
Abstract
We explored whether emotional intelligence (EI) and its four dimensions individually promoted approach-related behaviors (i.e., sociability) or mitigated avoidance-related behaviors (i.e., internalizing behaviors) in adults clinically diagnosed with anxiety prior to undergoing cognitive behavioral therapy. Participants were 160 patients (M age = 39.50 years, SD = 13.65, 28.1% male) who completed online questionnaires related to shyness, EI, sociability, and internalizing behaviors prior to the start of group treatment. We found sex-specific EI moderating effects on the relation between shyness and sociability. Among women, EI Self-Emotion Appraisal, a dimension of EI, moderated this relation (p < .05) by reducing the negative effects of shyness on sociability. In men, the EI Others’ Emotion Appraisal dimension played a comparable role. The findings suggest that EI may be a promising target of intervention to increase social approach behaviors in some clinically anxious patients, with particular relevance for understanding and addressing sex-related differences in socio-emotional abilities.
Keywords
Temperamental shyness is a foundational characteristic related to behavioral inhibition and anxious avoidance in real or imagined social situations (Crozier, 1979). It is linked to many poor psychosocial outcomes, including low social competence (Miller, 1995), social withdrawal (Asendorpf, 1990), poor peer relationships (Doey et al., 2014), low self-confidence (Chęć, 2019), low self-esteem (Crozier, 1995), maladaptive self-blame (Cheek et al., 1986), dysfunctional inward-focused coping strategies (Findlay et al., 2009), and internalizing behaviors in general (e.g., depression, social anxiety; Geng et al., 2021; Schneier et al., 2002). Despite numerous studies highlighting the poor psychosocial consequences associated with shyness, not all shy individuals experience these difficulties. This suggests there may be untested moderating factors that could explain this duality. In the present study, we examined whether individual differences in emotional intelligence (EI) served as one of the factors that affect the relation between shyness and approach-avoidance related behaviors, such as sociability and internalizing behaviors, respectively, especially in a clinical sample of adults in which these outcomes are considered problematic.
Emotional Intelligence
EI is a concept that connects emotions with cognition (Drigas & Papoutsi, 2018). It is defined as the ability to understand and utilize one’s own and others’ emotions to facilitate adaptive thinking and problem solving to achieve specific goals (Salovey & Mayer, 1990). In addition, EI is conceptualized as a set of socio-emotional skills that foster adaptive cognitive and emotional development (Basu & Mermillod, 2011). Corroborating this idea, studies have indicated that higher EI leads to overall success across various domains of psychosocial functioning, including social relations (Lopes et al., 2004), adaptive coping strategies (e.g., emotional regulation and stress resistance, Fteiha & Awwad, 2020; Laborde et al., 2014), and empathy, all of which contribute to resilience in social challenges (Beauvais et al., 2017). Conversely, low EI is associated with higher levels of clinical symptoms of anxiety and depression in both clinical and non-clinical groups (Fernández-Berrocal et al., 2006; Summerfeldt et al., 2011). Taken together, these studies suggest that EI is a theoretically grounded and empirically supported construct, making it a promising moderating factor of socio-emotional outcomes, including sociability and internalizing behaviors.
Approach- and Avoidance-Related Behavioral Patterns in Clinical Populations
Generally, a decline in prosocial behaviors are commonly documented in individuals with Generalized Anxiety Disorder (GAD), which involves excessive and uncontrollable worries across multiple domains, such as worries over finances, health, school, work, and life in general, and Social Anxiety Disorder (SAD), which is characterized by a persistent fear or anxiety about social situations and social scrutiny (American Psychiatric Association, 2022; Barrera & Norton, 2009). To manage heightened anxiety and perceived threats, individuals with GAD and SAD tend to rely on maladaptive approach strategies, such as reassurance-seeking (e.g., seeking validation from others, such as friends and family; Helbig-Lang & Petermann, 2010). While these strategies may provide temporary relief from anxiety, overreliance on them may maintain and even exacerbate anxiety in the long term. Such overreliance likely increases self-focused attention that intensifies anxiety and limits opportunities to engage with and learn from social feedback, which in turn may lead to interpreting social cues as negative by default (Leigh et al., 2021).
Avoidance behaviors are also a hallmark maladaptive coping strategy commonly observed across clinical populations. Notably, individuals with GAD and SAD frequently exhibit heightened avoidance behaviors, such as refraining from attending social events or avoiding decision-making, thereby further amplifying feelings of anxiety and isolation (Helbig-Lang & Petermann, 2010). Research has suggested that these individuals show a threat-related attentional bias characterized by heightened vigilance, which may sustain internal avoidance processes (i.e., worry) and reduce engagement with emotionally meaningful social cues (Bar-Haim et al., 2007).
EI and Maladaptive Psychosocial Outcomes
It is plausible that the characteristics of EI could attenuate avoidance behaviors, especially since this moderating influence has been documented in nonclinical samples of children. Specifically, Jung et al. (2023) found that in typically developing 8- to 9-year-olds, higher EI (measured as the mean of four subscales) weakened the association between shyness and avoidance behaviors (i.e., internalizing behaviors) and highlighted its protective role during early development and potential to foster healthier social adjustment. This moderating effect was not observed in young adults (Jung et al., 2025). Instead, among shy female adults, higher levels of social approach behaviors were associated with elevated scores of the EI dimension, Others’ Emotion Appraisal. This difference in EI moderating effects suggests that it may shape approach and avoidance behaviors in distinct ways across the lifespan, perhaps by buffering vulnerability in childhood and facilitating social engagement in adulthood. However, it remains unclear whether this pattern extends to clinical populations, as prior research has primarily focused on nonclinical samples.
Sex Differences
Although most EI research has suggested that there are no significant sex differences in EI (Meshkat & Nejati, 2017; Pardeller et al., 2017), a few studies have indicated there may be exceptions to this pattern (León et al., 2024; Petrides & Furnham, 2000). For instance, Di et al. (2022) reported that women scored higher on the EI subscale of Others’ Emotion Appraisal than men, whereas men scored higher on the Use of Emotion subscale. Similarly, Saklofske et al. (2003) also observed a gender difference in EI subscales: women exhibited higher scores in Appraisal of Emotions and Social Skills, while men scored higher in the Utilization of Emotions subscale. These findings indicate that global EI differences are relatively small, but that specific emotional competencies may vary across sexes. Such differences could partly explain why there are sex-related patterns in approach and avoidance behaviors, such as internalizing and social behaviors.
Indeed, a substantial body of research indicates that women are more vulnerable than men to the development of internalizing problems, including difficulties with anxiety and depression (Kessler, 2003; Pigott, 2003). This heightened vulnerability has been attributed, in part, to a greater tendency toward rumination (i.e., a passive focus on negative feelings or emotions) and an increased reliance on interpersonal processes such as social support (Johnson & Whisman, 2013; Stewart et al., 2022). Likewise, research has also documented sex-related differences in sociability and social tendencies. For example, Eagly and Wood (1991) reported that men exhibited lower levels of social engagement compared to women. More broadly, social behavioral differences have been attributed to learned behaviors shaped by cultural, social, and gender norms (Chaplin, 2015; Zahn-Waxler et al., 2000), as well as to underlying biological factors (McRae et al., 2008). Altogether, these findings underscore the importance of examining sex and EI as moderating factors of socioemotional processes, rather than as fixed or static determinants.
The Present Study
This study centered on two primary objectives. The first was to determine whether EI and/or its four dimensions moderated the relation between shyness and sociability in a clinical sample of individuals diagnosed with anxiety, with the aim of identifying social-emotional skills that might promote social approach behaviors (i.e., reduce their natural tendency to withdraw). The second objective was to determine whether EI and/or its four dimensions moderated the positive relation between shyness and internalizing behaviors, a particularly relevant question given the prominence of internalizing difficulties in clinically anxious populations.
Building on previous findings that EI moderates (a) the negative relation between shyness and sociability in a nonclinical sample of young adults (Jung et al., 2025), and (b) the positive relation between shyness and internalizing behaviors in young children (Jung et al., 2023), we hypothesized that relatively higher levels of EI would attenuate (1) the negative relation between shyness and sociability and (2) the positive relation between shyness and internalizing behaviors in our clinically anxious sample.
Although the Wang and Law Emotional Intelligence Scale (WLEIS) comprises four distinct dimensions (Self-Emotion Appraisal, Others’ Emotion Appraisal, Use of Emotion, Regulation of Emotion), most prior research has examined EI as a global construct when investigating mental health and social outcomes (e.g., Davis & Humphrey, 2014; Lopes et al., 2004; Schutte et al., 2007). Although the validity of the WLEIS subscales has been well established (Mendoza Flores et al., 2024; Shi & Wang, 2007), to our knowledge only one study has examined whether specific EI dimensions act as moderators. Specifically, Jung and collaborators (2025) found that the dimension Others’ Emotion Appraisal moderated the relation between shyness and sociability among young women, but not men. Given this singular finding, we examined the possibility of sex-specific dimensional effects, although our tests of these effects were exploratory.
Method
Participants
Participants were 160 adults between the ages of 17 and 75 (Mage = 39.50 years, SD = 13.65, 28.1% male) who were outpatients recruited from the Anxiety Treatment and Research Clinic (ATRC) at St. Joseph's Healthcare Hamilton, Ontario. Self-reported ethnicity of the sample was 90.7% White, 3.7% Black, 2.8% Asian, 0.9% Latino, 0.9% Middle Eastern, and the remaining 1.0% of the participants did not identify their ethnicity. Participants’ educational levels were reported as follows: 51.8% completed university/college, 15.8% completed some university/college, 15.8% completed high school, 7.9% completed postgraduate studies, 4.4 % completed some high school, and 4.3% completed some postgraduate studies. Diagnosis of an anxiety disorder was determined by qualified clinicians. Diagnostic profiles comprised 58.8% individuals diagnosed with GAD only, 15.6% diagnosed with SAD only, and 25.6% diagnosed with comorbid GAD and SAD. As a result, participants were treated as a heterogeneous anxiety-disordered sample rather than as an anxiety-diagnosis-specific subgroup, with no exclusions based on GAD, SAD, or comorbid GAD + SAD status.
Procedures
This study was conducted as part of a larger research program evaluating the effectiveness and quality of the cognitive-behavioral treatment (CBT) program at the ATRC. Researchers collected data from participants before attending a CBT program run by the [ATRC] at St. Joseph's Healthcare Hamilton. Participants of the program were outpatients who met the following diagnostic criteria listed in the Diagnostic and Statistical Manual of Mental Disorders (DSM-5): GAD and/or SAD. The participants completed extensive questionnaires before group treatment began but only measures pertaining to shyness, sociability, EI, social anxiety, and anxiety were of interest to this study. Before taking part in the study, all participants were briefed about the study procedures and signed a consent form. Research ethics approval for the study protocol was granted by the Hamilton Integrated Research Ethics Board.
In the larger research program, participants received a group-based CBT intervention to reduce anxiety symptoms and enhance emotion regulation, coping efficacy, and confidence in managing anxiety-provoking situations. Consistent with established CBT frameworks, the intervention addressed cognitive, behavioral, and physiological components of anxiety through techniques such as cognitive restructuring, relaxation training, and graduated exposure. These strategies were implemented to reduce avoidance behavior, challenge maladaptive cognitions, and foster more adaptive emotional and behavioral responses across anxiety-eliciting contexts.
Measures
Shyness and Sociability
These two constructs were measured by (a) the five highest-loaded items of the Shyness Scale (see Bruch et al., 1989), and (b) five items from the Sociability Scale, which are part of the original Cheek and Buss Shyness and Sociability Scales (Cheek, 1983; See S4 Shyness and Sociability Scale, for an example item). The items were rated on a 5-point scale, ranging from 0 = not at all to 4 = extremely. The α internal consistency was .90 for shyness and .86 for sociability.
Emotional Intelligence
Overview of the Four Dimensions Comprising Wong and Law Emotional Intelligence Scale (WLEIS)
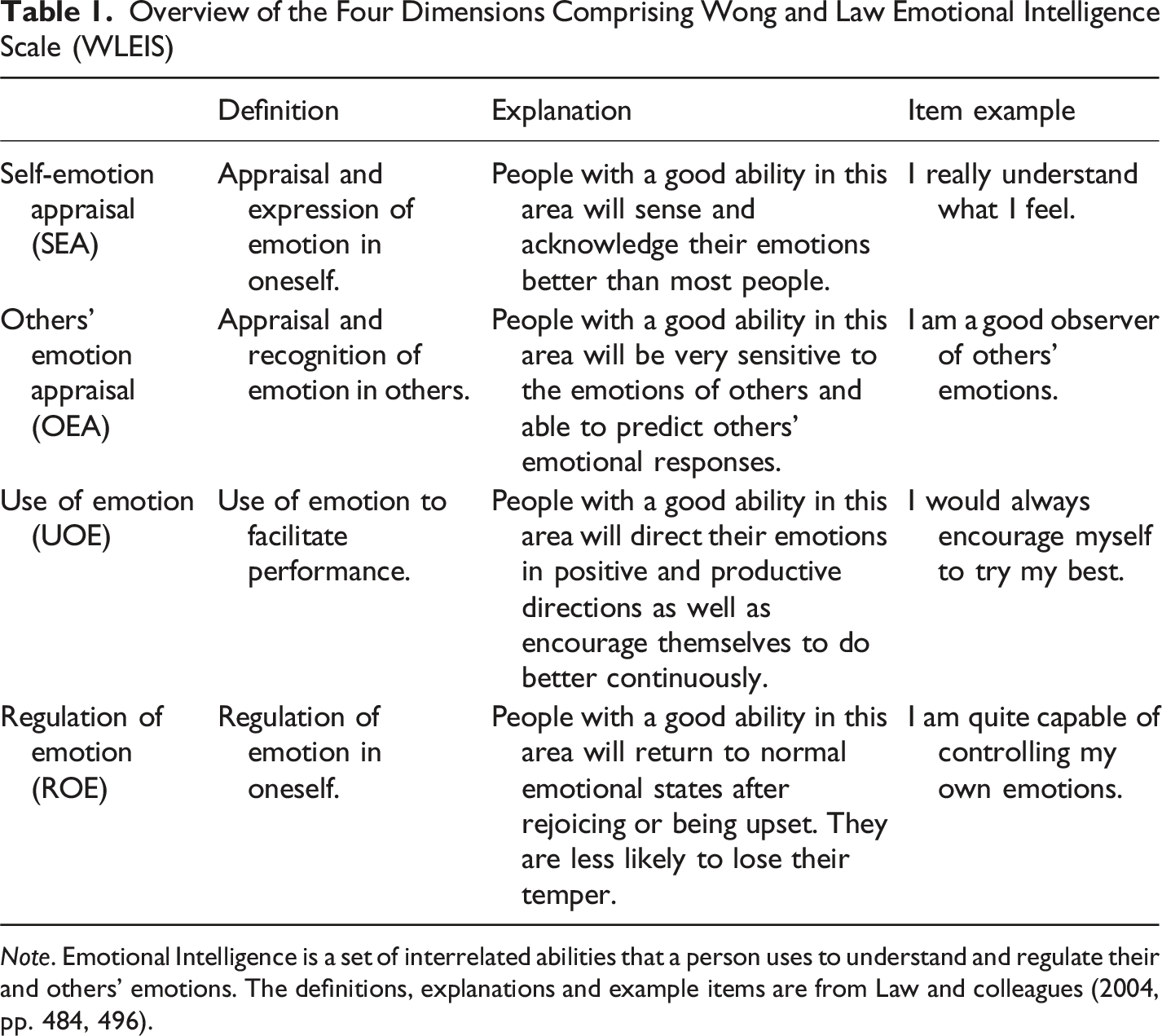
Note. Emotional Intelligence is a set of interrelated abilities that a person uses to understand and regulate their and others’ emotions. The definitions, explanations and example items are from Law and colleagues (2004, pp. 484, 496).
Internalizing Behaviors
The measure of internalizing behaviors was created by combining the Social Phobia Inventory (SPIN, Connor et al., 2000) and Depression Anxiety Stress Scale-21 (DASS-21, Lovibond & Lovibond, 1995a, 1995b) into a composite measure. The SPIN was a 17-item self-report measure in which items were rated on a 5-point scale, ranging from 0 = not at all to 4 = extremely, with higher scores indicating higher levels of social anxiety (See S5 SPIN for an example item). The DASS-21 is a 21-item self-report measure of depression, anxiety, and stress. The items were rated on a 4-point scale, ranging from 0 = did not apply to me at all to 3 = applied to me very much or most of the time, with higher scores indicating higher levels of negative emotional symptoms related to depression, anxiety, and stress. (see S6 DASS-21 for an example item). Although the DASS-21 and SPIN capture different emotional processes, general negative affect versus social fear and avoidance, this allowed us to assess a broader spectrum of internalizing behaviors. In fact, both measures together assessed the key symptoms of internalizing behaviors, historically characterized by sorrow, guilt, fear, and worry (Zahn-Waxler et al., 2000). Accordingly, the two measures were aggregated to create a composite score of internalizing behaviors. In our sample, the correlation between the SPIN and DASS-21 was r = .51, p < .01, indicating related but distinct constructs, and both scales had good internal consistency, with α values of .93. After standardizing the SPIN and DASS-21 scales (z-scores), the resulting composite demonstrated excellent internal consistency of .94.
Data Analyses
All analyses were performed using Model 1 of the Hayes PROCESS Macro, Version 4.2 for SPSS 30.0 (Hayes, 2022). We used multiple linear regressions to examine whether EI and its subscales moderated the relation between (a) shyness and sociability (i.e., approach-related behaviors) and (b) shyness and internalizing behaviors (i.e., avoidance-related behaviors). Thus, five different moderators were studied, including the EI mean and the four EI subscales of SEA, OEA, UOE and ROE. The covariates of age and sex were also entered into the analyses, as previous work indicated there might be age- and sex-related differences in EI (Kong, 2017). Pairwise correlations among the independent variables were examined to assess potential multicollinearity. All study variables, except for sex, were standardized (z-scored) to improve the interpretability of regression coefficients and reduce any potential impact of multicollinearity.
Results
Descriptive Statistics
Descriptive Statistics and Correlations for Study Variables (N = 160)
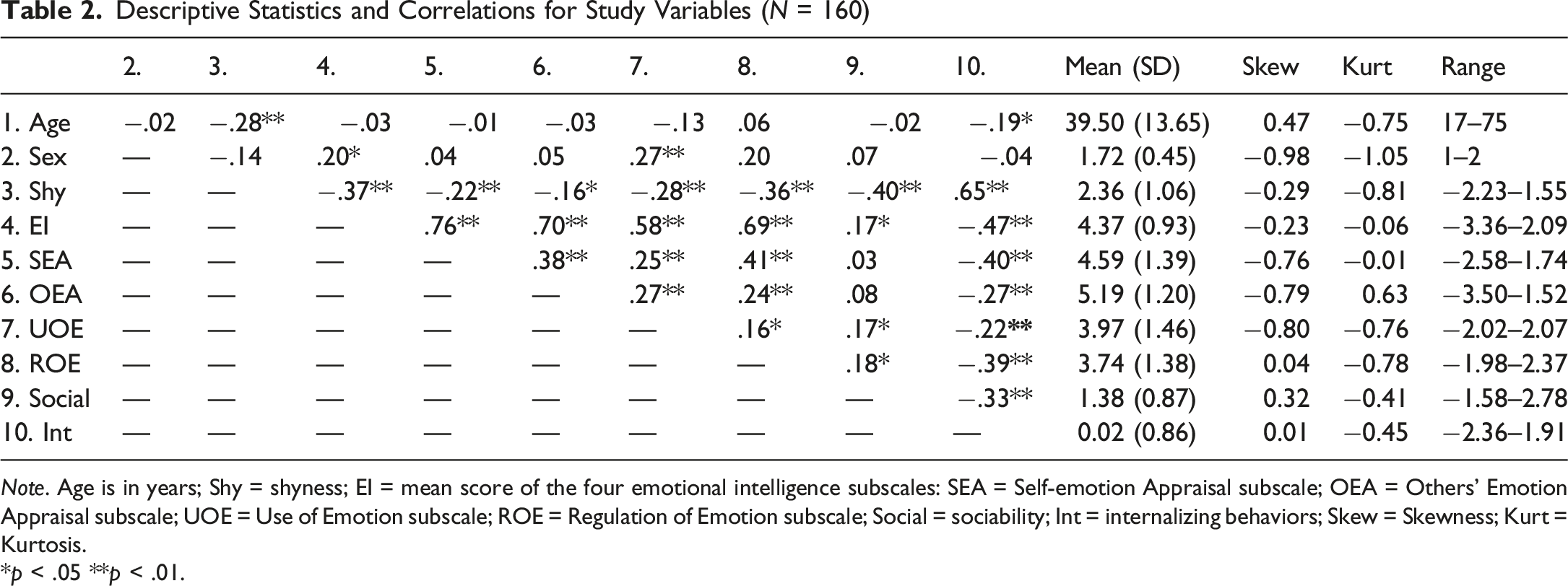
Note. Age is in years; Shy = shyness; EI = mean score of the four emotional intelligence subscales: SEA = Self-emotion Appraisal subscale; OEA = Others’ Emotion Appraisal subscale; UOE = Use of Emotion subscale; ROE = Regulation of Emotion subscale; Social = sociability; Int = internalizing behaviors; Skew = Skewness; Kurt = Kurtosis.
*p < .05 **p < .01.
Regression Analyses
Approach-Related Behaviors
Total Sample
Summary of the Moderation Models With Significant Interaction Effects: By Total Sample (N = 160), Women (n = 115) and Men (n = 45)
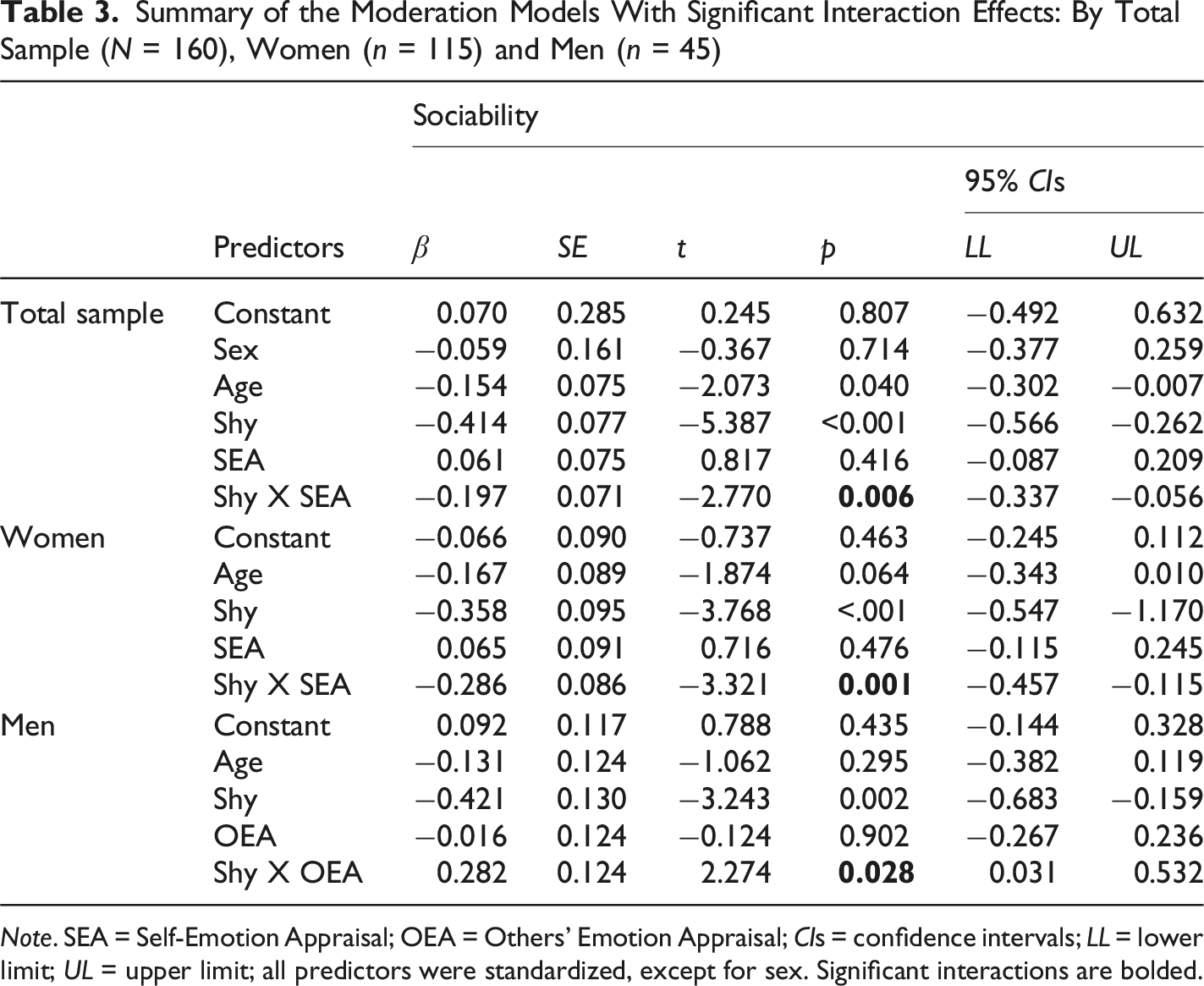
Note. SEA = Self-Emotion Appraisal; OEA = Others’ Emotion Appraisal; CIs = confidence intervals; LL = lower limit; UL = upper limit; all predictors were standardized, except for sex. Significant interactions are bolded.
Summary of the Significant Conditional Effects of Emotional Intelligence on the Relation Between Shyness and Sociability: By Total Sample (N = 160), Women (n = 115) and Men (n = 45)
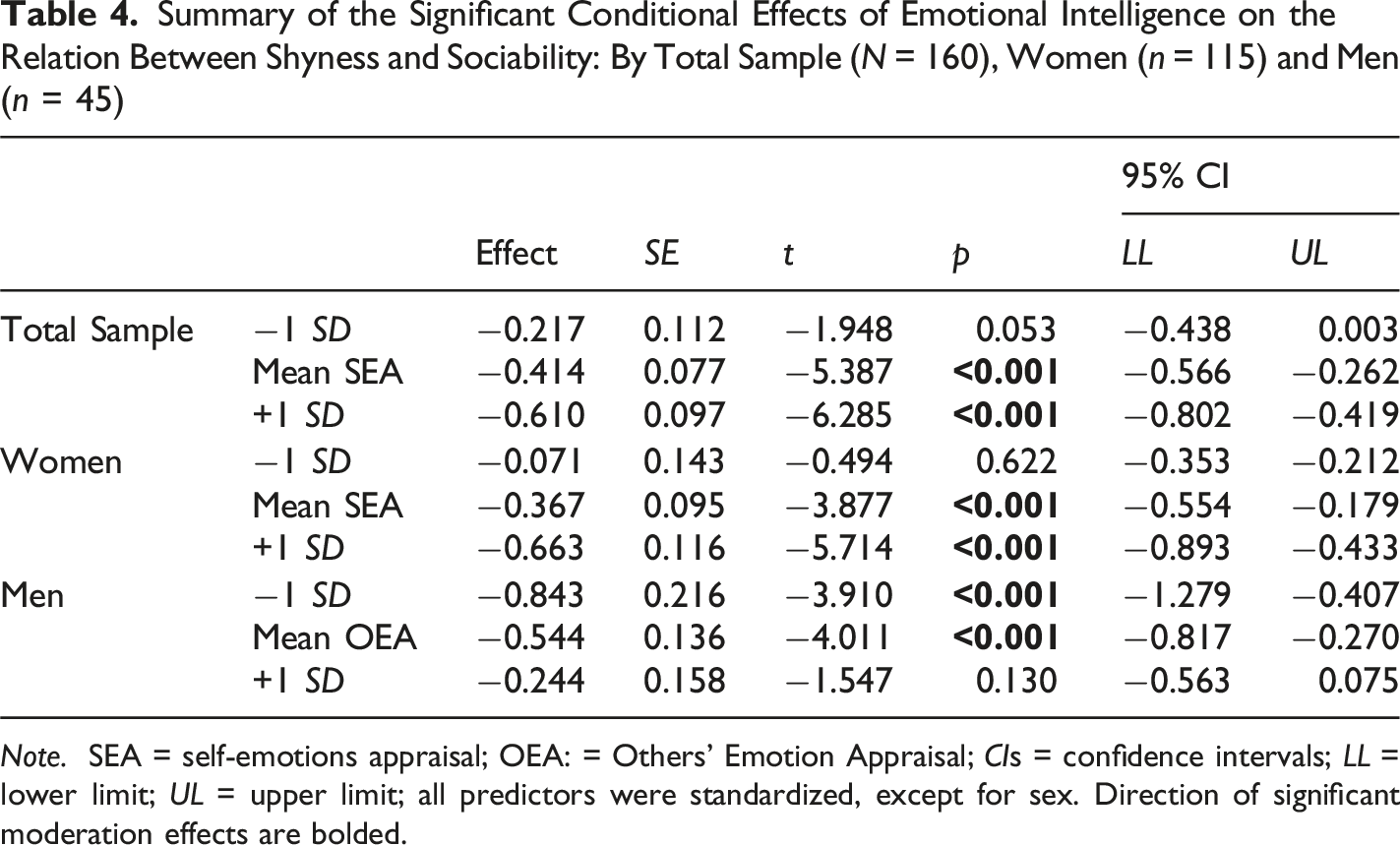
Note. SEA = self-emotions appraisal; OEA: = Others’ Emotion Appraisal; CIs = confidence intervals; LL = lower limit; UL = upper limit; all predictors were standardized, except for sex. Direction of significant moderation effects are bolded.
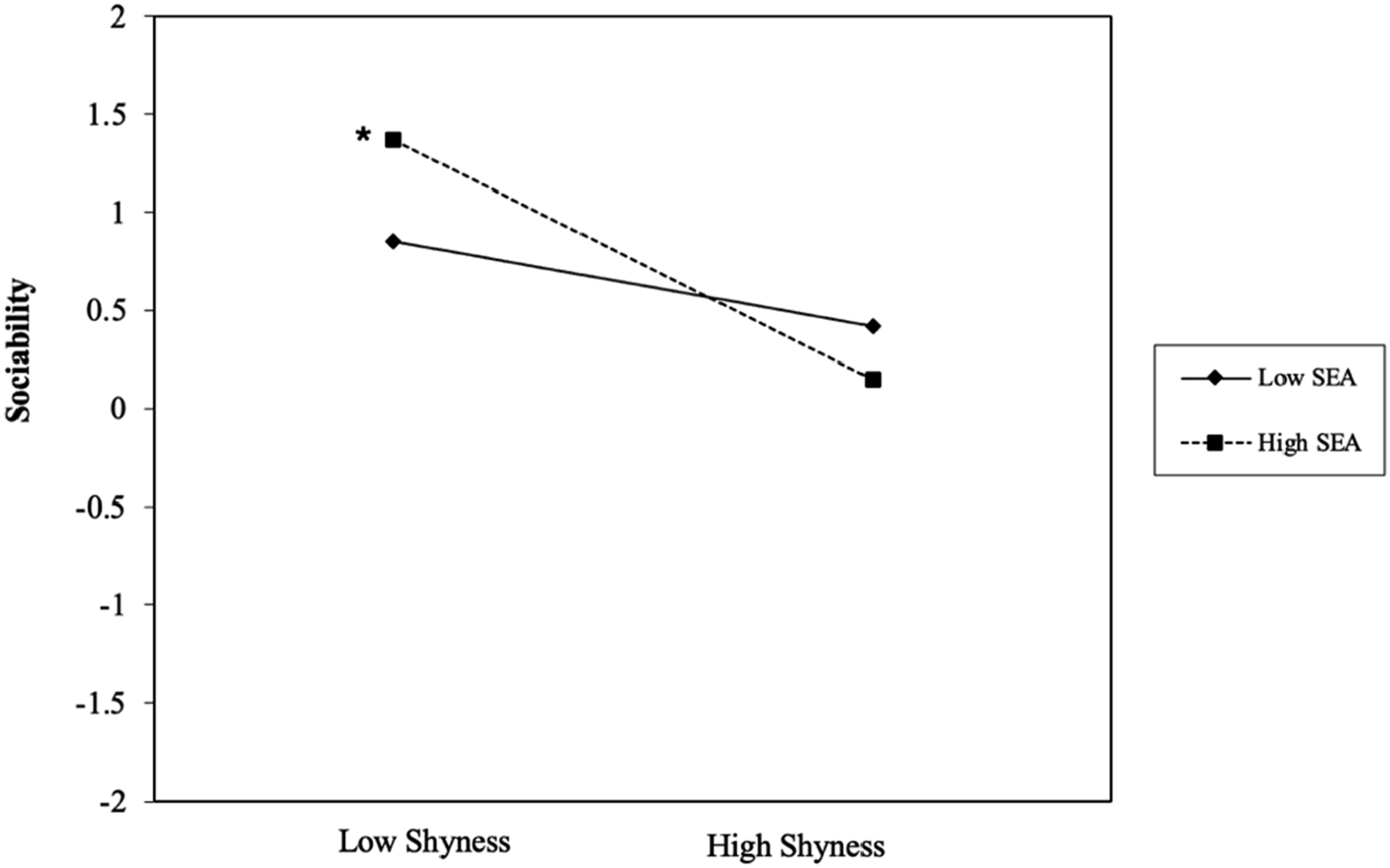
The moderating role of self-emotion appraisal (SEA) on the relation between shyness and sociability in the total sample (N = 160)
Women
Out of the five models, only the model with SEA as the moderator had a significant interaction effect. Altogether, the predictors explained 23.58% of the variance of sociability, R2 = 0.236, F (4, 110) = 8.49, p < .001. The interaction term involving SEA accounted for 7.66% of the variance in sociability (see Tables 3 and 4). Cohen’s local effect size f2 was 0.10, indicating a small to medium sized effect (Selya et al., 2012). A simple slope analysis indicated that women with low shyness had higher levels of sociability than women with high shyness, but the women with high shyness reported the highest average sociability scores with lower versus higher levels of SEA. (See Figure 2). The moderating role of self- emotion appraisal (SEA) on the relation between shyness and sociability in women (n = 115)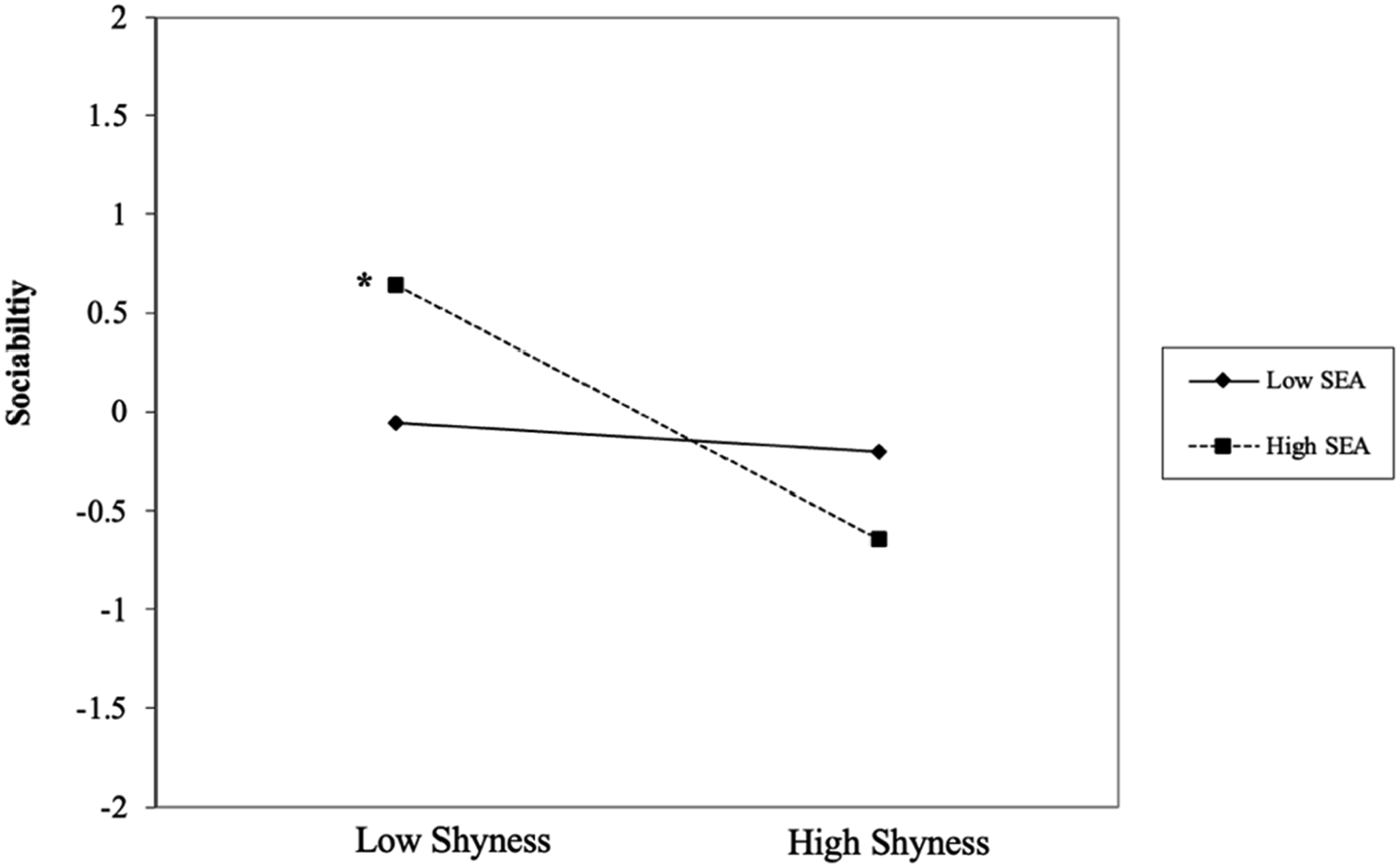
Men
Among the five models, only the model with OEA as the moderator had a significant interaction effect (Figure 3). The predictors together accounted for 36.92% of the variance in sociability, F (4, 40) = 5.85, p < .001. The interaction term alone accounted for 8.16% of the variance in sociability. Cohen’s local effect size f2 was 0.13, indicating a medium sized effect (Selya et al., 2012). A simple slope analysis showed that men with low shyness had higher levels of sociability than men with high shyness in general, but men with high shyness had the highest levels of sociability at higher versus lower levels of OEA. The Moderating role of others’ emotion appraisal (OEA) on the Relation between shyness and sociability in men (n = 45)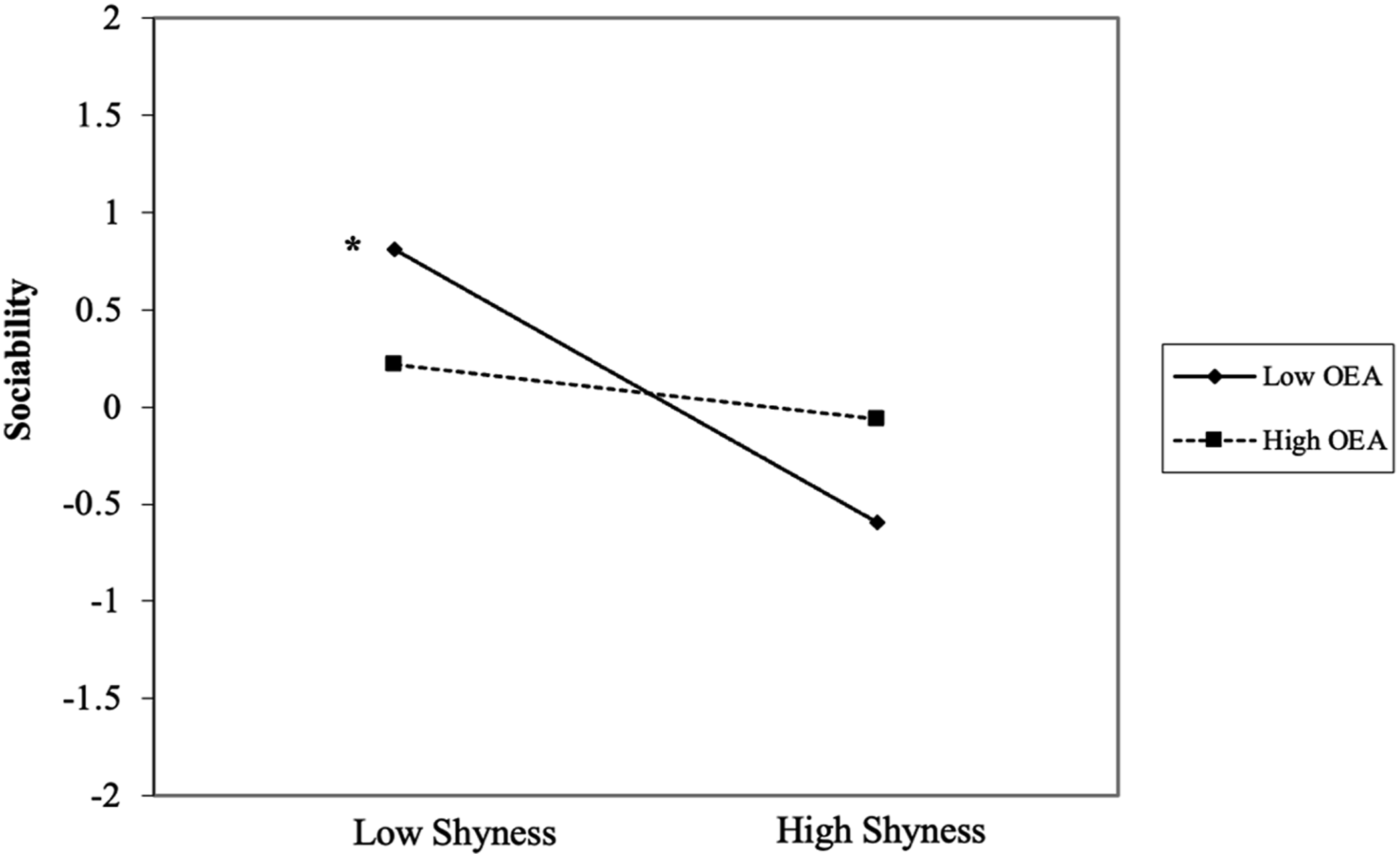
Avoidance-Related Behaviors
We conducted five separate moderation analyses to examine whether internalizing behaviors were predicted by shyness as moderated by each of the five EI moderators (i.e., EI mean, SEA, OEA, UOE, ROE). These five analyses were performed using the total sample as well as separately by sex. However, none of the interaction terms were significant within each of these models (see Table S3 for a subset of non-significant results). We infer from these results that in a clinical sample, the EI mean and its dimensions individually had no effect on the positive relation between shyness and internalizing-related behaviors.
Discussion
In a sample of adults clinically diagnosed with anxiety prior to undergoing cognitive behavioral therapy, we investigated whether individuals with higher EI, compared to those with lower levels, engaged in more approach-related behaviors and/or reduced avoidance-related behaviors. Our findings indicated that high shy women reported higher levels of social behavior when they had lower versus higher levels of Self-emotional Appraisal (SEA). This was also true for the total sample, but as our participants were predominantly women (∼72%), we presumed the results were mostly representative of shy females, and less so of shy men. In high shy men, higher levels of sociability were associated with higher versus lower levels of Others’ Emotion Appraisal (OEA). Last, we found no evidence to support EI, or any of its dimensions, as a beneficial skill for those with clinically diagnosed internalizing-related behaviors. These results are only partially in line with our hypotheses.
Approach-Related Behaviors
Shy Women and Emotional Intelligence
Contrary to our expectations, higher levels of SEA did not benefit high shy women. Instead, lower levels of SEA seemed to be more effective in promoting social behavior. One potential explanation for this may be that high shy women are particularly sensitive and attentive to their social discomfort, which may inhibit clear thinking and hinder meaningful participation in social interactions. It is possible that, within a clinical sample, a stream of negative, self-directed thoughts may recur persistently, disrupting an individual’s ability to respond appropriately in social situations (Leung et al., 2022; Makkar & Grisham, 2011). Alternatively, one might consider that if high shy women are less attuned to their feelings, they may be less aware of their emotional distress. This diminished awareness might, paradoxically, lend shy women some self-assurance, allowing them the means to better navigate social environments. Nonetheless, being aware of one’s own emotional state does not appear beneficial for high shy women in navigating interpersonal interactions. Given that women have a greater tendency to ruminate than men in response to anxiety, they likely need targeted strategies to better regulate their emotional state and redirect their focus away from negative thought patterns, especially when socializing (Johnson & Whisman, 2013; Nolen-Hoeksema, 2012). Last, it is also worth noting that the clinical characteristics of this sample may have masked the beneficial effects typically associated with relatively higher levels of EI. Accordingly, the present findings should be interpreted cautiously, as they remain preliminary and require replication in independent clinical samples before conclusions can be drawn.
Shy Men and Emotional Intelligence
Generally consistent with our hypothesis, higher levels of OEA as compared to lower levels were particularly advantageous for high shy men who exhibited higher levels of sociability. Research suggests that men’s ability to recognize others’ emotions is influenced by personal relevance, such that their accuracy in reading others’ emotions may improve in personally meaningful relationships but diminish in unfamiliar social and less personally significant social contexts (Stinson & Ickes, 1992). Among shy men, difficulties in accurately recognizing others’ emotions may be exacerbated by attentional bias. This was demonstrated during attentional tasks, in which anxious male participants had difficulty redirecting their attention from social threat stimuli compared to females (Zhang et al., 2017). Furthermore, accumulation of negative social experiences may undermine their confidence in social interactions and limit their opportunity for meaningful social connections (Kurtoğlu et al., 2024). As a result, some high shy men may feel awkward in face-to-face circumstances and display avoidant behaviors in socially demanding environments. Consequently, lower levels of OEA among shy men may increase the risk of impaired social engagement and increased emotional distress, especially in unfamiliar social situations (Doey et al., 2014). From a clinical perspective, enhancing awareness and responsiveness to others’ emotions may serve as a protective factor against social distress and facilitate more adaptive social functioning in high shy men (Teal et al., 2019).
Sex-Based Approaches to Clinical Interventions
Evidence-based interventions, such as CBT, have been shown to effectively promote approach-related behaviors by increasing interpersonal functioning and improving emotional regulation (Bomyea et al., 2020; Etkin et al., 2023). For shy individuals, these interventions offer structured opportunities to develop social competence through techniques such as gradual exposure to feared social situations and cognitive restructuring of maladaptive beliefs (Heimberg, 2002). Shifting away from heightened emotional self-appraisal (i.e., SEA) may foster social behaviors in high shy women. In addition, evidence-based therapeutic approaches that incorporate exercise and targeted meditation training may be particularly effective in reducing distress stemming from increased self-awareness and encouraging self-compassion, especially in shy women (Rojiani et al., 2017; Saeed et al., 2019). By contrast, low interpersonal emotional awareness (i.e., OEA) may act as a barrier to social functioning among high shy men. When men struggle to identify and interpret others’ emotional cues, interventions that rely on emotional processing may be less effective. Instead, combining repeated exposure to social situations with structured feedback and a skills-based approach may improve emotional recognition accuracy and promote greater attentional focus on others (Schneier & Goldmark, 2015). Incorporating these sex-based differences through clinical interventions may facilitate the development of more nuanced and targeted approaches for fostering sociability.
Nonetheless, we should note our observed sex differences reflect group-level patterns rather than fixed individual characteristics, with substantial variability within each sex. Thus, several ethical and practical considerations warrant careful attention. From an ethical perspective, interpreting average sex differences without sufficient caution may risk reinforcing essentialist assumptions, obscuring within-group heterogeneity, and neglecting gender diversity and individual identities. From a practical standpoint, overreliance on sex-based guidance may undermine individualized clinical assessment and intervention planning. Moreover, applying sex-informed approaches without careful consideration of developmental, contextual, and clinical factors may reduce treatment effectiveness. Consequently, our findings support a nuanced understanding of sex differences that promote flexible, person-centered treatment approaches rather than uniform sex-based interventions.
Avoidance-Related Behaviors
Contrary to our initial hypothesis, we found no interaction effects on the relation between shyness and internalizing-related behaviors by EI or by any one of its four dimensions in our clinical sample. This result was consistent with the findings of Jung et al. (2025), who reported that EI did not mitigate the effects of internalizing behaviors on socializing behaviors in a sample of nonclinical shy young adults (17–24 years of age). We propose that these comparable findings across different types of populations (i.e., clinical and nonclinical) may be attributable to at least two factors. First, the correlation between shyness and internalizing behaviors in both studies was strong (rclinical = 0.65 in the present study, r nonclincial = 0.67 in Jung et al., 2025), indicating that a substantial amount of the variance was already explained (42% and 46%, respectively, in each of the studies). This, in turn, limited the amount of variance in which to detect any moderation effect. Second, if the two constructs were functionally or conceptually alike, then a moderation effect may not be theoretically meaningful. We, therefore, suspect that the statistical challenge in finding an interaction effect was due to the relatively strong correlation between shyness and internalizing behaviors, especially as the internalizing construct was for the most part narrowly defined by anxiety symptoms, which are closely linked to shyness (Blöte et al., 2019). Collectively, the absence of moderation effects for internalizing behaviors may reflect both conceptual overlap between shyness and anxiety and methodological constraints. These findings warrant cautious interpretation and highlight the importance for future studies to replicate and extend this work across diverse populations.
Strengths, Limitations, and Future Directions
There are several strengths of this study. First, to our knowledge, no other research has investigated EI as a potential moderator of the relation between shyness and sociability/internalizing behaviors, respectively, in clinical samples characterized by anxiety. As EI is a relatively new construct, its role in individuals with clinical disorders is underexplored. Nonetheless, although EI is generally thought to play a vital role in healthy relationships and promote overall well-being (Antonopoulou, 2024), our findings on sex-specific effects suggest that a more nuanced understanding of its influence is needed. Specifically, higher levels of EI (i.e., SEA) were not only disadvantageous for shy women in social contexts but may also act as a deterrent to social engagement. Second, we found sex-based differences in the role of EI. While women did not benefit socially from a greater self-awareness, shy men were more sociable if they demonstrated a strong ability to understand others’ emotions. Not only did the direction of EI effects differ by sex, but so too did the component of emotion and its influence on the relation between shyness and social behavior. It suggests that any investigation into EI should consider all four dimensions separately, and sex differences, in both clinical and nonclinical samples.
The current study also had several limitations. First, the presence of comorbid disorders limited our capacity to isolate the effects of GAD and SAD. This is noteworthy because comorbid conditions may contribute substantially to the severity of anxiety symptoms (Newman et al., 1998). Accordingly, future studies would benefit from the systematic assessment of diagnostic profiles to support comorbidity-informed grouping and disorder-specific analyses. Second, information regarding participants’ prior psychological or pharmacological treatments was not collected. Consequently, we cannot rule out the possibility that previous therapy or medication use may have influenced participants’ levels of emotional intelligence or shyness. Future research should consider assessing treatment history to better understand its impact on these study variables. Third, the current study included participants from a wide age range, which may have introduced developmental variability (e.g., psychological, cognitive, behavioral) into the relations among study variables. Although we statistically controlled for age, future studies may benefit from examining a more age restricted clinical sample to reduce potential developmental confounds. Fourth, SES and ethnicity were not included as covariates, as achieving diversity in our sample proved particularly challenging during COVID-19. This limitation may have introduced sampling bias and reduced generalizability, as most participants self-identified as White. Subsequent studies should incorporate a more demographically diverse sample to strengthen external validity. Fifth, our findings were based entirely on self-report. Unlike behavioral measures, self-reports rely on participants’ personal perceptions, which often lead to subjective response biases. Obtaining objective data such as through observational measures, experimental tasks, or other complementary measures (e.g., social skills, leadership skills, and workplace performance) would, (a) reduce single method bias, (b) better reflect the complexity of the construct, and (c) improve reliability through converging evidence (e.g., Gómez-Leal et al., 2021). Sixth, although the DASS-21 and SPIN assessed somewhat distinct yet overlapping emotional processes, general negative emotional distress versus social fear and avoidance, their aggregation was intended as a theory-driven approach to capturing a broader spectrum of internalizing behaviors, including distress-, fear-, and self-evaluative emotional process. Nonetheless, combining these measures into a single composite may have masked differential aspects of EI interacting with social anxiety-related versus broader negative affect-related internalizing problems. Accordingly, future research should examine these measures both jointly and separately to clarify whether EI moderation effects differ across anxiety-specific versus broader general negative affect clinical populations. Finally, the male models were underpowered at .71, increasing the probability of failing to detect a real effect. Given the reduced power, results for our male subsample should be viewed as preliminary and interpreted with appropriate caution. Future research should address this limitation by recruiting larger clinical samples and employing alternative research designs, such as person-centered or longitudinal approaches. These methods may be particularly well suited for examining EI across the lifespan, where both stability and change can be examined (Laursen & Hoff, 2006; Parker et al., 2021).
Further investigations are needed to examine EI’s role across different clinical populations, perhaps first focusing on mood disorders as previous studies have reported a well-documented negative correlation between EI and depression (Sergi et al., 2021). Given emerging evidence linking EI to mental health outcomes, prioritizing clinical samples may be especially informative and could support the development and evaluation of targeted EI-based interventions (Zoromba et al., 2023). Ultimately, clinical trials may demonstrate the practicality of incorporating EI training in treatment programs with the purpose of altering negative emotional patterns and promoting more adaptive emotional functioning.
Conclusions
Our results suggested that the effects of EI and its dimensions on mental health are nuanced and likely multifaceted. For instance, only in shy women did we find that higher levels of self-focused emotions (i.e., heightened feelings of anxiety or embarrassment) hindered social interactions, which is consistent with research that reported women tend to internalize emotional distress (Chaplin, 2015). In comparison, shy men with lower levels of appraising others’ emotions were disadvantaged in social contexts, in line with the viewpoint that men relate through shared activities rather than emotional intimacy (Baumeister & Leary, 1995). Taken together, these findings suggest that distinct components of EI may influence social functioning through different mechanisms for women and men. Thus, pulling apart how EI and its component parts work within clinical populations will require more finely tuned research that considers both sex differences and the multidimensional nature of EI. Such research may be valuable for clinicians seeking to improve social-emotional awareness in individuals with internalizing and/or externalizing disorders.
Supplemental Material
Supplemental Material - Shyness Associations With Approach/Avoidance-Related Behaviors in Clinically Anxious Adults in Canada: The Moderating Role of Emotional Intelligence Differs for Women and Men
Supplemental Material for Shyness Associations With Approach/Avoidance-Related Behaviors in Clinically Anxious Adults in Canada: The Moderating Role of Emotional Intelligence Differs for Women and Men by Soyoung Jung, Christina A. Brook, Karen Rowa,Louis A. Schmidt in Psychological Reports
Footnotes
Acknowledgement
The authors gratefully acknowledge funding support from the Social Sciences and Humanities Research Council of Canada. We also wish to thank the patient population for their participation and the clinical staff at the ATRC for their assistance with data collection.
Ethical Considerations
Hamilton Integrated Research Ethics Board approved the study protocol of this research.
Consent to Participate
Written informed consent was obtained from all participants prior to data collection.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by an operating grant from the Social Sciences and Humanities Research Council of Canada awarded to LAS (Grant number 435-2017-1010).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data are available upon reasonable request.
Supplemental Material
Supplemental Material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.