
Abstract
Type D personality, characterized by increased levels of both negative affectivity and social inhibition has been consistently associated with poor psychological wellbeing, with perceived stress and diminished social support often posited as imperative mediating pathways. The current study aimed to (1) examine the association between Type D personality and disordered eating symptomology, (2) identify the potential sequential mediating pathways through social support and perceived stress that may underlie the link between Type D personality and disordered eating, and (3) identify if Type D personality has predictive utility in analyses adjusting for Type D subcomponents (negative affect and social inhibition). A sample of 761 participants (Mage = 19.17, SD = 2.68, ages 18–52) completed measures assessing Type D personality (DS14), social support (ISEL), perceived stress (PSS) and symptoms of disordered eating (EDE-QS). Our findings revealed that Type D personality was associated with increased disordered eating symptomology, and this association was serially mediated through diminished social support and greater perceived stress. Here, Type D personality was associated with reduced social support, which in turn, predicted greater levels of perceived stress, leading to increased disordered eating symptoms. However, after adjusting for the main effects of negative affect and social inhibition, the main effects for Type D personality became non-significant. While these findings suggest potential pathways linking Type D personality to disordered eating, the effects are primarily driven by the social inhibition and negative affect subcomponents.
Introduction
Individual Differences and Disordered Eating
Eating disorders refer to a cluster of psychiatric disorders which are typically characterized by distinctive symptoms related to maladaptive eating behaviors and atypical body weight (Schmidt et al., 2016). Prior research has estimated that the lifetime prevalence for eating disorders are 2.2% for men and 8.4% for women (Galmiche et al., 2019). The prevalence of disordered eating in younger adults, such as amongst university students, has been noted to be particularly high, with approximately 20% of college students classified as having an eating disorder (Alhaj et al., 2022). Moreover, the prevalence rates of eating disorders have been found to have increased significantly amongst college students in recent years (Daly & Costigan, 2022). Consequently, eating disorders have been noted to constitute a substantial economic burden, with an estimated economic cost of $64.7 billion annually in USA alone (Streatfeild et al., 2021).
One line of research has aimed to identify the role of individual differences in eating disorder symptomology. In particular, traits encapsulating facets of negative affectivity such as neuroticism, trait anxiety, anger and poor self-esteem have been consistently associated with greater eating disorder symptomology (Davis & Fischer, 2013; Gilmartin et al., 2022; Koposov et al., 2023; Shea & Pritchard, 2007). More recent evidence suggests that not only the experience of negative emotions (i.e., negative affectivity), but the simultaneous suppression of these emotions (i.e., social inhibition), may be particularly detrimental for physical and mental health outcomes (Mols & Denollet, 2010). The joint tendency to experience an array of negative emotions, and simultaneously inhibit the expression of these emotions, is referred to as Type D personality (i.e., Distress personality) (Denollet, 2005). While Type D was initially proposed as an independent predictor of adverse health outcomes in cardiac patients (Denollet et al., 1996), more recent evidence has linked Type D personality to a myriad of mental health outcomes such as poor self-esteem (Huis et al., 2011), depression (Gupta & Basak, 2013), and anxiety (Howard & Hughes, 2012). However, while Type D individuals have been noted to report greater dissatisfaction with their physical appearance, increased preoccupation with being overweight, and are more likely to self-rate themselves as overweight (Borkoles et al., 2010), no study to date has examined the association between Type D personality and disordered eating.
Type D Personality and Social Support
Given their socially inhibited nature, Type D individuals are posited to feel tense and insecure in the presence of others (Denollet, 2005; Gest, 1997), and tend to avoid social situations due to their perceived danger (Asendorpf, 1993; Denollet, 2000), as well as their increased vulnerability to social-evaluative threats (Denollet, 2012). In fact, prior evidence suggests that Type D individuals possess a cognitive bias of interpersonal interpretation (Grynberg et al., 2012; Howard et al., 2018), whereby they perceive negativity from others during social interactions (O'Riordan, Howard, Brown, & Gallagher, 2020; O'Riordan, Howard, & Gallagher, 2020). These biased perceptions of social interactions amongst Type D individuals have resulted in increased social anxiety symptomology (Timmermans et al., 2019), with Type D personality conferring a 9.1-fold increased odds of high social interaction anxiety and a 7.6-fold increased likelihood of social phobia (Kupper & Denollet, 2014). Thus, it is not surprising that Type D personality has been continually associated with diminished social support (Ginting et al., 2016; Polman et al., 2010; Sararoudi et al., 2011; Shao et al., 2017; Staniute et al., 2015; Williams et al., 2008). Importantly, the diminished social support experienced by Type D individuals has been linked to adverse physical and psychological health outcomes, such as greater physical symptoms (Williams & Wingate, 2012), increased psychological distress (Wang et al., 2025), poorer health rated quality of life (Staniute et al., 2015), and poorer self-care behaviors (Park et al., 2021). Thus, given the influence of social support on the development and exacerbation of disordered eating symptomatology (Kim et al., 2023; Stern et al., 2023), this lower social support may constitute a potential pathway linking Type D personality to disordered eating.
Type D Personality and Perceived Stress
Increased perceptions of, and reactions to, psychological stress have been propounded as a key mediating factor linking Type D personality to adverse physical and psychological health outcomes (Kupper & Denollet, 2007, 2018; Sher, 2005). In fact, several prior studies have consistently asserted that the relationship between Type D personality and adverse mental health outcomes may be facilitated via increased perceptions of everyday life stress, with numerous studies linking Type D personality to heightened perceptions of life stress (Allen et al., 2019b; O'Riordan, Howard, & Gallagher, 2020; Williams & Wingate, 2012), as well as abnormal psychophysiological responses to acute stress (O'Riordan, Gallagher, & Howard, 2023; O'Riordan, Howard, et al., 2023). Indeed, greater perceptions of stress have been noted to mediate the association between Type D personality and physical symptoms (Allen et al., 2019b; Smith et al., 2018). These prior findings which accentuate the association between Type D personality and perceptions of everyday life stress align with the transactional model of stress and coping, which propounds that individual differences, such as personality traits, influence the appraisal of, and response to, everyday life stressors (Lazarus, 1984). Moreover, prior research has consistently linked greater exposure to, and perception of, stress to the etiology, maintenance, and symptom severity of disordered eating (Beukes et al., 2010; Crowther & Chernyk, 1986; Hay & Williams, 2013; Hubert Lacey et al., 1986; Thurston et al., 2018). Thus, the heightened perception of stress consistently observed among Type D individuals may represent a key factor influencing disordered eating symptomatology.
Serial Mediation Effects of Social Support and Perceived Stress
While several studies have highlighted the mediating role of both diminished social support (Park et al., 2021; Staniute et al., 2015; Wang et al., 2025; Williams & Wingate, 2012) and perceived stress (Allen et al., 2019b; Smith et al., 2018), in the association between Type D personality and adverse physical and psychological health outcomes, these factors likely do not operate in isolation, but rather in a sequential fashion. In fact, it has been postulated that the increased self-reported stress frequently reported by Type D individuals may pertain to their socially inhibited nature (O'Riordan, Howard, Brown, & Gallagher, 2020). Supportive social relationships have been consistently posited as an effective stress coping response, promoting adaptive appraisals of external stressors (Thoits, 1995). According to the stress buffering hypothesis, greater perceptions of social support from others can enhance stress coping by providing individuals with the necessary emotional and tangible resources to deal with the demand of an imposed stressor, thereby attenuating and/or eliminating perceptions of stress (Cohen & Wills, 1985). In line with this assertation, others have indicated that the association between Type D personality and increased levels of perceived stress are mediated via poorer social relationship quality (O'Riordan, Howard, & Gallagher, 2020), and diminished levels of social support (Williams & Wingate, 2012). Thus, the heightened perceptions of stress reported by Type D individuals appear to be driven by reduced social support. Similarly, others have highlighted that the influence of reduced social support and increased perceptions of stress on disordered eating symptomatology also operates in a serial manner, with diminished social support promoting heightened perceptions of stress, which in turn predict greater disordered eating symptomology (Kwan & Gordon, 2016). Therefore, given that social support mediates the association between Type D personality and perceived stress (Williams & Wingate, 2012), and that perceived stress mediates the association between diminished social support and increased disordered eating symptomatology (Kwan & Gordon, 2016), the association between Type D personality and disordered eating symptoms may be serially mediated via reduced social support, which increases perceptions of stress and, in turn, promotes increased disordered eating symptomology.
The Independent Effect of Type D Personality, Negative Affect and Social Inhibition
Type D personality is posited to represent a synergistic interaction of negative affect and social inhibition, rather than an additive effect of both constructs combined (Kupper & Denollet, 2014; Lodder, 2020; Lodder et al., 2021). Here, it is suggested that social inhibition moderates the effects of negative affect on physical and psychological health outcomes, whereby the influence of negative affect is exacerbated amongst those who inhibit the expression of their negative emotions (Kupper & Denollet, 2007). Thus, Type D personality is suggested to represent the inhibition/suppression of negative emotions, and is propounded to predict outcomes in analyses adjusting for the main effects of social inhibition and negative affect (Smith, 2011). In order to test this predictive utility of Type D personality, recent evidence suggests that analyses should examine the effects of a continuous Type D interaction term based on the product of the negative affect and social inhibition subscales (NA × SI), and determine if this interaction term predicts health outcomes whilst controlling for the independent main effects of negative affect and social inhibition (See Lodder et al., 2021). However, while some research has corroborated the predictive utility of this Type D interaction term in analyses adjusting for the independent main effects of negative affect and social inhibition (Allen et al., 2019a, 2019b; Howard et al., 2011; O'Riordan, Howard, et al., 2023), others have reported null effects, suggesting that the effects observed for Type D are primarily driven by these individual subcomponents (Akram et al., 2018; O'Riordan, Howard, & Gallagher, 2020; Stevenson & Williams, 2014). In fact, a recent systematic review of the Type D literature indicated that approximately half of the effects reported for Type D in prior research are primarily driven by either negative affect or social inhibition alone, rather than the combined synergistic interaction between these traits (Lodder et al., 2021).
The Current Study
Thus, the current study extends prior research in several domains. Firstly, while prior research has linked negative affective variables (e.g., neuroticism, trait anxiety, anger and poor self-esteem) to greater eating disorder symptomology (Davis & Fischer, 2013; Gilmartin et al., 2022; Koposov et al., 2023; Shea & Pritchard, 2007), no study to date has examined the association between the inhibition of negative emotions (i.e., Type D personality) and disordered eating. Moreover, although diminished social support (Park et al., 2021; Staniute et al., 2015; Wang et al., 2025; Williams & Wingate, 2012) and perceived stress (Allen et al., 2019b; Smith et al., 2018), have both been noted to mediate the association between Type D personality and a range adverse outcomes, little research has examined how these mediating factors operate in a serial fashion to influence psychological well-being. Finally, more recent evidence suggests that many of the effects attributed to Type D personality may be primarily driven by its subcomponents, social inhibition and negative affectivity, rather than the synergistic interaction between the two traits (Lodder et al., 2021). This highlights the need for additional research to determine the predictive utility of Type D personality for social support, perceived stress, and psychological well-being, above and beyond the individual effects of negative affectivity and social inhibition. Accordingly, the current study aims to, (1) elucidate the role of the inhibition of negative emotions (i.e., Type D personality) in predicting disordered eating symptomology, (2) examine whether social support and perceived stress mediate this association in a serial fashion, and (3) determine whether Type D personality has predictive utility beyond its individual subcomponents, negative affectivity and social inhibition.
Materials and Methods
Participants
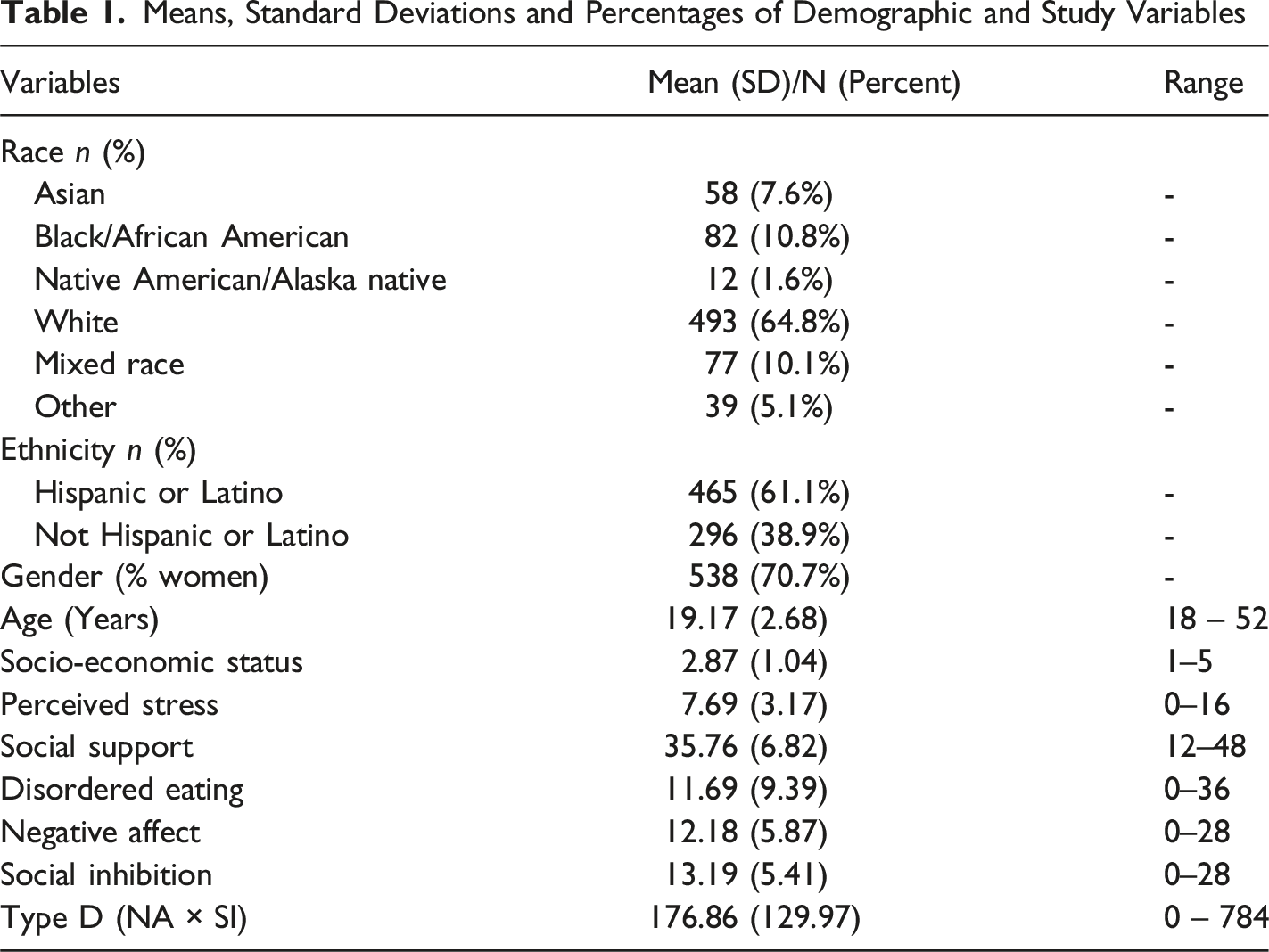
The current sample consisted of 761 undergraduate students, with a mean age of 19.17 (SD = 2.68). A total of 538 (70.7%) participants were women, 211 (27.7%) were men and 12 (1.6%) were non-binary/other. Participants were recruited to the current study using the University’s online research participation system (SONA). In exchange for completing the current study, students received one course credit. Prior to completing questionnaires, all participants provided written consent and were debriefed on completion of the study questionnaires. The study was approved by the Institutional Research Board at The University of Texas at San Antonio. Data was collected during the fall semester 2024. Only participants with complete study data were included in the current study. Furthermore, a G-power analysis indicated that a sample of N ≥550 was required to detect small effects (p = .05, f2 = 0.02) with a power of .80, indicating that the current sample was adequately powered.
Design
The currently study employed a correlational cross-sectional design. The predictor variables included negative affect, social inhibition and Type D personality, operationalized as a continuous interaction term based on the product of the individual subscales (NA × SI). Our outcome variable was eating disorder symptoms, and our mediating variables included self-reported social support and perceived stress.
Type D Personality
Type D personality was assessed using the DS14 Type D personality scale (Denollet, 2005). The DS14 is a 14-item scale. The social inhibition and negative affect subscales are both composed of 7 items each. Each item on the DS14 is scored on a 5-point Likert scale ranging for 0 (false) to 4 (true). Participants are required to rate the degree to which each statement describes themselves on this 5-point Likert scale. Examples of items measuring negative affect include “I often take a gloomy view of things” and “I am often down in the dumps”. Examples of items measuring social inhibition include: “I am a closed kind of person” and “I find it hard to start conversations”. Scores on the social inhibition and negative affect subscales can range from 0-28. Both subscales were found to have strong internal consistency, with a Cronbach’s α of .86 and .80, for the negative affect and social inhibition items, respectively. Traditional research has operationalized Type D as a categorical construct, with scores ≥10 on both subscales indicating Type D caseness (Denollet, 2005). However, this method has been criticized as it can inadvertently create lucky cuts that may yield spurious findings, and may also reduce the sensitivity of statistical tests (Coyne & de Voogd, 2012; Lodder, 2020; Smith, 2011). Consequently, recent evidence suggests that Type D personality is best represented as a continuous interterm using the negative affect and social inhibition subscales (Ferguson et al., 2009). In fact, this method is recommended when testing the synergistic effect of Type D personality, and it’s predictive utility above the main effects of negative affect and social inhibition (Lodder, 2020). Thus, we computed a continuous Type D interaction term (NA × SI), based on the product of negative affect and social inhibition scores.
Disordered Eating
Eating disorder symptoms were assessed using the Eating Disorder Examination Questionnaire-Short Version (EDE-QS) (Gideon et al., 2016). The EDE-QS is 12 item scale measuring symptoms of anorexia nervosa, bulimia nervosa and binge eating disorder. Participants responded on a 4-point scale range from 0 (0 days/Not at all) to 3 (6–7days/markedly), how often they had experienced each symptom over the past week. Scores range from 0–36, with higher scores indicating greater disordered eating severity. Example items include: “Have you tried to control your weight or shape by making yourself sick (vomit) or taking laxatives?” and “Have you had a sense of having lost control over your eating”. The EDE-QS has been shown to have strong internal consistency in samples of individuals with an eating disorder as well as in the general population (Gideon et al., 2016). In the current study, the EDE-QS also displayed strong internal consistency, with a Cronbach’s α of .92.
Perceived Stress Scale
Perceived stress was measured using the 4-item perceived stress scale (Cohen et al., 1983). Participants are required to respond on a 5-point Likert scale ranging from 0 (never) to 4 (very often), how often they felt a particular way over the past month. Example items include: “In the last month, how often have you felt difficulties were piling up so high that you could not overcome them?” and “In the last month, how often have you felt that you were unable to control the important things in your life?”. The scale had a Cronbach’s α of .74, indicating strong internal consistency.
Social Support
The 12-item Interpersonal Support Evaluation List was used to assess respondents’ perceived availability of three separate functions of social support, including appraisal, belonging, and tangible subscales (Cohen et al., 1985). Four items are used to measure each facet of social support. Participants are required to indicate how true each statement is about themselves on a 5-point Likert scale ranging from 1 (Definitely False) to 4 (Definitely True). Example items include: “There is someone I can turn to for advice about handling problems with my family” and “when I need suggestions on how to deal with a personal problem, I know someone I can turn to”. Items for each subscale are totaled to create a scale for each subscale, and a measure of total perceived availability of social support is computed as the sum of the three subscales. The social support scale displayed strong internal consistency with a Cronbach’s α of .83.
Data Analyses
Based on suggestions from prior research (Lodder, 2020), Type D personality was computed as the product of the negative affect and social inhibition subscales, representing a continuous interaction term (NA × SI). Correlational analyses were firstly conducted to examine the unadjusted associations between study variables. Subsequently, hierarchical multiple linear regression models were conducted to examine the association between Type D personality, perceived stress, social support and disordered eating after adjusting for potential confounding variables including age, gender, race, ethnicity and socio-economic status. Here, confounding variables were entered into models at Step 1 followed by the Type D interaction term at Step 2 (NA × SI). In order to examine the influence of the Type D subcomponents, and to identify if Type D personality had predictive utility in analyses adjusting for these individual subcomponents, follow-up regressions were conducted. Here, confounding variables were entered at Step 1, followed by negative affect and social inhibition at Step 2, and the Type D interaction term (NA × SI) at Step 3.
Mediation analyses were conducted to examine the potential serial mediating effects of Type D personality on disordered eating symptomology via social support and perceived stress. Model 6 of the PROCESS module for SPSS was used to test serial mediation. Type D was entered into models as the predictor variable, and disordered eating as the outcome variable. Social support was entered into models as mediator 1, and perceived stress as mediator 2. Potential confounding variables including age, gender, race, ethnicity and socio-economic status were entered as covariates. Follow-up mediation analyses were conducted with negative affect and social inhibition also entered into models as covariates, to examine if the indirect effects of Type D withstood adjustment for the individual subcomponents. Finally, in order to examine the potential independent effects of social inhibition and negative affect on disordered eating via social support and perceived stress, mediation analyses were conducted with negative affect and social inhibition entered into models in place of the Type D interaction term. Type D and the counterpart subcomponent were included in these models as covariates to determine the independent predictive utility of each facet.
Results
Descriptive Statistics
Means, Standard Deviations and Percentages of Demographic and Study Variables
Correlational Analyses Between Type D (NA × SI), Social Support, Perceived Stress and Disordered Eating
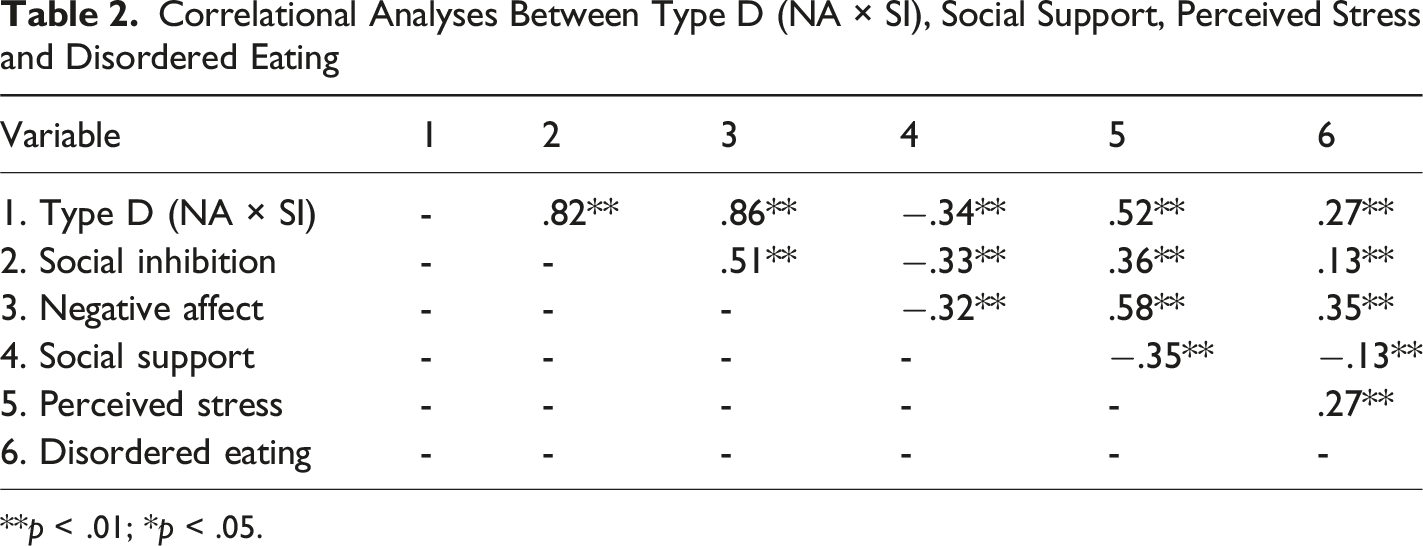
**p < .01; *p < .05.
Regression Analyses of the Associations Between Type D Personality, Social Support, and Perceived Stress
Regression Analyses for the Influence of Type D Personality, Negative Affect and Social Inhibition on Measures of Social Support, Perceived Stress and Disordered Eating
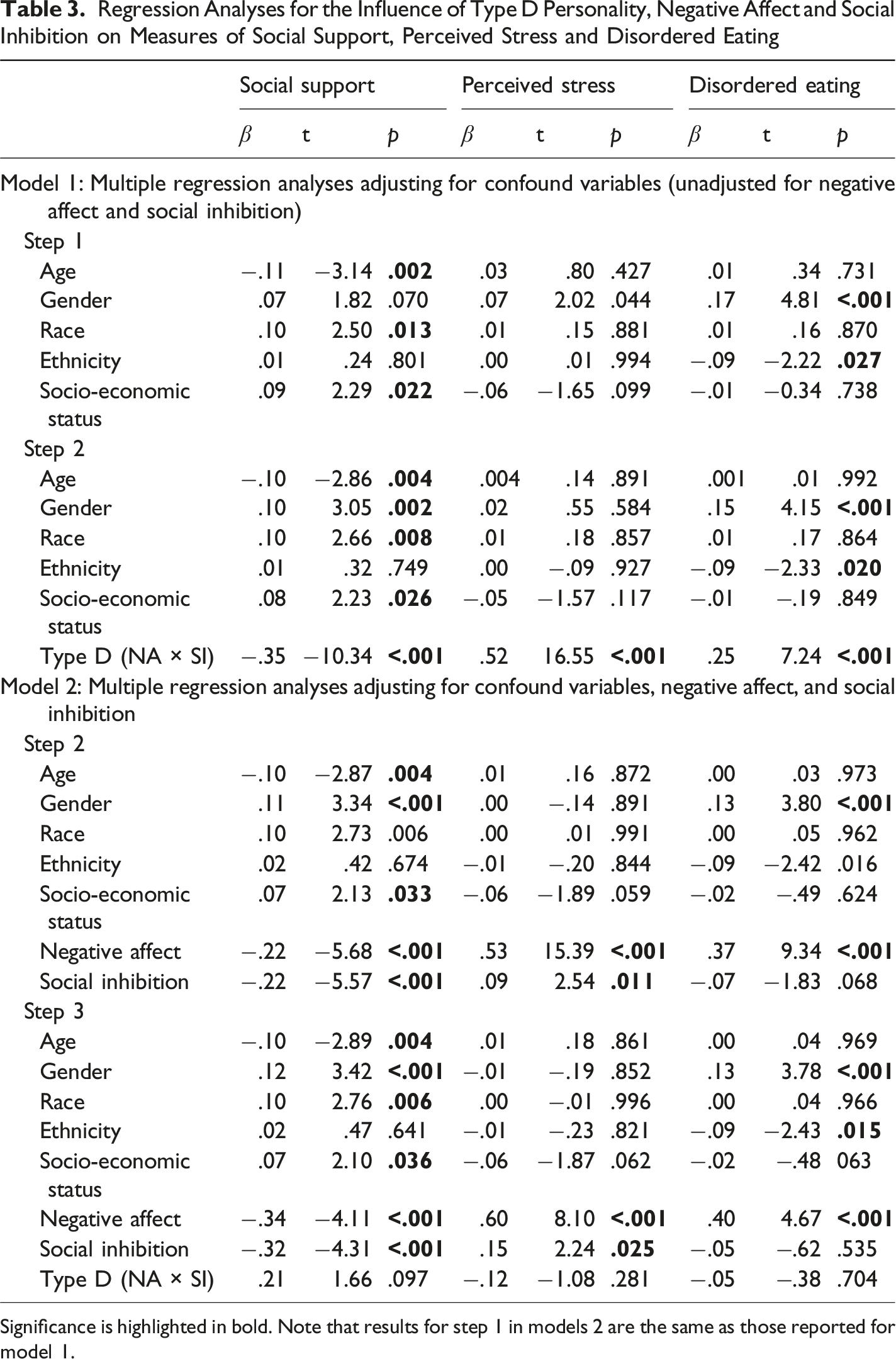
Significance is highlighted in bold. Note that results for step 1 in models 2 are the same as those reported for model 1.
Serial Mediation Analyses
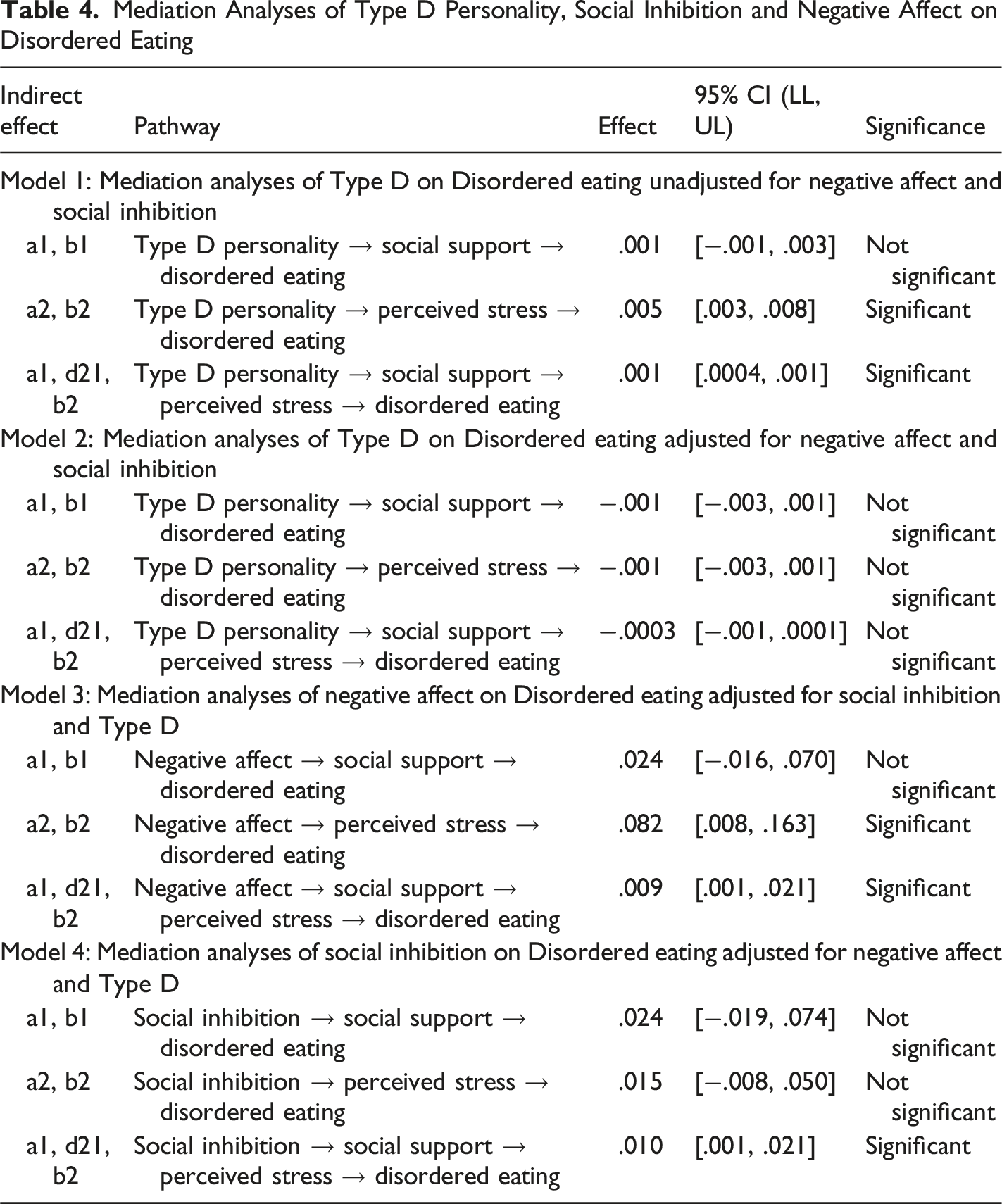
Mediation Analyses of Type D Personality, Social Inhibition and Negative Affect on Disordered Eating
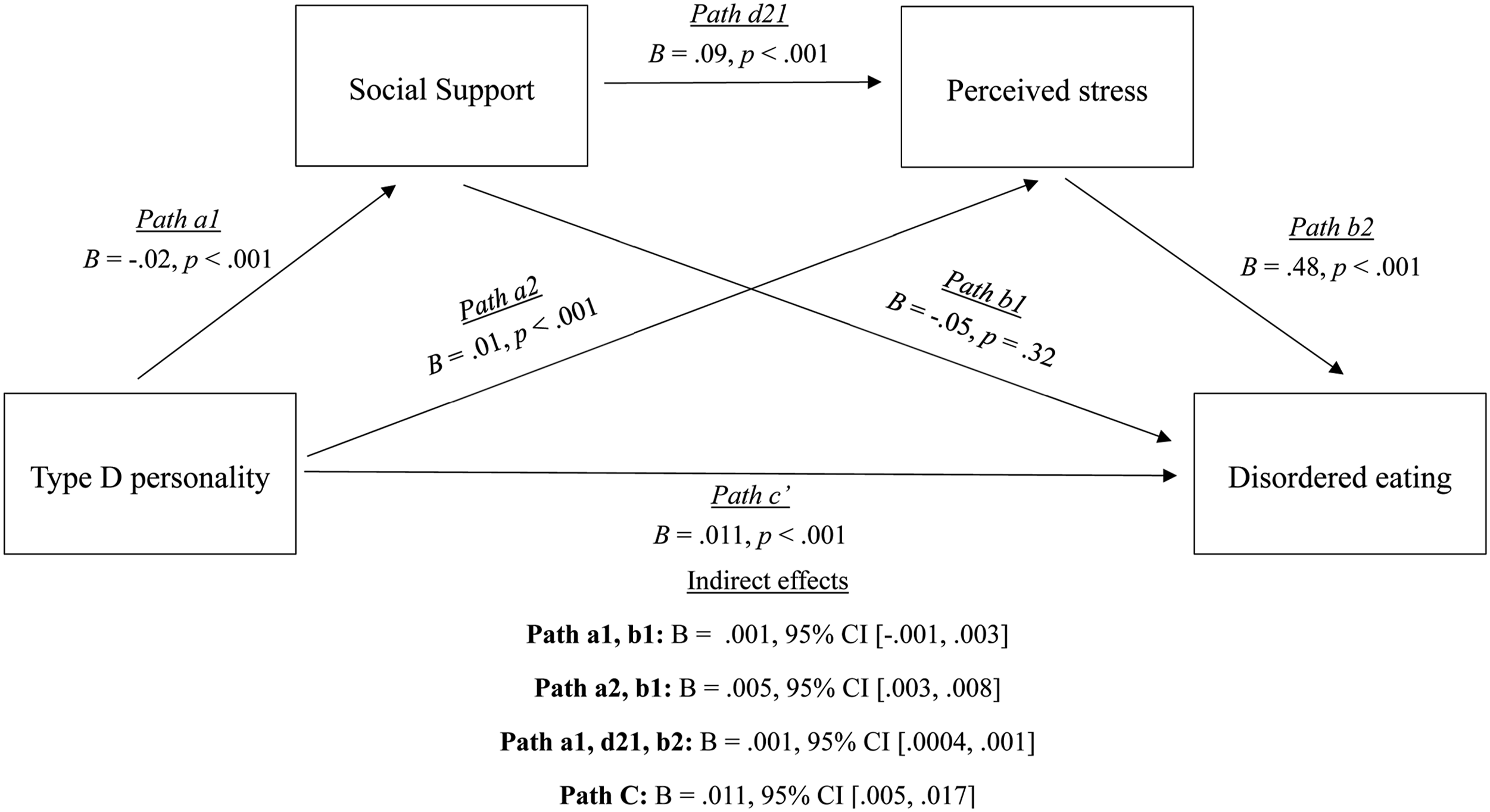
Serial mediation path diagram: Indirect effects of Type D personality on disordered eating through social support and perceived stress
Analyses Adjusting for the Main Effects of Negative Affect and Social Inhibition
Follow-up regression and serial mediation models were conducted to examine whether the aforementioned significant effects of the global Type D construct remained statistically significant after adjusting for the main effects of negative affect and social inhibition.
Adjusted Regression Analyses
In follow-up hierarchical multiple linear regression models, potential confounding variables were entered at Step 1, followed by the main effects of negative affect and social inhibition at Step 2, and the continuous Type D interaction term at Step 3. As seen in Table 3, model 2, the associations observed between Type D personality, social support, perceived stress and disordered eating were no longer significant after adjusting for negative affect and social inhibition (all p’s ≥ .097). In these models, negative affect significantly predicted lower social support, β = − .34, t = 4.11, p < .001, as well as greater levels of perceived stress, β = .60, t = 8.10, p < .001, and disordered eating, β = .40, t = 4.67, p < .001. Additionally, social inhibition was associated with lower levels of social support, β = −.32, t = 4.31, p < .001, and greater levels of perceived stress, β = .15, t = 2.24, p = .025, but not disordered eating (p = .535).
Adjusted Serial Mediation Analyses
In follow-up mediation models, the aforementioned mediation model was replicated, with the social inhibition and negative affect subcomponents added into models in addition to other potential confounding variables (i.e., age, gender, race, ethnicity and socio-economic status). As seen in Table 4 (Model 2), after adjusting for the main effects of negative affect and social inhibition, all significant indirect mediation effects of Type D personality on disordered eating became non-significant.
In order to examine the predictive utility of the individuals’ subcomponents, mediation analyses were conducted with the social inhibition and negative affect subcomponents entered into models as separate predictor variables in place of the Type D personality interaction term. In addition to the aforementioned confounding variables, Type D personality and the remaining subcomponent were included in these analyses as covariates in order to determine the independent prediction of each subcomponent. As seen in Figure 2, negative affect predicted increased disordered eating through greater levels of perceived stress (path a2, b2), B = .082, 95% CI [.008, .163]. Additionally, negative affect indirectly influenced disordered eating through a serial mediation pathway involving social support and perceived stress (Paths a1, d21, b2), B = .009, 95% CI [.001, .021]. Specifically, higher negative affect was associated with lower social support, which contributed to increased perceived stress, ultimately leading to greater disordered eating. There was also a direct effect of negative affect on disordered eating, B = .518, 95% CI [.240, .795], indicating partial mediation. Serial mediation path diagram: Indirect effects of negative affect on disordered eating through social support and perceived stress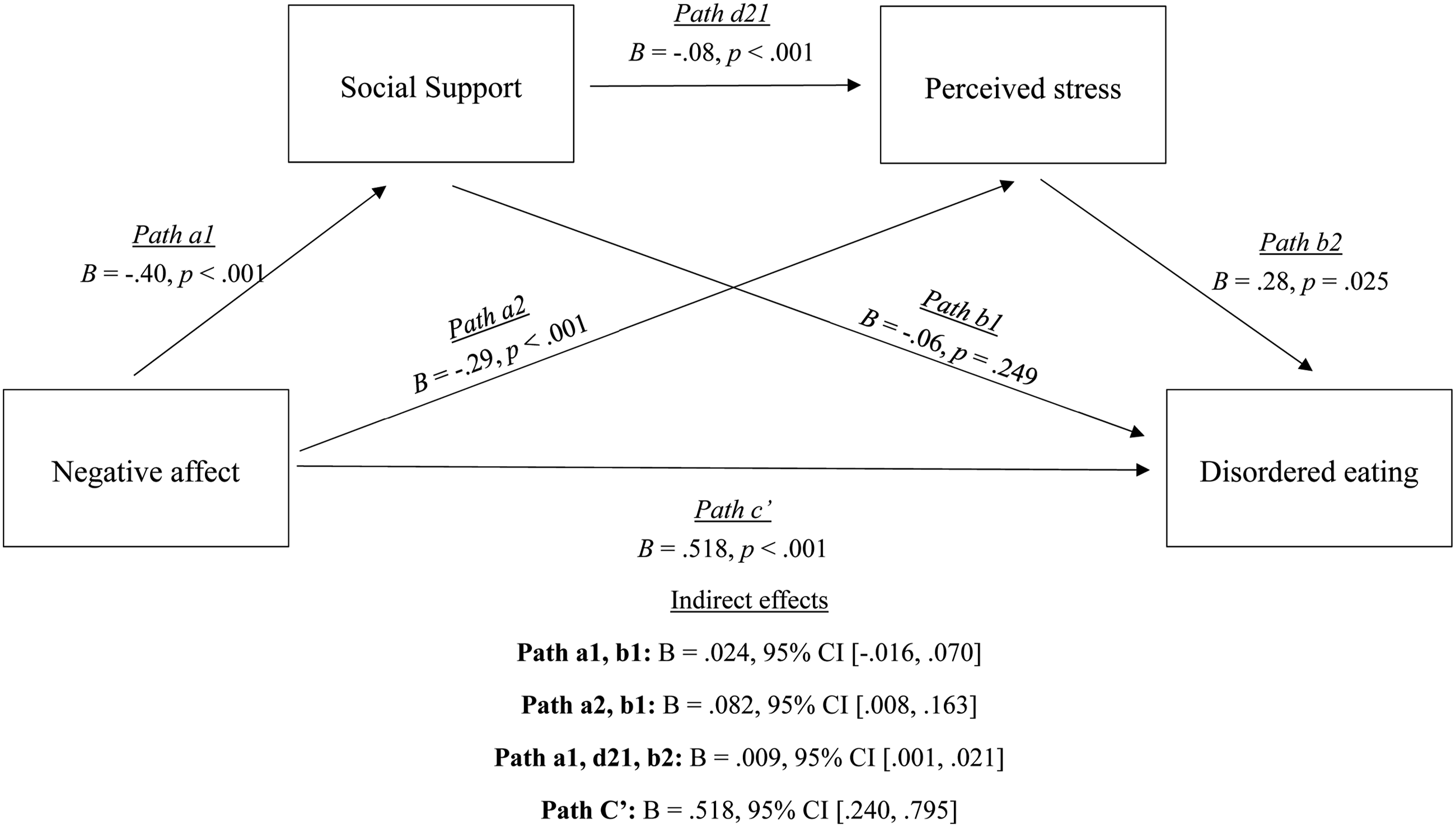
Finally, in the mediation analyses examining the indirect effects of the social inhibition subcomponent, a significant serial mediation effect emerged for the association between social inhibition and disordered eating through both social support and perceived stress (Paths a1, d21, b2), B = .010, 95% CI [.001, .021]. Unsurprisingly, greater levels of social inhibition were associated with diminished social support. In turn, diminished social support was associated with greater perceived stress, which predicted increased disordered eating symptoms (see Figure 3). The direct effect of social inhibition of disordered eating was not significant, B = −.13, 95% CI [−.390, .130], indicating that this association was fully mediated via social support and perceived stress. No other mediation effects were observed for the association between social inhibition and disordered eating. Serial mediation path diagram: Indirect effects of social inhibition on disordered eating through social support and perceived stress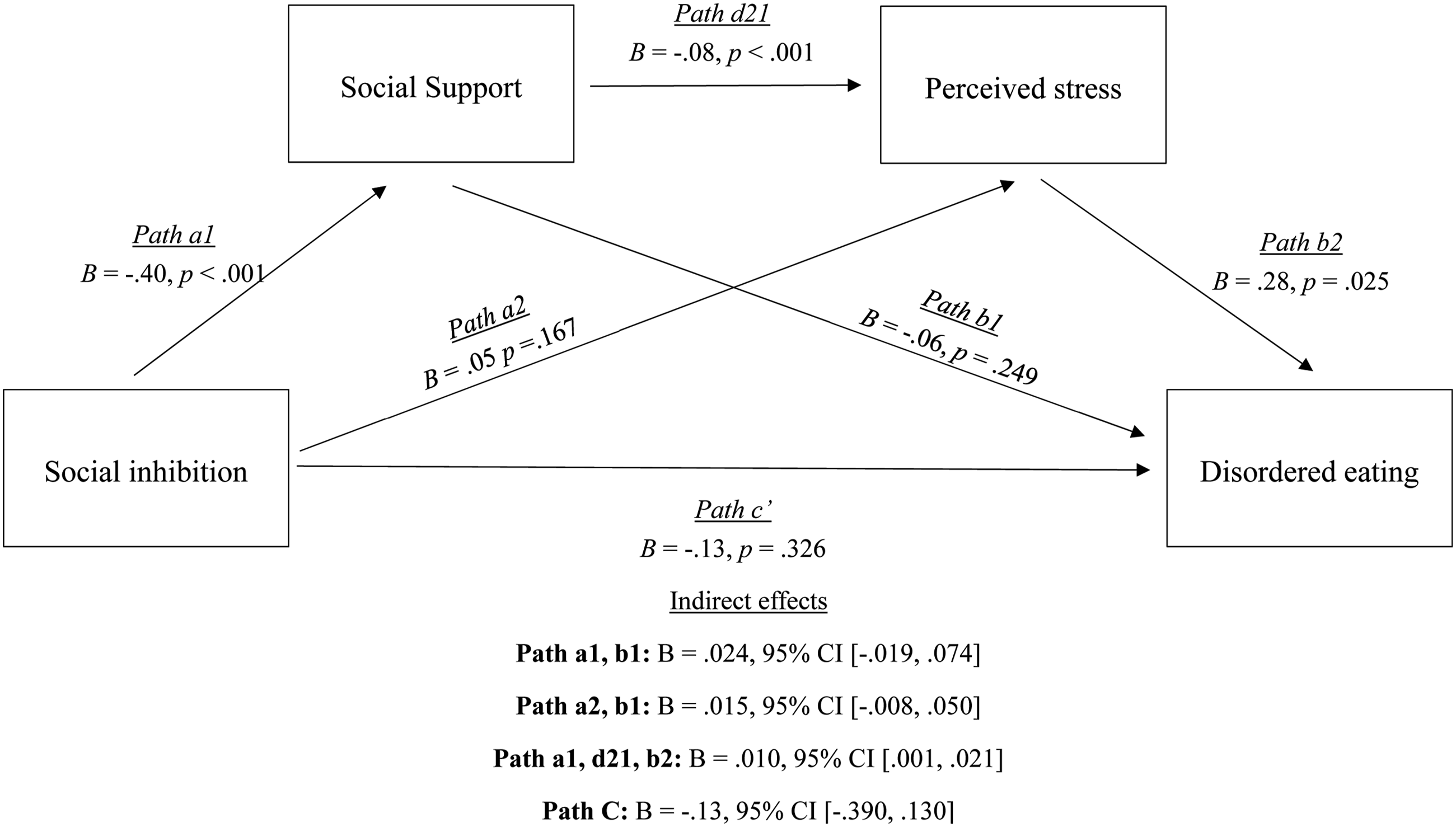
Discussion
Objective of the Current Study
The current study aimed to (1) examine the association between Type D personality and disordered eating, (2) identify the potential sequential mediating pathways through social support and perceived stress that may underlie the link between Type D personality and disordered eating, and (3) examine the independent direct and indirect effects of social inhibition and negative affect on disordered eating, and to identify if Type D personality had predictive utility in analyses adjusting for these subcomponents. Our findings indicate that Type D personality was significantly associated with greater eating disorder symptomology, as well as diminished social support and greater perceived stress. Additionally, the association between Type D personality and disordered eating symptomology was serially mediated via social support and perceived stress. Here, Type D personality was associated with reduced social support, which in turn, predicted greater levels of perceived stress, leading to increased disordered eating symptoms. However, after adjusting for the main effects of negative affect and social inhibition, both the direct and indirect effects of Type D personality on disordered eating symptomology became non-significant, indicating that the Type D effects were driven by these individual subcomponents, rather than a synergistic interaction.
Type D Personality and Disordered Eating: the Mediating Effects of Social Support and Perceived Stress
Eating disorders have a prevalence rate of approximately 20% amongst college students (Alhaj et al., 2022), with evidence indicating that the number of college students classified as having an eating disorder has increased significantly in recent years (Daly & Costigan, 2022). Thus, there has been an effort placed on identifying individual differences in disordered eating symptomology (Dufresne et al., 2020). While prior research has linked a range of negative affect variables to disordered eating symptomology (Davis & Fischer, 2013; Gilmartin et al., 2022; Koposov et al., 2023; Shea & Pritchard, 2007), the current study is the first to examine if Type D personality, characterized by the joint tendency to experience negative emotions (i.e., negative affect), and simultaneously suppress these emotions (social inhibition), predicts disordered eating symptomology. More recently, Type D individuals have been noted to report greater dissatisfaction with their physical appearance, lower satisfaction with various body parts, increased preoccupation with being overweight, and are more likely to self-rate themselves as being overweight (Borkoles et al., 2010). The findings of the current study extend on this prior literature by demonstrating that Type D personality not only contributes to various facets of poor body image but also plays a significant role in the manifestation of disordered eating symptoms.
Both diminished social support (Birmachu et al., 2021; Bodell et al., 2011) and increased perceptions of stress (Beukes et al., 2010; Hay & Williams, 2013) have been consistently linked to greater eating disorder symptomology. In fact, evidence suggests that these factors operate in sequential fashion, with diminished social support promoting heightened perceptions of stress, which in turn, predicts greater disordered symptomology (Kwan & Gordon, 2016). Interestingly, perceived stress has been posited as a key pathway facilitating the association between Type D and physical and mental health outcomes (Allen et al., 2019b; O'Riordan, Howard, & Gallagher, 2020; Williams & Wingate, 2012), with reduced social support being an important factor contributing to greater perceived stress among Type D individuals (Williams & Wingate, 2012). Consistent with prior literature, our mediation analyses revealed that greater perceptions of stress mediated the association between Type D personality and disordered eating symptomology. Interestingly, our findings also indicated a serial mediation effect, whereby lower levels of social support amongst Type D individuals predicted increased levels of self-reported stress, which in turn, predicted greater disordered eating symptomology. This mechanistic pathway may offer a potential area of intervention to decrease disordered eating symptomology amongst Type D individuals via socially supportive or stress reduction interventions.
The Predictive Utility of Type D Personality Above Negative Affect and Social Inhibition
Type D personality is posited to represent a synergistic interactional effect of both negative affect and social inhibition, whereby the inhibition of negative emotions is propounded to be particularly toxic for physical and mental health outcomes (Kupper & Denollet, 2007, 2014). Here, it is suggested that Type D personality represents the inhibition/suppression of negative emotions, rather than solely the experience of negative emotions (Denollet et al., 1995, 2000), and thus, should predict outcomes above and beyond the first order main effects of social inhibition and negative affect (Lodder, 2020; Smith, 2011). However, one of the primary criticisms consistently proffered at the Type D construct is that many of the effects observed in the literature do not actually represent a true synergistic interactional effect indicative of the inhibition of negative emotions, but rather are the product of the first order main effects of either social inhibition and negative affect (Coyne & de Voogd, 2012; Smith, 2011). In the current study, our follow-up analyses adjusting for the main effects of negative affect and social inhibition, revealed that the effects observed for Type D personality became non-significant. These findings indicate that both the direct effect of Type D personality on disordered eating, as well as the indirect mediation effects via diminished social support and greater perceived stress are primarily driven by social inhibition and negative affect, rather than a true synergistic interaction. In line with these findings, a growing body of research which haave conducted similar follow-up analyses have also reported non-significant Type D effects after adjusting for negative affect and social inhibition (Akram et al., 2018; O'Riordan, Howard, & Gallagher, 2020; Stevenson & Williams, 2014). In fact, a recent systematic review of the Type D personality literature has indicated that approximately half of the reported effects of Type D personality in prior studies are driven by either the negative affect or social inhibition subcomponent (Lodder et al., 2021).
Interestingly however, both social inhibition and negative affect were found to independently predict diminished social support and greater perceptions of stress, with negative affect also predicting disordered eating symptomology. Additionally, both social inhibition and negative affect were indirectly associated with disordered eating symptomology in serial mediation analyses. Thus, these findings may accentuate the importance of examining the individual subcomponents of Type D personality, rather than the global construct, in understanding the psychosocial mechanism linking personality to measures of social support, perceived stress and psychological well-being. In particular, more recent research has placed focus on the social inhibition subcomponent of Type D personality (Denollet & Duijndam, 2019), and the prediction of its constituent facets including social withdrawal, interpersonal sensitivity and behavioral inhibition for stress coping (Duijndam, Kupper, et al., 2020) and acute stress reactivity (Duijndam et al., 2020a, 2020b, 2025). Thus, one specific avenue for future research is to examine how the social inhibition component, and its constituent facets, contributes to stress-related processes and the development or maintenance of adverse physical and psychological wellbeing.
Limitations and Directions for Future Research
The current study is not without limitations. Firstly, the cross-sectional design precludes the definitive determination pertaining to the directionality of associations proposed here. While the proposed mediation pathways were based on prior research on both Type D personality (O'Riordan, Howard, & Gallagher, 2020), and disordered eating (Kwan & Gordon, 2016), there may be alternative explanations that explain the relationship between Type D personality, social support, perceived stress and disordered eating. Thus, we suggest that future research employ a longitudinal design to confirm the directionality proposed in the current study, and identify if the Type D facets predict prospective increases in disordered eating symptomology over time. Additionally, the current study employed a validated and reliable measure of disordered eating, with good sensitivity to identify a diagnosis of an eating disorder (Gideon et al., 2016). However, this measure assessed general disordered eating symptoms across a broad range of categories, rather than a specific eating disorder (e.g., anorexia nervosa, bulimia nervosa, binge eating disorder). Therefore, we recommend that future research examine symptomology specific measures of disordered eating. Finally, the current sample consisted of undergraduate students, who are relatively young (M = 19.17). Given the high prevalence of disordered eating in the particular cohort (Alhaj et al., 2022), examining personality differences in disordered eating symptoms amongst this cohort is imperative for identifying individuals who are vulnerable to developing eating disorder symptoms. However, considering that the prevalence of disordered eating varies significantly by age (Wells et al., 2006), it is unclear whether the associations observed here would remain significant in other cohorts. Therefore, we recommend that future research replicate the current findings in other age groups.
Conclusion
In sum, current study indicates that Type D personality is associated with increased disordered eating symptomology. This association is mediated by diminished social support and greater perceived stress, where reduced social support among Type D individuals predicts higher perceived stress, which, in turn, leads to more pronounced disordered eating symptoms. However, the direct and indirect effects of Type D personality on disordered eating symptomology became non-significant in analyses adjusting for the main effects of negative affect and social inhibition. Follow-up adjusted analyses revealed significant independent mediation effects of both social inhibition and negative affect via diminished social support and greater self-reported stress. These findings suggest that the effects observed for Type D on disordered eating symptomology are primarily driven by the social inhibition and negative affect subcomponents, rather than a synergistic interactional effect of both constructs combined.
Footnotes
Ethical Considerations
The study procedures were reviewed and approved by the institutional review board at the University of Texas at San Antonio (FY23-24-366).
Consent to Participate
Written informed consent was obtained from all participants.
Author Contributions
Adam O′ Riordan: Conceptualization, Formal analysis, writing original draft, writing, reviewing and editing. Aisling Costello: Conceptualization, Formal analysis, writing original draft, writing, reviewing and editing.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data will be made available upon reasonable request.
Disclosure
The authors have no conflicts of interest to report. The authors confirm that the research presented in this article met the ethical guidelines, including adherence to the legal requirements of the USA and received approval from the University of Texas at San Antonio Institutional Review Board.