
Abstract
Emotional Intelligence (EI) is associated with adolescent wellbeing, and associations between EI and problem behaviours (internalising and externalising) are also emerging. The incremental validity of EI over wellbeing as a predictor of problem behaviours has received less attention but may offer a more nuanced understanding of the contribution of emotional factors that give rise to problem behaviours. We hypothesised that EI would be predictive of positive wellbeing and negatively related to psychological distress and further that lower emotional awareness and regulation were expected to predict internalising and externalising behaviours. In a sample of 422 adolescents, we conducted linear regressions to examine the relationship between EI scores and subjective wellbeing, eudaimonic wellbeing, and psychological distress. As expected, higher emotional awareness, expression and regulation predicted subjective and eudaimonic wellbeing and was inversely predictive of psychological distress. Hierarchical linear regressions examined if EI and measures of wellbeing and psychological distress predicted problem behaviours while considering differences in gender. Externalising behaviours were predicted by subjective wellbeing and psychological distress, emotional regulation, and gender, while internalising behaviours were predicted by subjective wellbeing and psychological distress, emotional awareness, and emotional regulation. Findings emphasised the relative importance of effective emotional regulation in relation to adolescent wellbeing, psychological distress, and problem behaviours which may have implications for targeted development of EI.
Keywords
Introduction
Adolescence is a developmental stage characterised by significant physical, social and psychological change where the impact of stress and adversity can have negative consequences on mental health, and wellbeing (Sisk & Gee, 2022). The World Health Organisation defines mental health as “a state of mental well-being that enables people to cope with the stresses of life, realize their abilities, learn well and work well, and contribute to their community” (World Health Organization, 2022, p. 7), incorporating both a positive dimension relating psychological wellbeing and a negative dimension encompassing stress. The onset of 62.5% of all mental health issues occur prior to the age of 25 years with the peak age reported to be 14.5 years, highlighting the importance of establishing protective factors and promoting wellbeing and positive psychological adjustment during the crucial developmental period of adolescence (Solmi et al., 2022) and even earlier.
Emotional intelligence (EI) is reported to be positively associated with adolescent subjective and cognitive wellbeing (Llamas-Díaz et al., 2022; Schutte et al., 2007) and negatively related to the experience of psychological distress (Espinosa & Rudenstine, 2020; Kugbey et al., 2018; Slaski & Cartwright, 2002). Psychological distress and poor wellbeing have also been linked to increased engagement in problem behaviours in adolescents (Arslan, 2019). The links between EI and wellbeing have been well established (Schutte et al., 2007), with associations between perceived emotional capabilities and problem behaviours also emerging (Downey et al., 2010; Resurrección et al., 2014), however, the incremental validity of EI over wellbeing as a predictor of problem behaviours has received less attention to date and has been flagged as an important next step for researchers (Martins et al., 2010).
Models of psychological wellbeing are often described from two perspectives; hedonic and eudaimonic (Cooke et al., 2016; Deci & Ryan, 2008; Dodge et al., 2012). Hedonic wellbeing, also referred to as subjective wellbeing, represents a positive subjective assessment of one’s global cognitive and affective states where the experience of positive affect (such as happiness, joy, satisfaction) is greater than the experience of negative affect (such as sadness, fear, disappointment) (Cummins, 2010; Diener et al., 2006; Ryan & Deci, 2001). In contrast, multidimensional concepts of eudaimonic wellbeing move beyond quantifying the extent to which a person feels ‘well’ but seeks to understand factors that influence optimal experience and outcomes for individuals, that ultimately lead to fulfilment of one’s true potential (Ryan & Deci, 2001). While subjective and eudaimonic wellbeing are inherently related, both incorporating positive personal evaluations, they are distinct, as eudaimonic conceptualisations measure other traits and behaviours, with an emphasis on purpose and striving as essential components for wellbeing (Cooke et al., 2016; Deci & Ryan, 2008). For example, Ryff and Keyes (1995) describe a model of eudaimonic wellbeing as a sum of factors that may give rise to positive affect including self-acceptance, personal growth, purpose in life, autonomy, environmental mastery and existence of quality interpersonal relationships, with a focus on components that relate to future goals and achievement.
In adolescents, higher wellbeing has been shown to be associated with outcomes including academic success (Cárdenas et al., 2022), quality parental and peer relationships (Kiuru et al., 2020), better perceived physical health and fewer risky-health behaviours (Hoyt et al., 2012). Conversely, poor wellbeing has been shown to predict a greater incidence of mental health issues and problem behaviours (Lereya et al., 2022; Patalay & Fitzsimons, 2018). While contributors to each of these outcomes are complex and varied, including variable influences from socioeconomic status, gender, family dynamics, environmental factors, school connectedness, self-esteem and cognitive ability (Patalay & Fitzsimons, 2018; Raniti et al., 2022), an underlying mechanism linking these outcomes to wellbeing appears to be self-perceptions of emotional capabilities, particularly aspects that relate to emotional awareness and regulation (Pauletto et al., 2021); abilities encompassed by EI.
EI encompasses emotion-related behaviours and knowledge including the recognition, expression, use and regulation of emotions and emotion-related information, especially in relation to fostering healthy and adaptive functioning (Mayer et al., 2004; Mayer & Salovey, 1995). EI has two prominent models; the ability model which characterises EI as emotion-related competencies and declarative knowledge (Mayer et al., 2004; Mayer & Salovey, 1995; Salovey & Mayer, 1990), and the trait model which describes EI as self-perceived abilities related to emotions, that guide behavioural responses in emotion-related situations (Petrides, 2010; Petrides et al., 2007). Meta-analyses have indicated that EI is a predictor of mental, psychosomatic and health outcomes in adults and adolescents (Martins et al., 2010; Schutte et al., 2007). EI may foster wellbeing and limit psychological distress in a number of ways: through effective emotion regulation facilitating the experience of more positive affect and less rumination in negative emotions (Gómez-Baya & Mendoza, 2018), or providing a basis for fostering positive relationships and obtain social support through authentic and effective communication (Zhao et al., 2020).
With regards to the type of EI model used to examine these relationships with psychological distress and wellbeing, Martins et al. (2010) and Schutte et al. (2007) found that both constructs of EI are predictive of mental, psychosomatic and physical health outcomes, but trait EI tended to be the stronger predictor. In this study, we focus on trait EI, which has been found to be a good predictor of adolescent outcomes (O'Connor et al., 2019) and has shown incremental validity over ability EI in the prediction of specific aspects of adolescent adjustment (Davis & Humphrey, 2012; Di Fabio & Saklofske, 2014).
Gender differences have been observed regarding emotion-related behaviours which may influence wellbeing outcomes. It has been reported that adolescent females score slightly higher on ability EI measures than males but males have higher self-reported EI (D'Amico & Geraci, 2022). Additionally, females have been observed to show more positive emotions and internalising emotions (e.g. anxiety, sympathy) and males showing more externalising emotion (e.g. anger) than females (Chaplin & Aldao, 2013), with cognitive reappraisal as an emotion-regulation strategy being observed more frequently in females compared to males (Zhang et al., 2020). Additional research is required to better understand how gender differences influence the relationship between EI and wellbeing in adolescents, as noted by Llamas-Díaz et al. (2022) that less than one third of research examining adolescent EI and wellbeing controlled for gender despite being a known influence of EI outcomes.
Psychological distress describes both the mental and physical suffering arising from the experience of unpleasant emotions (Horwitz, 2007) which has been associated with undesirable adolescent outcomes including poor academic performance (Rothon et al., 2009), poor physical health (Arbour-Nicitopoulos et al., 2012), and suicidal ideation (Kim, 2021). The experience of psychological distress has in part been attributed to less adaptive emotional regulation in circumstances of adversity, either through lack of regulation strategies or maladaptive coping selection (Schäfer et al., 2017). While psychological distress is highly negatively related with wellbeing, research shows that they are not opposite ends of the same continuum (Lereya et al., 2022; Winefield et al., 2012). This suggests that the examination of both psychological distress and wellbeing is important to properly understand adolescent mental and psychological outcomes, in line with the recommendation that wellbeing research should include multiple measures representing a range of theoretical perspectives (Winefield et al., 2012).
Psychological distress and poor wellbeing have been linked to increased engagement in problem behaviours which are often delineated in two broad categories; internalising and externalising behaviours (Achenbach, 1978; Arslan, 2019). Internalising behaviours are those which are focussed inward and typically manifest through symptoms such as negative affect, social withdrawal and somatic complaints and more severe presentations can lead to mental health issues such as depression and anxiety (Hansen & Jordan, 2020), social difficulties including lower-quality relationships with peer and parents (Luijten et al., 2021), academic problems and school drop-outs or substance abuse (Liu et al., 2011). Externalising behaviours are reflected outward and involve negative acts upon the external environment such as aggression, delinquency, hyperactivity and impulsivity (Liu, 2004). Both internalising and externalising behaviours are observed across the genders although internalising behaviours have been observed more in females and externalising have been observed more in males (Liu, 2004; Liu et al., 2011). Recent studies suggest that deficits in self-perceived emotional capabilities and competence play a notable role in the engagement in problem behaviours by adolescents (Cheung et al., 2020; Downey et al., 2010; Resurrección et al., 2014). As such, EI may produce incremental predictive validity over wellbeing measures in predicting problem behaviours as it captures the specific emotion-related skills and behaviours of emotional regulation and social understanding, which are involved in managing challenging situations and avoiding problematic behaviours. While wellbeing measures focus on overall positive feelings and achievement, EI provides a more nuanced understanding of how individuals navigate emotional challenges and interpersonal dynamics, potentially predicting problem behaviours more effectively.
In a study investigating wellbeing and psychological adjustment, Arslan (2019) reported that self-perceived emotional competence (characterised by self-perceived emotional regulation, self-control and empathy) was predictive of externalising behaviours in adolescents such that those with fewer emotional capabilities reported more engagement with externalising behaviours including conduct, attention and hyperactivity problems. Furthermore, a study by de la Barrera et al. (2019) found that adolescents with low self-esteem and low self-reported emotional competence, particularly with regards to emotional expression and management developed conduct (externalising) problems. With regards to internalising behaviours, the same study found that adolescents who pay more attention to their emotions and were less able to manage their emotions experienced more emotional (internalising) problems (de la Barrera et al., 2019). Likewise, a study examining adolescent EI, social skills and problem behaviours found that EI had an inverse relationship to problem behaviours with poorer emotional intelligence related to greater engagement in problem behaviours and this relationship was even more pronounced for females (Salavera et al., 2019). Taken together, these studies highlight the importance of emotional competencies as protective factors against engaging in problem behaviours and underscore emotional dysregulation as a potential precursor to engagement in internalising and externalising behaviours.
This study aims to examine the relationship between trait EI and different measures of adolescent psychological adjustment and will investigate potential gender differences in these variables. We seek to examine the relative predictive potential of EI and measures of wellbeing and psychological distress on problem behaviours in adolescents while considering potential gender differences. We hypothesised that EI would be predictive of positive wellbeing and negatively related to psychological distress. Furthermore, lower emotional awareness and regulation were expected to predict internalising and externalising behaviours, beyond the contribution of other wellbeing measures.
Method
Sample
Participants were selected using non-probability convenience sampling. All students completing Year 8 at three independent Australian schools were invited to participate; one was an all-girls’ school and two were all-boys’.
A priori power analysis was conducted to establish the required sample size for linear multiple regression with eight predictors, effect size of 0.10, at the 95% confidence level. It was determined that a minimum sample size of 158 was required. The initial sample comprised 430 participants, indicating that the study was adequately powered, although 8 were removed due to completing less than 50% of the total survey. The final sample consisted of 422 students of ages ranging between 13 and 14 years (M = 13.29, SD = .46), of which 83 were female and 339 were male.
Ethics and Consent
All study procedures were performed in compliance with relevant laws and institutional guidelines and approval to conduct the research was granted by the relevant institutional Human Research Ethics Committee (Reference number 2016/280). Parental consent was obtained prior to participant recruitment, whereby all parents of eligible students were informed of the study and were given opportunity to provide consent for their child to take part. All students with parental consent were then invited to participate. Those students who consented to take part in the study completed an online survey in a classroom setting, supervised by a teacher.
Measures
Adolescent Swinburne University Emotional Intelligence Test (SUEIT)
The Adolescent SUEIT is a 57-item, self-report measure of emotional intelligence containing four subscales: Emotional Recognition and Expression (ERE) (10 items, α = .74), Understanding and Analysing Emotions (UAE) (19 items, α = .80), Emotional Reasoning (ER) (10 items, α = .75) and Emotional Management and Control (EMC) (18 items, α = .78) (Luebbers et al., 2007). Participants use a five-point Likert scale, ranging from 1 = ‘very seldom’ to 5 = ‘very often’ to indicate how they typically feel, think and act. A higher subscale score reflects higher self-reported proficiency for that EI skill set.
General Health Questionnaire-12
The 12-item GHQ is a self-report measure of psychological distress, suitable for adolescents and adults, designed to screen for non-psychotic and minor psychiatric disorders (Goldberg & Williams, 1988). Two key areas are assessed using this tool; the inability to carry out normal functions and the appearance of new and distressing symptoms. Participants indicate how their health has been in general over the last few weeks by responding to items using a four-item Likert scale from 0 to 3. A total score ranging from 0 to 36 is calculated with a score above 15 indicative of distress and above 20, indicative of severe problems and psychological distress. The measure has been found to be a valid measure of psychological wellbeing in young adolescents with adequate internal reliability reported in a school sample (α = .88) (Tait et al., 2003).
EPOCH
The 20-item EPOCH is a measure of markers of positive wellbeing in adolescents and integrates both hedonic (subjective) and eudaemonic perspectives of wellbeing (Buerger et al., 2023). It assesses five key characteristics; Engagement (4 items, α = .74), Perseverance (4 items, α = .80), Optimism (4 items, α = .81), Connectedness (4 items, α = .81) and Happiness (4 items, α = .86) (Kern et al., 2016). Participants respond to each item using a five-point Likert scale ranging from 1 = ‘almost never’ to 5 = ‘almost always’ to show how well each item describes them. A general wellbeing factor can also be calculated by taking the average of the 5 subscale scores and has been shown to have good model fit and validity (Buerger et al., 2023).
Personal Wellbeing Index – School Children Version (Cummins & Lau, 2005)
The Personal Wellbeing Index – School Children Version is a self-report measure of subjective wellbeing designed for school-aged children and adolescents. Each item covers one quality of life domain including standard of living, health, life achievement, personal relationships, personal safety, community-connectedness and future security. Respondents indicate how happy they are with each life domain on a scale from 1 = ‘very sad’ to 10 = ‘very happy’. An optional additional item covers how happy the respondent is with their life as a whole. Each life domain can be considered individually or aggregated together to form the Personal Wellbeing Index total score (α = .82) (Tomyn & Cummins, 2011).
Strengths and Difficulties Questionnaire (Goodman, 1997; Goodman et al., 1998)
The SDQ is a self-report behavioural screening questionnaire suitable for adolescents aged 11-16 years of age. The questionnaire measures emotional symptoms (5 items, α = .75), conduct problems (5 items, α = .72), hyperactivity/inattention (5 items, α = .69), peer relationship problems (5 items, α = 65) and prosocial behaviour (5 items, α = .61) (Goodman et al., 1998). In low risk or general populations such as the one utilised in the current study, Goodman et al. (2010) advocate these scales can be suitably collapsed into 3 key subscales measuring internalising problems (emotional symptoms + peer relationship problems), externalising problems (conduct problems + hyperactivity symptoms) and prosocial behaviour. Previous research has reported acceptable internal reliability for each of the 3 subscales (α = .76−.83) (Hessel et al., 2017).
Results
Data Preparation
All analyses were carried out using SPSS version 29. The data was first examined to ensure suitability for analysis. No missing data or extreme outliers were identified. Examination of the distribution of each outcome revealed no major violations, except for personal wellbeing index scores which were significantly positively skewed. This variable was transformed to address the skewness with separate analyses conducted using the untransformed and transformed variables with little differences observed. Consequently, the following analyses are reported using the untransformed personal wellbeing index scores.
Descriptive and Correlational Analyses
Descriptive Statistics and Pearson’s Correlation Coefficients of Study Variables
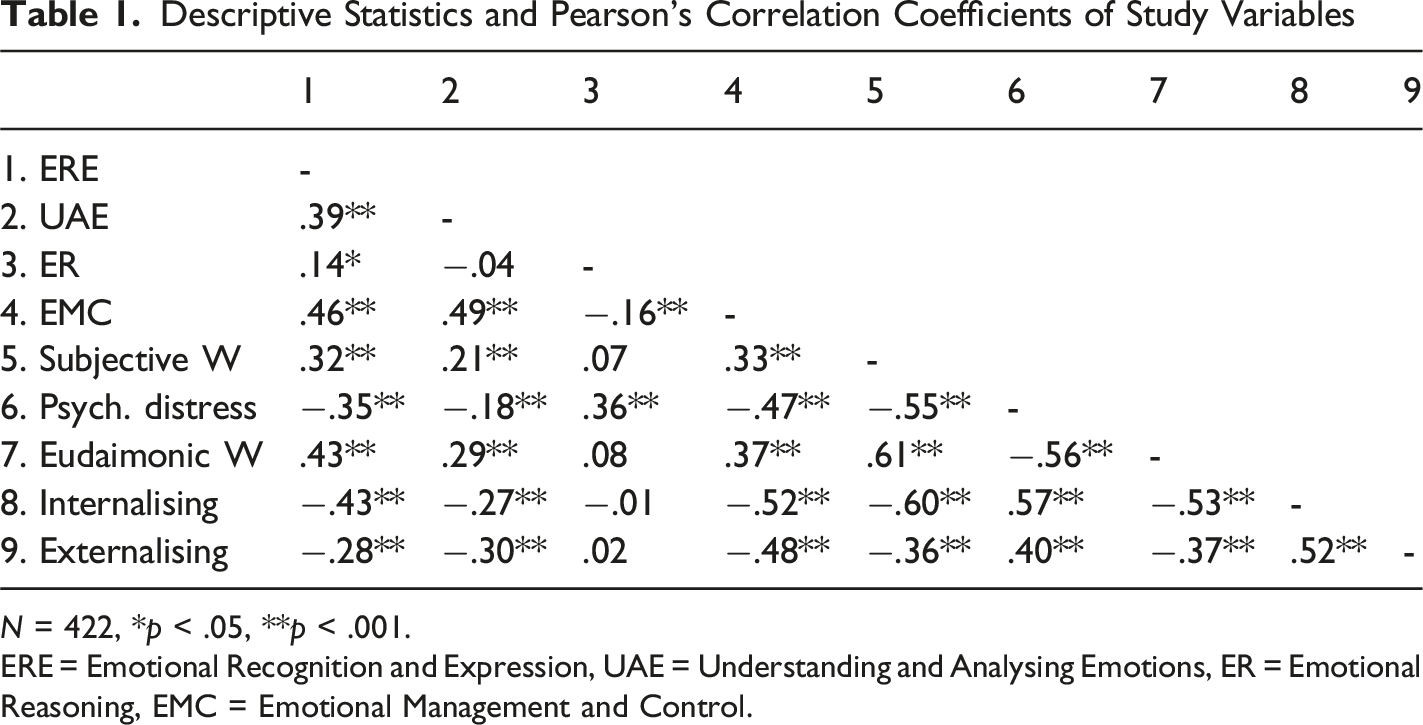
N = 422, *p < .05, **p < .001.
ERE = Emotional Recognition and Expression, UAE = Understanding and Analysing Emotions, ER = Emotional Reasoning, EMC = Emotional Management and Control.
Scale Descriptives, Internal Reliability and One-Way ANOVAs
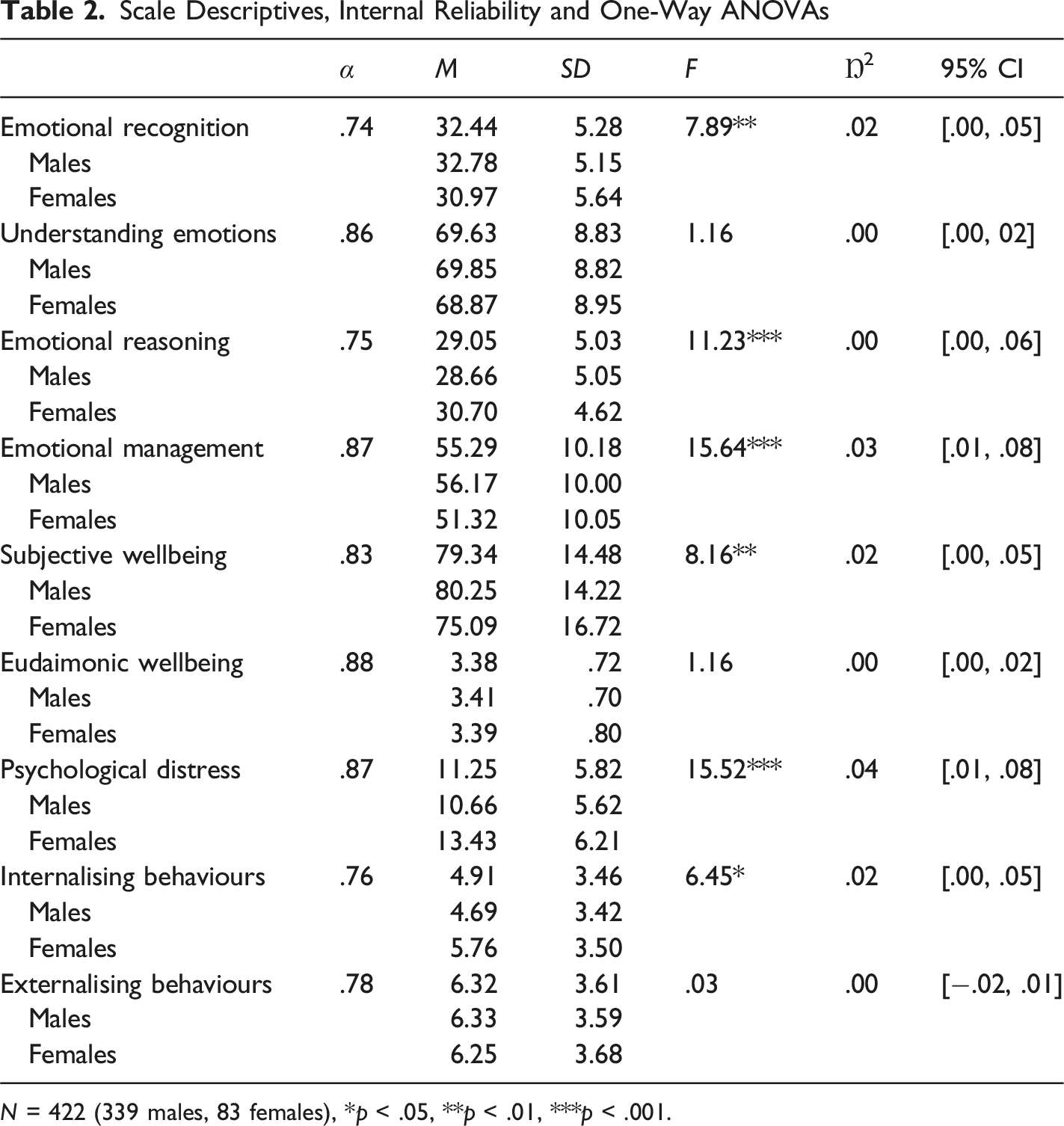
N = 422 (339 males, 83 females), *p < .05, **p < .01, ***p < .001.
Regression Analyses
Multiple Linear Regression Analyses Predicting Wellbeing and Psychological Distress With EI as Predictor Variables
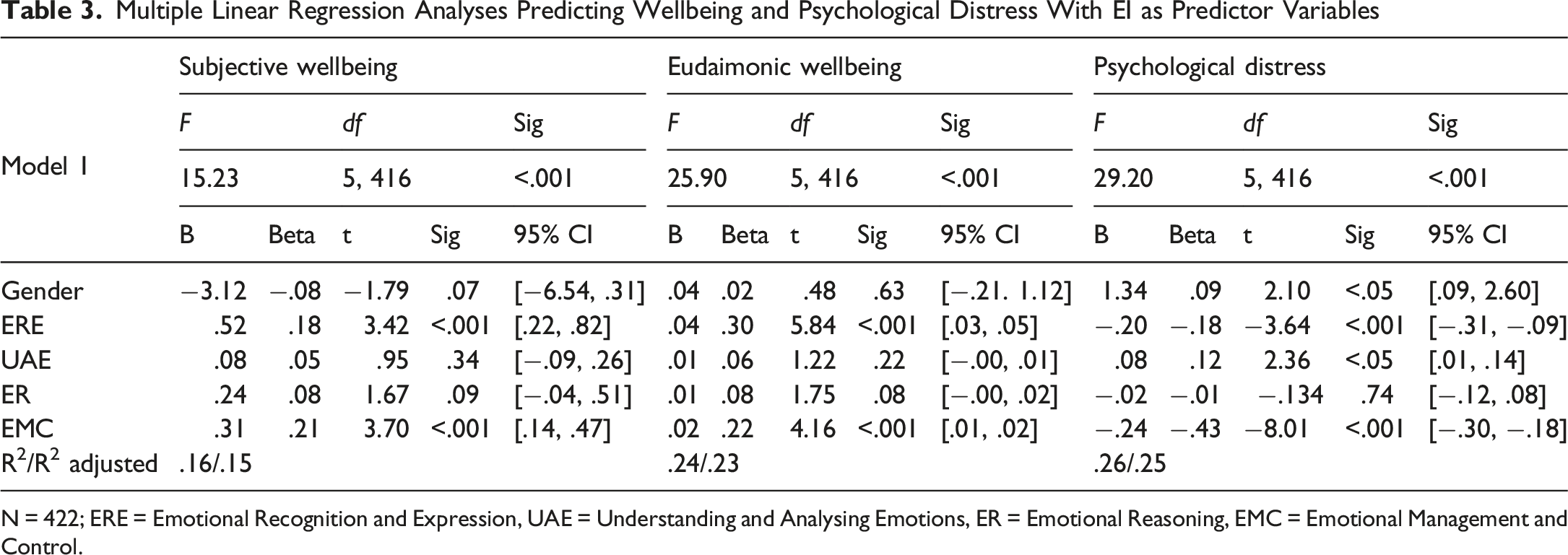
N = 422; ERE = Emotional Recognition and Expression, UAE = Understanding and Analysing Emotions, ER = Emotional Reasoning, EMC = Emotional Management and Control.
Each of the regression models were significant with EI dimensions predicting a significant amount of variance in subjective wellbeing (F (5,416) = 15.23, p < .001, R2 = .16), eudaimonic wellbeing (F (5,416) = 25.90, p < .001, R2 = .24), and psychological distress (F (5,416) = 29.20, p < .001, R2 = .26). In the eudaimonic model, ERE had the strongest effect on wellbeing (β = .30), followed by EMC (β = .22). In the subjective wellbeing model, the same EI dimensions were the most important predictors, with EMC showing the strongest effect on wellbeing (β = .21), followed by ERE (β = .18). In the model of psychological distress, EMC was found to be the strongest predictor (β = −.43), followed by ERE (β = −.18), UAE (β = .12), and then gender (β = .09). Examination of tolerance values for each model revealed no evidence of multicollinearity.
Hierarchical Linear Multiple Regression Analyses
Hierarchical Multiple Linear Regression Analyses of Problem Behaviours With EI and Wellbeing as Predictor Variables
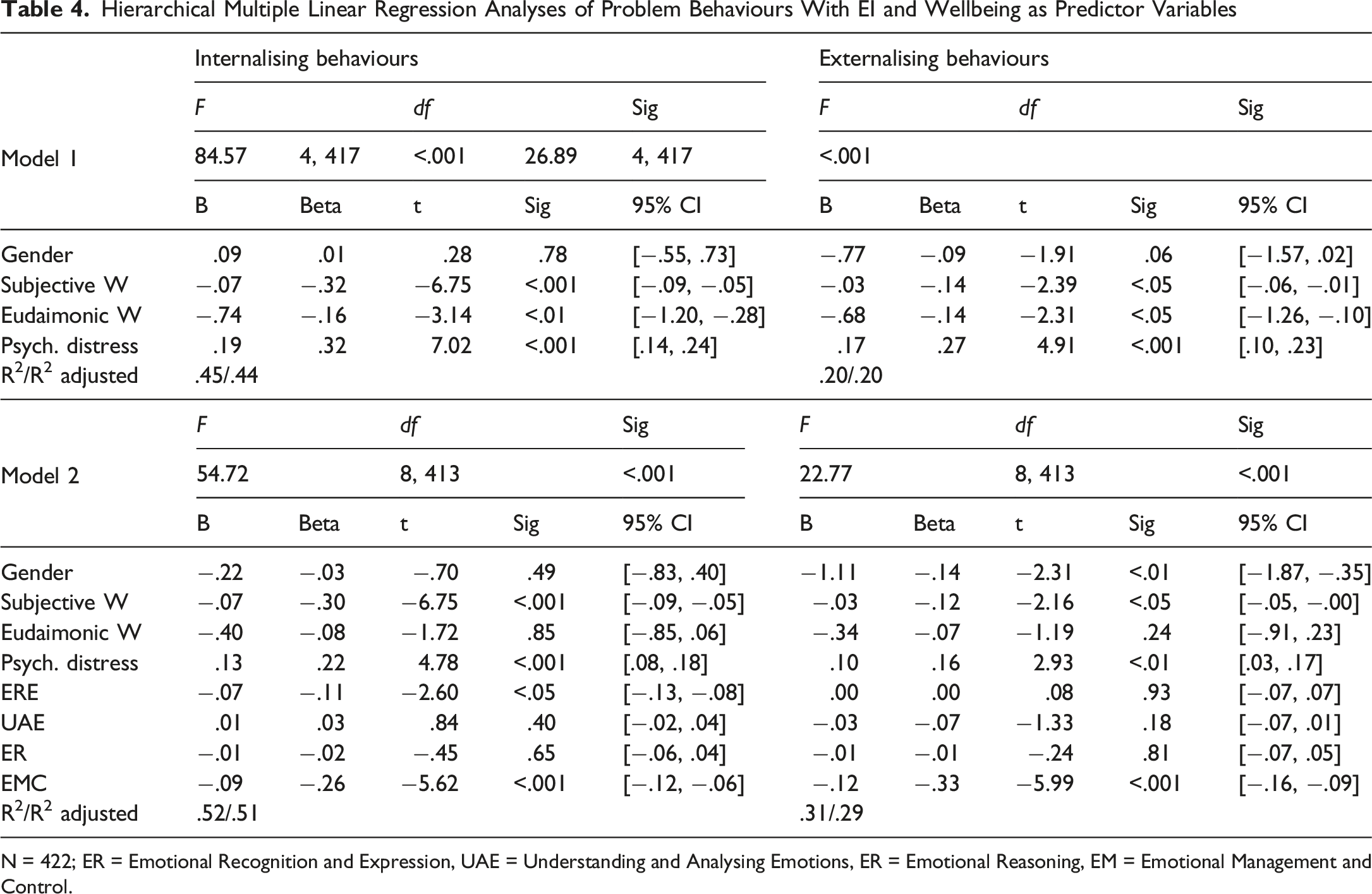
N = 422; ER = Emotional Recognition and Expression, UAE = Understanding and Analysing Emotions, ER = Emotional Reasoning, EM = Emotional Management and Control.
The internalising behaviours model was significant at Model 1, (F (4,417) = 84.57, p < .001, R2 = .45), with wellbeing and psychological distress accounting for 45% of the total variance in internalising behaviours. Subjective wellbeing and psychological distress both had the strongest effect on internalising behaviours (β = −.32) and (β = .32) respectively, followed by eudaimonic wellbeing (β = −.16). Model 2 predicting internalising behaviours was also significant, (F (8,413) = 54.72, p < .001, R2 = .52), accounting for 52% of the total variance in internalising behaviours and the model was significantly improved by the additional of the EI variables, (FΔ (4,413) = 14.18, p < .001, R2Δ = .07). With the inclusion of EI subscales in the model, eudaimonic wellbeing no longer significantly contributed to the prediction of internalising behaviours, but subjective wellbeing and psychological distress remained significant predictors, albeit to a reduced magnitude, (β = −.30) and (β = .22) respectively. Of the EI subscales, ERE and EMC significantly contributed to the prediction of internalising behaviours, with EMC (β = −.26) showing a stronger effect on internalising behaviours than ERE (β = −.11), and subjective wellbeing showing the strongest effect on internalising behaviours in the model overall (β = −.30). Examination of all tolerance and VIF values revealed no evidence of multicollinearity or singularity in the internalising behaviours model.
The externalising behaviours model was significant at Model 1, (F (4,417) = 26.89, p < .001, R2 = .20), with wellbeing and psychological distress accounting for 20% of the total variance in externalising behaviours. Psychological distress showed the strongest effect on externalising behaviours in the model (β = .27), followed by eudaimonic wellbeing and subjective wellbeing (β = −.14). Model 2 predicting externalising behaviours was also significant, (F (8,413) = 22.77, p < .001, R2 = .31), accounting for 31% of the total variance in externalising behaviours and the model was significantly improved by the additional of the EI variables, (FΔ (4,413) = 15.03, p < .001, R2Δ = .10). With the inclusion of EI subscales in the model, eudaimonic wellbeing no longer significantly contributed to the prediction of externalising behaviours, subjective wellbeing remained a significant predictor, as did psychological distress, albeit to a reduced magnitude. Gender also a significant predictor of externalising behaviours in Model 2 (β = −.14), showing a stronger effect on externalising behaviours than both subjective wellbeing (β = −.12), and psychological distress (β = .16). Of the EI subscales, only EMC significantly contributed to the prediction of externalising behaviours but showed the strongest effect on externalising behaviours of all the variables entered in the model (β = −.33). Examination of tolerance and VIF values revealed no evidence of multicollinearity or singularity in the externalising behaviours model.
Discussion
This study examined the relationship between adolescent EI competencies, wellbeing, psychological distress, and problem behaviours in a large sample of adolescents. We explored whether EI showed incremental validity in the prediction of problem behaviours, over and above the influence of gender, wellbeing, and psychological distress. It was observed that greater EI competencies were predictive of higher subjective and eudaimonic wellbeing, less psychological distress and were predictors of adolescent internalising and externalising behaviours once gender, wellbeing, and psychological distress had been accounted for. In line with expectations, this study found that emotional awareness, expression, and regulation were predictive of positive wellbeing outcomes, as well as lower psychological distress and problem behaviours in adolescents. Being male was particularly relevant for the prediction of engaging in externalising behaviours, however, gender appeared to be less predictive of engagement in internalising behaviours in this sample.
The current study observed that EI scores were predictive of all measures of psychological wellbeing, highlighting the importance of such emotional processes. Emotional awareness, effective communication of emotions as well as greater emotional management and control were found to be the best predictors of positive wellbeing represented by subjective and eudaimonic wellbeing and less psychological maladjustment, represented by psychological distress. These findings are in line with a growing body of adolescent research which emphasises emotional competence as a protective factor for optimal wellbeing, where awareness and effective regulation of emotional states appear to be key mechanisms (Ciarrochi & Scott, 2006; de la Barrera et al., 2019; Lereya et al., 2022; Schutte et al., 2010). Our research also supports the findings from other studies in adolescents that identified that increased internalising of problems is inversely related to one’s levels of social skills and EI (Salavera et al., 2019). In this sample, internalising behaviours was predicted by poorer subjective wellbeing and greater psychological distress, highlighting the role of negative affect in such behaviours. Of the emotional processes considered in this study, emotional regulation and control was by far the strongest predictor of internalising behaviours; with adolescents who reported being able to manage strong emotions being less likely to internalise their emotional experience through anxiety, depression, or withdrawal. Additionally, adolescents who reported less awareness and ability to effectively communicate their emotions were more likely to internalise their emotional experience. This pattern of findings is consistent with the notion that social withdrawal is a characteristic of internalising behaviours in adolescents which in part involves less communication with others (Hansen & Jordan, 2020). Similar studies have reported that internalising behaviours can arise from excessively attending to emotions (e.g. rumination) (Fernández-Berrocal et al., 2006), which was not entirely consistent with our data. While rumination involves repeatedly attending to negative emotions, other aspects of rumination such as adopting a negative self-concept or lack of subsequent problem-solving efforts may explain these findings, rather than awareness of negative emotions alone. Given that emotional awareness appeared to be related to less internalising behaviours in our study, awareness and accurate definition of one’s current emotional state may be an important pre-cursor to implement effective emotion regulation strategies and a possible explanation for the inverse association between emotional recognition and expression and internalising behaviours observed in our sample (Fernández-Berrocal et al., 2006; Mayer et al., 2008).
With regards to externalising behaviours, emotional management and control was also the strongest predictor in this sample, with adolescents who reported engaging in acts of aggression, delinquency, or hyperactivity and impulsivity also reported less ability to manage and control strong emotions. Adolescents who reported greater experience of negative emotions, especially when they caused mental and physical suffering, who were also not able to regulate or control these emotions were more likely to engage in behaviours that were harmful or violate social norms. These finding are in line with recent research in adolescent samples that showed that a combination of low self-esteem and emotional competence (perception, expression and management of emotions) predicted the development of behavioural problems (de la Barrera et al., 2019). Effective emotional management and control may inhibit problem behaviours through the production of productive coping strategies such as seeking social support or problem-focussed coping (Downey et al., 2010). Excessive suppression of emotion has been theorised to limit cognitive resources for other tasks such as problem-solving or maintaining healthy peer relationships (Gross & Cassidy, 2019), which presents an alternative perspective on how emotional regulation might relate to problem behaviours. Gender was also found to be a predictor of externalising behaviours, such that being male was predictive of engaging in these behaviours. Although males have been reported to engage in externalising behaviours more than females in prior research (Liu, 2004), the mechanism for the relationship observed in the study is not entirely clear. Given there were only minor differences between the genders regarding the level of engagement in externalising behaviours in this sample, it may be that the impact of gender is related more to emotional management of control in the prediction of externalising behaviours, which was also reported to be higher in males in this sample. Detailed examination of this possible relationship was out of the scope of the current study but presents an opportunity for further research.
With regard to other gender differences observed in this study, males reported higher emotional recognition and expression and emotional management and control than females in this sample, which is in line with previous research that suggests adolescent males tend to have higher self-reported EI (D'Amico & Geraci, 2022). In our study, more internalising behaviours were reported by females which is also consistent with previous work (Liu et al., 2011; Luijten et al., 2021). No group gender differences were identified in this sample regarding externalising behaviours, which was inconsistent with prior research that suggests males tend to engage in these types of behaviours more often (Liu, 2004). Despite this, gender was found to be predictive of externalising behaviours, such that being male was associated with engaging in these behaviours, as previously discussed. Our sample included relatively fewer females than males and this finding should therefore be interpreted with caution.
The results of our study supported previous findings that higher levels of wellbeing on measures that incorporate goals and aspirations (eudaimonic wellbeing) are associated with low psychological distress and higher subjective wellbeing (Deci & Ryan, 2000). With regard to the dialogue concerning the need to measure both positive wellbeing and psychological distress when considering overall wellbeing (Winefield et al., 2012), the current study showed that while these presented as related constructs with obvious conceptual overlap, as reflected in the higher correlations, the conceptualisations of wellbeing were found to be distinct and therefore offer unique contributions to our understanding of the overall mental and psychological health of adolescents. Indeed, in line with the World Health Organization (2022) dyadic conceptualisation of mental health as incorporating positive dimensions of psychological wellbeing and a negative dimension of stressors, adolescent mental health can be better understood by considering the sum of a range of measures. In this way, this study has added support to the notion that researchers are best served by considering multiple perspectives of wellbeing simultaneously when examining interrelated constructs.
Limitations
Despite the large sample size and use of age-appropriate measures, the current study has some limitations. Findings are limited by some conceptual overlap between predictor variables, a gender imbalance in the sample and the cross-sectional and self-report aspects of the research design. Given that this study was cross-sectional in design, it is not possible to infer causality towards the relationship between the wellbeing and EI assessments and problem behaviours. We were interested in in comparing the role of EI in the prediction of problem behaviours, relative to measures of well-being in this study, and were not able to control for common correlates of factors of EI and mental health such as personality and cognitive ability (Elfenbein & MacCann, 2017; Patalay & Fitzsimons, 2018; Petrides et al., 2007), thus effect sizes should be interpreted with caution. Future studies should seek to account for these factors to improve accuracy in the predictions. Given the gender imbalance within the sample, a larger female proportion would have been preferable when examining the potential mediating role gender plays between EI and the behaviours assessed. Gender differences in relation to wellbeing and engagement in problem behaviours appear to be an underexamined relationship (Luijten et al., 2021; Patalay & Fitzsimons, 2018), so future studies should also seek to investigate this in a structured manner.
Conclusions
The results of the current study indicate that EI plays a role in the prediction of wellbeing and problem behaviours, offering additional predictive power beyond measures of psychological distress, eudaimonic and subjective wellbeing. The results also offer support for the notion that EI is a predictor of adolescent wellbeing, no matter how wellbeing is conceptualised. Previous research has shown that EI can be developed (Hodzic et al., 2018; Mattingly & Kraiger, 2019; Schutte et al., 2013), and others suggest that EI training in educational settings could increase subjective wellbeing and in turn, impact the prevention of emotional disorders in adolescents (Davis et al., 2019; Llamas-Díaz et al., 2022). The findings of the current study that emotional regulation, awareness and expression are predictors of wellbeing and problem behaviours is noteworthy given other factors that influence these outcomes are not always as potentially malleable or occur under an individual’s volition. This research has highlighted the role of EI with regards to adolescent wellbeing and problem behaviours and suggests that higher EI in adolescents is likely to be beneficial.
Footnotes
Ethical Considerations
All procedures were performed in compliance with relevant laws and institutional guidelines and approval to conduct the research was granted by Swinburne University Human Research Ethics Committee on 15/12/2016 (Reference number 2016/280). Parental consent was obtained prior to participant recruitment. Participants gave written consent before completing study surveys.
Consent to Participate
Parental consent was obtained prior to participant recruitment. All students with parental consent were then invited to participate. Participants gave written consent before completing study surveys online in a classroom setting, supervised by a teacher.
Author Contributions
All authors contributed to the study conceptualisation and methodology. Justine Lomas was responsible for the formal analysis, project administration and writing the original draft of this manuscript. Luke A. Downey and Con Stough were responsible for supervision and review and editing the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.