip codes (2024). The SVI places greater emphasis on social composition metrics, including the proportion of a neighborhood that is living without health insurance or living with a disability (Agency for Toxic Substances and Disease Registry, 2024; Robert Graham Center - Policy Studies in Family Medicine & Primary Care, 2021). Unfortunately, relatively little work has examined area-level deprivation via the SDI or SVI, and no study to date has compared relationships across these two measures of social deprivation.
With existing work sparse and findings mixed (Fagg et al., 2013), research is needed to clarify relationships between social deprivation (across both the SDI and SVI) and mental health symptoms. One potential confound that may have contributed to past mixed findings is that these relationships could differ for participants of different identities. For example, sexual or gender minority (SGM) populations experience a higher risk for living in socially deprived areas (Hatzenbuehler et al., 2024; Henderson et al., 2022). Some research suggests that approximately 40% of youth without stable housing identify as SGM (Philbin et al., 2022). Further, neighborhoods with a greater density of SGM residents tend to have a disproportionate lack of resources, including less access to supportive public services (Lee et al., 2018). SGM residents also have less access to public infrastructure (e.g., parks, health clinics, HIV testing sites) and poor environment exposure (e.g., air pollution; Lee et al., 2018).
A wealth of research further demonstrates that SGM participants are at greater risk for mental health symptoms, including depression, anxiety, substance use, and suicidal thoughts and behaviors (Kia et al., 2021; Plöderl & Tremblay, 2015). These disparities are best understood within the framework of Minority Stress Theory, which posits that stressors associated with one’s SGM identity, such as discrimination and harassment, can contribute to negative mental health outcomes (Meyer, 2003). Minority stressors often stem from structural stigma, defined as institutional, cultural, and societal forces that limit a group’s ability to increase overall well-being and pursue resources and opportunities (Hatzenbuehler et al., 2024). Both structural stigma and discrimination impact access to employment, education, and housing, all of which may lead to higher levels of social deprivation (Hatzenbuehler et al., 2024; Kia et al., 2021; Philbin et al., 2022; Robert Graham Center - Policy Studies in Family Medicine & Primary Care, 2021).
Importantly, mental health disparities among SGM adults appear to be exacerbated by living conditions. SGM residents in highly socially deprived areas frequently endorse more severe negative mental health symptoms than those living in less deprived areas (Philbin et al., 2022). Yet, the field has not directly assessed relationships between social deprivation and mental health symptoms in SGM populations, particularly within the realm of schizotypy and paranoia. Given prior work showing both higher mental health symptoms and worse social deprivation among SGM populations, it is possible that the social deprivation-mental health relationship is stronger among this group. Alternatively, minority stressors may overshadow the impacts of social deprivation among this group. This is an empirical question in need of study.
This study aimed to fill this gap, examine associations between area-level social deprivation and mental health outcomes, including schizophrenia-like symptoms, and compare relationships with SDI and SVI indices. We hypothesized that greater social deprivation would be associated with worse mental health symptoms (higher levels of anxiety, depression, schizotypy, and paranoia). Further, we hypothesized that the relationships between social deprivation and mental health symptoms (i.e., anxiety, depression, schizotypy, and paranoia) would be moderated by SGM status, such that social deprivation would be more strongly associated with mental health symptoms for SGM adults. Additionally, we hypothesized that SGM participants would have higher levels of social deprivation, lower income, and be more likely to report past mental health diagnoses and treatment than non-SGM participants. Addressing these research gaps regarding social deprivation’s role on mental health may lead to a more comprehensive understanding of the effects of social deprivation for vulnerable groups, specifically SGM populations.
Methods
Participants & Procedures
Participants (n = 533) were recruited through Prolific, an online survey platform (//www.prolific.com), and were eligible for the study if they were 18 years of age or older, residing in the United States, and fluent in English. Additionally, participants were required to have a smartphone for additional procedures not relevant to the current analyses. Following signup, Prolific redirected participants to complete the survey through Qualtrics. Participants provided informed consent and completed assessments of mental health symptoms (anxiety, depression, schizotypy, and paranoia). Participants also completed a variety of tasks and self-report questionnaires that were not relevant to the scope of the current research question. At the end of the study, participants provided demographic information, including their residential zip code, sexual orientation, and gender identity. The survey took approximately 30 minutes for participants to complete, and participants were compensated $6 through Prolific. Throughout the survey, five attention check items (e.g., “Driving from New York to San Francisco is generally faster than flying between these cities” and “I find that I often walk with a limp, which is the result of a skydiving accident”) were included to ensure participants were adequately attending to the survey (Chapman & Chapman, 1983). The university’s Institutional Review Board approved all procedures.
Measures
Sexual and Gender Minority (SGM) Status
Participants were dichotomized into SGM and non-SGM groups based on their self-reported sexual orientation and gender identity within the study’s demographics form. Participants who identified as a sexual orientation other than “heterosexual” (including “gay or lesbian,” “bisexual,” “pansexual,” “queer,” or “unsure or questioning”) were classified as a sexual minority group member. Participants who identified as “transgender” or “nonbinary” were classified as a gender minority group member. Participants were included in the SGM group if they were a member of either a sexual or gender minority group. This approach of dichotomizing SGM and non-SGM groups is consistent with previous research in the field that has included sexual and gender minority people in a single SGM group (Livingston et al., 2017; Newberger et al., 2022), and allows inclusion of gender minority participants, who are frequently excluded from studies when their samples are too small for subgroup comparison. Furthermore, minority stressors and systemic barriers are commonplace across SGM identities (Henderson et al., 2022; Moorhead et al., 2024).
Social Deprivation Index (SDI)
SDI was calculated from participants’ zip codes using a database provided by the Robert Graham Center - Policy Studies in Family Medicine & Primary Care (2021). The SDI, a single number ranging from 0-100, is calculated based on seven characteristics for the area, all reflected as the proportion of residents with a given characteristic: living in poverty, with an education level under 12 years, living within a single-parent household, renting housing, living in overcrowded housing, without a car, and those under 65 years old who are unemployed (Robert Graham Center - Policy Studies in Family Medicine & Primary Care, 2021). Higher scores on the SDI indicate worse social deprivation (Robert Graham Center - Policy Studies in Family Medicine & Primary Care, 2021). The SDI has demonstrated appropriate reliability for examining associations with health-related outcomes (Butler et al., 2012).
Social Vulnerability Index (SVI)
Similar to the SDI, participants’ residential zip codes were used to calculate their SVI score using a database provided by the Agency for Toxic Substances and Disease Registry (Agency for Toxic Substances and Disease Registry, 2024). The SVI, a single number ranging from 0 to 1, is calculated using 16 variables from four central domains, including socioeconomic status, household characteristics, racial and ethnic minority status, and housing and transportation (Agency for Toxic Substances and Disease Registry, 2024). Higher values of the SVI indicate greater social deprivation (Agency for Toxic Substances and Disease Registry, 2024). The SVI has demonstrated reliability in assessing correlates of health outcomes (Agency for Toxic Substances and Disease Registry, 2024).
Generalized Anxiety Disorder-7 (GAD-7)
The GAD-7 is a 7-item self-report scale that assesses anxiety symptom severity over the previous two weeks (Spitzer et al., 2006). The measure uses a Likert scale to indicate severity of seven symptoms aligning with generalized anxiety disorder (American Psychiatric Association, 2022; Spitzer et al., 2006). Higher scores indicate worse anxiety (Spitzer et al., 2006). Within the present study, the GAD-7 demonstrated excellent internal reliability (α = .94).
Patient Health Questionnaire-8 (PHQ-8)
The PHQ-8 is an 8-item self-report scale that assesses severity of depressive symptoms (Kroenke et al., 2009). The PHQ-8 features a Likert scale assessing eight components of depression (American Psychiatric Association, 2022; Kroenke et al., 2009). Higher scores indicate worse depression (Kroenke et al., 2009). The PHQ-8 demonstrated excellent internal reliability in the present study (α = .91). The PHQ-8 excludes item 9 of the PHQ-9, which assesses suicidality. This item was excluded due to the online nature of the study, as participant risk would not be able to be addressed by the researchers. The PHQ-8 and PHQ-9 are highly correlated (Wu et al., 2020) and use of the PHQ-8 through online surveys is consistent with other published literature (Marshall et al., 2024; Thake et al., 2025).
Schizotypal Personality Questionnaire-Brief Revised (SPQ-BR)
The SPQ-BR is a 32-item scale that assesses schizotypy (Cohen et al., 2010). The questionnaire allows participants to indicate the strength of their agreement on a 5-point Likert Scale. The SPQ-BR features three subscales, including Interpersonal, Disorganized, and Cognitive-Perceptual schizotypy symptoms (Cohen et al., 2010). Higher scores indicate higher schizotypy (Cohen et al., 2010). The SPQ-BR demonstrated excellent internal reliability in the present study (α = .95).
Paranoia Scale
The Paranoia Scale is a 20-item scale that assesses paranoid thoughts within the general population (Fenigstein & Vanable, 1992). The scale asks participants to rate the applicability of several statements that apply to their thinking (e.g., “someone has it in for me”) on a 5-point Likert scale. Higher scores indicate worse severity of paranoia (Fenigstein & Vanable, 1992). The Paranoia Scale demonstrated excellent internal reliability in the present study (α = .94).
Analyses
All analyses were conducted using SPSS Statistics version 29 (IBM Corp, 2023). Participants were excluded from the analyses if they responded incorrectly to more than 2 attention check items, if they were in the fastest 10% of response times, or if they did not provide responses to the included measures. To address the first hypothesis, Pearson’s R correlations were run to assess relationships between SDI, SVI, and mental health symptoms (i.e., schizotypy, anxiety, paranoia, and depression).
To address the second hypothesis, Hayes’ PROCESS Macro (Hayes & Little, 2022) was used to investigate whether SGM status moderated associations between the SDI/SVI and mental health symptoms. This procedure uses OLS regression to assess moderation. For each analysis, either SDI or SVI was entered as the independent variable, SGM status was entered as a moderator, and mental health symptoms (schizotypy, anxiety, paranoia, depression) were entered as dependent variables in separate models. This resulted in 8 models. To assess differences between SGM and non-SGM groups in SVI and SDI scores, independent samples t-tests were used, and to assess group differences for relevant sociodemographic and treatment history variables (i.e., income, mental health diagnostic history, and mental health treatment history), chi-square analyses were used.
Results
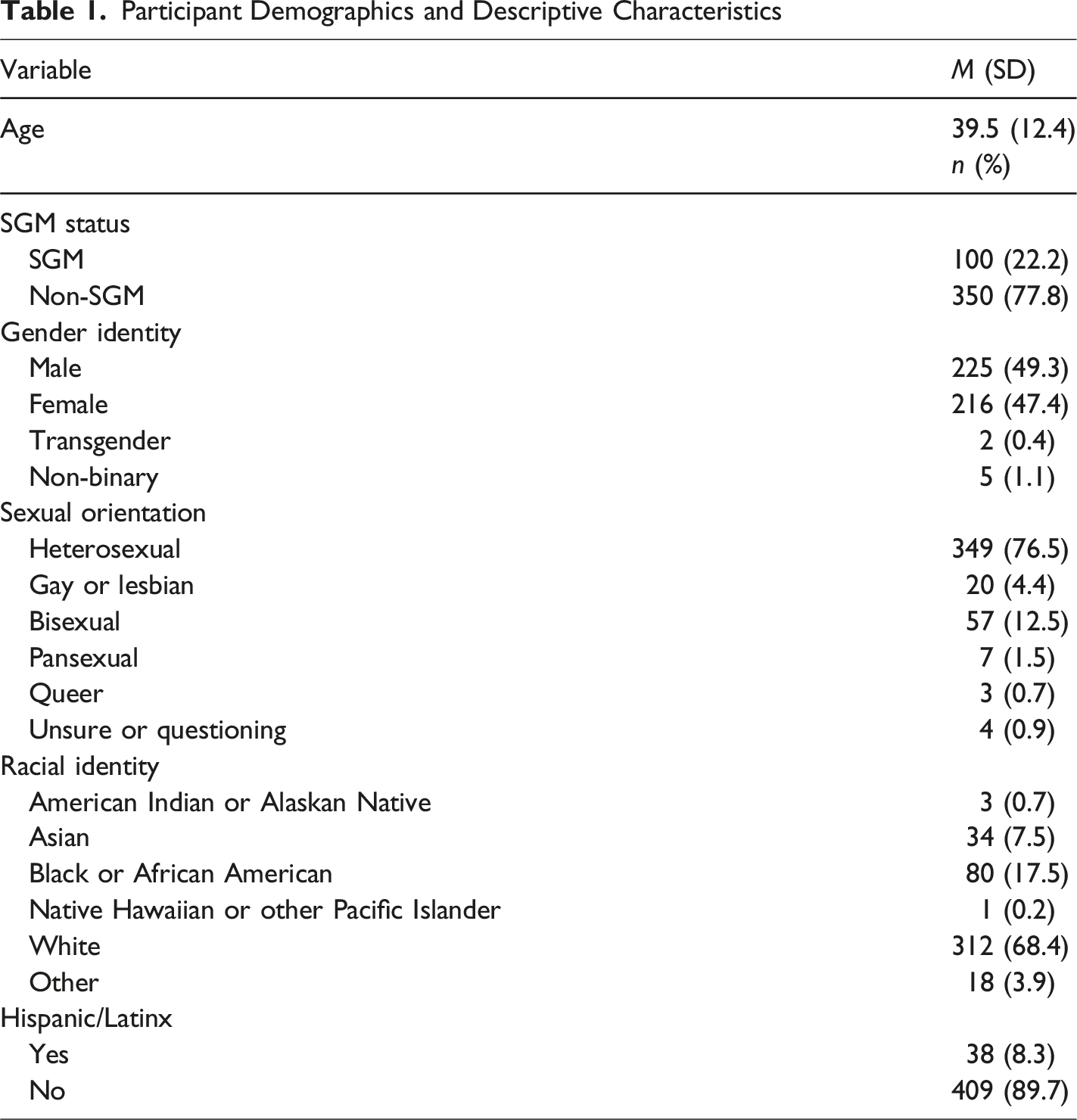
Participant Demographics and Descriptive Characteristics
Pearson’s Correlations Between Relevant Variables
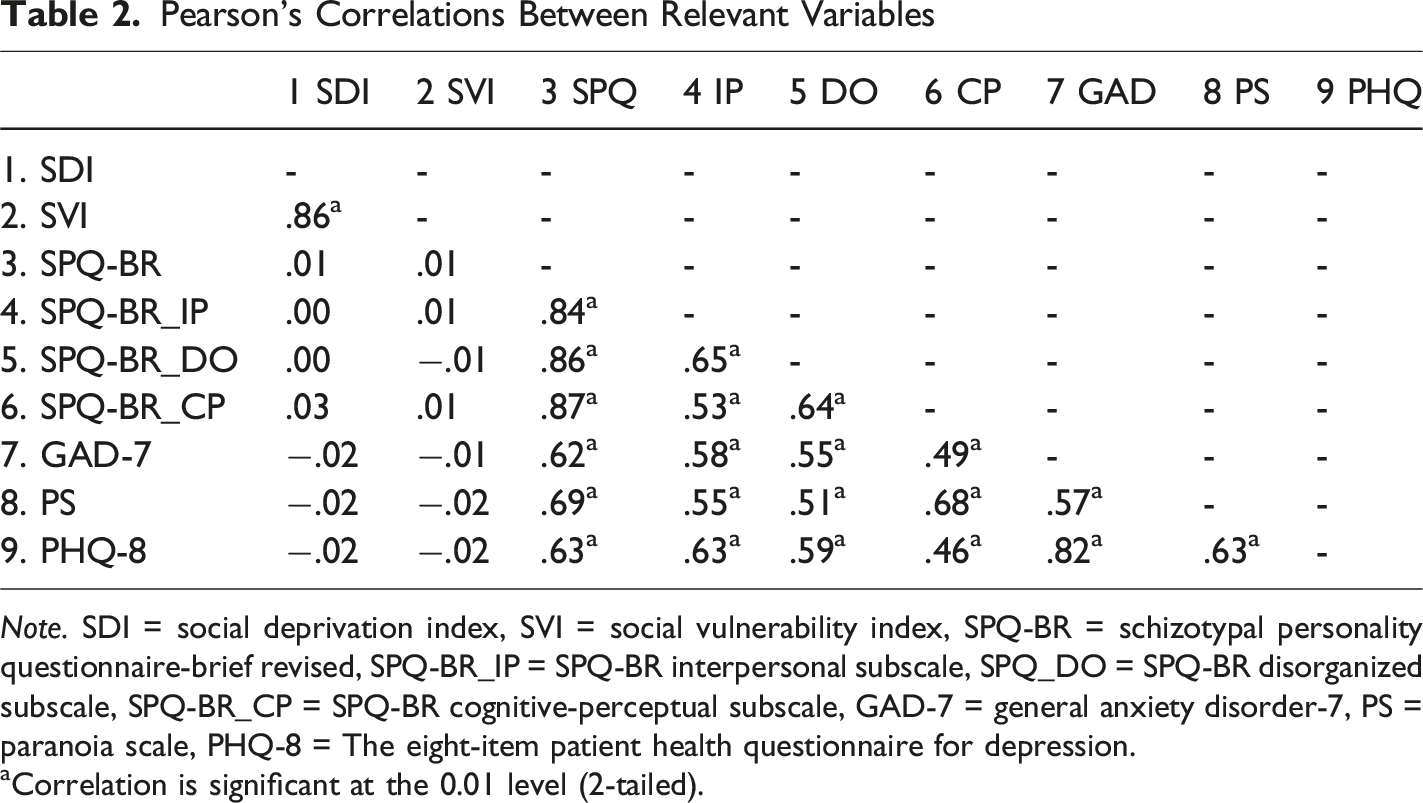
Note. SDI = social deprivation index, SVI = social vulnerability index, SPQ-BR = schizotypal personality questionnaire-brief revised, SPQ-BR_IP = SPQ-BR interpersonal subscale, SPQ_DO = SPQ-BR disorganized subscale, SPQ-BR_CP = SPQ-BR cognitive-perceptual subscale, GAD-7 = general anxiety disorder-7, PS = paranoia scale, PHQ-8 = The eight-item patient health questionnaire for depression.
aCorrelation is significant at the 0.01 level (2-tailed).
Results for SGM Identity Moderating SDI and Mental Health Symptoms
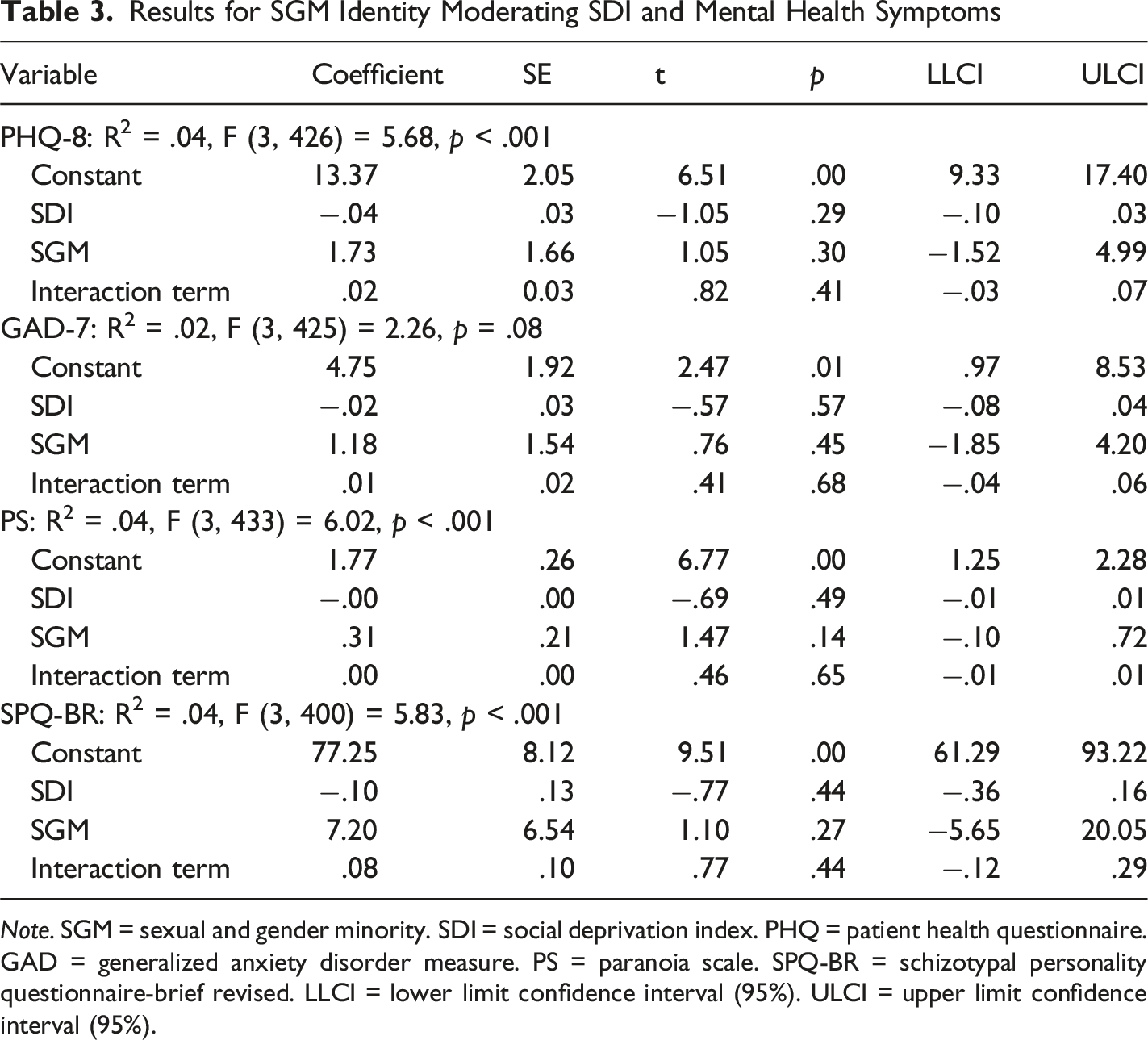
Note. SGM = sexual and gender minority. SDI = social deprivation index. PHQ = patient health questionnaire. GAD = generalized anxiety disorder measure. PS = paranoia scale. SPQ-BR = schizotypal personality questionnaire-brief revised. LLCI = lower limit confidence interval (95%). ULCI = upper limit confidence interval (95%).
Results for SGM Identity Moderating SVI and Mental Health Symptoms
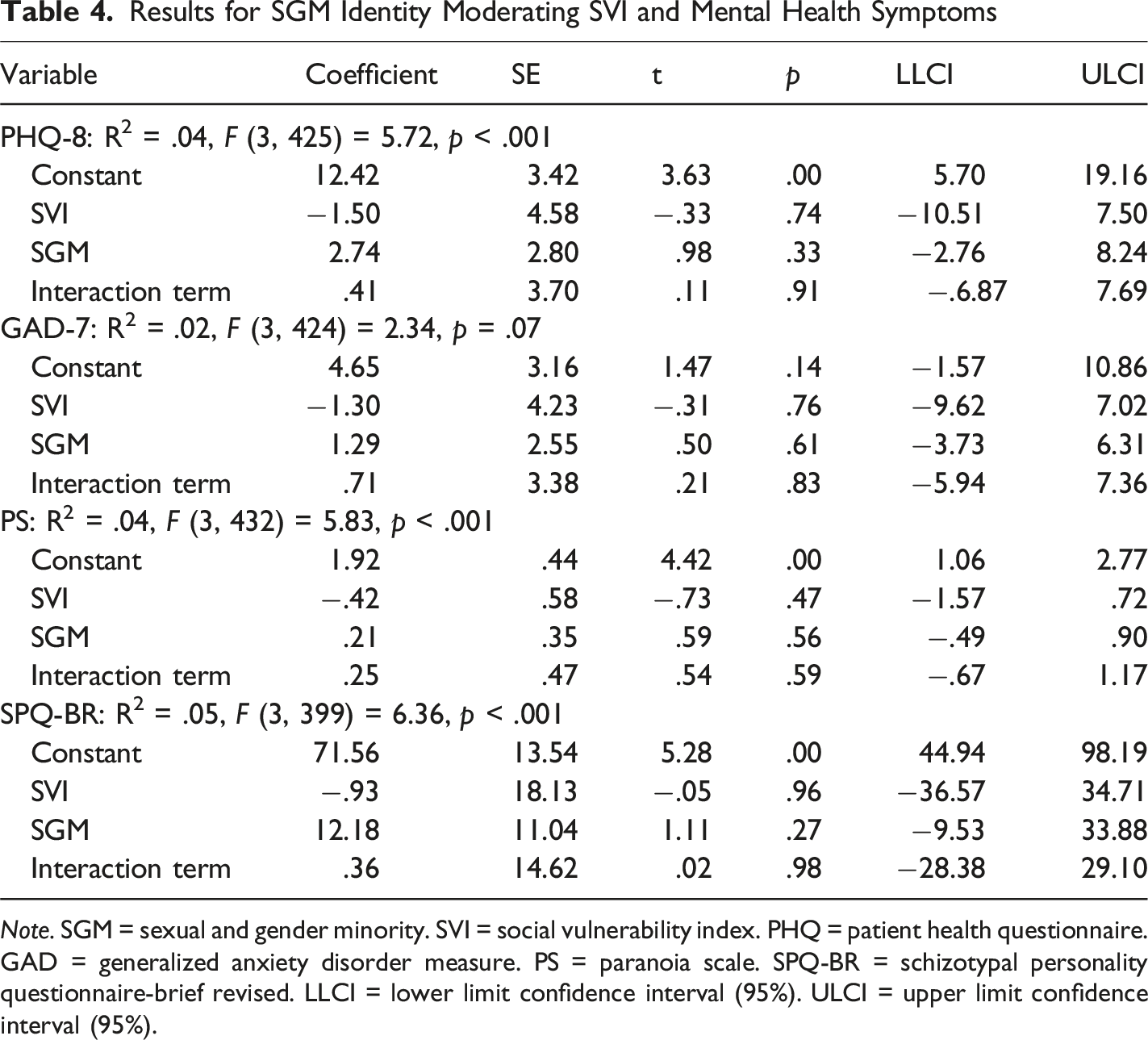
Note. SGM = sexual and gender minority. SVI = social vulnerability index. PHQ = patient health questionnaire. GAD = generalized anxiety disorder measure. PS = paranoia scale. SPQ-BR = schizotypal personality questionnaire-brief revised. LLCI = lower limit confidence interval (95%). ULCI = upper limit confidence interval (95%).
While moderations were non-significant, there were significant group differences on key variables. SGM participants had significantly higher SDI scores [t (436) = −1.70, p = .043] than non-SGM participants. Further, SGM participants had lower income compared to non-SGM participants, [X 2 (5, 450) = 15.00, p = .01] and were more likely to report a past mental health diagnosis [X 2 (1, 450) = 19.15, p < .001] and past mental health treatment [X 2 (1, 450) = 14.67, p < .001] than non-SGM participants. Notably, SVI scores did not differ significantly between SGM and non-SGM groups, [t (434) = −1.30, p = .20].
Discussion
The current study explored associations between social deprivation and mental health symptoms (i.e., anxiety, depression, schizotypy, and paranoia) within SGM and non-SGM groups. Contrary to hypotheses, social deprivation was not significantly associated with any mental health symptoms in the overall sample. Moreover, SGM status did not moderate associations between social deprivation and symptoms. Despite this, SGM participants reported experiencing significantly more mental health and financial difficulties. Specifically, SGM participants were significantly more likely to have lower income levels, live in socially deprived areas, and report past mental health diagnoses and treatment than non-SGM participants, suggesting that SGM groups may experience more mental health and socioeconomic difficulties than cisgender, heterosexual people. These findings align with previous literature among SGM participants, underscoring the significant disparities experienced by this group.
No significant associations were found between social deprivation and schizotypy, anxiety, paranoia, or depression. This is consistent with some past research that found no significant relationship between deprivation and mental health (Dunn et al., 2015; Dupéré et al., 2012; Fagg et al., 2013). Yet, findings are inconsistent with more recent literature suggesting that negative mental health symptoms are more common among residents of areas with high social deprivation (Astell-Burt et al., 2012; Barr, 2018; Griggs et al., 2022; McElroy et al., 2019; Short et al., 2018). One explanation for disparate findings may be based on sample differences. Associations may vary depending on the population examined, such as different regions in the United States or certain minoritized groups. This is in line with research on intersectional identities. Current literature suggests that experiences of stigma related to both one’s racial identity and sexual orientation are associated with disparities in anxiety and depression symptoms (Bi et al., 2020), and significant risks exist for the internalization of damaging attitudes towards one’s own dual minority identities (Sarno et al., 2021). The current sample and analyses may have been too broad to capture nuanced relationships specific to certain groups. Indeed, the SGM sample for this study was primarily composed of sexual minority participants, with a smaller subset identifying as a gender minority. Our sample was too small to examine differences based on additional identities, such as race. Future work should examine the role of intersectional identities on the mental health effects of social deprivation.
Additionally, social deprivation may have a larger impact on mental health during childhood and adolescence. Low socioeconomic status and adverse neighborhood conditions are correlated with depressive symptoms (Barr, 2018); thus, development may be negatively impacted through lower resource availability in areas of high social deprivation (Letourneau et al., 2011). Residing in a socially deprived area during development may also have downstream effects on mental health later in life. Research is needed to assess the impact of both childhood and adult deprivation levels on mental health symptoms in SGM groups, particularly using longitudinal methods to determine whether childhood deprivation levels affect mental health in adulthood.
Results using the SDI and SVI were largely in-line with each other and the two measures were highly correlated. While the SDI and SVI include similar metrics, such as poverty and unemployment, the SVI includes social factors as well, such as proportion of the population that is a racial and ethnic minority, is proficient in English language, and lacks health insurance (Agency for Toxic Substances and Disease Registry, 2024; Robert Graham Center - Policy Studies in Family Medicine & Primary Care, 2021). The only disparate finding between these measures was that the SGM group had significantly higher levels of deprivation on the SDI but not the SVI. This finding indicates that it may be beneficial to examine social deprivation in multiple ways, including the SDI, SVI, and other qualitative measures.
Future work should aim to create and validate measures of social deprivation that may be better predictors of mental health symptoms. This may be initiated through qualitative interviews in which participants can voice which aspects of their neighborhood environment affect their mental health, through a discussion of their individualized, nuanced experiences with deprivation. In particular, SGM participants may have unique experiences in their neighborhood that are currently missed through established measures, such as the SDI or SVI. For instance, the social deprivation measures do not include how accepting of SGM identities a neighborhood may be, which is likely related to SGM residents’ experience in the area and their overall mental health. Additionally, zip codes are representative of large geographic areas and may not capture stressors or protective factors that happen at a small, neighorhood-level. Overall, diversifying measurement approaches would allow for a more comprehensive perspective of SGM and non-SGM social deprivation and its link to mental health.
Of note, the current study did not assess individual-level protective factors, such as social support, community connection, or economic stability. Some literature supports higher income levels as a buffer against anxiety, depression, and quality of life (Gresenz et al., 2001; Ribeiro et al., 2017; Shields-Zeeman & Smit, 2022), and increases in income are correlated with improved mental health (Shields-Zeeman & Smit, 2022). Income inequality and depressive symptoms are also related (Ribeiro et al., 2017). Therefore, it is possible that the participants residing in areas of high social deprivation may have individual protective factors that buffer the effects of their environment, such as relatively higher income or greater economic stability compared to their average neighborhood level. Moreover, social protective factors may be particularly relevant to assess for SGM participants, due to the importance of social support for mental health within this group (Jacmin-Park et al., 2022; Kia et al., 2021; Paceley et al., 2017). Literature exploring perceptions of social support on SGM participants’ well-being found that acceptance and support from family members, friends, and the broader community protects against stress, depression, and anxiety (Jacmin-Park et al., 2022; Paceley et al., 2017). Future work should investigate the role of protective factors on social deprivation and mental health for both SGM and non-SGM participants.
SGM participants were more likely to report past mental health diagnoses and treatment than non-SGM participants. Consistent with our findings, a wealth of research suggests that SGM groups experience higher rates of mental health diagnoses and worse symptom severity when compared to non-SGM groups (Plöderl & Tremblay, 2015; Hatzenbuehler et al., 2024; Henderson et al., 2022). Mental health disparities in SGM populations are theorized to be due, in part, to the increased stressors they experience related to their SGM identity (Meyer, 2003). Moreover, while stigma and discrimination are significant barriers to seeking treatment for SGM groups (Hatzenbuehler et al., 2024), SGM groups tend to engage in mental health treatment frequently (Artime et al., 2024; Benjamin et al., 2023; Conner et al., 2023). Therefore, despite established mental health disparities in this group, research has shown that symptoms can be reduced through appropriate, affirmative treatments (Hinrichs & Donaldson, 2017; Johnson, 2012). Additional research is needed to examine whether barriers and facilitators to mental health treatment for SGM people vary depending upon their level of social deprivation.
SGM participants had significantly higher social deprivation (as measured by the SDI) and lower income compared to non-SGM participants, although SGM status did not significantly moderate associations between social deprivation and mental health symptoms. These findings are consistent with past research suggesting that SGM groups tend to live in areas with worse social deprivation (Kia et al., 2021) and have lower income (Butler et al., 2012). SGM groups experience societal-level inequities such as discrimination in housing, employment, and education (Philbin et al., 2022), perpetuated by exclusionary policies that result in lower availability of resources (Hatzenbuehler et al., 2024). While minority stress was not directly measured in this study, moderation findings suggest that stressors experienced by SGM groups do not amplify potential mental health effects of social deprivation. In other words, SGM groups may not experience a stronger association between social deprivation and mental health symptoms, as their baseline levels of stress may be heightened, resulting in a ceiling, rather than additive, effect. Additional research is needed to directly examine the extent to which environmental stress and minority stress interact in SGM groups.
This study has limitations. As this study was conducted online, participation required access to a device with internet. This may limit generalizability, particularly since the included measures assessed social deprivation. Despite this limitation, our sample represented the full range of scores on the SDI and SVI. Additionally, this study included a combined SGM group, as examination of subgroups was not feasible with the current sample size. While this approach is consistent with other research (Livingston et al., 2020; Outland, 2016), further examination of specific subgroups is needed and would be beneficial. While sexual minority and gender minority participants often experience similar stressors (Henderson et al., 2022; Moorhead et al., 2024), some nuance of their unique experiences may be missed by collapsing into a single SGM group.
Further, individual-level contributors to social deprivation (e.g., access to a car, unemployment) were not assessed in this study, precluding us from examining interactions between area-level and individual-level factors on mental health. Lastly, history of mental health diagnoses and treatment were based on self-report from participants. In the future, researchers may wish to incorporate clinical interviews or medical record review to examine these variables more comprehensively.
Future work should investigate barriers to mental healthcare for SGM groups residing in areas of high social deprivation outside of the United States, including financial constraints, as well as their satisfaction with the mental health services they have received. Additionally, work is needed to assess the interaction between area-level and individual-level factors of social deprivation (e.g., income and social support) on mental health symptoms, including whether SGM community connection may buffer the effects of social deprivation on mental health. A conceptualization of social deprivation that considers both economic and social facets of an individual’s experience may also be helpful. Formulation of a more comprehensive social deprivation measure may benefit from a qualitative interview or mixed methods approach, in which participants’ perceptions of the role of these factors on mental health could be assessed. Specifically, participants could be asked to reflect on their neighborhood environment, including which aspects may serve as positive and negative contributors to their mental health. For SGM participants, discussion of minority stressors and positive community connection may be particularly fruitful for examining environmental stress and protective factors.
Footnotes
Acknowledgements
Research reported in this presentation was funded by the Drapeau Center for Undergraduate Research (DCUR) through an Eagle Scholars Program for Undergraduate Research (Eagle SPUR) grant for Bea Twilbeck. Additional funding was contributed by the University of Southern Mississippi’s School of Psychology. All methods are approved by the University of Southern Mississippi IRB. (Ethical Clearance Reference Number: 22-1466).
Ethical Considerations
All methods are approved by the University of Southern Mississippi IRB (Ethical Clearance Reference Number: 22-1466).
Consent to Participate
The study was approved by the University of Southern Mississippi IRB (Ethical Clearance Reference Number: 22-1466) on December 14, 2022. Participants provided written informed consent prior to study participation.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Drapeau Center for Undergraduate Research through an Eagle Scholars Program for Undergraduate Research (Eagle SPUR) grant for Bea Twilbeck at the University of Southern Mississippi. Additional funding was contributed by the University of Southern Mississippi’s School of Psychology.
Declaration of Conflicting Interests
The authors declare no potential conflicts of interest within the realms of research, authorship, and/or publication.
Data Availability Statement
Data is available from the corresponding author upon reasonable request.