
Abstract
The current progressive adoption of online platforms and web-based interventions, within the context of Cognitive Behavioral Therapy (CBT) services, offers a novel opportunity to scale evidence-based psychotherapy. In the present work, we depict the development of a web and native application within the Italian landscape, GRETA (Graphic Robotic Engine for Therapy Automation). GRETA provides the following functions: (a) Management of therapy appointments and payments; (b) Clinical data, therapy progress, and sessions summary between professionals; (c) Production of the medical report and notes for external institutions; (d) Homework, materials, psychometric measures, progress reports, and therapy notes; (e) Systematic monitoring of the therapeutic process and outcomes; (f) Ensuring confidentiality, security, and integrity of patient information; (g) Collection, aggregation, and analysis of anonymized patient data through statistical reports and graphical dashboards. Beyond the technological implementation, this study also assesses the effectiveness of therapy delivered through GRETA. Pre-post treatment comparisons were conducted on a sample of 442 patients discharged for any reason by the CBT service, categorized into three diagnostic groups: anxiety disorder, depressive disorder, and comorbid anxiety and depressive disorder. Results revealed significant improvements in symptom severity and functional adjustment across all groups. Future developments of GRETA will involve integrating Artificial Intelligence-based features, such as predictions of clinical outcomes.
Keywords
Introduction
Pursuing effective therapeutic interventions is an essential ethical principle in mental health care. This ethical mandate encompasses providing help-seeking individuals access to treatments demonstrating efficacy and commitment to their well-being (Guil et al., 2023; Margison et al., 2000). The term “evidence-based”, initially rooted in clinical practice guidelines within medicine, highlights the application of the most reliable evidence when making decisions about patient care (Cook et al., 2017). This approach mandates a “conscientious, explicit, and judicious” assessment of available evidence, a principle fundamental for delivering responsible interventions (Sackett et al., 1996).
The evolution of psychotherapy research, stemming from early scepticism about the efficacy of psychotherapeutic interventions (Eysenck, 1952), has moved to a pursuit to verify the effectiveness of treatments (Brown et al., 2014). In 2008, the UK Government initiated the NHS Talking Therapies (NHS-TT) program, to increase access to evidence-based psychological treatments, in line with National Institute for Health and Clinical Excellence (NICE) guidelines (Clark, 2011; Griffiths & Steen, 2013).
Cognitive Behavioral Therapy (CBT) is an “active, problem-focused, and time-sensitive approach to treatment that aims to reduce emotional distress and increase adaptive behaviour in patients with a host of mental health and adjustment problems” (Wenzel, 2017). CBT emerges within the landscape of a multitude of psychotherapeutic approaches due to its adherence to empirical validation and its demonstrated capacity to meet the criteria set forth by evidence-based practice (Gerger et al., 2020; Griffiths & Steen, 2013; Margison et al., 2000).
Positive outcomes of CBT interventions are shown to be caused, among other factors, by (a) homework execution, (b) clinical monitoring, and (c) therapy structuring and adherence to CBT protocols (Becker-Haimes et al., 2022; Griffiths & Steen, 2013; Kazantzis et al., 2016). Homework execution concerns patients allocating between-session time to performing actions as suggested by the therapist, to promote cognitive and behavioral change (Kazantzis et al., 2016). Nonetheless, the effectiveness of CBT interventions is typically monitored through session-by-session outcome measures evaluating symptoms and adaptive functioning progress, thus ensuring a shared view of the therapy status between patient and therapist (Becker-Haimes et al., 2022; Cohen et al., 2013). However, various reasons often don’t permit adherence by the therapist or the patient to the points mentioned above, thus reducing the therapy efficacy (Boswell et al., 2013).
Digital technologies have notably revolutionized mental health care, presenting an innovative avenue that resonates with the principles of evidence-based practice. The digital revolution in mental health encompasses a broad spectrum, spanning various levels of interaction among patients, mental health professionals, and digital platforms. It ranges from therapeutic content consumption by the patient-platform dyad, to patient-therapist interaction fully mediated by the platform, to a more limited patient-therapist interaction partially supported by the platform (Tuerk et al., 2019).
The widespread adoption of online platforms and web-based interventions offers an unprecedented opportunity to scale evidence-based practices (Lutz et al., 2023; Tuerk et al., 2019). Digital technologies facilitate ongoing, real-time patient progress monitoring, allowing therapists and researchers to track data regarding symptom expression between therapy sessions. This ability enables the comprehensive assessment of patient advancement and intervention effectiveness in the long term, aligning with the measurement needs inherent in evidence-based practice (Lutz et al., 2023; Margison et al., 2000; Tuerk et al., 2019). This digitalization process has the potential to yield a positive impact on the area of CBT, facilitating clinicians and patients to overcome obstacles related to homework execution, monitoring of clinical advancements, and structuring of therapeutic interventions.
Indeed, CBT has emerged as a pioneering approach within the digitalization of mental health care. Its versatility and adaptability have facilitated its integration into online platforms and web-based interventions more extensively than other psychotherapeutic approaches (Denecke et al., 2022). This involvement in digital innovation has enabled CBT to transcend traditional therapy boundaries, promoting new avenues for patient-therapist engagement mediated by digital platforms (Alavi et al., 2020; Denecke et al., 2022). The dialogue between CBT and digital technologies has expanded access to evidence-based interventions and revolutionized the monitoring and assessment of patient progress (Brown et al., 2014; Margison et al., 2000; Tuerk et al., 2019).
Denecke and colleagues recently conducted a literature review of studies that explore the characteristics and utilization of CBT within mobile health (mHealth) applications (Denecke et al., 2022). The authors delineate two distinct groups of technologies. Firstly, mHealth apps leverage technologies that operationalize tangible CBT techniques including cognitive restructuring, behavioral activation, and problem-solving strategies. Second, technologies focused on increasing user experience, adherence, therapy engagement, and questionnaire filling.
GRETA (Graphic Robotic Engine for Therapy Automation) is a novel web and native application developed within the Italian landscape, that embodies a bridge between the two classifications of mHealth technologies delineated by Denecke and colleagues (2022). GRETA serves as a comprehensive tool supporting the entire spectrum of CBT-oriented psychotherapy, aiding in the tracking of therapy progress, and facilitating clinicians in securely archiving all documentation within a reserved and protected space. In the present work, we depict the development of GRETA through qualitative and quantitative measures, aiming to describe this platform in support of the CBT process.
Methods
Overview of the GRETA Platform Implementation
The GRETA platform design and conception were performed by a diverse team of researchers, clinicians, and experts in informatics. This mHealth framework comprises users, including CBT patients and clinicians, and a service provider called inTHERAPY. The latter represents an Italian network of cognitive-behavioural psychotherapists, led by the guidance of Studi Cognitivi Group, an Italian research and training institute in cognitive and behavioral therapies, and focused on providing evidence-based CBT to Italian-speaking adults, in person or remotely.
The primary objective of GRETA is to facilitate the CBT process. Clinicians are provided with a secure repository to store patient-related documents, socio-anamnestic details, and clinical information. Additionally, they can efficiently handle session scheduling via a calendar interface. Furthermore, patients and therapists can communicate between sessions using an online chat feature. Patients benefit from a user-friendly platform that enables them to respond to questionnaires and engage in behavioural tasks conveniently from their homes; this facilitates systematic data collection to monitor therapy progress. Hence, the collected data can be exported in .xlsx, .csv, .pdf, and other formats, allowing researchers to produce statistical reports and analyses.
Overview of the Functions Provided by GRETA
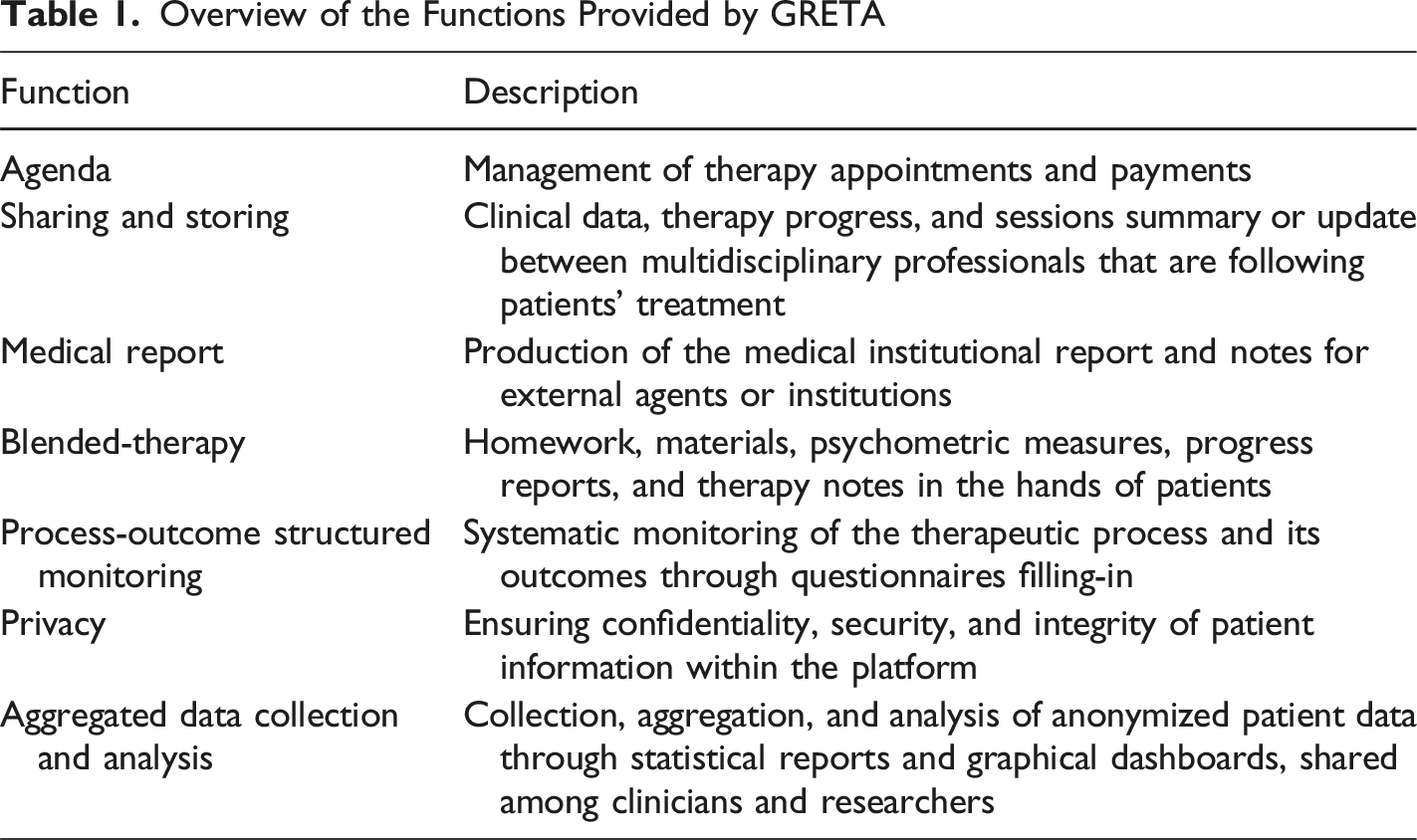
Integrated Tools for Clinical Information Gathering
GRETA incorporates a comprehensive set of tools designed for systematic information gathering within the context of CBT. These tools are integrated to facilitate both clinicians and patients in a thorough assessment of various aspects relevant to the therapeutic process. The information collection tools within GRETA include:
Anamnestic Questionnaire
A structured questionnaire covering diverse aspects of the individual’s background, childhood, relationships, family dynamics, and significant life events. Questions range from family structure to experiences during childhood and adolescence.
Personal History Assessment
In-depth exploration of the individual’s personal history, covering educational background, occupational history, relationship status, and satisfaction, providing insights into various life domains.
Health and Lifestyle Survey
A comprehensive survey covering smoking habits, alcohol consumption, drug use, dietary patterns, sleep habits, physical health, and any history of accidents, surgeries, or medical conditions.
Standardized Psychological Assessment
A series of standardized psychological assessments, including the Generalized Anxiety Disorder-7 (GAD-7) (Spitzer et al., 2006), the Patient Health Questionnaire Depression Scale-9 (PHQ-9) (Spitzer et al., 1999), the Work and Social Adjustment Scale (WSAS) (Mundt et al., 2002a), among other psychometric instruments. - The GAD-7 is a 7-item self-report questionnaire assessing anxiety symptoms, rated on the same 0–3 scale. It demonstrates excellent internal consistency (α = .92). Total scores range from 0 to 21, with cutoff points for minimal (0–4), mild (5–9), moderate (10–14), and severe (≥15) anxiety. - The PHQ-9 is a 9-item self-report measure of depressive symptoms, each rated on a 4-point scale (0–3). It shows good internal consistency (α = .89). Total scores range from 0 to 27, with cutoff values indicating minimal (0–9), mild (10–14), moderate (15–19), and severe (≥20) depression.
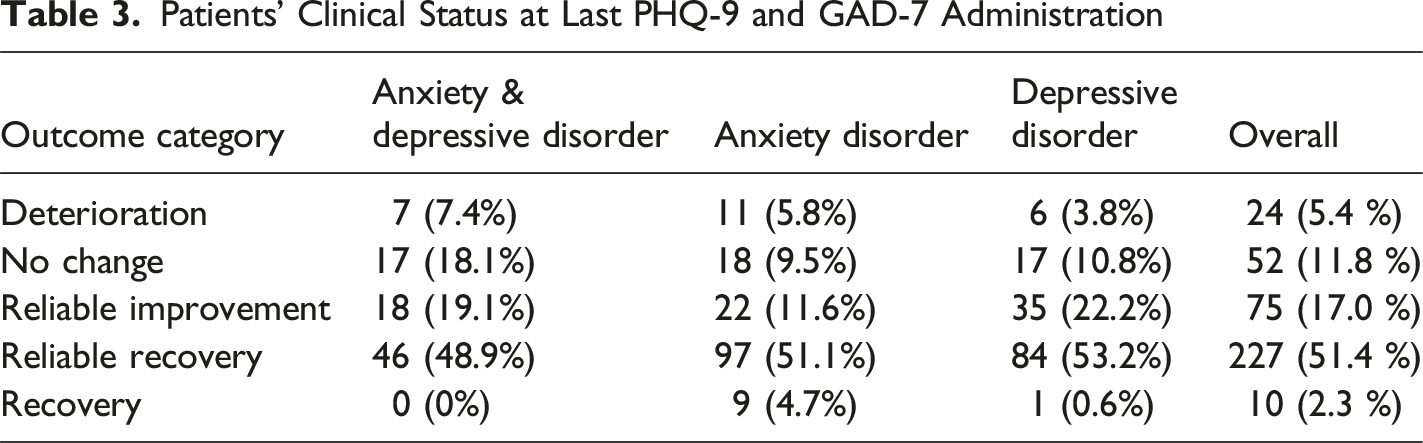
These two questionnaire scores can be combined longitudinally from first to last administration to define patients’ clinical status as Recovery, Reliable Recovery, Reliable Improvement, No Change, or Deterioration (NHS Digital, 2020). Moreover, patients scoring below clinical thresholds at baseline can be categorized as Not at caseness at the start of the treatment (NHS Digital, 2020). - The WSAS is a 5-item self-report measure assessing functional impairment in work, home management, social and private leisure, and relationships. Items are rated on a 9-point scale (0–8), with good internal consistency (α = .81).
Homework
A series of tasks proposed by the therapist to the patient, such as self-monitoring (systematic observation of self’s thoughts, emotions, and body feelings), activity scheduling (behavioral activation strategies), graded exposure plans (strategies to overcome avoidance), and skills application.
The platform is designed with a flexible architecture that also allows for the integration of new assessment tools and instruments when needed by the clinical team.
Software Interfaces
The GRETA software is served to external and internal end users via a web browser interface or mobile application. Additionally, a backend REST API interface level is available for backend-to-backend integrations, which could be useful to interact with GRETA from other external software for scientific and research purposes.
Software Integrations
These are integrations that already exist and are leveraged in the system: • InTherapy CRM, automatically provides synchronized patients’ contact data between inTherapy and GRETA, to facilitate patients’ journey from first booking to service delivery • Zoho Analytics, for scientific and statistical analyses of data produced and made available by GRETA
Design of the Input Interface
The user interface (UI) is designed to make navigation simple and immediate. Once logged in with credentials, the user can always navigate with an awareness of the functionality and the point in the tree structure they are currently in; this is evidenced by the navigator, which is consistently displayed at the top of the page. The navigator is presented to the user in the following format:
GRETA offers a responsive interface accessible both through its website and mobile application. This design feature guarantees a consistent and optimal user experience, regardless of the chosen access point. Whether navigating through the website or the app, GRETA adapts effortlessly to various devices and screen sizes, ensuring a seamless and user-friendly interaction.
Patients can initiate their journey autonomously, either by scheduling a first visit through the inTHERAPY website or by engaging in an introductory phone call facilitated by the Clinical Contact Center, offering a preliminary reception and guidance service. When the therapist records the patient on GRETA, an email is sent to the patient containing login credentials for their confidential area, payment instructions, and a request for consent to the Terms and Conditions. The psychodiagnostic assessment, overseen by a Case Manager (CM) both in-person and online, encompasses a diagnostic-oriented initial visit following DSM-5 criteria (APA, 2013). Standardized test completion is facilitated through the GRETA platform, followed by a feedback session with the CM to discuss assessment results and treatment recommendations.
Upon completion of the assessment, the Case Manager compiles a Diagnostic and Therapeutic Indication Report (RIT). This report is transmitted to the Clinical Administration via GRETA, where it is used to identify the most suitable clinical unit and therapist based on indications, therapist competencies, service availability, and patient preferences. Subsequently, the patient proceeds to their initial treatment visit with the assigned therapist. Treatment progress is regularly monitored through GRETA by the therapist, clinical secretariat, and clinical supervision unit. Leveraging clinical effectiveness indicators, GRETA facilitates the personalized and flexible adaptation of the patient’s clinical procedures. Figure 1 illustrates the patient’s journey in inTHERAPY. The patient’s journey in inTHERAPY
Processing Design: Technical Implementation of Data Storage and Automated Scoring Algorithm
For each test, a set of questions is defined (along with their respective response types) and the criteria for calculating subscales are established. The criteria may also consider patient-related variables (e.g., biological sex or age). Each execution triggers GRETA to calculate the result, which is then saved for subsequent use in monitoring.
The utilization of data gathered through GRETA encompasses two distinct objectives: firstly, a patient-specific application for symptom monitoring, conducive to therapeutic interventions; secondly, an anonymized and aggregated format designed to contribute to scientific research endeavors.
All interactions with GRETA occur through encrypted protocols (HTTPS and SSL), and the data is hosted in European data centers in compliance with General Data Protection Regulation (GDPR) standards (Regulation, 2016). The management of personal information also adheres to the provisions outlined by GDPR.
Different users can access GRETA, depending on their role and function at inTHERAPY, and they can have access to two levels of access: • External end users: ° Patient: Through GRETA, patients can fill out psychometric tools essential for diagnosis and therapy monitoring. They can view material the therapist shares (e.g. therapy notes, key messages, self-help materials) and access a chat system that allows them to maintain constant contact with their therapist. • Internal end users: ° Case Manager: The psychotherapist who meets the patient at their first appointment and is the one who makes the diagnosis and suggests the therapy. ° Principal Therapist: The primary psychotherapist associated with the patient and performs the therapy journey. ° Co-Therapist: Other possible clinical professional associated with the patient, as a secondary therapist. ° Clinical Supervisor: Typically, a senior-level psychotherapist who oversees the progress of the therapy. • Back office end users: ° System Administrator and Clinical Administrator: They have authorizations that exclusively allow the creation of new user accounts and/or new roles, as well as the management of these within their area of expertise. ° Clinical Center Administrator: Identifies users responsible for managing the initial contact with the patient, as well as referring the patient to the therapist.
Design of the Output Interface
When the patient logs in to GRETA, a dashboard is presented displaying therapy sessions to be paid for and those already paid, scheduled appointments, as well as questionnaires or tasks assigned by their therapist. Through the menu, the user can access a shared notice board where the therapist can provide supportive material for the psychotherapeutic process, the tools assigned by the therapist for its execution, and the chat system to stay in touch with the therapist. Regarding questionnaires and tasks, the patient can review past submissions, and reminders can be set to prompt the patient to complete a specific questionnaire.
Therapists accessing GRETA are redirected directly to the dossier page, where they can view the patients under their care, the therapy status, and any upcoming scheduled sessions. The menu allows the therapist to access the appointments section, where they can check their schedule and schedule a new appointment, the tools section, where they can assign questionnaires or tasks to a patient, the chat section, where they can stay in touch with patients, and the media section where they can upload multimedia materials to share with patients. The tools section provides the therapist with a wide selection of psychodiagnostic questionnaires useful in the assessment and monitoring phases of therapy, the patient’s health condition, and homework. When the patient completes questionnaires, the results are made available in the ‘monitoring’ section. They can be easily interpreted with a line or bar graph that can be easily exported in PDF format. Figure 2 depicts an example; it is worth noting that anxiety scores temporarily increased when the patient began a structured program of social exposures. Depression scores also showed a slight increase initially, reflecting the patient’s engagement with core feelings of inadequacy after a long period of avoidance and social withdrawal. These patterns do not indicate a worsening of the disorder, but rather the expected emotional activation associated with confronting feared situations during therapy. Examples of a patient’s therapy journey as depicted by clinical questionnaire scores, from the first to the last filling-in. Each dot represents a questionnaire completion requested by the clinician. The (A) graph represents the WSAS scores (Mundt et al., 2002b); the (B) graph represents the PHQ-9 scores (Spitzer et al., 1999); the (C) graph represents the GAD-7 scores (Spitzer et al., 2006)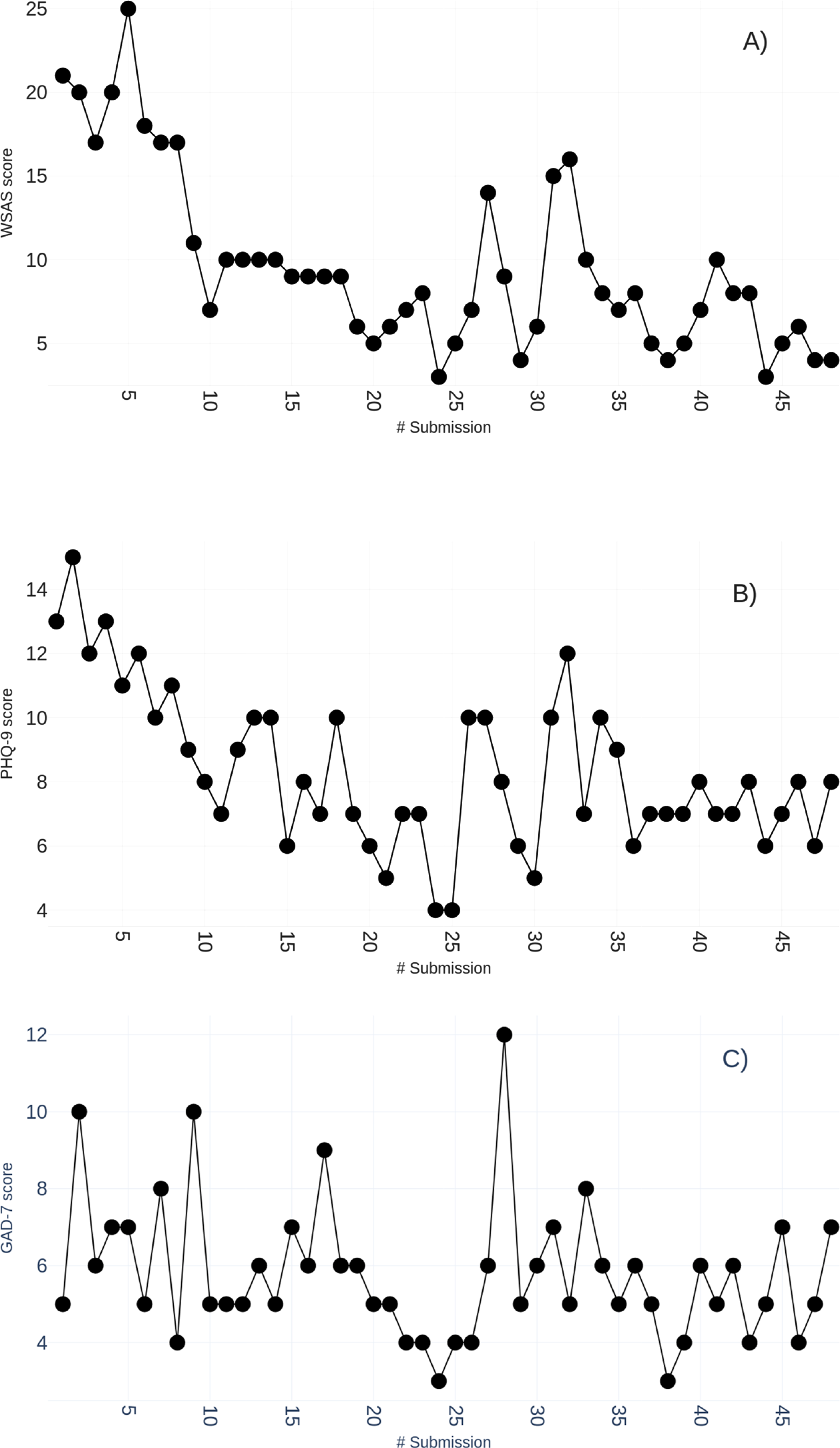
Pre-post Treatment Analyses
To assess the effectiveness of therapy, we conducted descriptive and inferential analyses on the subgroup of patients who have been discharged by the CBT service for any reason (i.e, both those who completed the full treatment course and those who dropped out) (Wakefield et al., 2021).
Specifically, a series of robust mixed ANOVAs were performed considering the violation of normality assumptions with time (pre-treatment vs. post-treatment) as a within-subjects two-levels variable and the presence of an anxiety or depressive or comorbid anxiety and depressive disorder as a between-subjects three-levels variable. Outcome measures included scores on the GAD-7, PHQ-9, and WSAS questionnaires. This approach allowed us to evaluate both overall pre-post changes in symptom severity and functioning, as well as differential patterns of improvement between patients in the three groups.
Additionally, a chi-square test of independence was conducted to examine whether there was a significant association between diagnostic group membership (anxiety, depression, or comorbid anxiety and depression) and treatment completion status (dropout vs. therapy completion). This analysis aimed to determine whether the likelihood of discontinuing therapy differed across diagnostic categories.
All analyses were conducted in R (R Core Team, 2025) and RStudio version 2025.5.1.513 (Posit team, 2025), using an alpha level of 0.05. Informed consent for participation and data processing was obtained from all participants, in accordance with the Declaration of Helsinki (World Medical Association, 2013) and with the approval of the Ethics Committee of Sigmund Freud University, Vienna.
Results
GRETA Platform Development
The GRETA platform development started in March 2021 and it has been operational since March 2022.
The following results refer to the time frame from March 2022 to October 2024. 6110 individuals represent the GRETA users. Among these, 5620 are patients and 490 are psychotherapists. Other professionals such as computer scientists, clinical supervisors, clinical administrators, and researchers collaborate with the company. 197 patients contacted the Clinical Contact Center and received an invitation link to the GRETA platform, but never logged in. This subset accounts for 3.5% of the patient user base that may present resistance to using the digital platform. Patients utilized GRETA for durations ranging from a minimum of 1 day to a maximum of 951 days (platform age at the time of analysis). On average, patients utilized the platform for 145 days.
The clinical results collected through GRETA are presented in a comprehensive graphical dashboard, and organized into five distinct sections to provide a detailed overview of various aspects of the GRETA platform’s impact and effectiveness (Figures 3(A), 3(B), 3(C), 3(E)). The graphical representations ensure a visually intuitive presentation of insights for clinicians and researchers involved in the InTHERAPY project. Examples of graphical reports built in the Zoho Analytics dashboard. (A) Geographical origin of patients; pink represents female patients and blue male patients. (B) Therapy journeys: the horizontal axis depicts the total number of therapy sessions each patient performed, and the vertical axis shows the total duration in days of each therapy. Vertical and horizontal bars show the mean for each axis. (C) Distribution of the number of diagnoses in the sample of patients. (D) Comparison of average scores of the GAD-7 a clinical questionnaire, before and after therapy completion. The red line indicates the clinical score cutoff; the value depicted over the bars represents the sample size. (E) Therapy efficiency representation, as described by the NHS-TT program: the vertical axis represents the cumulative percentage of patients; the horizontal axis represents the ordinal number of therapy appointments; the blue line represents the reliably improved patients in clinical symptoms, and the yellow line represents the recovered patients in clinical symptoms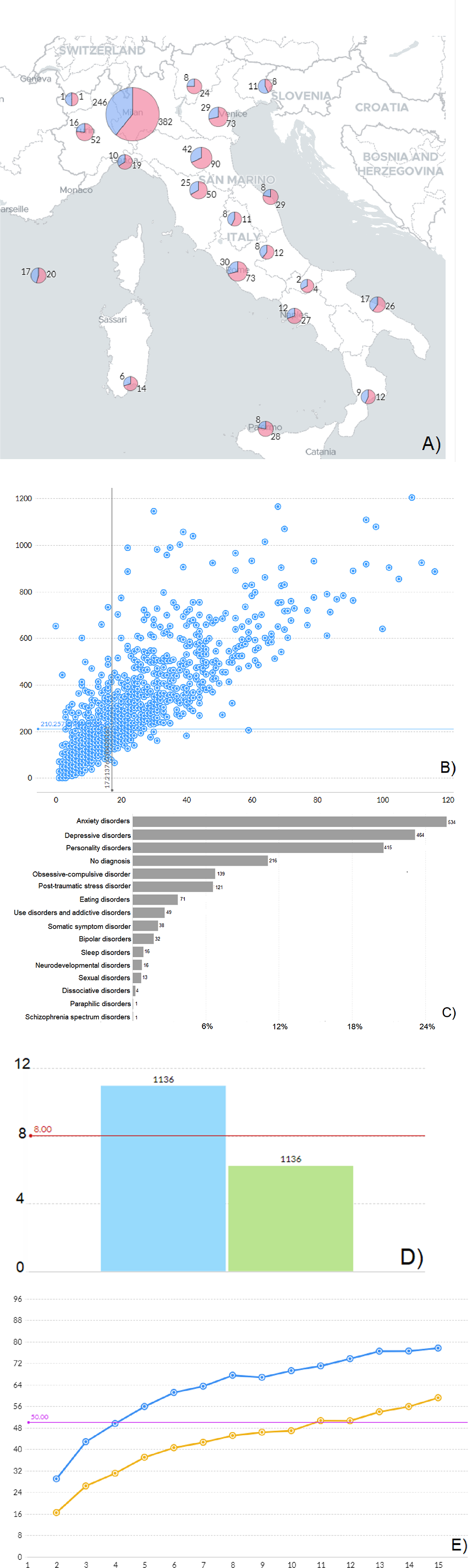
The first dashboard section encompasses sociodemographic information about the sample of patients, including their geographical origin, sex, and age.
The second section focuses on the process-key quality indicators of therapy delivered, such as • Total number of therapy sessions delivered, • Distribution of therapy status (i.e., ongoing evaluation, ongoing therapy, dropout from therapy, finished therapy, follow-up), • The average number of waiting days before starting the therapy, • The average number of therapy sessions per month, • Rate of questionnaires filling in.
The third section delves into clinical and diagnostic information, providing a comprehensive understanding of the patient’s mental health profiles, including categorical diagnostic presentation, the distribution of the number of diagnoses in the sample of patients, the average number of diagnoses per patient, and CBT approaches adopted by therapists (i.e., metacognitive therapy, rational-emotive behavior therapy, dialectical behavior therapy, compassion focused therapy, etc.).
The fourth and fifth sections of the dashboard offer an overview of outcome-key quality indicators in terms of efficacy and effectiveness of treatments. These analyses serve to highlight the progress and changes observed throughout the therapeutic interventions, through clinical and psychosocial functioning questionnaire scores comparing the start and the end of the treatment, in the whole sample, or for specific diagnostic or clinical profiles (for example, comparing patients with or without a personality disorder). These sections are set to monitor therapy outcomes in alignment with the criteria outlined by the English NHS-TT program (Griffiths & Steen, 2013). These sections evaluate the effectiveness of the therapeutic interventions by tracking predefined outcome measures, contributing valuable data for ongoing assessment of therapy progression.
Pre-post Treatment Analyses
The sample of subjects who were discharged for any reason comprised 442 patients; those who completed the full treatment course were 238 (53.8%), and those who dropped out were 204 (46.2%). Patients were categorized into three diagnostic groups: comorbid anxiety and depressive disorder (n = 94), anxiety disorder (n = 190), and depressive disorder (n = 158). The overall mean age was 37.5 years (SD = 12.5), with a median of 35 years (range = 18-79). Mean ages ranged from 36.0 years (SD = 11.6) in the comorbid anxiety and depressive disorder group to 39.2 years (SD = 13.0) in the depressive disorder group; mean age in the anxiety disorder group was 36.9 (SD = 12.4). The sample was predominantly female (60.2%, n = 266); females were 60.6 % in the anxiety and depressive disorder group, 60.0% in the anxiety disorder group, and 60.1% in the depressive disorder group. A total of 54 patients (12.2%) were classified as Not at caseness at the start of treatment, including 6 patients (6.4%) with comorbid anxiety and depressive disorder, 33 patients (17.4%) with anxiety disorder, and 35 patients (22.2%) with depressive disorder.
Due to violations of normality assumptions and the presence of extreme values, a series of robust ANOVAs were conducted using the WRS2 package (Mair & Wilcox, 2020). This approach provides reliable estimates under conditions of heteroscedasticity and non-normal data distributions.
Descriptive Statistics for Symptom Severity and Functional Impairment by Diagnostic Group. The Values Refer to Mean ± Standard Deviation
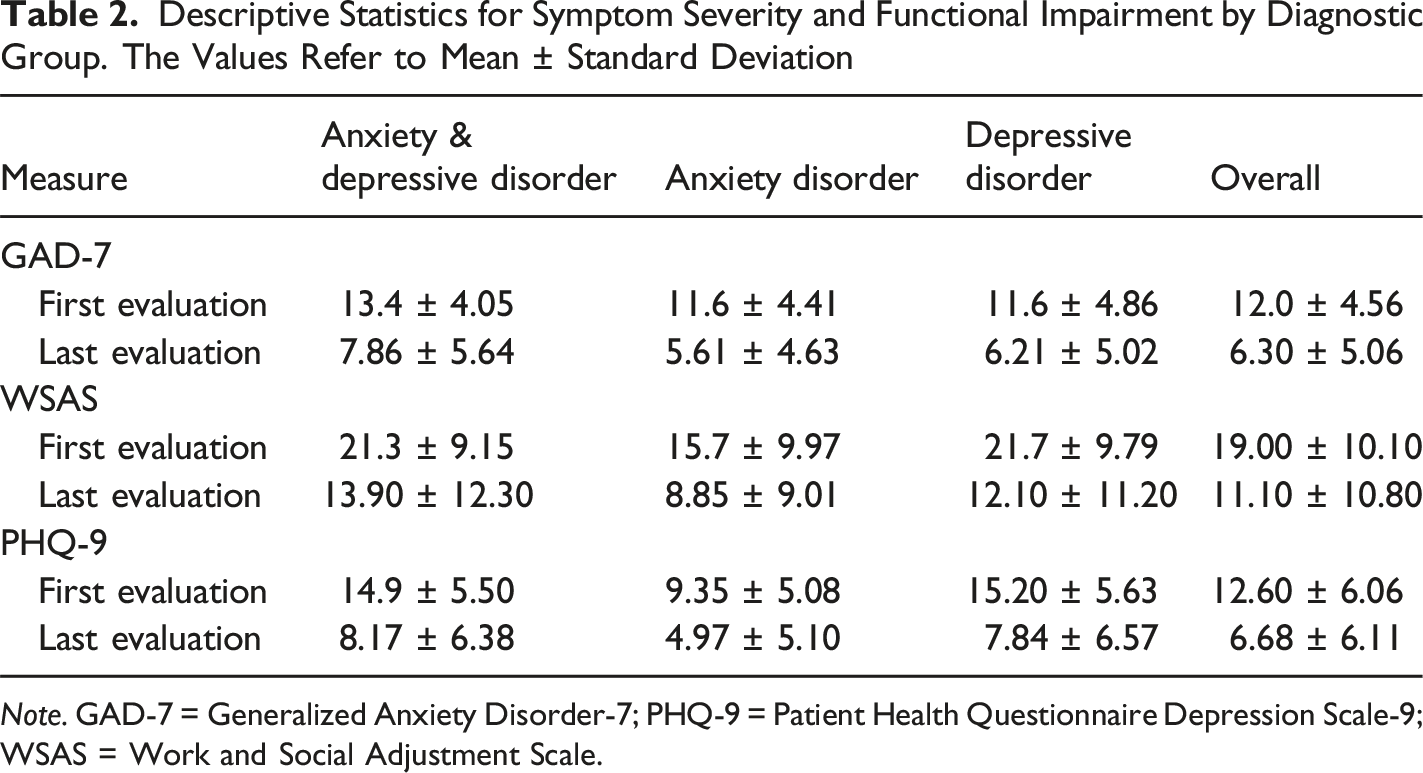
Note. GAD-7 = Generalized Anxiety Disorder-7; PHQ-9 = Patient Health Questionnaire Depression Scale-9; WSAS = Work and Social Adjustment Scale.
Patients’ Clinical Status at Last PHQ-9 and GAD-7 Administration
Results of the Mixed Between/Within-Subjects ANOVA on GAD-7 Scores
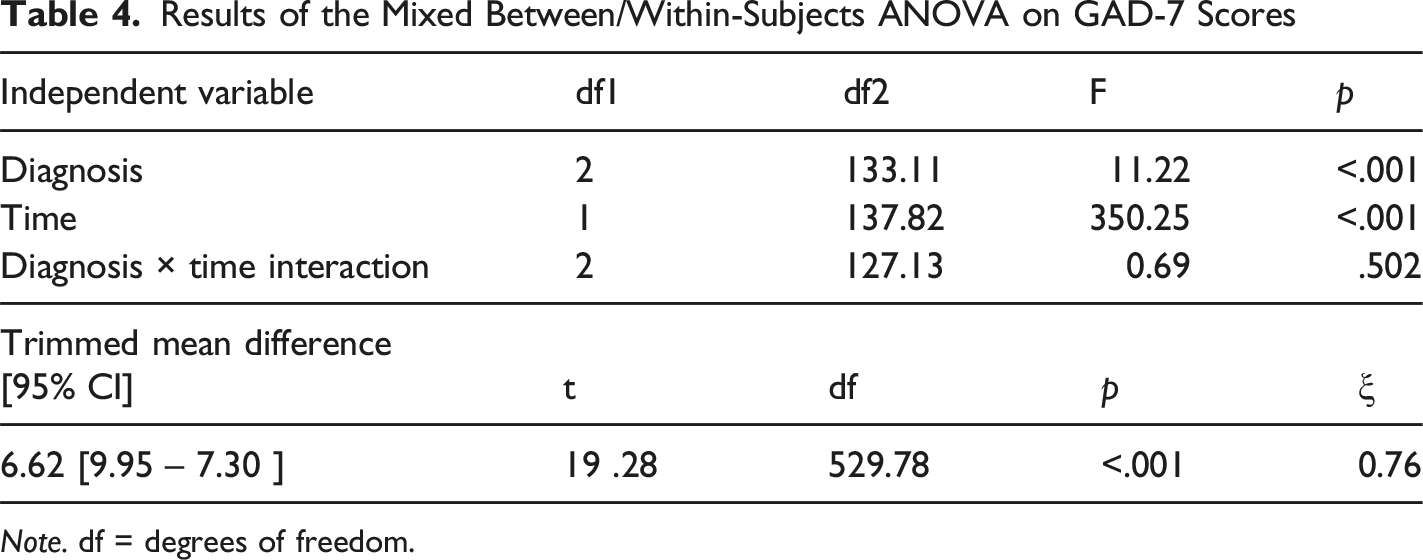
Note. df = degrees of freedom.
Between-Group Contrasts (Lincon)
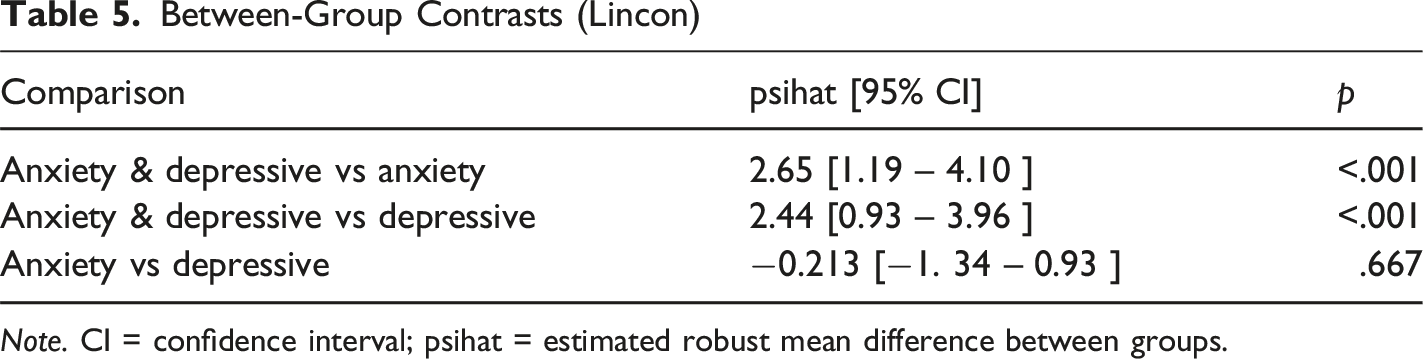
Note. CI = confidence interval; psihat = estimated robust mean difference between groups.
Results of the Mixed Between/Within-Subjects ANOVA on PHQ-9 Scores
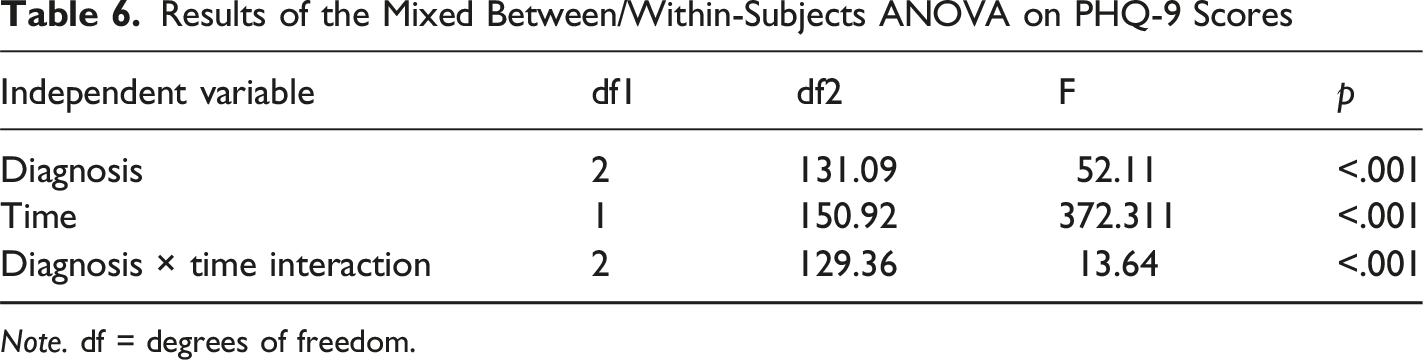
Note. df = degrees of freedom.
Temporal Contrasts Within Each Diagnostic Group (Yuen’s Test, 20% Trimmed Means)
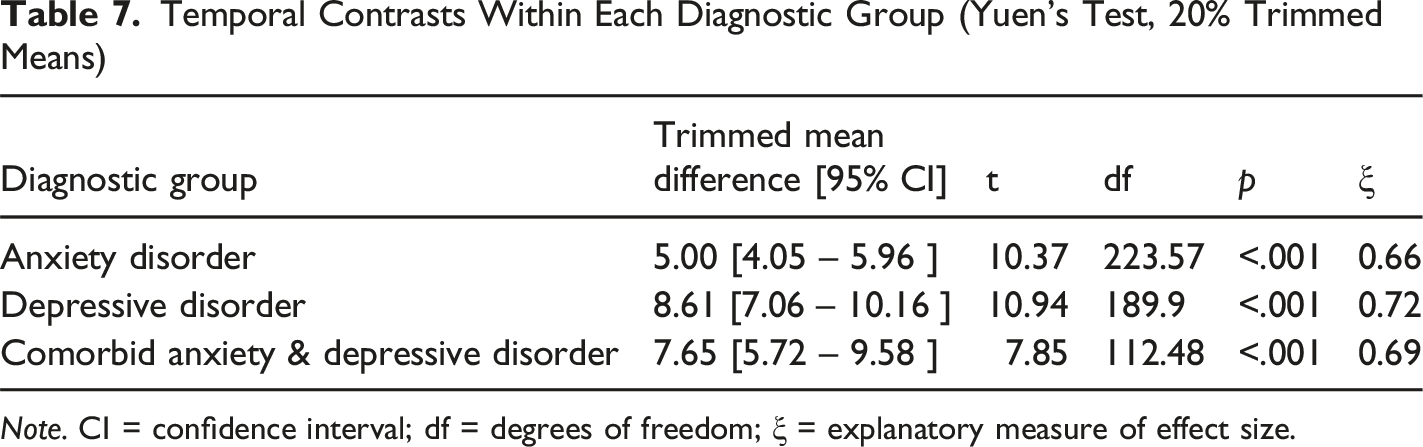
Note. CI = confidence interval; df = degrees of freedom; ξ = explanatory measure of effect size.
Between-Group Contrasts at the First Time Point (Lincon)
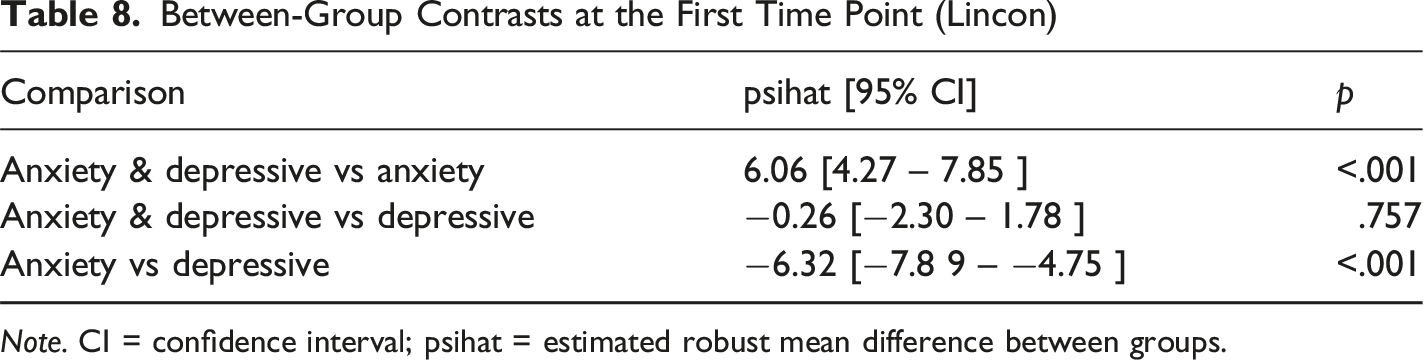
Note. CI = confidence interval; psihat = estimated robust mean difference between groups.
Results of the Mixed Between/Within-Subjects ANOVA on WSAS Scores
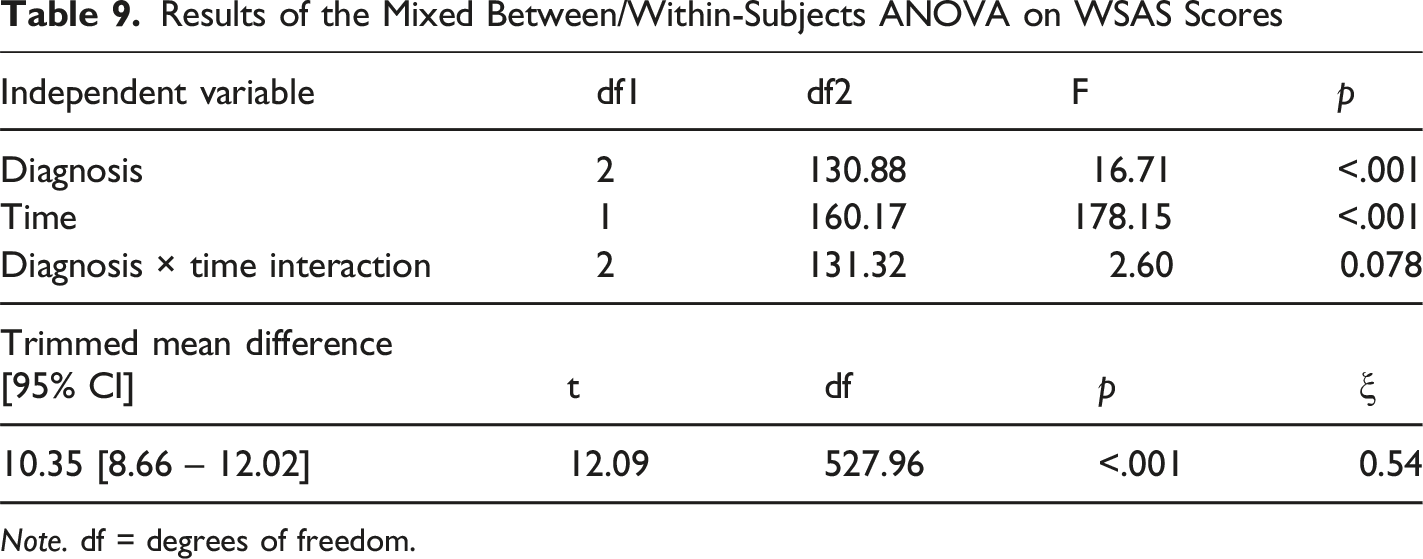
Note. df = degrees of freedom.
Between-Group Contrasts (Lincon)
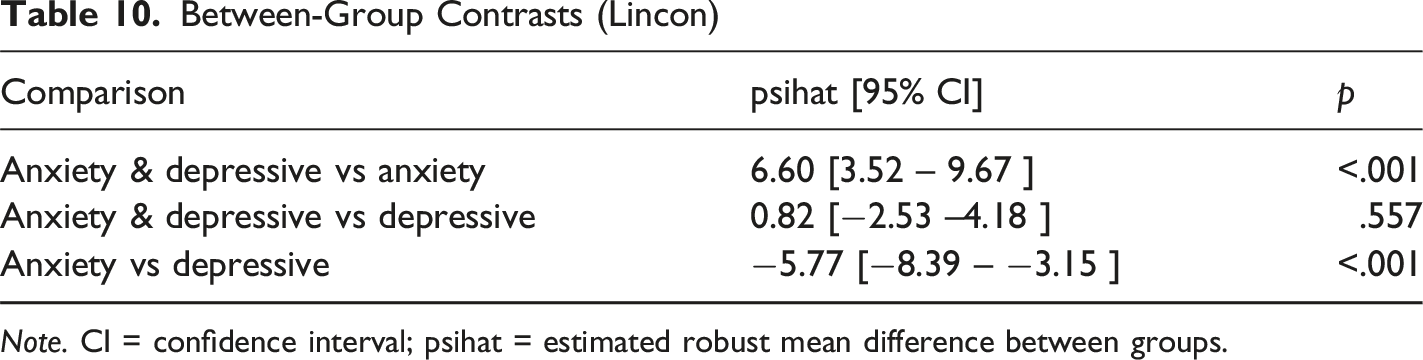
Note. CI = confidence interval; psihat = estimated robust mean difference between groups.
Across all measures, a significant main effect of time emerged, indicating that all diagnostic groups showed a statistically significant reduction in anxiety and depression symptom severity (PHQ-9, GAD-7) as well as in work and social adjustment difficulties (WSAS) following therapy.
For the PHQ-9, both the main effects of time and diagnosis, as well as their interaction, were significant. Post-hoc analyses revealed that, at baseline, patients with comorbid anxiety and depressive disorders and those with depressive disorders alone reported significantly higher symptom severity compared to patients with anxiety disorders only, whereas the two depression-related groups did not significantly differ from each other. The same pattern was observed at post-treatment, although between-group differences were smaller in magnitude, and all three groups, on average, reported scores below the clinical threshold. The within-group reductions were large across diagnoses (effect sizes ranging from 0.66 to 0.72).
For the WSAS, the model showed significant main effects of both time and diagnosis, but no significant time × diagnosis interaction. This suggests that all groups experienced comparable improvement in work and social functioning following therapy. Post-hoc contrasts indicated that participants with comorbid anxiety and depressive disorders and those with depressive disorders alone showed higher functional impairment than those with anxiety disorders, whereas no significant differences emerged between the two depression-related groups. The overall reduction in functional difficulties was statistically significant (effect size = 0.54).
Similarly, for the GAD-7, there were significant main effects of time and diagnosis, but no significant interaction. Participants with comorbid anxiety and depressive disorders reported higher anxiety symptom severity than both single-diagnosis groups, whereas no significant difference was found between anxiety- and depression-only participants. Symptom reduction over time was large (effect size = 0.76).
Overall, these findings indicate that therapy led to substantial and clinically meaningful improvements across all diagnostic groups, with significant reductions in depressive and anxiety symptoms and improved daily functioning. While baseline severity levels varied by diagnosis, treatment effectiveness appeared broadly comparable across groups.
Lastly, the chi-square test assessing the association between diagnostic group and treatment completion status revealed no statistically significant relationship, χ2 (2, N = 442) = 5.33, p = .070.
Discussion
Principal Results
In the present work, we introduce the conceptualization and implementation of the online platform GRETA, contextualized within the Italian landscape, to support CBT-oriented psychotherapy. GRETA facilitates the tracking of therapy progress and the secure archiving of documentation. The evidence-based approach supported by digitalization represents a pioneering advancement in the field of psychotherapeutic services in Italy. A comparable platform has been developed in Italy to support clinical psychology services for children and adolescents (Colombo et al., 2022).
The comprehensive data collected through GRETA’s implementation and the graphical representation of results are in line with the evaluation guidelines for measuring the quality of psychotherapy outlined by national guidelines, such as the U.S. Department of Health and Human Services (Brown et al., 2014). These guidelines highlight the need for quality psychotherapy services to collect data regarding the (a) Capability for delivering evidence-based psychotherapy and measuring outcomes, (b) Access/frequency of visits, (c) Documentation of evidence-based treatments in medical records, (d) Consumer-reported and provider-reported content of psychotherapy, (e) Outcomes reported by consumers, family members, and others. Each of these is collected through GRETA, ensuring the InTherapy psychotherapy service monitors the structure, the process, and the outcome of the therapies provided by clinicians.
Nonetheless, data collection as performed by the GRETA platform is considered mandatory for all National Health Service ― the publicly funded healthcare system in England ― as described in the NHS-TT program (Clark, 2011; Griffiths & Steen, 2013). The data collection performed by the NHS-TT program furnishes a comprehensive nationwide depiction of the utilization of psychotherapy services in England and facilitates various secondary applications, including commissioning, clinical audit, research, service planning, inspection and regulation, monitoring of government policies and legislation, local and national performance management and benchmarking, as well as national reporting and analysis (Clark, 2011; Griffiths & Steen, 2013). Importantly, the GRETA platform is also currently being employed as a research infrastructure to support longitudinal investigations on psychotherapy processes and outcomes, providing standardized data collection across multiple time points and measures (Ocera et al., 2025). Of particular significance is the fact that the InTherapy service, facilitated through the GRETA platform, emerges as the inaugural Italian private therapy service aligning with national guidelines articulated by a healthcare system to ensure the practice adheres to evidence-based principles.
It is worth noting that the acceptance and utilization of telepsychology services from the client’s perspective are strongly correlated with the perceived advantages and barriers of telepsychology, the perceptions of usefulness, and the subject’s behavioral intention, as depicted in the Unified Theory of Acceptance and Use of Technology (Sora et al., 2021; Venkatesh et al., 2003). Therefore, patients encountering obstacles in utilizing technology should receive support from clinicians to optimize their engagement with the platform (Venkatesh et al., 2003). In our service, this assurance is achieved through the interactive utilization of GRETA, complemented by therapy sessions conducted by clinicians, facilitating a triadic dialogue involving the patient, therapist, and the platform. It is worth noting that the attrition rate of 3.7% observed in our patient sample is lower than what is depicted by a recent work focusing on digital mental health apps and software-based solutions (Nwosu et al., 2022).
Pre-post Treatment Analyses
The pre-post treatment analyses further corroborate the effectiveness of the therapeutic interventions delivered within the GRETA platform. Across all diagnostic groups, statistically significant improvements were observed in anxiety and depression symptom severity, as well as in psychosocial functioning, as measured by the PHQ-9, GAD-7, and WSAS scales, indicating that the platform-supported CBT interventions were effective in producing clinically meaningful changes. Notably, while patients presenting comorbid anxiety and depressive disorders exhibited higher baseline symptom severity, all diagnostic groups achieved post-treatment scores below clinical thresholds, underscoring the generalizable benefit of CBT interventions supported by GRETA.
These results align with international findings from large-scale outcome monitoring systems such as the NHS-TT program (Clark, 2011; Clark et al., 2018), highlighting that systematic data collection and digital integration can enhance both the transparency and the clinical quality of psychotherapy services.
Specifically, the temporal contrasts performed within each diagnostic group revealed large pre-to post-treatment improvements across all groups; these are consistent with those reported in the NHS-TT meta-analysis by Wakefield et al. (2021), which found large effect sizes for reductions in anxiety (GAD-7, d = 0.80) and depression (PHQ-9, d = 0.78), and a moderate effect for functional impairment (WSAS, d = 0.54), in patients that were discharged for any reason. Similarly, in our sample, Yuen’s tests indicated large within-group improvements across all diagnostic categories for both depressive (PHQ-9, ξ = 0.66-0.72) and anxiety symptoms (GAD-7, ξ = 0.76), and moderate improvements in functional impairment (WSAS, ξ = 0.54). , suggesting that treatment effectiveness in the Italian inTHERAPY program is comparable in magnitude to that observed in the English NHS-TT system. However, it is important to note that the estimates in the present study were derived using a robust ANOVA approach based on trimmed means, which differs from the conventional parametric methods typically employed in meta-analytic effect size calculations.
Limitations
Some potential limitations that should be considered include the following. First, our study primarily focuses on the implementation and outcomes of the GRETA platform within the Italian landscape. It’s crucial to acknowledge that the findings and effectiveness of the platform may not be directly generalizable to other cultural contexts, healthcare systems, or languages. Nonetheless, the demographics, socioeconomic status, and technology literacy of the individuals who engaged with GRETA might introduce bias, limiting the external validity of the results. Indeed, the acceptance of GRETA use depends on users’ access to technology and their digital literacy.
Further Developments
The contemporary digitalization landscape in psychotherapy research and clinical practice is also witnessing a progressive integration of Artificial Intelligence (AI), particularly predictive Machine Learning (ML), which offers unprecedented opportunities to gain relevant insights into the psychotherapy process (Aafjes-van Doorn et al., 2021; Delgadillo, 2021). AI refers to the field of computer science that aims to create systems capable of performing tasks that typically require human intelligence, such as problem-solving, decision-making, and learning. ML, a subset of AI, focuses on the development of algorithms that enable computers to learn and adapt from data, improving their performance and accuracy over time (Briganti & Le Moine, 2020).
The integration of ML predictive models within a digital platform such as GRETA would offer promising opportunities for improving the assessment and treatment of psychopathology; however, a robust computational psychotherapy framework is yet to be developed to fully realize their potential (Briganti & Le Moine, 2020; Imel et al., 2015). Therapists using GRETA for collecting information regarding their patients could benefit from online predictions regarding probable events within therapy, such as possible early dropouts (Bennemann et al., 2022): once initial clinical and socio-demographic information characterizing the patient is collected through the platform, the integration of AI models could provide alert systems regarding potential early dropouts, through the selected predictive ML models. This integration would allow for real-time analysis of patient data, enabling the platform to recognize patterns or indicators that may signify a heightened risk of premature termination of therapy (Giesemann et al., 2023).
Consequently, therapists could adapt their approaches, offering more targeted and personalized interventions to address the specific needs or challenges that might contribute to the risk of early dropout. This proactive adjustment of therapeutic strategies could target modifiable factors such as motivation, treatment expectations, and practical barriers (Cooper et al., 2023).
Conclusions
The present work introduced the GRETA platform, an innovative online tool designed to support CBT-oriented psychotherapy within the Italian context. The present framework is aligned with healthcare services national guidelines, contributing to a pioneering Italian private evidence-based therapy service. The future integration of predictive ML models within platforms like GRETA holds promise for enhancing the assessment and treatment of psychopathology, paving the way for more personalized and effective therapeutic interventions.
Footnotes
Ethical Considerations
The study was conducted in accordance with the Declaration of Helsinki and was approved by the Ethics Committee of the Faculty of Psychotherapy Science and the Faculty of Psychology of the Sigmund Freud University, Wien (approval no. CCZCDCLBBYBCBK90688) on February 22, 2024, with the need for written informed consent waived.
Author Contributions
Conceptualization: SG and GC; Data curation: SG, IN, RP, MF; Methodology: GMR, SS; Project administration: GC, IN, GMR, SS; Software: IN; Supervision: GC; Visualization: SG, AO, IN; Writing - original draft: SG, AO, LT; Writing - review & editing: GC.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data sharing is not applicable to this article as no datasets were generated or analyzed during the current study.