
Abstract
A recent trial in older adults with anxiety symptoms in primary care found no differences in outcome between an ACT and CBT intervention. The current study aimed to identify moderators and non-specific predictors of treatment response to these two interventions. The sample consisted of 314 older adults who were randomized to either ACT or CBT. Anxiety symptom severity (measured with the GAD-7) was the main outcome variable. Demographics, (psycho)pathology, social support, and psychological processes were examined as predictors. No moderator variables were identified. More severe anxiety and depression symptoms at baseline predicted a worse short- and long-term response to ACT and CBT, while higher levels of mastery predicted a better short-term treatment response in both conditions. When interpreting these results, the lack of sufficient statistical power to detect multiple modest interaction effects should be taken into account. Based on the results of the present study, it is not possible to allocate patients to the intervention that is likely to be most effective for them. The prognostic effects of anxiety and depression symptom severity and mastery may hold implications regarding treatment enhancement strategies in general. The study was registered in the Netherlands Trial Register (NL6131; NTR6270).
Keywords
Introduction
Anxiety disorders and symptoms are one of the most prevalent mental health issues in older adults and are associated with considerable distress and impairment (Grenier et al., 2011; Simning & Seplaki, 2020; Volkert et al., 2012). Although anxiety in later life has received an increasing amount of scientific attention over the last decades, the literature on psychological treatment for older adults with anxiety symptoms is still limited and mainly focused on the evaluation of face-to-face cognitive behavioral therapy (CBT) (Dworschak et al., 2022; Gorenstein & Papp, 2007; Gould et al., 2012). To broaden the scope of this field of research and advance treatment of anxiety symptoms in later life, we conducted a randomized controlled trial (RCT) to evaluate the short- and long-term effectiveness of Acceptance and Commitment Therapy (ACT) in a sample of older adults with anxiety symptoms (Witlox et al., 2021). ACT is a behavior therapy that promotes an acceptance-based attitude towards (negative) feelings and thoughts and stimulates people to (re)connect with their core values and act in accordance with these (Hayes, 2004). In the RCT, a blended ACT intervention (i.e., online ACT in combination with face-to-face support) was compared to face-to-face CBT only, which could be regarded as treatment-as-usual in the study setting (Witlox et al., 2021). We found no differences in the effectiveness of ACT and CBT on anxiety symptom severity at posttreatment and one-year follow-up (cp. Sun et al., 2024). Examining the within-group effect sizes, both groups demonstrated a substantial and statistically significant decline in anxiety symptom severity from baseline to posttreatment. This decrease was sustained one year after baseline in both conditions (Witlox et al., 2021).
Building on our previous RCT, the current study aims to refine our understanding of treatment response by identifying treatment moderators. By examining baseline characteristics that differentially predict response to ACT versus CBT, we aim to provide clinically relevant insights that could guide treatment selection (Kraemer et al., 2002). In addition to studying moderators, we also seek to identify non-specific predictors—variables that predict treatment response regardless of treatment type—to improve prognostic assessment and clarify which patients are more or less likely to benefit from therapy in general.
To our knowledge, moderators and non-specific predictors of treatment response, specifically to ACT and CBT for anxiety, have not yet been studied in an older population. In contrast, in younger adults such predictors have been examined in two studies, both using data from a trial that compared face-to-face ACT and CBT in a sample of 121 adults (maximum age of 60 years, mean age of 37.93 years (SD = 11.79)) with mixed principal anxiety disorder diagnoses (Davies et al., 2015; Wolitzky-Taylor et al., 2012). ACT was found to be the optimal treatment (in terms of anxiety symptom improvement) for patients with a comorbid mood disorder at baseline, while CBT outperformed ACT among patients without a comorbid mood disorder. Furthermore, for the participants with moderate baseline levels of anxiety sensitivity, CBT outperformed ACT (Davies et al., 2015). Behavioral avoidance (operationalized as the unwillingness to endure physical sensations caused by a hyperventilation task) also moderated treatment effect: patients with higher baseline levels of behavioral avoidance benefited more from ACT than CBT (Wolitzky-Taylor et al., 2012). Neuroticism and heart rate variability were identified as non-specific predictors, with higher baseline levels being associated with poorer outcomes in both ACT and CBT (Davies et al., 2015; Wolitzky-Taylor et al., 2012).
While these findings provide valuable insights into treatment response in younger adults, it remains unclear whether these moderators and non-specific predictors also apply to older adults. A recent systematic review of moderators and non-specific predictors of outcome following various psychological and pharmacological treatments for late-life anxiety identified thirteen studies examining 49 predictors or moderators (Kyriacou et al., 2023). Most studies focused on CBT (n = 11) and targeted Generalized Anxiety Disorders (n = 8). Although 23 of the 49 non-specific predictors or moderators measured at posttreatment and 14 of the 33 non-specific predictors or moderators measured at follow-up were statistically significant, only one non-specific predictor — baseline worry severity —predicted treatment outcome in late-life anxiety disorder in three or more studies. Moreover, in examining predictors of treatment outcomes in older adults for psychological treatments addressing common mental health problems in general, another recent meta-analysis identified 42 studies, of which seventy-one percent investigated the efficacy of cognitive-behavioral therapy (CBT), with most studies focusing on depression and anxiety. In these studies, 28 factors were identified as significant predictors of treatment outcomes in at least one study (Schmidt et al., 2024). Homework completion consistently predicted a positive treatment outcome, whereas higher baseline symptom severity often predicted a worse treatment outcome, irrespective of the condition. Additionally, for most predictors, the evidence was mixed or inconclusive, requiring replication.
The demographic, (psycho)pathology, social support, and psychological factors examined in the present study as moderators and non-specific predictors show substantial overlap with significant variables as investigated in previous studies and included in the meta-analyses of Kyriacou et al. (2023) and Schmidt et al. (2024). As previous studies on treatment outcome predictors in older adults examined relatively few psychological processes, we measured psychological processes in more detail. More specifically, we aimed to assess those psychological processes at the start of treatment that are specifically targeted in ACT. Several recent systematic reviews and meta-analyses on the working mechanisms of ACT have concluded that changes in constructs related to the acceptance of inner experiences are associated with outcome, but that strong causal evidence is lacking (e.g., Johanssen et al., 2022; Stockton et al., 2019). Accordingly, we assessed the level of mindfulness, the endorsement of experiential avoidance, and the use of strategies to cope with inner experiences (such as self-blame, rumination, and catastrophizing). We did so as these variables may also be putative moderator variables, allowing differential treatment allocation.
In sum, in the current study, we will examine moderators of short-term and long-term treatment response to blended ACT and face-to-face CBT for older adults with anxiety symptoms. Secondly, we are also interested in non-specific predictors of treatment response to the two interventions. Since there is no solid body of scientific literature to inform hypotheses about putative moderators and non-specific predictors of treatment response to ACT and CBT for anxiety symptoms in later life, we will use an exploratory approach and include a broad selection of demographic and clinical baseline variables.
Methods
This study utilized data from a cluster-randomized, single-blind, controlled trial conducted in the Netherlands. The trial evaluated the effectiveness of a brief blended ACT intervention compared to brief face-to-face CBT over 12 months. Randomization occurred at the level of the therapists participating in the study (n = 40), and consequently, they either provided only blended ACT (n = 20) or only CBT (n = 20) to the study participants. Details about the study design and methods have been published elsewhere (Witlox et al., 2018). The trial was registered in the Netherlands Trial Register (NL6131 (NTR6270)) and approved by the medical ethics committee of Leiden University Medical Center (LUMC; no. P16.248).
Participants and Procedure
Between November 2017 and March 2019, participants were recruited in 38 general practices in the Netherlands. Patients aged 55– 75 from the participating general practices were sent a letter containing information about the study and an invitation to participate. Those interested in participation could register on a study website, after which they entered a screening procedure. Inclusion criteria were: age between 55 and 75 years, presence of mild to moderate anxiety symptoms (score between 5 and 15 on the Generalized Anxiety Disorder-7 (GAD-7; Spitzer et al., 2006), mastery of the Dutch language, internet access, and the possibility to spend up to 30 min per day on the intervention. Exclusion criteria were: unstable severe medical condition(s); severe cognitive impairment; very high or low anxiety symptom severity (GAD-7 score <5/> 15); severe depressive symptoms, score ≥20 on the Patient Health Questionnaire (PHQ-9; Kroenke et al., 2001); psychological or psychopharmacological treatment (stable benzodiazepine or SSRI use excepted) within the last three months; severe role impairment in at least two life areas (score of ≥8 on two or three items of the Sheehan Disability Scale (SDS; Leon et al., 1997); high suicide risk (M.I.N.I.-Plus; Lecrubier et al., 2020); substance use disorder (M.I.N.I.-Plus); lifetime diagnosis of bipolar disorder or schizophrenia (medical record and M.I.N.I.-Plus). Eligible participants signed an online informed consent form and finalized the baseline assessment, after which they were informed about their treatment allocation. Participants completed four main assessments: at baseline (T0), posttreatment (T1; three months after baseline), 6 months after baseline (T2), and 12 months after baseline (T3). In the current study, we will analyze the direct outcome of treatments at the end of treatment (T1) and the long-term maintenance of outcome at the latest follow-up assessment (T3). The assessments included online self-report questionnaires and a telephone interview conducted by trained and supervised research assistants who were masked to randomization.
Interventions
Therapists
Mental health counselors provided therapy. Around 2008, general practices in the Netherlands started employing mental health counselors in response to the increasing demand for treatment of psychological problems and the high costs and limited capacity of mental health care institutions (OECD, 2014). The counselors provide short-term psychological treatment to patients with mild to moderately severe psychological complaints. In the present study, most counselors were master’s graduates in psychology (n = 13), social psychiatric nurses (n = 14), or social workers (n = 5). Years of experience in providing individual psychological treatment ranged from three to 42, with a median of sixteen years.
Blended Acceptance and Commitment Therapy
Participants in the Blended ACT condition completed the online ACT module ‘Living to the Full’ (Bohlmeijer & Hulsbergen, 2008, 2015) and attended four face-to-face sessions with the mental health counselor at their general practice. The module comprises nine lessons that revolve around the six core processes of ACT: acceptance, cognitive defusion, contact with the present moment, self-as-context, personal values, and committed action. Participants completed the module in eight to twelve weeks, which required them to spend 15-30 minutes on the online module each day. The four face-to-face sessions with the mental health counselor were based on a protocol developed by the authors of Living to the Full and served to increase motivation, repeat key exercises, and discuss problems that arose while working with the module.
Cognitive Behavioral Therapy
Participants in the CBT condition attended four face-to-face sessions and completed homework exercises as part of their treatment. The sessions took place over a timespan of eight to twelve weeks. A treatment protocol was developed (by authors N.G., M.W., V.K., and P.S.) that focused on identifying and challenging negative cognitions and reducing anxiety-related avoidance behavior. Furthermore, it contained information and exercises related to specific types of anxiety (panic, worrying, social anxiety) and common side effects of anxiety (sleeping problems, physical tension). After the intake session, the counselor and client collaboratively set treatment goals. In the second and third sessions, homework was evaluated, key exercises/information were repeated, and the counselor and participant agreed on a plan regarding homework exercises for the succeeding weeks. The last session was dedicated to evaluating the client’s progress and formulating a relapse prevention plan.
Measurements
Outcome Variable
Anxiety Symptom Severity at T1 and T3
Anxiety symptom severity at T1 and T3 was assessed with the GAD-7, a widely used seven-item anxiety screener with good psychometric properties (Spitzer et al., 2006). Total scores range from 0 to 21, with higher scores reflecting more severe anxiety symptoms in the last two weeks. The Cronbach’s alpha values for the GAD-7 in the current study sample at Time 1 (T1) and Time 3 (T3) were 0.86 and 0.87, respectively.
Predictor Variables
All predictor variables were assessed during the baseline measurement.
Domain 1: Demographics
Age, gender, romantic relationship status, educational level, and weekly work hours (both paid and voluntary) were assessed using a self-developed questionnaire. Recent negative life events were assessed with a self-developed yes/no question: “In the past 6 months, did you experience one or more major negative events?”. Participants who responded ‘yes’ could describe the event in a textbox.
Domain 2: (Psycho)pathology
Anxiety Symptom Severity
Anxiety symptom severity at T0 was measured with the GAD-7 (Spitzer et al., 2006). Cronbach’s alpha for the GAD-7 at T0 in the current study sample was 0.78.
Depression Symptom Severity
Depression symptom severity was measured with the PHQ-9 (Kroenke et al., 2001), a nine-item self-report questionnaire with good psychometric properties. Total scores range from 0 to 27, with higher scores indicating higher symptom severity in the previous two weeks. Cronbach’s alpha for the PHQ-9 in the current sample was 0.73.
Presence of Anxiety Disorder
Trained research assistants conducted the Mini-International Neuropsychiatric Interview (Lecubrier et al., 2020) by phone to assess the presence of generalized anxiety disorder, panic disorder, agoraphobia, specific phobia, social phobia, obsessive-compulsive disorder, posttraumatic stress disorder, and illness anxiety disorder.
Psychiatric Medication Use
Participants completed a yes/no question to indicate if they had used benzodiazepines and/or SSRIs during the preceding three months.
Somatic Problems
Physical problems in the previous year were assessed using a self-developed checklist, which listed the 25 most common (chronic) medical conditions, according to Statistics Netherlands. Participants could also report somatic problems they experienced that were not included in the checklist.
Domain 3: Social Support
Affective Social Support and Problem-Solving Social Support
Bovier et al. (2002) developed a 14-item questionnaire to measure social support and psychological resources. The questionnaire consists of four scales, of which one measures affective social support (the availability of people who express emotional involvement with and care for the participant during challenging situations; 2 items) and another problem-solving social support (the availability of people one can confide in and receive advice from when challenging situations occur; 4 items). Items are answered on a scale ranging from 0 to 4, and higher scores on each subscale represent higher levels of the measured construct. All four scales have proper psychometric properties (Bovier et al., 2002). In the current study sample, Cronbach’s alpha values were 0.87 for affective social support and 0.83 for problem-solving social support.
Domain 4: Psychological Processes
Self-Esteem and Mastery
The other two subscales of the 14-item questionnaire of Bovier et al. (2002) mentioned above were used to measure self-esteem (defined as one’s overall sense of worthiness as a person; 4 items), and mastery (people’s belief that their life’s course is under their own control in contrast to being fatalistically ruled; 4 items). In the current study sample, Cronbach’s alpha values were 0.76 for self-esteem and 0.78 for mastery.
Experiential Avoidance
The Acceptance and Action Questionnaire-II (AAQ-II) is a validated unidimensional measure (Jacobs et al., 2008) that assesses experiential avoidance. Experiential avoidance is a key concept in ACT. It refers to the unwillingness to remain in contact with aversive private experience and the behaviors aimed at altering these experiences or the events that elicit them (Jacobs et al., 2008). AAQ items are scored on a 7-point scale, with total scores ranging from 7 to 49, where higher scores indicate higher levels of experiential avoidance. Cronbach’s alpha for the AAQ-II at T0 in the current study sample was 0.87.
Mindfulness Facets
The Five Facet Mindfulness Questionnaire-Short Form (FFMQ-SF) was used to assess mindfulness, defined as the ability to bring one’s attention to experiences in the present moment in a nonjudgmental manner (Bohlmeier et al., 2011). The questionnaire comprises 24 6-point items (ranging from 0 to 5) that measure five facets of mindfulness: observing (4 items), describing (5 items), acting with awareness (5 items), non-judging (5 items), and non-reactivity (5 items). The sum score of all items reflects the level of mindfulness, with higher scores indicative of higher levels. The questionnaire has good psychometric properties (Bohlmeier et al., 2011). In the present study, we used the total scale score to measure an individual’s level of mindfulness, thereby restricting the number of predictive variables in our statistical analyses. Cronbach’s alpha for the FFMQ-SF at T0 in the current study sample was 0.69.
Cognitive Emotion Regulation Strategies
The participants completed the following four subscales of the Cognitive Emotion Regulation Questionnaire (CERQ) (Garnefski & Kraaij, 2007) deemed most relevant for measuring psychological processes underlying the effectiveness of ACT: (1) self-blame, referring to thoughts of putting the blame of what you have experienced on yourself, (2) rumination, referring to thinking about the feelings and thoughts associated with a negative event (3) positive reappraisal, referring to thoughts of giving a negative event a positive meaning in terms of personal growth and (4) catastrophizing, referring to thoughts of explicitly emphasizing the terror of what you have experienced. To reduce the number of independent variables, the subscales of other-blame, putting into perspective, positive refocusing, acceptance, and planning were excluded. We also did not include the subscale ‘acceptance’ as the items of this CERQ subscale primarily relate to thoughts of resigning oneself to what has happened (e.g., ‘I think that I have to accept the situation’). However, accepting subjective experiences (instead of circumstances) without trying to alter them is more relevant for ACT and the FFMQ measuring mindfulness better captures this aspect of acceptance. The subscales consist of four 5-point items each, with total scores for each scale ranging between 0 and 16. Higher scores on a subscale indicate that this cognitive coping strategy is more often used to regulate emotions. The CERQ has good psychometric qualities (Garnefski & Kraaij, 2007). Cronbach’s alpha values for the four selected subscales in the current study sample were as follows: α = 0.79 for self-blame, α = 0.77 for rumination, α = 0.86 for positive reappraisal, and α = 0.82 for catastrophizing.
Statistical Analysis
All analyses were performed using the R statistical software environment (R Foundation for Statistical Computing, 2020). Analyses followed the intention-to-treat principle, which necessitated the imputation of missing data. We used Multiple Imputation by Chained Equations (MICE), with the predictive mean matching procedure, in which the missing outcome of a participant is imputed with the observed outcome from another participant with a comparable predicted mean outcome. This procedure guarantees that the imputed data have plausible values (van Buuren, 2012). A total of 100 imputed datasets were analyzed, and their results were combined to yield the presented estimates.
Analyses were conducted separately for short-term (T0-T1) and long-term (T0-T3) treatment response. To identify moderators and non-specific predictors, we used a domain approach similar to the one outlined by Fournier et al. (2008) and more recently by Huibers et al. (2016). Continuous variables were standardized, and categorical variables were effect-coded. First, we grouped the predictors in four domains (i.e., demographics, (psycho)pathology, social support, and psychological processes). To prevent excessive multiple testing, we conducted omnibus tests to compare the fits of three nested models within each domain: a simple model (regressing GAD-7 end-score on baseline GAD-7 score and treatment condition), an additive model (adding main effects of all the predictors in the domain) and a full prediction model (also adding interaction terms between treatment condition and each predictor in the domain). Using the Wald test, we examined whether the full prediction model provided a significantly better fit to the data than the simple and additive models (α = 0.05). If the omnibus tests indicated that the full domain model had a superior fit, we used a stepwise procedure to identify the prescriptive and prognostic variables within that domain. In step 1, the full prediction model was inspected, and variables significant at a threshold of α = 0.2 were selected and combined into a new model. If an interaction between a predictor variable and the treatment variable fell below the significance threshold, the main effect of the predictor was carried through to the next step, irrespective of it being significant itself (maintaining the principle of marginality). The main effects of baseline anxiety symptom severity and treatment condition were always carried through to the next step, irrespective of their statistical significance. In step 2, the second model was examined, and the same process was applied using a stricter threshold value of α = 0.1. In Step 3, the same process was repeated, but with a threshold of α = 0.05.
In domains where the full prediction model did not provide a superior fit, but the additive fit the data better than the simple model, we used the same procedure, but only aimed at identifying non-specific predictors. We build a final prediction model that combines the variables from all domains that were significant at the 0.05 level in the third step of the domain-specific analyses. The variables that remained significant at the 0.05 level in this final model were considered moderators and/or non-specific predictors.
Results
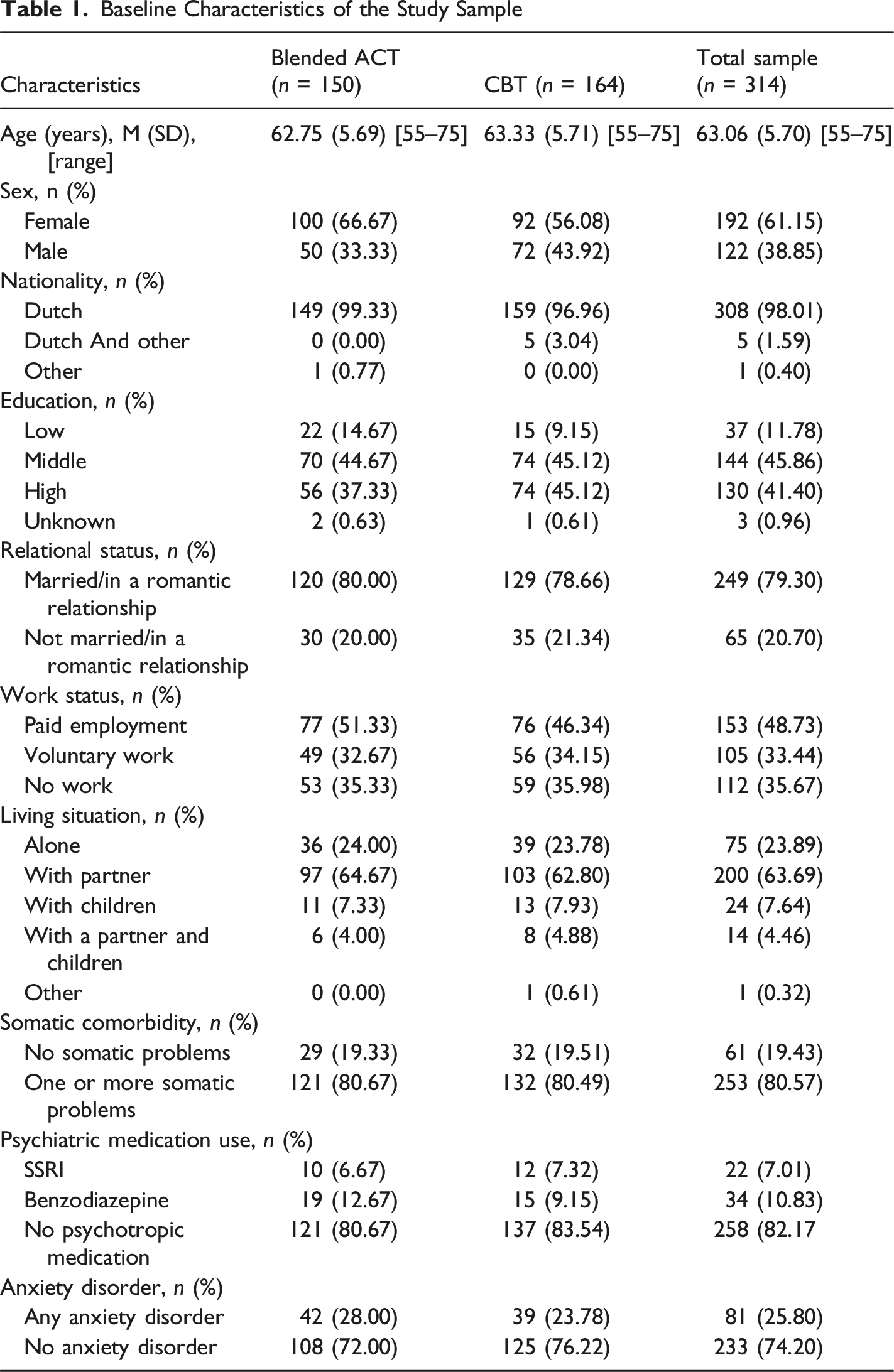
Baseline Characteristics of the Study Sample
Moderators
Results of the Omnibus Tests Comparing Domain-specific Simple, Additive, and Full Prediction Models
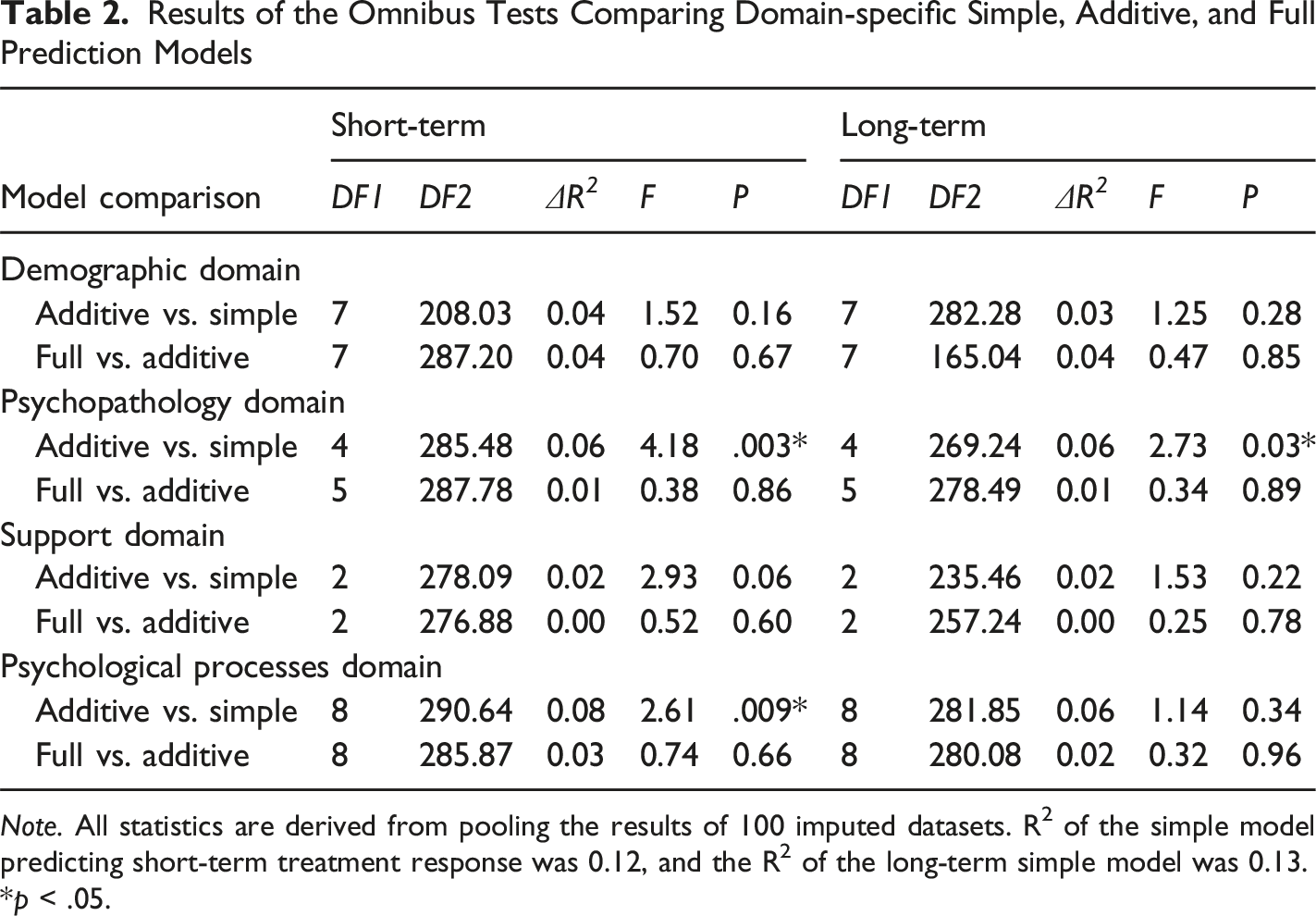
Note. All statistics are derived from pooling the results of 100 imputed datasets. R2 of the simple model predicting short-term treatment response was 0.12, and the R2 of the long-term simple model was 0.13.
*p < .05.
Non-Specific Predictors
Short-Term Treatment Response
Stepwise Inspection of Non-specific Predictors of Short-Term Treatment Response: (psycho)pathology Domain
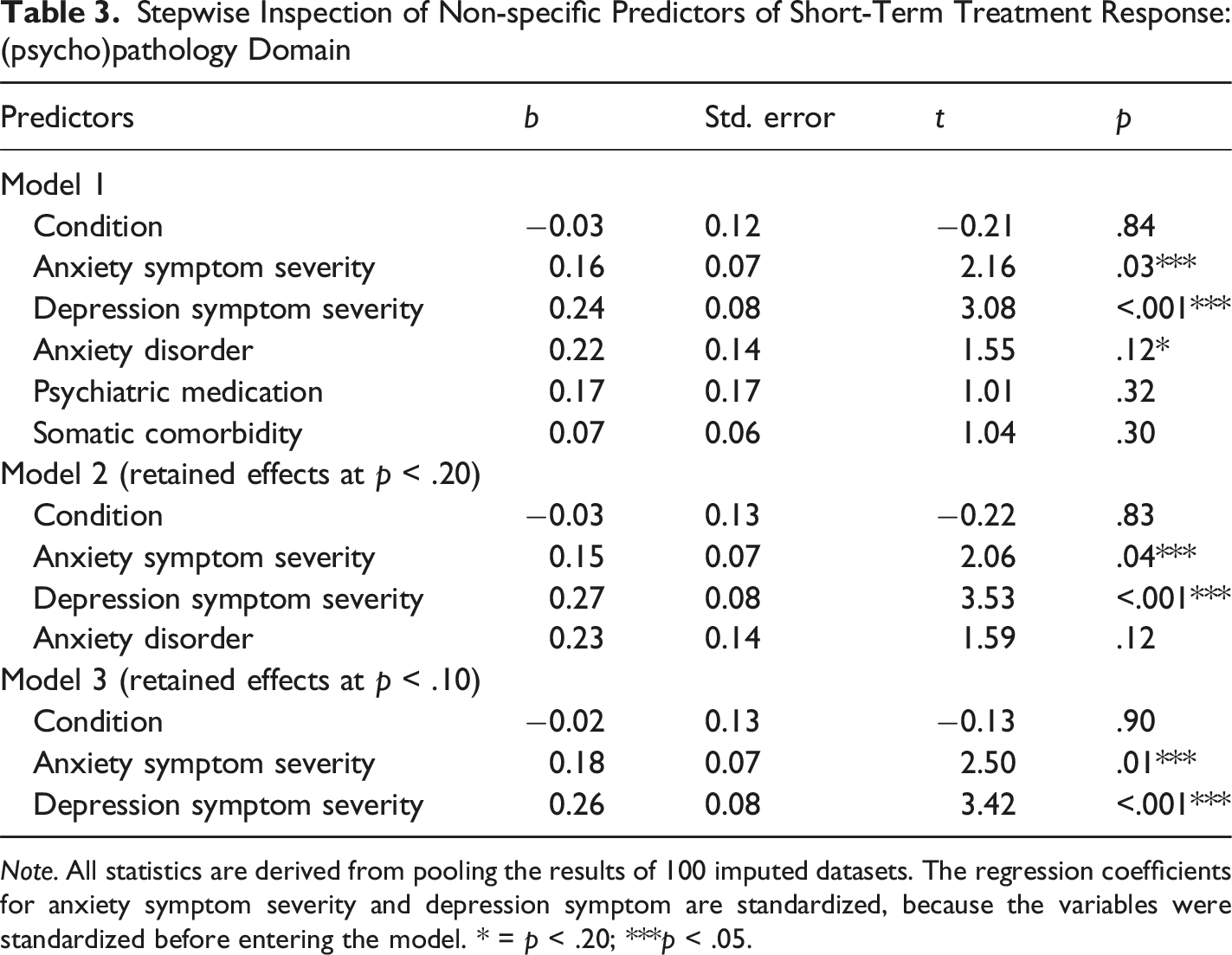
Note. All statistics are derived from pooling the results of 100 imputed datasets. The regression coefficients for anxiety symptom severity and depression symptom are standardized, because the variables were standardized before entering the model. * = p < .20; ***p < .05.
Stepwise Inspection of Non-specific Predictors of Short-Term Treatment Response: Psychological Processes Domain
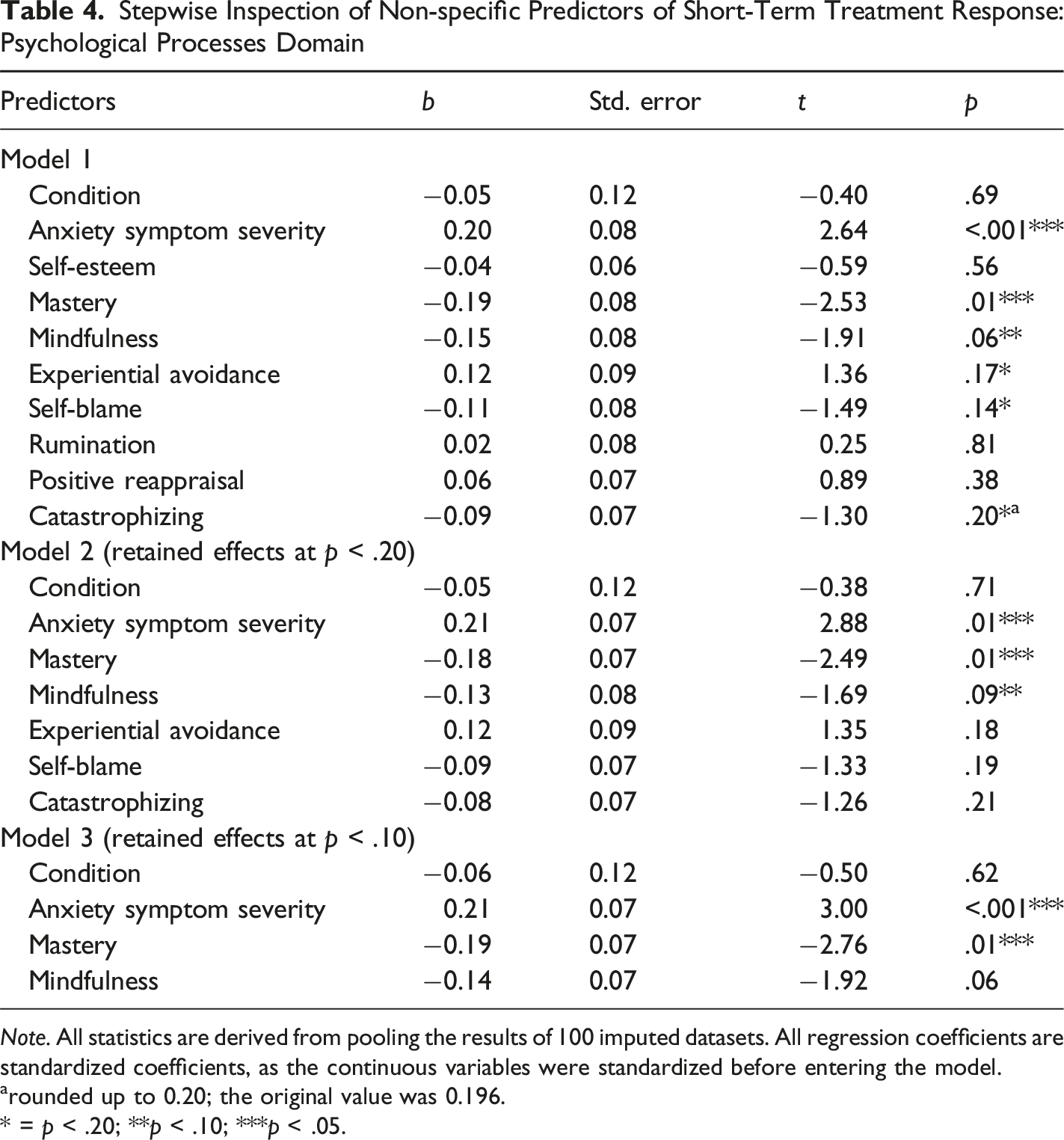
Note. All statistics are derived from pooling the results of 100 imputed datasets. All regression coefficients are standardized coefficients, as the continuous variables were standardized before entering the model.
arounded up to 0.20; the original value was 0.196.
* = p < .20; **p < .10; ***p < .05.
Long-Term Treatment Response
Stepwise Inspection of Non-specific Predictors of Long-Term Treatment Response: (psycho)pathology Domain
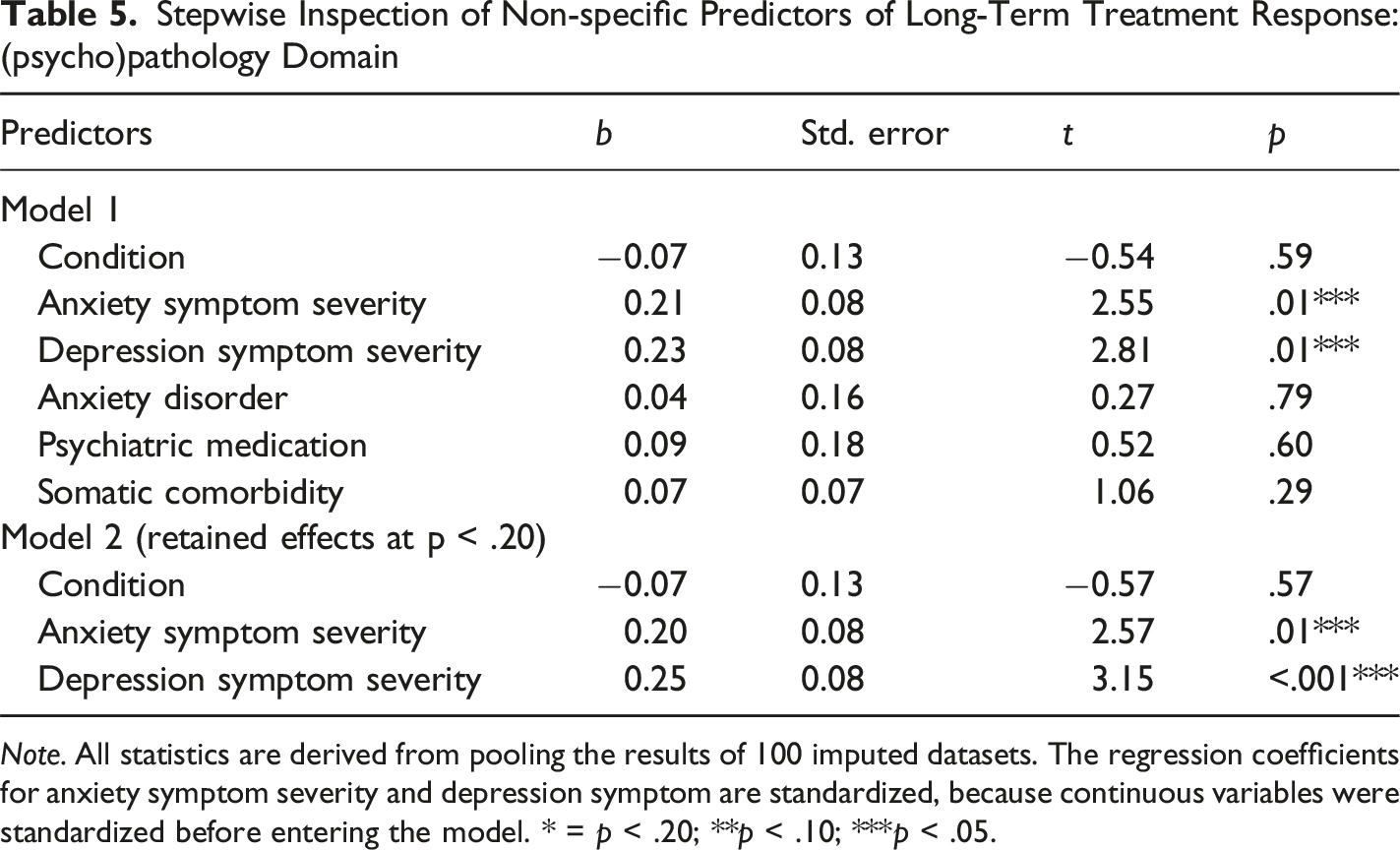
Note. All statistics are derived from pooling the results of 100 imputed datasets. The regression coefficients for anxiety symptom severity and depression symptom are standardized, because continuous variables were standardized before entering the model. * = p < .20; **p < .10; ***p < .05.
Discussion
This study examined predictors of short-term and long-term treatment response to a blended ACT intervention vs. a face-to-face CBT intervention in older adults with anxiety symptoms. These two brief interventions were previously found to be equally effective for this patient population (Witlox et al., 2021). We were primarily interested in identifying moderator variables, as insight into how ACT and CBT differentially affect specific subgroups of patients could inform evidence-based personalized treatment assignment. However, we did not identify any moderators of treatment response to either the blended ACT intervention or the CBT intervention.
The secondary aim of this study was to identify non-specific predictors of treatment response. These predictors provide prognostic information about which subgroups of anxious older adults are likely to respond more or less favorably to treatment, irrespective of the treatment being the ACT or the CBT intervention. Three non-specific predictors were identified. First, more severe anxiety symptoms, as well as depression symptoms at baseline, were found to be predictive of poorer short-term and long-term treatment response to both the ACT and CBT interventions. Second, baseline mastery levels were predictive of short-term treatment response, with higher levels being associated with more favorable responses in both treatment conditions.
Regarding baseline anxiety symptom severity, our results are in line with the findings of two recent meta-analyses (Kyriacou et al., 2023; Schmidt et al., 2024) showing that several predictors which are related to baseline anxiety symptom severity, including worry severity, state-anxiety severity, anxiety severity, and GAD severity, were primarily but not uniformly related to outcome with participants with higher anxiety levels at baseline manifesting higher anxiety levels after treatment. Regarding baseline depression symptom severity, earlier studies into the prescriptive and prognostic effects of comorbid depression on treatment response in anxious patients present mixed findings. Some studies found comorbid baseline depression to be associated with worse anxiety outcomes across different treatments (Chambless et al., 1997, 2000; Steketee et al., 2001; Watanabe et al., 2010), while others found that it did not predict posttreatment anxiety severity (Balkom et al., 2008; Kampman et al., 2008; Rief et al., 2000; Schuurmans et al., 2009). In the study from Wolitzky-Taylor and colleagues (2012), depressive comorbidity was found to be a moderator of treatment response. Patients with a comorbid depressive disorder responded better to ACT than CBT, which the authors ascribed to ACT being a more transdiagnostic treatment that targets psychological constructs related to both anxiety and depression. Considering the mixed findings so far, more research into how comorbid depressive symptoms are associated with treatment response in anxious patients is indicated. Ultimately, these studies could inform clinical practice on whether and how the subgroup of anxious patients with comorbid depression (symptoms) could benefit from additional/adapted treatments.
Mastery, the other prognostic variable identified in this study, is part of a set of closely connected psychological constructs (a.o., locus of control, self-efficacy) that are all related to one’s perceived control over situations or events (Ly et al., 2019). Perceived control variables have been examined in the context of psychological treatment. Higher baseline values of different measures have repeatedly been demonstrated to be related to more favorable treatment outcomes across a broad spectrum of psychological conditions (including anxiety) and treatments (Borkovec & Costello, 1993; Chambless et al., 1997; Price et al., 2008; Safren et al., 1997; Sotsky et al., 1991). People with higher levels of perceived control show increased task motivation and stronger intentions to complete planned behaviors, and also demonstrate more effort and persistence when faced with obstacles or adversity (Bandura et al., 1982; Maddux et al., 1982). In a psychotherapy setting, this might translate into an increased ability and motivation to actively engage with the treatment, thereby improving treatment outcomes.
Besides mastery, none of the other psychological processes studied proved to be independently predictive of anxiety reduction. The fact that psychological variables such as mindfulness, experiential avoidance, and emotion regulation at baseline failed to show incremental predictive value for anxiety at posttreatment or follow-up on top of anxiety levels at baseline, however, does not imply that these factors are not possible predictors of treatment outcome (Kraemer et al., 2001). Statistically controlling for symptom severity may over-adjust for the role of putative mechanisms in the reduction of anxiety and remove constituent components from the predictors themselves, e.g., the worry component in mindfulness, experiential avoidance, and emotion regulation. Symptom severity and psychological processes show a high degree of convergence, and systematically controlling for symptom severity may result in mutilated psychological constructs (Struijs et al., 2021). Future studies must be more attentive to possible shared components that can help elucidate the relationships with outcome in more detail to prevent throwing out the baby with the bathwater.
Some limitations of the current study have to be discussed. First, like most studies on treatment moderators, the current study was a post-hoc analysis of RCT data, which was not primarily designed to test for treatment moderators. Consequently, the study was underpowered to detect multiple modest interaction effects (McClelland & Judd, 1993). To truly advance evidence-based personalized treatment assignment in mental health care, moderator analyses should be conducted in larger study samples. Adequate statistical power could also be achieved by combining participant-level data from multiple studies using individual patient data (IPD) meta-analyses (Buntrock et al., 2024). Furthermore, studies specifically designed to confirm the moderating effects of variables are essential for the development of decision tools for personalized treatment assignment, but these are currently lacking (Schneider et al., 2015). A second limitation is the absence of a non-active control condition. Because of this, we cannot ascertain whether the identified prognostic effects truly reflect a difference in treatment response between participants, or if individuals scoring higher on mastery and lower on depression severity would have also shown relatively larger symptom improvement without (active) treatment. Third, a substantial number of participants did not complete the post-treatment and/or follow-up measurements, resulting in a considerable amount of missing data. However, we aimed to handle this problem optimally by imputing data using predictive mean matching, which is a well-established imputation method (van Buuren, 2012). Although the use of multiple imputation is preferable even when data are not missing at random and provides important advantages over more common deletion techniques, bias cannot be fully eliminated (Woods et al., 2024) and the high attrition rate limits generalizability. Fourth, the generalizability of the results is limited by the fact that several exclusion criteria were used during participant recruitment for the RCT.
Most importantly, people over 75 years and those with more severe psychological and/or physical conditions were excluded from participation. This reduces the heterogeneity and representability of the study sample. Last, we did not examine interactions between predictor variables, as we already conducted a large number of statistical tests. Therefore, we do not know if the prognostic effects we observed vary as a function of other predictor variables. Examining these more complicated relations between predictor variables is an important task for future studies. Given these limitations, future research, preferably in studies primarily designed to investigate prescriptive and non-specific predictors of treatment outcomes in anxious patients, is needed to replicate and elaborate on these findings.
Clinical Implications
The present randomized controlled trial comparing ACT with CBT in the treatment of anxiety symptoms in older adults shows that mental health counselors in general practice can successfully provide blended ACT and face-to-face CBT to this group of patients. As the present study results did not identify moderators of treatment outcome, it is not possible to allocate patients to the intervention that is likely to be most effective for them based on their pretreatment characteristics. These results suggest that both treatments can be widely applicable and that the choice between blended ACT and face-to-face CBT for anxiety symptoms in later life can be guided by client- and therapist preferences and practical considerations.
Moreover, the prognostic effects of anxiety and depression symptom severity and mastery as non-specific predictors suggest that extra attention is needed for more severe patients and patients who believe to a lesser degree that their life’s course is under their own control. A recent meta-analysis identified self-efficacy-related cognitions concerning one’s ability to cope with threatening situation or sensations as vital mechanisms of therapeutic change (Breuninger et al., 2019). Taken together, this could imply that patients with lower levels of mastery at the outset of treatment might benefit from additional therapeutic strategies to enhance their self-mastery. Enhancing mastery-related cognitions is often an implicit target during psychological treatment. Treatment could be augmented with interventions explicitly targeting mastery-related cognitions. This could be achieved by assigning homework to acquire specific skills and implementing them in daily life. Furthermore, brief and experimental procedures to enhance self-efficacy, such as recalling autobiographical self-efficacy memory episodes, have been developed and tested (Paersch et al., 2021, 2025). Further research is needed to establish if and how mastery-related cognitions can be directly targeted, and whether such treatment enhancement strategies indeed lead to more favorable treatment outcomes.
Footnotes
Ethical Considerations
The study was approved by the Medical Ethics Committee of Leiden University Medical Center (P16.248).
Consent to Participate
Eligible participants signed an informed consent form.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a grant from ZonMw (grant number 531001205).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Trial Registration
The study was registered in the Netherlands Trial Register (NL6131; NTR6270) and approved by the Medical Ethics Committee of Leiden University Medical Center (P16.248).
Data Availability Statement
The authors confirm that all data underlying the findings are fully available without restriction. Because of ethical and legal restrictions, our data involving clinical participants are not freely available in the manuscript, supplemental files, or in a public repository. However, data is available upon request via the first author (