
Abstract
Attentional bias modification (ABM) is cost-effective, accessible, and could meet the increasing demand for mental-health treatment. However, ABM paradigms that reliably modify attentional biases (AB) and symptoms are still required. Consequently, we examined the feasibility of a novel ABM intervention (gaze-contingent consonant and dissonant music heard when looking at positive and negative faces, respectively). Contingency awareness and use, and participant adherence and dropout assessed if the intervention could be done. Negative affect, state rumination, and negative AB (longer dwelling on sad and angry faces) after a single session (Study 1, N = 13), and negative affect, trait rumination, depression, anxiety, and negative AB after four sessions (Study 2, N = 10) assessed whether the intervention should continue. The intervention could be done as (1) the music versions and their contingency were discerned and deliberately controlled by some participants, and (2) the participants adhered to the study with no dropouts. Although reductions in positive affect were seen across the studies, the intervention should continue to be explored as on the whole, reduced negative affect (or no change), state and trait rumination, depression, anxiety, and baseline negative AB were also found post-intervention in descriptive data. However, some participants tolerated the dissonance tracks (i.e., negative-face viewing continued), clinically-relevant changes in rumination, depression, and anxiety scores were seen in few participants, and AB change (attenuation/reversal/increase) depended on the contrast (emotional-neutral and/or emotional-emotional). An evaluation of the studies showed that task instructions, music selection, and the number of sessions to be delivered requires further exploration. In conclusion, gaze-contingent music ABM is feasible and should be further explored to ensure it works as intended for a larger number of individuals. The differing emotional-neutral/emotional-emotional results could underlay/contribute to the lack of AB change found in the commonly used emotional-neutral ABM literature. Thus, both contrasts should be assessed.
Introduction
In the 2022 wave of the UK Mental Health of Children and Young People surveys (Newlove-Delgado et al., 2022), the likelihood (i.e., “unlikely”, “possible”, or “probable”) of a child or young person having a mental health disorder was estimated from Strengths and Weaknesses Questionnaire (Goodman & Goodman, 2011) responses. It was reported that almost a quarter (22%) of the 17–24-year-olds had a “probable” mental-health disorder, with a further 14% “possibly” having a mental-health disorder. Although, the National Institute for Health and Care Excellence recommends psychological intervention (e.g., cognitive behavioural therapy), few access these types of services. For example, only 3% of the 18 – 24 year-olds with a probable mental-health disorder, accessed psychological therapy in the UK in 2017 to 2018 (Rzepnicka et al., 2022). In reality, there are long waiting lists, a lack of engagement during treatment, a high rate of attrition, and up to 50% of those who engage in treatment do not achieve satisfactory treatment responses (Colizzi et al., 2020; Craske & Stein, 2016; Punton et al., 2022; Rodwin et al., 2022). There is also a high risk of relapse associated with depression and anxiety in young adults (39%–72%) (Robberegt et al., 2022). As the mental-health needs of many young adults are still unmet, alternative interventions that increase accessibility and engagement are needed (Colizzi et al., 2020; Hollis et al., 2017). An intervention would also need to be low-cost given the potential numbers in need and high reoccurrence rates. Attentional bias modification (ABM) interventions are considered to be cost-effective, able to increase accessibility, and meet the increasing demand for mental-health treatment, especially when used as a first-line tool or in conjunction with other approaches (Blackwell, 2020; Gober et al., 2021).
Modifying Attentional Biases
An attentional bias (AB) is the tendency for a person to attend to a certain type or types of information whilst ignoring other types of information. Attending to positive information (i.e., positive attentional biases) versus negative information (i.e., negative attentional biases [NAB]) has been shown to have differential consequences on emotional functioning (Arditte & Joormann, 2014; Koster et al., 2011). While NAB have been linked to depression and anxiety (Kircanski et al., 2012; McLaughlin et al., 2007; Mogg & Bradley, 2016), it should be noted that some individuals with depression and anxiety may not display NAB, and some may show a bias away from negative stimuli (i.e., avoidance) (Krings et al., 2020; Mogg & Bradley, 2018). When present, NAB are thought to involve a reduced ability to disengage attention from, and inhibit, negative information (Koster et al., 2011). ABM interventions aim to alleviate symptoms by encouraging a shift in attention from negative stimuli to positive stimuli. With repeated enforcement, disengagement from negative stimuli becomes implicitly learnt. ABM has not proven to be universally effective. While some studies have shown that a reduction in NAB has correlated with a reduction in symptoms of depression and anxiety (Hsu et al., 2021; Jones & Sharpe, 2017; Lazarov et al., 2017; Yang et al., 2015), others have found no change (Duque & Vazquez, 2018) or a reduction in symptoms without AB change (Baert et al., 2010). Further, the effectiveness of ABM in terms of symptom reduction varies with, for example, symptom severity (subclinical vs. disorder level), disorder type (social or general anxiety vs. post-traumatic stress disorder), and bias direction (towards or away) (Baert et al., 2010; Boettcher et al., 2012; Duque & Vazquez, 2018; Fodor et al., 2020; Jones & Sharpe, 2017; Li et al., 2023).
Unsuccessful ABM interventions on depression and anxiety may result from the complexity or combinations of cognitive processes involved in depression and anxiety. For instance, AB in anxiety can present as a bias towards and/or away from threat (i.e., they fluctuate over early vs. late information processing stages) and can be influenced by factors such as an individual’s goals (e.g., achieving a desired emotional state) (Bantin et al., 2016; Kruijt et al., 2019; Lisk et al., 2020; Mogg & Bradley, 2016). Irrespective of the AB presentation, ABM may be unsuccessful due to a lack of engagement and/or boredom as ABM paradigms are repetitive in nature (Beard et al., 2012; Kuckertz et al., 2020). As such, there is still a need for procedures that more reliably lead to a shift in biases and further studies to determine the most effective clinical applications (Hang et al., 2021; Jones & Sharpe, 2017). The cognitive-motivational framework of anxiety (Mogg & Bradley, 2018) suggests that an ABM intervention targeting a variety of cognitive processes within its paradigm (e.g., goal-directed attentional orienting and switching, implicit and/or explicit learning, motivational engagement, and interference) may increase its efficacy. To this end, we combined ABM with music. Music was incorporated to a) modulate areas of the brain associated with AB and ABM, b) reduce cognitive interference, and c) facilitate an implicit and goal-directed/motivated reduction in the time spent attending to threat/dysphoric stimuli.
Music, the Brain, and Attentional Biases
Given the theoretical importance of cognitive/attentional control in AB, depression, and anxiety, musically induced modulation of brain areas vital to emotional regulation and cognitive control such as the prefrontal cortex (e.g., attentional deployment), anterior cingulate cortices (ACC) (e.g., emotional information assessment and directing attentional resources), hippocampus (e.g., spatial processing and emotional regulation), and amygdala (e.g., emotionally-valenced information processing and attention modulation), make musical interventions particularly relevant to the treatment of depression and anxiety (Alluri et al., 2015; Bartsch & Wulff, 2015; Brown et al., 2004; Bush et al., 2000; De Raedt & Koster, 2010; Etkin & Wager, 2007; Keller et al., 2013; Koelsch, 2015; Koster et al., 2011; MacDonald et al., 2000; Madonna et al., 2019; Marchetti et al., 2012; Mohanty et al., 2007; Ochsner et al., 2012; Sambataro et al., 2014; Sridharan et al., 2008; Zald, 2003). For example, the dorsolateral prefrontal cortex (DLPFC) is involved in keeping track of the music in time, the (dorsal) ACC with musical memory, and the amygdala and hippocampus with music-evoked emotion (e.g., pleasure and reward) (Jacobsen et al., 2015; Plakke & Romanski, 2014; Särkämö et al., 2013).
Hyperactivation, hypoactivation, and altered functional connectivity between these regions are associated with both depression and anxiety (De Raedt & Koster, 2010; Ferdek et al., 2016; Madonna et al., 2019; Pizzagalli, 2011). The lateral prefrontal cortex is proposed as a region through which a change in AB is facilitated (Clarke, Browning, et al., 2014). During effective inhibitory control, which is lacking in depression and anxiety, the ACC is thought to regulate DLPFC control of the hippocampus (Anderson et al., 2016; De Raedt & Koster, 2010). Hypoactivation of the ACC and DLPFC, for example, reduces their ability to modulate other structures (Etkin et al., 2010; Ferdek et al., 2016; Hopfinger et al., 2000) and therefore effective inhibitory control is not achieved. Transcranial stimulation of the DLPFC can be associated with successful inhibition of negative stimuli (Vanderhasselt et al., 2017). The ACC and DLPFC are stimulated by music, alongside other artificial stimulation sites, and functional connectivity in attentional systems are increased without the need for a trained administrator and the adverse effects associated with artificial stimulation (Alluri et al., 2015; Brown et al., 2004; Keller et al., 2013; King et al., 2019; Overvliet et al., 2021).
Additionally, both depression and anxiety have been associated with cognitive interference from non-task related information (Boehme et al., 2015; Joyal et al., 2019). Music has been shown to enhance performance (faster response time and/or greater accuracy) on tasks requiring distractor conflict resolution. Using the Stroop task (Stroop, 1992), Masataka and Perlovsky (2013) showed that background music reduces cognitive interference as demonstrated by faster response times and fewer errors. This finding has also been found using a modified attention network task (Fan et al., 2002). Joyful background music was associated with faster response times compared to music portraying tenderness and sadness, and silence (Fernandez et al., 2020). Music also has an implicit effect on visual attention. The emotional tone conveyed by the music influences emotional perception, affecting fixation latency, duration and number, and the saliency of objects (Bravo, 2014; Invitto et al., 2017; Mera & Stumpf, 2014; Millet et al., 2021). Emotionally congruent information (i.e., happy face–major chords and sad face–minor chords) facilitates the processing of each type of visual stimuli (Bakker & Martin, 2014). When negative and positive pictures are presented simultaneously, participants spend less time looking at, and fixating on, negative pictures when positive background music is played. Conversely, participants spend less time looking at, and fixating on, positive pictures when negative background music is played (Arriaga et al., 2014).
Music and Attentional Bias Modification
Previous studies have examined the motivational effect of music to facilitate AB change. Godara et al. (2019) found faster disengagement from negative stimuli in dysphoric participants when the goal stimuli had been reinforced with music, with participants reporting a preference for a music reward (10 seconds of track play) compared to a monetary reward (.062 euros). Lazarov et al. (2017) and Shamai-Leshem et al. (2021) used music as a reward when participants with social anxiety disorder (SAD) (Lazarov et al., 2017) or major depressive disorder (MDD) (Shamai-Leshem et al., 2021) fixated on the target stimuli within a free viewing paradigm. The music reward was removed (stopped playing) when the to be avoided negative stimuli were fixated on. A control condition of continuous background music was also examined. A significant decrease in dwell time on negative stimuli was found in the music-reward condition compared to the continuous background-music condition and significant reductions in symptoms were shown post-treatment in both studies. Findings favoured the music-reward condition for participants with SAD (i.e., lower symptom scores and more participants with clinically-significant reductions), whereas both conditions were effective for participants with MDD (i.e., no significant differences in post-intervention and follow-up symptom scores). The difference seen between SAD and MDD results could potentially be related the target stimuli (neutral vs. happy, respectively) and reduced reward processing in MDD (Shamai-Leshem et al., 2021). Meta-analysis studies (Harney et al., 2023; Panteleeva et al., 2018; Tang et al., 2020) suggest that music listening may have a larger effect on depression than anxiety, thus it is possible that continuous background music may be more effective for participants with MDD compared to participants with SAD.
In the current studies, we focussed on depression and generalised anxiety disorder (GAD) symptoms as they have shown substantial increases in GP reporting in the UK for younger persons, particularly females (Slee et al., 2021). While mood-congruent AB are thought to operate in depression and anxiety (i.e., persons with depression maintain their gaze on dysphoric stimuli, and persons with anxiety avoid and/or maintain their gaze on threat-related stimuli), we included depression- and anxiety-related stimuli (i.e., sad and angry faces) as comorbidity can effect AB presentation (i.e., may be depression- or anxiety-related), AB towards angry faces can be found for individuals with MDD, GAD may not be associated with disorder-specific stimuli, and GAD (or anxiety) symptoms can be reduced when training away from angry or sad faces (Armstrong & Olatunji, 2012; de Rutte et al., 2025; Goodwin et al., 2017; Hankin et al., 2010; Kishimoto et al., 2021; LeMoult & Joormann, 2012; Leyman et al., 2007; Suslow et al., 2020; Woody et al., 2016; Yang et al., 2015). Both neutral and happy faces were included as few studies explore AB within emotional-emotional pairings (Blanco et al., 2019) and intervention effects on emotional-neutral and emotional-emotional pairings.
We hoped to utilise the emotional congruency effect and the differing emotional responses to consonant and dissonant music to modify participants’ AB. Consonant and dissonant music have been shown to differentially affect emotional responses. Consonant music correlates with positive emotions and is rated as pleasant, whereas increasing levels of dissonance are associated with negative emotions and adjectives such as unpleasant, irritating, annoying, and angry (Blood et al., 1999). The initial playing of the consonant version of a music track may facilitate viewing of the more positive face in a pairing (emotional congruency). As the participants are instructed to view the faces naturally, it is likely that the negative face in the pairing would also be viewed. When the participant’s gaze was detected on the negative face (sad or angry) area of interest (AOI), a dissonant version of the same music track would be heard. It was hypothesised that a negative emotional response would be elicited, motivating participants to direct their gaze away from negative stimuli. Goals related to the avoidance of negative consequences can be motivating (Godara et al., 2019). Once their attention was disengaged from the negative face AOI, the consonant version of the track would be heard again. Increased gazing at the positive stimulus (neutral and happy faces) AOI, and therefore a reduction in NAB, would be motivated by the relatively positive emotional effects elicited from the consonant music (associated with positive stimuli/AOI). With repeated exposure, the participant would implicitly learn to disengage their attention from negative stimuli in favour of positive stimuli.
However, it is possible that some individuals may not be deterred by the dissonant version of the music track. Depressed and/or anxious individuals, in particular, may use maladaptive coping styles such as rumination, which involves self-referential, repetitive, and/or frequent thoughts (Koster et al., 2011). Previous research suggests that ruminators have a bias towards negative (sad) music and attend to positive (joyful) music for less time than non-ruminators (Garrido, 2009; Lei et al., 2007). It is therefore possible that ruminators in the current study may be attracted to the negative valence associated with dissonant music, as with sad music (Garrido, 2009), and not be deterred by it. NAB may increase due to a congruency effect (i.e., dissonant music-negative faces). To this end, two feasibility studies were conducted with the aims of identifying whether gaze-contingent musical ABM (GCM-ABM) could be done, whether GCM-ABM should continue to be explored, and if so, how (Eldridge et al., 2016). Our trial design (i.e., exposure to consonant and dissonant versions of a music track in the same trial) had not been previously investigated so it was unknown whether 1) the switch between each version would generally be discerned, 2) the contingency could be discerned and used, 3) dissonance exposure would negatively affect mood overall, 4) participants would engage in multiple sessions of exposure, and 5) any changes in NAB would be displayed.
To assess whether GCM-ABM could be done, a semi-structured interview was conducted in Study 1, and participant comments and dropout were recorded in Study 2. GCM-ABM could be done if there was an awareness of the consonant and dissonant track versions and their contingency, deliberate gaze-control was attempted, and there was low participant dropout. To assess whether GCM-ABM should continue to be explored, we measured positive affect [PA], negative affect [NA], state rumination [SR], and the relative percentage dwell time (RPDT) on negative faces when paired with neutral faces (negative-neutral contrasts) and happy faces (negative-happy contrasts) over a single session (Study 1). Exploration would continue in Study 2 if a positive impact on participants (i.e., reduced NA, SR, and baseline NAB) was found post-intervention in descriptive data. To assess whether GCM-ABM should continue to be explored after Study 2, we focussed on changes in PA, NA, trait rumination (TR), depression, anxiety, and baseline NAB after four daily sessions. Exploration would continue if a positive impact on participants (i.e., reduced NA, TR, depression, anxiety, and baseline NAB) was found post-intervention in descriptive data. If GCM-ABM was deemed feasible (i.e., it could be done and should be proceeded with), an evaluation of what did and did not work in Study 1 and 2 would guide how to proceed further.
Study 1
The aims of Study 1 were to assess whether GCM-ABM could be done and should continue to be explored. We examined participant awareness of the consonant and dissonant track versions and their contingency, whether deliberate gaze-control was attempted, and if there was any modulation of momentary mood and NAB after a single session of GCM-ABM.
Study 1 Materials and Methods
Participants
Study 1 – Participants’ Mood Score, and Symptom Status and Severity.
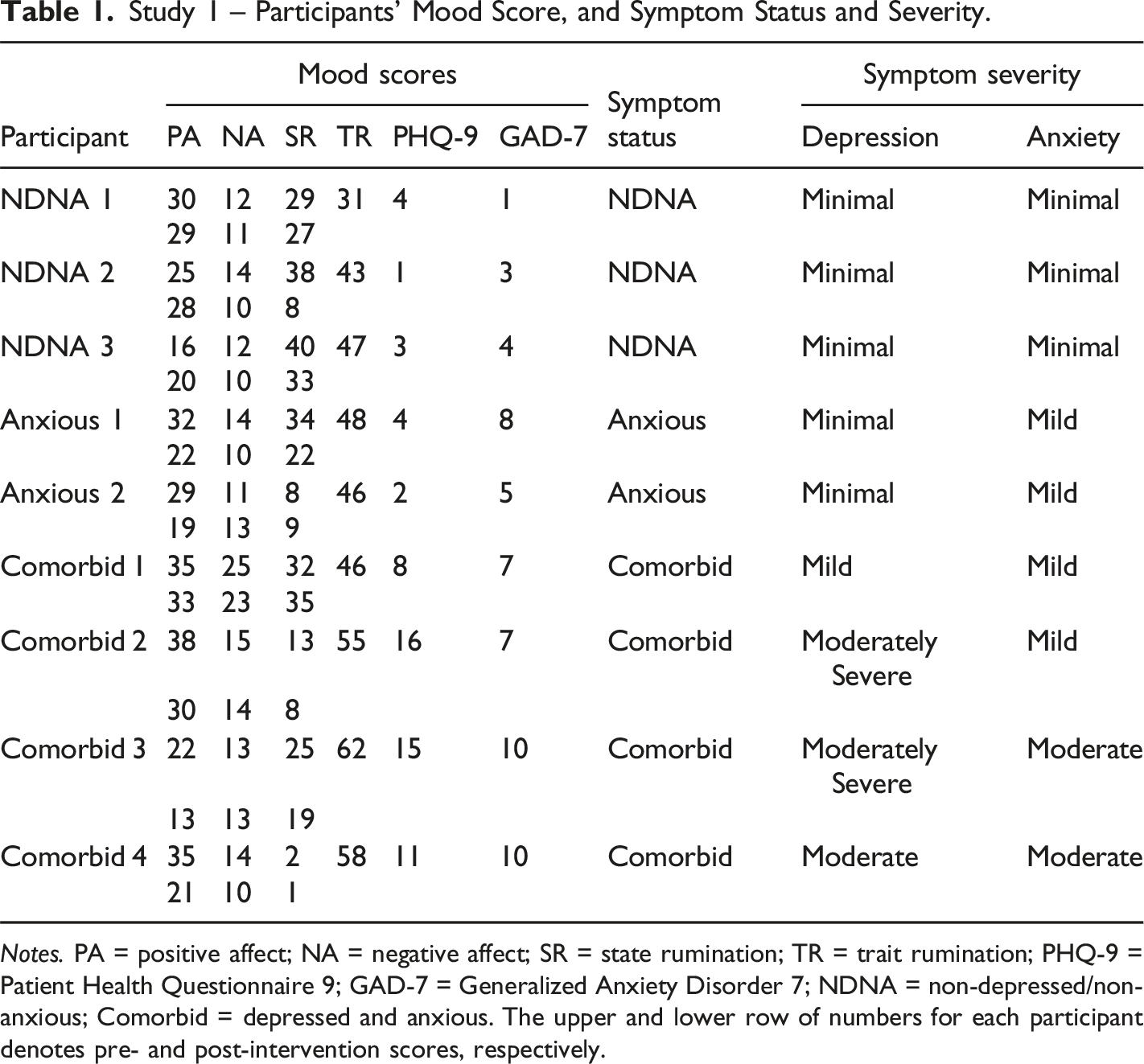
Notes. PA = positive affect; NA = negative affect; SR = state rumination; TR = trait rumination; PHQ-9 = Patient Health Questionnaire 9; GAD-7 = Generalized Anxiety Disorder 7; NDNA = non-depressed/non-anxious; Comorbid = depressed and anxious. The upper and lower row of numbers for each participant denotes pre- and post-intervention scores, respectively.
Procedure
Participants completed an online self-report questionnaire via JISC Online surveys (https://www.onlinesurveys.ac.uk/) to screen for depression, anxiety, and TR, 1–3 days before a lab-based study session. At the start of the lab-based session, participants completed paper-based PA, NA, and SR measures, followed by an AB measure (AB-measure). After a five-minute break, participants received two blocks of GCM-ABM. The participants had another five-minute break before completing the AB-measure and momentary mood measures again, in that order. A semi-structured interview was then conducted. Participating took approximately 1.5 hours in total. Consent was provided during study enrolment (written), at the start of the online survey (checked tick box), and at the start of the lab-based session (written).
Measures
Depression
The Patient Health Questionnaire 9 (PHQ-9) (Kroenke & Spitzer, 2002) scale was used to screen for the presence and severity of depression after the removal of the suicidal ideation item. A score of 0 (not at all) to 3 (nearly every day) is assigned for each item giving a total of between 0 and 24. The lower cut-off point for mild, moderate, moderately severe, and severe depression are scores of 5, 10, 15, and 20, respectively, with a score of ≥10 having a specificity and sensitivity of 88% for MDD (Kroenke & Spitzer, 2002). Although the suicidal ideation item was removed due to ethical concerns, the interpretation of final scores remains the same (Kroenke & Spitzer, 2002).
Anxiety
The Generalized Anxiety Disorder 7 (GAD-7) (Löwe et al., 2008) scale was used to screen for the presence and severity of anxiety. A score of 0 (not at all) to 3 (nearly every day) is assigned for each of the 7 items, giving a total of between 0 and 21. The lower cut-off point for mild, moderate, and severe anxiety are scores of 5, 10 and 15, respectively, with a score of ≥10 suggesting the presence of GAD and other anxiety disorders. The scale demonstrates high internal consistency (α = 0.89) (Löwe et al., 2008).
Affect
The Positive Affect Negative Affect Schedule (PANAS) (Watson et al., 1988) measured how much each participant was experiencing 20 emotions (10 positive and 10 negative items) in the moment. Each item, an affective state such as ‘distressed’ was rated on a 5-point scale (very slightly or not at all = 1 to extremely = 5). The scores for positive items were totalled to provide the positive affect (PA) score and the scores for negative items were totalled to provide negative affect (NA) score. Each totalled affect score ranged from 10 to 50, with higher scores representing higher levels of affect.
Rumination
The 8-item Brief State Rumination Inventory (BSRI) (Marchetti et al., 2018) measured the level of self-reported rumination being experienced in the moment (SR). Participants drew a vertical line on a horizontal line to indicate the degree to which they disagree or agree (0 to 100%, respectively) with each statement. Higher total scores represented higher levels of SR.
We measured trait rumination (TR) tendency as a response to depression using the Ruminative Response Scale (RRS) (Nolen-Hoeksema, 1991). The RRS required respondents to indicate how they had responded to 22 items over the previous fortnight using a 4-point Likert scale ranging from 1 (‘almost never’) to 4 (‘almost always’). The score for each item was summed to obtain a total score ranging from 22 to 88. Higher scores indicate a higher level of TR. The scale shows excellent internal consistency as well as adequate convergent and predictive validity (Nolen-Hoeksema et al., 1993, 1994).
Gaze Location
Participants were seated between 59 and 66 cms away from a desk. A keyboard, Tobii TX300 eye-tracker and a 21-inch monitor positioned on top of the desk (see Supplemental Material for hardware details). The standard 5-point calibration procedure for the Tobii system was conducted before each AB-measure and GCM-ABM block.
Attentional Bias Measure
A modified dot-probe task (MacLeod et al., 2002) was presented via E-Prime 2.0 software (Schneider et al., 2002) to measure participant AB. An instruction slide was presented at the start of the task asking participants to (1) look at the cross and the dot as quickly as possible when they appeared, (2) view the facial stimuli in a natural way when presented, and (3) press the ‘space bar’ to start the task when they were ready. Each trial of the AB-measure task began with a blank screen for 500 ms. A fixation cross then appeared in the centre of the screen until there was a fixation of 100 ms. Two faces from the same actor were then presented to the left and right of where the fixation cross had been located for 1000 ms. The faces, selected from the FACES database (Ebner et al., 2010), were presented in sad-angry, sad-happy, sad-neutral, angry-happy, angry-neutral, and happy-neutral facial expression pairings. Once the faces had disappeared, a white dot appeared in the centre of one of the face’s previous location until there was a fixation of 100 ms. The trial presentation is shown in Figure 1. (see Supplemental Material for stimuli details). The AB-measure block comprised 96 trials which were shown randomly. The same block was used for both of the AB-measures (2 × 96 = 192 trials in total). The trials were counterbalanced for stimulus gender, and the side of the screen the facial expression type and dot appeared on. AB-measure trial presentation information.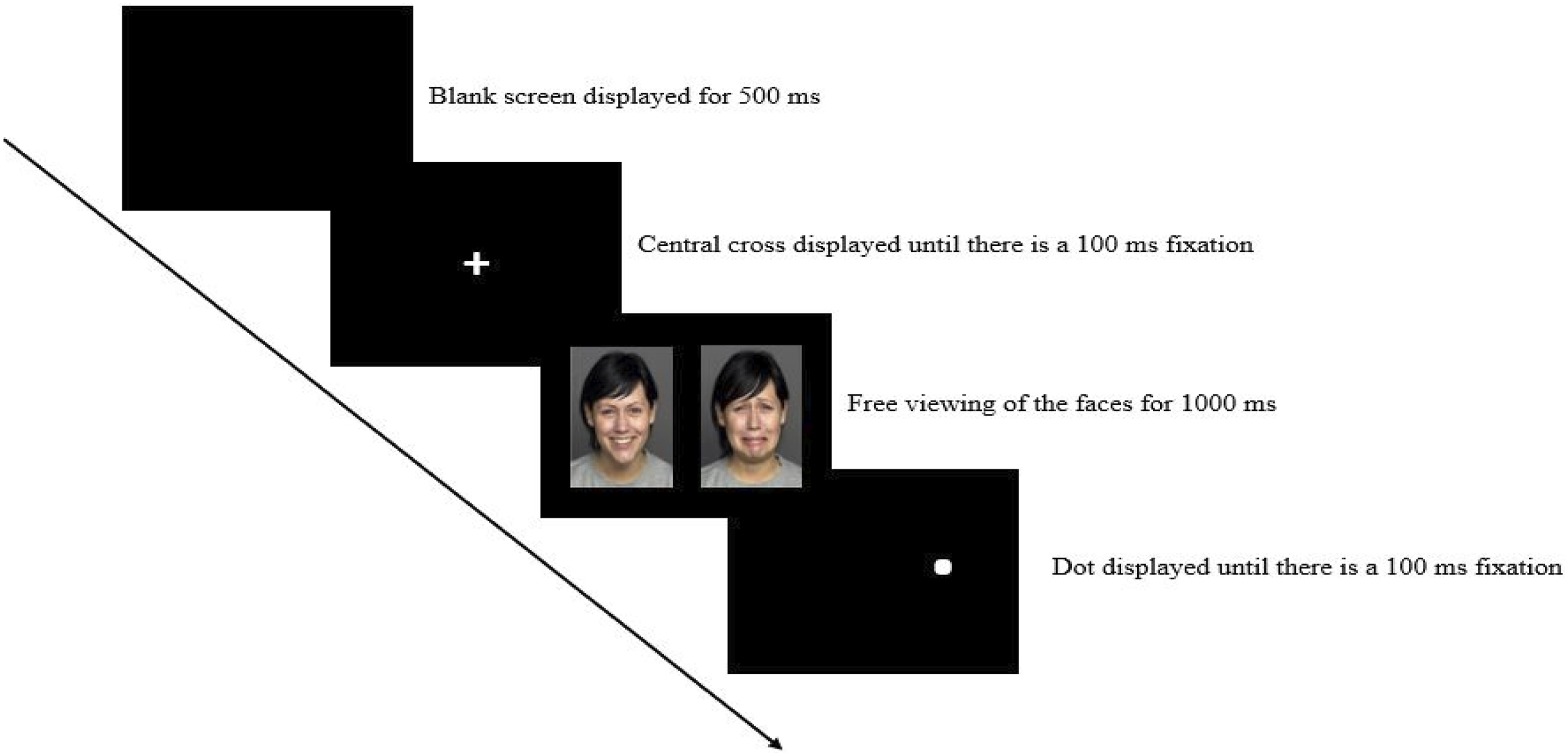
Gaze-Contingent Musical Attentional Bias Modification
The AB-measure block instruction screen (without the dot information) was presented, and a music track began playing contemporaneously at the onset of the instruction screen and played continuously throughout each of the two GCM-ABM blocks. A consonant and dissonant version of an algorithmically generated music track (harps) accompanied one of the GCM-ABM blocks, and a consonant and dissonant version of a music track composed in a romantic period style (violins) accompanied the other (see Supplemental Material and Bravo (2013) and Bravo et al. (2020) for a detailed description of the music tracks’ musical structure). The default setting for the music was that the consonant version of the track was audible, and the dissonant version was inaudible during music play without gaze-contingency (see Figure 2). Each trial began with the blank screen (500 ms) followed by the fixation cross (until a fixation of 100 ms had occurred). The facial slide was then presented for 2500 ms and consisted of sad-neutral, angry-neutral, sad-happy, and angry-happy facial expression pairings. During this slide, the consonant and dissonant tracks’ audibility was controlled by the participant’s eye-gaze location. The participants were not informed of the gaze-contingent control/contingency. When the participant looked at the sad or angry faces, the dissonant version became audible, and the consonant version became inaudible. The music setting returned to default (consonant version audible/dissonant version inaudible) when the participant looked away from the sad or angry faces, and at the end of the facial slide presentation. The GCM-ABM block contained 96 trials which were shown randomly. Each participant received two GCM-ABM blocks (2 × 96 = 192 trials in total). The trials were counterbalanced for stimulus gender, and the side of the screen the facial expression type appeared on. GCM-ABM trial presentation and music play information.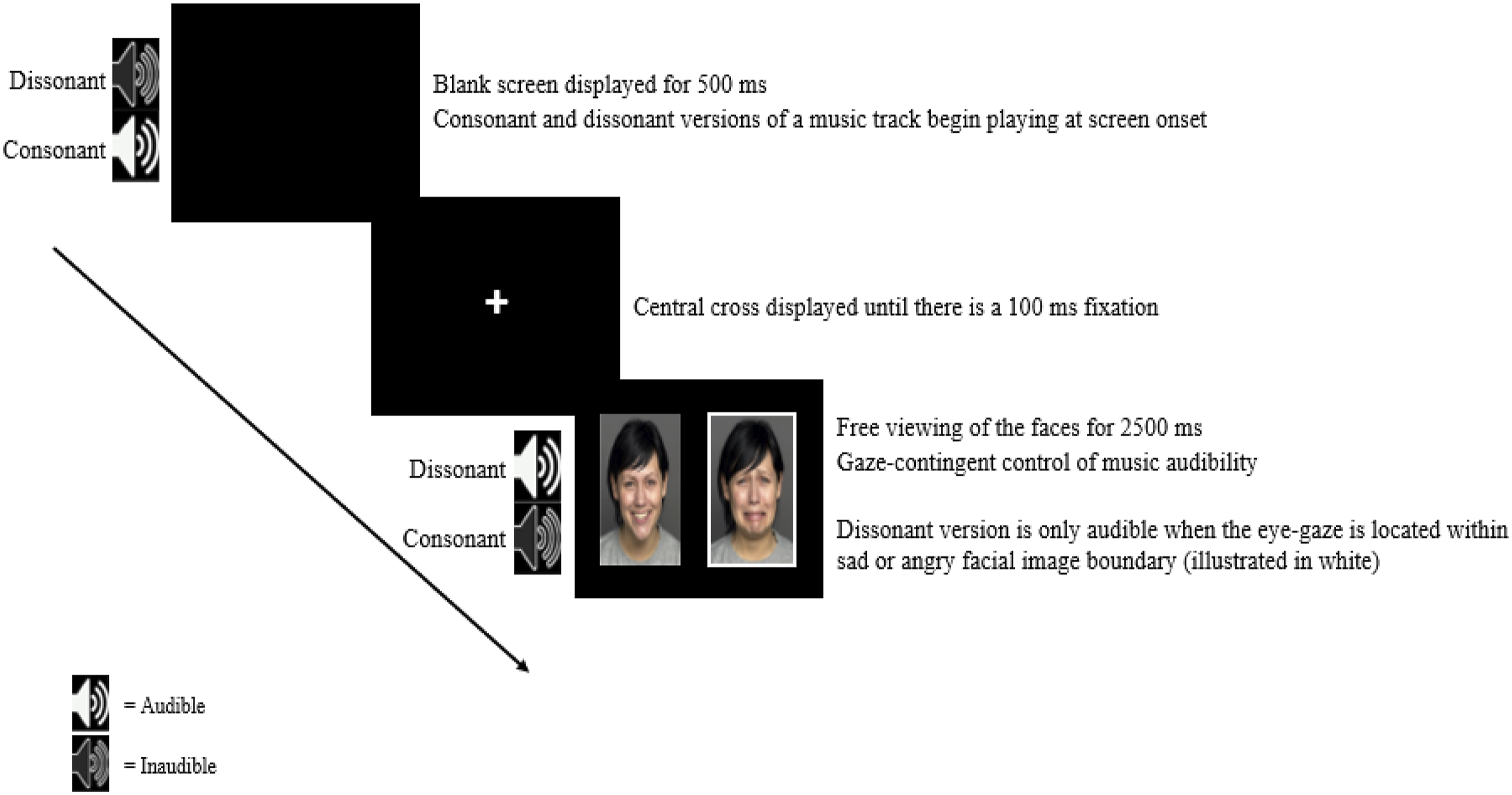
Semi-structured Interview
Participants were asked about their 1) awareness of the music (i.e., attention drawing/distractibility, and how many types of music they heard), 2) thoughts and feelings about the music (probes: liking, preference, emotions, and description of changes [if mentioned]), and 3) overall experience (probes: engagement, enjoyment level, and mood after taking part). We report on 1), 2) (i.e., changes), and 3) as they directly relate to our feasibility aims.
Data Analysis
Descriptive analyses were performed with the Statistical Package for the Social Sciences, version 25 (IBM Corp, 2017).
Symptom Status
A cut-off of ≥5 points on each scale represented the presence of depression (PHQ-9) and anxiety (GAD-7) (Kroenke & Spitzer, 2002; Löwe et al., 2008). Therefore, participants who scored <5 on both the PHQ-9 and the GAD-7 scales were classified as being non-depressed/non-anxious. Participants who scored ≥5 on the PHQ-9 and <5 on the GAD-7 scales were classified as depressed, or anxious if they scored <5 on the PHQ-9 and ≥5 on the GAD-7 scales. Participants who scored ≥5 on both the PHQ-9 and the GAD-7 scales were classified as having comorbid depression and anxiety.
Attentional Biases
Fixations in the eye-tracking data were detected using the saccades package (Titus von der Malsburg, 2019) within R Studio (R Core Team, 2021), and only fixations with a minimum duration of 100 ms were used in later computations (Ferrari et al., 2016). For each participant, the fixation durations for each expression type in negative-neutral and negative-happy pairings were summed to provide the total dwell time (TDT). For negative-neutral pairings, the AB scores were calculated as the proportion of the TDT on the negative face relative to the TDT on both the negative face and its corresponding neutral face (i.e., the relative percentage dwell time [RPDT]). For negative-happy pairings, AB scores were calculated as the proportion of the TDT on the negative face relative to the combined TDT on both the negative face and happy face. Scores above 50% indicated longer dwelling on emotional or negative faces whereas a score below 50% indicated less dwelling these faces (Lazarov et al., 2017; Shamai-Leshem et al., 2021). The eye-tracking metric is indicative of later-stage processing/attentional maintenance which is demonstrated in both depression and anxiety, and is relatively more reliable (e.g., compared to first-fixation latency/location) in terms of internal consistency and test-retest measures (Skinner et al., 2018; Suslow et al., 2020; Waechter et al., 2014).
Study 1 Results
Participant Characteristics
Study 1 - Group Descriptive and Bias Score Data.
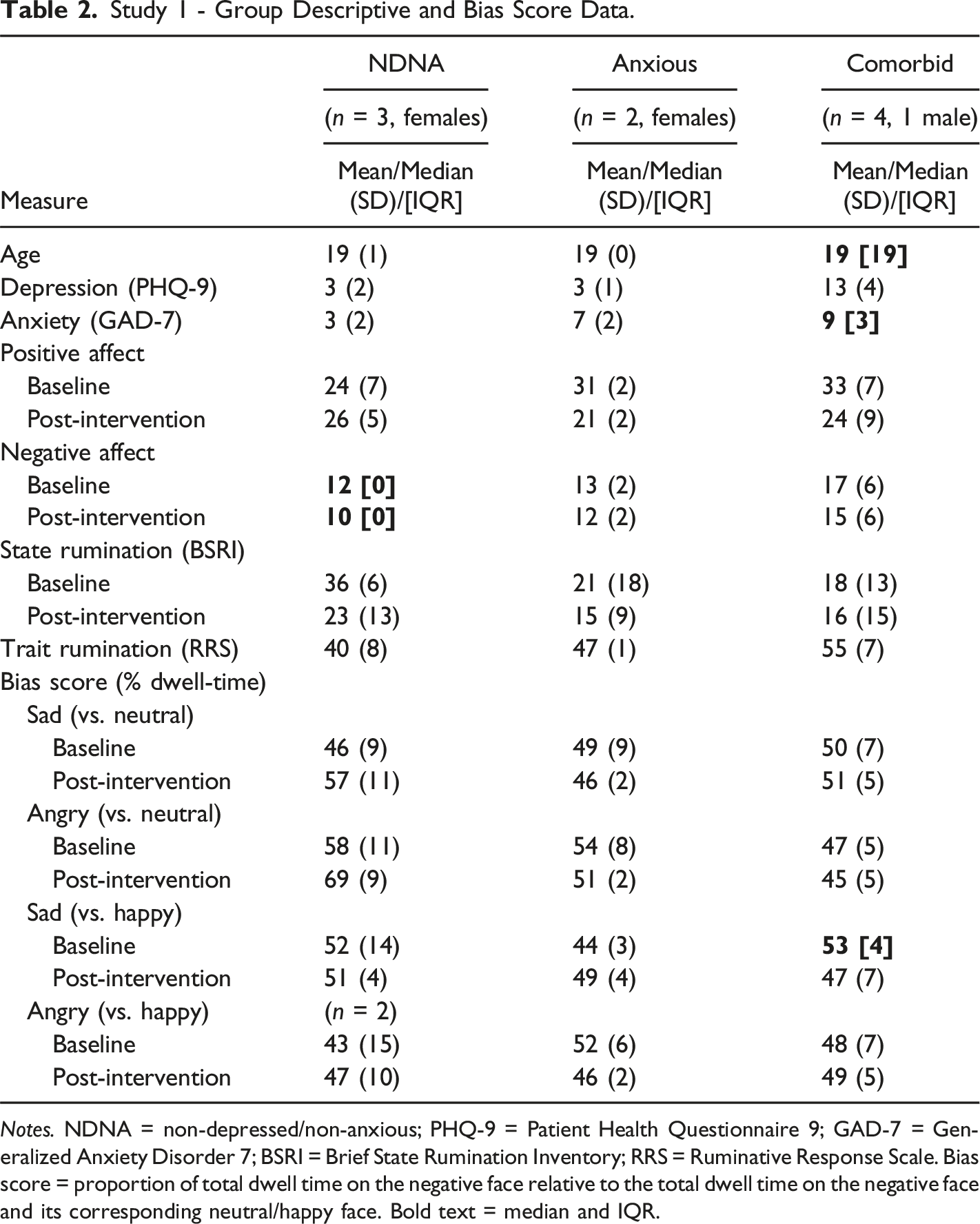
Notes. NDNA = non-depressed/non-anxious; PHQ-9 = Patient Health Questionnaire 9; GAD-7 = Generalized Anxiety Disorder 7; BSRI = Brief State Rumination Inventory; RRS = Ruminative Response Scale. Bias score = proportion of total dwell time on the negative face relative to the total dwell time on the negative face and its corresponding neutral/happy face. Bold text = median and IQR.
Music and Contingency Awareness, and Deliberate Gaze-Control
All of the participants were aware of and paid attention to the music, with the harps track being preferred by more participants (n = 5) than the violins track (n = 3) (liked both = 1). One participant was not distracted by the music while the remaining eight described it as being distracting in relation to the task (facial viewing = 2, having more focus than the task = 1, something to do alongside the task = 1), and the dissonant music versions (n = 4). Participants reported hearing 2 to 4 music tracks (2 tracks = 6, 3 tracks = 1, 4 tracks = 2), with the dissonant versions being counted as separate tracks by some (n = 3). Eight of nine participants were aware of the dissonant versions/a change, with the dissonant version being described as such (n = 1) or with other descriptors (n = 7) (e.g., ‘discordant’, ‘off key’, and ‘unpleasant [one]’). Of these eight participants, three participants described a link between the music and their viewing pattern/gaze but not the contingency (e.g., ‘…it seemed the minute the music changed, my eyes moved or was it my eyes were moving and the music changed’ and, ‘especially because it [the music] sounded kind of scary and like sad so I would tend to notice the faces that were kind of more like angry and emotions like that.’).
Three others were explicitly aware of the music contingency, with two applying gaze-control to stop hearing the dissonant versions (e.g., ‘When I looked at the unhappy it [the music] was just like not in tune so it did make me annoyed. So, I would look at the happy face more.’). The third used gaze-control a little but stopped due to task conflict (i.e., ‘I tried to concentrate on the task [viewing the faces naturally] but my brain wanted to like look in a way to create some nice addition to the music. But I was trying to concentrate on the task, I was trying to generalise to the faces.’).
Of note, the aversiveness of the dissonant versions could lead to avoidance and playing around (e.g., '...the sad [dissonant] part felt like it was in the [violins] song, it was part of the song whereas the second one [harps dissonant version] it was just so annoying. You would look at the sad face, it was so out of tune I would look immediately at the happy one [face]. Whereas the first song [violins], I was going backwards and forward between them [consonant and dissonant versions] because I liked to hear, it felt like it just went well together.’). And, rather than aversiveness, a participant found the switch ‘interesting’.
Overall Experience
Participants reporting having an ‘interesting’ (n = 4) or ‘okay’ experience (n = 2) overall. Three participants stated they enjoyed taking part, while another did not due to the dissonant music. All of the participants reported being engaged in the task, although the majority (n = 7) noted that engagement levels were lower at the end of the session compared to the start. Reasons included lowered energy/tiredness/fatigue (n = 4), difficulties focussing/concentrating (n = 5), mind wandering (n = 3), and boredom (n = 1). Some participants found that the music increased engagement (n = 2), or that the music blocks felt quicker (n = 1), were preferred (n = 1) or were more engaging (n = 2) than the AB-measure blocks. Four participants did not feel their mood had changed after taking part, while others felt they were less anxious (n = 2), had less energy/tiredness/fatigue (n = 2), felt less attentive (n = 1), or were irritated as a result of the dissonant music versions (n = 1).
Three participants reported tiredness of the eyes post-intervention, with one reporting that the AB-measure was harder on the eyes.
Momentary Mood
Positive Affect
Average PA scores (e.g., items such as ‘alert’, ‘attentive’, and ‘active’) increased post-intervention for NDNA group (2 points). Average PA scores decreased post-intervention for the anxious group (10 points) and comorbid group (9 points) (see Table 2 and Supplemental Material for PA item scores).
Negative Affect
Average NA scores decreased post-intervention for the NDNA group (2 points), anxious group (1 point), and comorbid group (2 points) (see Table 2 and Supplemental Material for NA item scores).
State Rumination
Average SR scores decreased post-intervention for the NDNA group (13 points), anxious group (6 points), and comorbid group (2 points) (see Table 2).
Attentional Biases
Emotional-Neutral Pairings
Sad Faces
RPDT on sad faces increased post-intervention for the NDNA group (11%) and the comorbid group (1%). RPDT on sad faces reduced post-intervention for the anxious group (3%) (see Table 2).
Angry Faces
RPDT on angry faces increased post-intervention for the NDNA group (11%). RPDT on angry faces reduced post-intervention for the anxious group (3%) and the comorbid group (2%) (see Table 2).
Negative-Happy Pairings
Sad Faces
RPDT on sad faces reduced post-intervention for the NDNA group (1%) and comorbid group (6%). RPDT on sad faces increased post-intervention for the anxious group (5%) (see Table 2).
Angry Faces
RPDT on angry faces increased post-intervention for the NDNA group (4%) and comorbid group (1%). RPDT on angry faces reduced post-intervention for the anxious group (6%) (see Table 2).
Exploratory Analyses
Exploratory non-parametric analyses were conducted due to the small sample. Wilcoxon signed rank tests showed that the difference between T1 and T2 PA, NA, SR, and AB scores were non-significant for each group (see Supplemental Material S2. to S4. for non-significant test data).
Individual Attentional Bias Change
As the groups comprised individuals with baseline AB towards negative faces and AB away from negative faces, which affects group averages, individual baseline and post-intervention AB data were plotted to examine the direction of AB change (see Figure 3(a)–3(d)). Individual Baseline and Post-intervention Relative Percentage Dwell Times For Emotional-Neutral and Emotional-Emotional pairings. Notes. NDNA = non-depressed/non-anxious. Relative percentage dwell time = proportion of total dwell time on the negative face relative to the total dwell time on the negative face and its corresponding neutral/happy face. Negative-neutral and negative-happy pairings are shown in Figures 3(a) and 3(b), and Figures 3(c) and 3(d), respectively. Negative AB attenuated/reversed (except for NDNA participants [Figures 3(a) and 3(b)]). Avoidant AB attenuated/reversed (except for Comorbid 2 [Figure 3(b)]).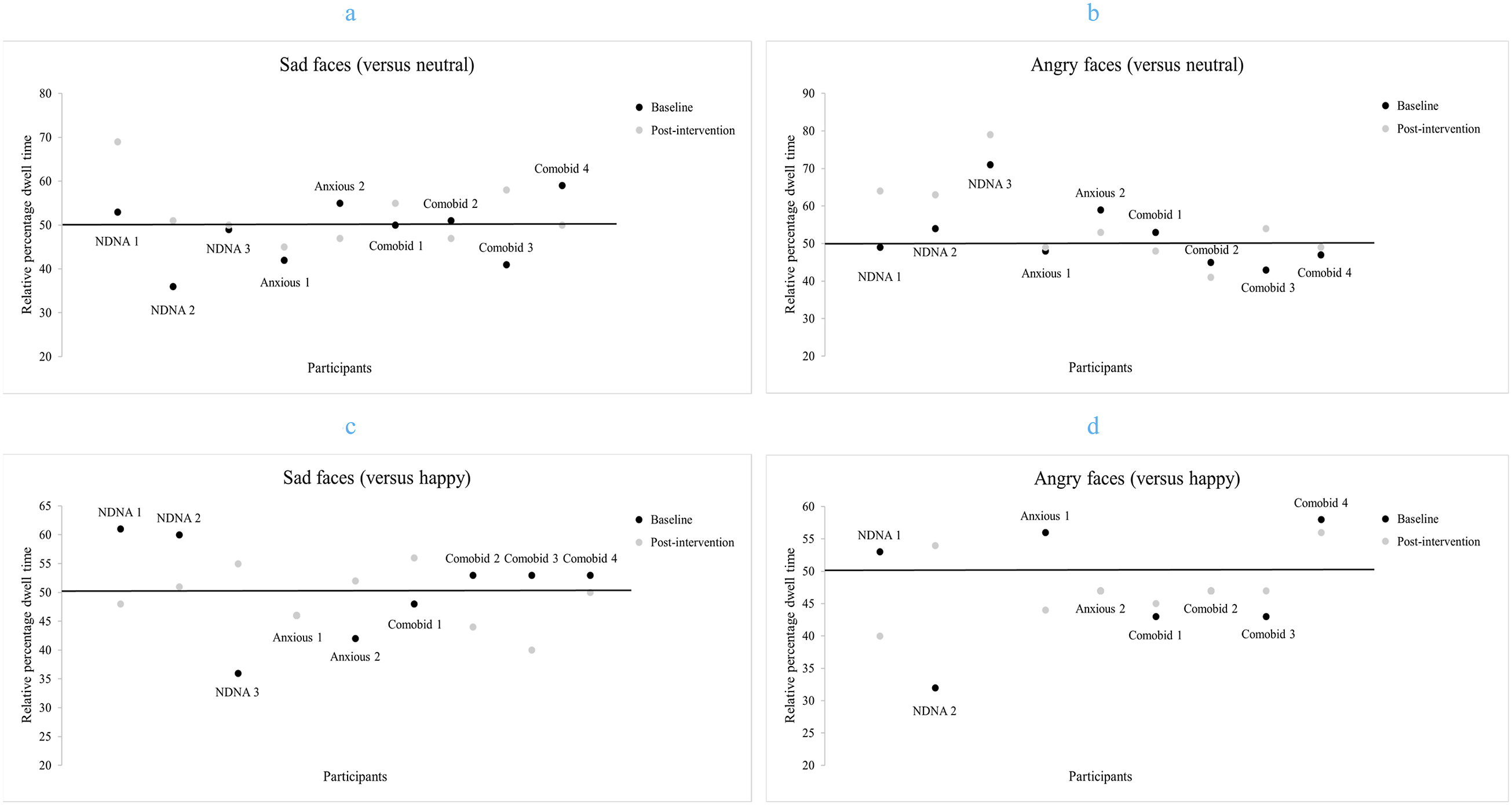
Negative Attentional Biases
In negative-neutral pairings, baseline NAB (an AB score above 50%) were more pronounced post-intervention for the NDNA participants (see Figures 3(a) and 3(b)). In contrast, baseline NAB attenuated/reversed post-intervention (i.e., RPDT reduced) for the anxious and comorbid participants (see Figures 3(a) and 3(b)).
In negative-happy pairings, baseline NAB attenuated/reversed post-intervention for the NDNA, anxious, and comorbid participants (see Figures 3(c) and 3(d)).
Avoidant Attentional Biases
In negative-neutral pairings, baseline avoidant AB (an AB score below 50%) attenuated/reversed for the NDNA, anxious, and three of the four comorbid participants (see Figures 3(a) and 3(b)).
In negative-happy pairings, baseline avoidant AB attenuated/reversed for the NDNA, anxious, and comorbid participants. No post-intervention AB change was seen for three individuals (i.e., Anxious 1 [sad-happy pairings], Anxious 2 and Comorbid 2 [angry-happy pairings]) (see Figures 3(c) and 3(d)).
Study 1 Discussion
The aims of Study 1 were to assess whether GCM-ABM could be done and should continue to be explored as our trial design (i.e., potential exposure to both consonant and dissonant music) had not been previously investigated. GCM-ABM could be done if there was an awareness of the consonant and dissonant track versions(/a change) and their contingency, and deliberate gaze-control was attempted. Exploration would continue in Study 2 if reduced NA, SR, and NAB were found post-intervention in descriptive data. Our findings show that GCM-ABM can be done as the majority of participants were aware of the dissonant versions/a change, their contingency (or a gaze-music link), and some used gaze-control to deliberately avoid the dissonant version of the music track. Further, that exploration should continue in Study 2 as reductions in NA, SR, and baseline NAB were found post-intervention in anxious and comorbid group descriptive data. This was important given that some of the theoretical outcomes of ABM are a reduction in NAB and rumination.
However, as our findings are only descriptive, we do not know if the AB changes described here are a result of GCM-ABM or other factors such as cognitive load. For example, the emotional processing of negative stimuli and the experience of negative emotions can be attenuated by introducing high task demand/cognitive load (Maranges et al., 2017; Sebastian et al., 2017; Wang et al., 2016). Dissonant music’s unexpected and complex structure requires a greater degree of information integration during its processing, imposing greater demands on existing cognitive resources than consonant music (Bonin & Smilek, 2016; Bravo et al., 2020; Yoo et al., 2022). The effect of music on cognition may last 10–15 minutes after exposure (Schellenberg, 2005) and our post-intervention AB measure was conducted within this time frame (i.e., 5 minutes post-intervention). Our descriptive data are similar in nature to the attenuation, or reversal of emotional biases observed under divided attention conditions in that NAB can be displayed during a full attention condition but a positive AB under a divided attention condition and vice versa (Knight et al., 2007). It is therefore possible that the anxious and comorbid participants’ cognitive processing/load was impacted at the outset of the AB measure thus displaying the same pattern of response for negative-neutral and negative-emotional pairings. In contrast, the NDNA particpants cognitive processing/load could have been impacted during negative-happy pairings as there is higher conflict between the negative versus positive emotional valences (in emotional-emotional pairings) compared to emotional versus neutral emotional valences (in emotional-neutral pairings), resulting in higher cognitive load. (Greif & Waring, 2018). Thus, for the NDNA particpants, the impact of the music on cognitive processing/load was potentially only evident when the cognitive processing demands of the task increased (Bonin & Smilek, 2016) (i.e., during negative-happy AB measure trials). If GCM-ABM was deemed feasible overall, cognitive load would be considered when determining how to proceed with the intervention.
Another factor that could be considered is arousal. While arousal levels were not directly assessed, increased arousal, indirectly demonstrated by the NDNA participants’ higher post-intervention scores for affective states such as ‘alert’ (Posner et al., 2005), may have increased the saliency of emotional faces when paired with neutral faces (Mather & Sutherland, 2011), and possibly resulted in the uniformed increase in RPDT on emotional faces. In contrast, the anxious and comorbid participants reported reductions in PA levels (i.e., less arousal) and did not show this uniformed increase in RPDT on emotional faces. While these reductions may be in line with the lowered energy levels/fatigue and boredom reported in the semi-structured interview, it could also be associated with depression- and/or anxiety-related factors, such as an inability to maintain (initial) positive affect levels over time (i.e., the course of the session), and a high level of instability in the experience of positive affect (Heller et al., 2009; Pawluk et al., 2021). The consequence of PA reduction on depression and anxiety levels should be considered, and PA would be assessed in Study 2.
Encouragingly, the music/GCM-ABM blocks were more engaging, increased engagement, or were preferred by the majority of participants, even though the dissonant music version was included in these blocks. However, task instruction and the level of dislike of the dissonant music version would need to be considered when determining how to proceed with the intervention as it may influence if and how much deliberate gaze-control is used. And while we only had one report of irritableness and lack of enjoyment on account of the dissonant music and the participant’s (Comorbid 3) NA/irritable score did not increase post-intervention, proceeding with multiple sessions of GCM-ABM in Study 2 would provide an opportunity to examine repeated exposure to the dissonant music versions.
Study 2
The aims of Study 2 were to assess whether GCM-ABM could be done and should continue to be explored in a larger study. We examined participant adherence and dropout, and if there was any modulation of momentary mood, TR, depression, anxiety, and baseline NAB after four daily sessions. Four sessions were conducted as a previous ABM study (Wells & Beevers, 2010) showed significant reductions in symptoms following four sessions, and the number of training sessions can significantly influence post-intervention effects, with a larger number of training sessions being associated with larger effects (Hang et al., 2021; Jones & Sharpe, 2017).
Study 2 Materials and Methods
Participants
Study 2 – Participants’ Mood Score, Symptom Status and Severity, and Bias Scores.
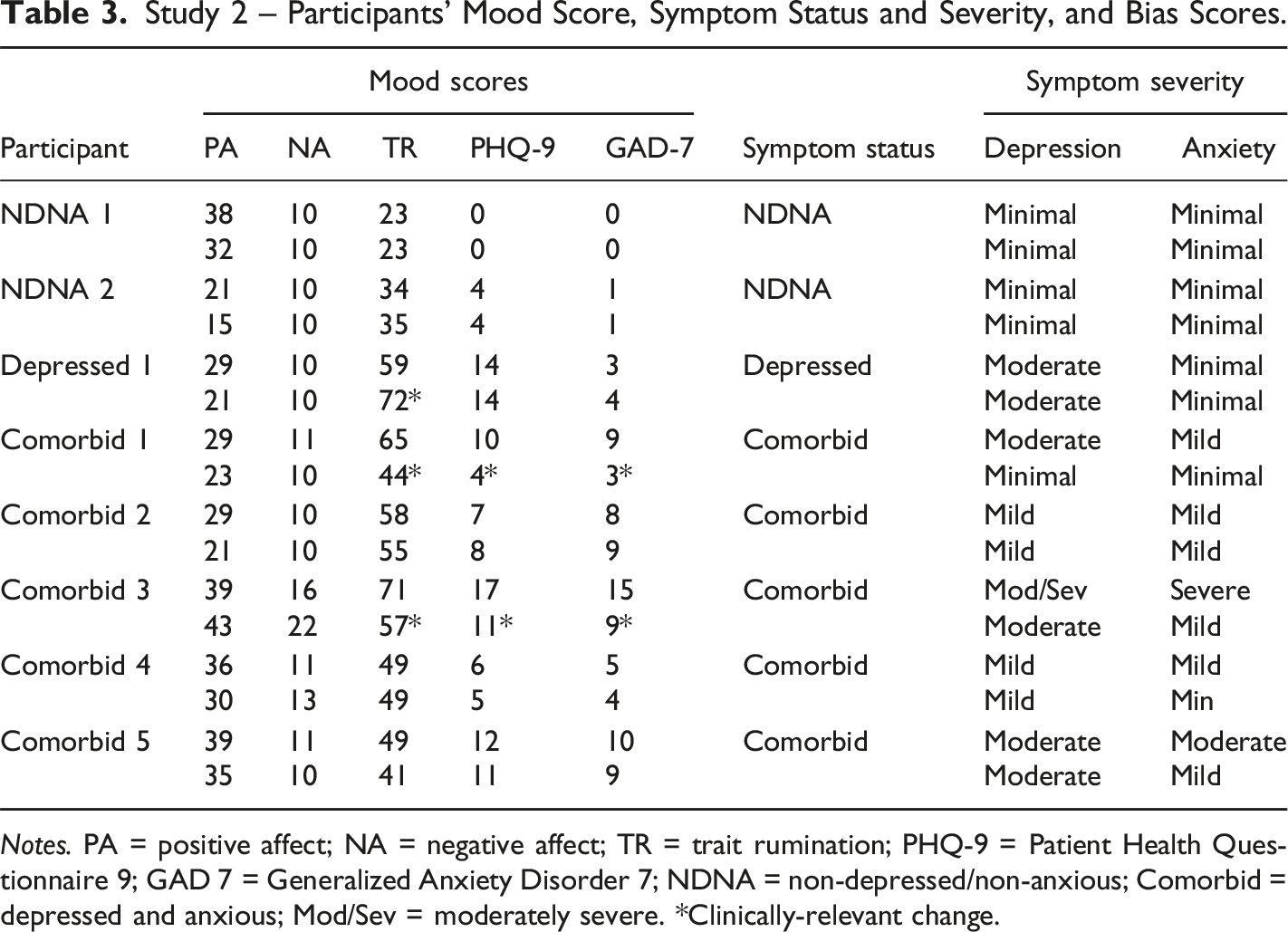
Notes. PA = positive affect; NA = negative affect; TR = trait rumination; PHQ-9 = Patient Health Questionnaire 9; GAD 7 = Generalized Anxiety Disorder 7; NDNA = non-depressed/non-anxious; Comorbid = depressed and anxious; Mod/Sev = moderately severe. *Clinically-relevant change.
Procedure
The participants in Study 2 completed the same tasks, in the same order, as outlined in Study 1’s procedure except (1) the SR measure was not completed, (2) the tasks were completed once a day, for four days, and (3) the online self-report questionnaire was completed at home, for a second time, after the lab-based session on the 4th day. The depressed participant completed 3 sessions (due to the researcher’s absence) and completed their second online survey at home, after the lab-based session on the 3rd day.
Measures
Participants completed the same (1) momentary mood (PANAS), TR (RRS), depression (PHQ-9), and anxiety (GAD-7) scales, (2) AB-measures, and (3) GCM-ABM blocks as described in Study 1, and they were conducted in the same manner.
Gaze Location
Eye-gaze location was conducted in the same manner as described in Study 1. In the current study, participants were seated between 52 and 66 cms away from the desk.
Thoughts and Feelings About the Music
Participants were provided an opportunity during debriefing to share their thoughts and feelings on the music should they wish.
Data Analysis
Data analysis was conducted in the same manner as described in Study 1. As pre- and post-intervention depression, anxiety, and TR scores were collected in Study 2, clinically-relevant changes in mood scores were examined in line with previous ABM/rumination studies (Roberts et al., 2021; Yang et al., 2015).
Rumination
To examine clinically-relevant changes in TR (RRS) scores, reliable change index (RC) calculations (Jacobson & Truax, 1991) were performed. An RC score of >1.96 indicated a clinically-relevant change (Jacobson & Truax, 1991). RC scores were computed using the formula as seen in (1) (X2 = post-intervention score; X1 = pre-intervention score; Sdiff = the standard error of the difference between the pre- and post-intervention scores).
Clinically-Relevant Changes
Based on psychotherapy literature (Kroenke, 2012; Toussaint et al., 2020), a reduction of 5 points on the PHQ-9 and 4 points on the GAD-7 was used to indicate clinically-relevant changes. Based on ABM literature (Yang et al., 2015), a post-intervention score falling within ±2 standard deviations of the nonclinical group’s mean depression score was used to indicate clinically-relevant changes.
Study 2 Results
Participant Characteristics
Study 2 Group Descriptive, Mood, and Bias Score Data.
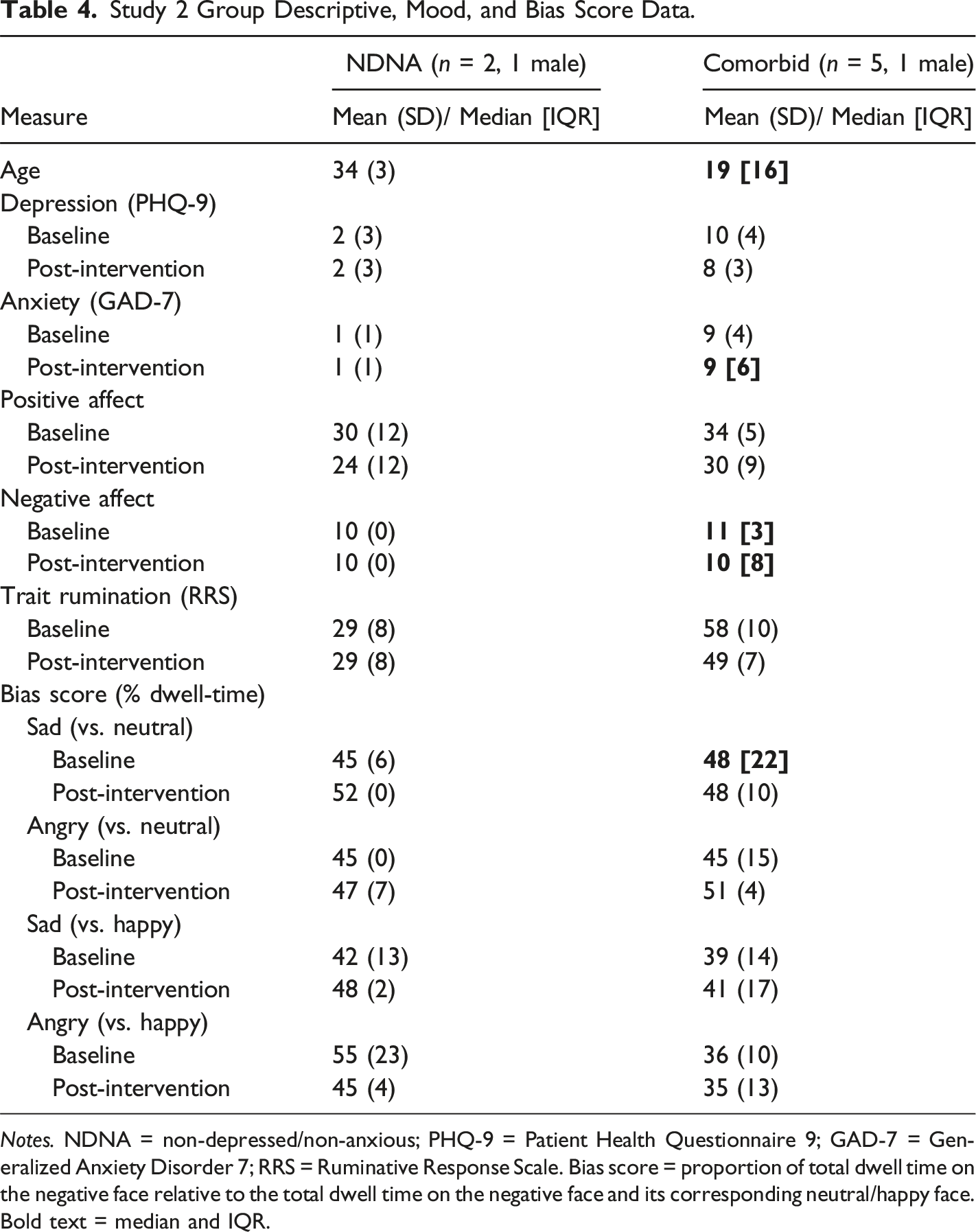
Notes. NDNA = non-depressed/non-anxious; PHQ-9 = Patient Health Questionnaire 9; GAD-7 = Generalized Anxiety Disorder 7; RRS = Ruminative Response Scale. Bias score = proportion of total dwell time on the negative face relative to the total dwell time on the negative face and its corresponding neutral/happy face. Bold text = median and IQR.
Adherence
With the exception of the depressed participant who was unable to complete all of the sessions due to the researcher’s absence, all of the sessions and study components were completed.
Thoughts and Feelings About the Music
Five participants opted to/had time to provide comments about the music. All of these participants were aware of the dissonant version/a change. None of these participants used the term dissonant, rather, terms such as ‘distorted’, ‘disconcerting’, ‘key change’, and ‘minor’ were used. Three participants described the contingency, with two applying gaze-control to avoid the dissonant versions (e.g., ‘…I realised that the music changed according to the image I looked at….so it made me avoid looking at the sad images.’). Of note, one participant with contingency awareness and deliberate gaze-control described differing responses to the dissonant music versions and consequential use of gaze-control (i.e., ‘Harps made me anxious. Harps made me want to avoid the expression that were sad or not neutral. Whereas with violins, I was able to look at both [faces] and was able to look at the sad expressions longer’).
Momentary Mood
Positive Affect
Average PA scores (e.g., items such as ‘enthusiasm’ and ‘active’) reduced post-intervention for the NDNA group (6 points) and comorbid group (4 points) (see Table 4 and Supplemental Material for PA item scores).
Negative Affect
Average NA scores did not change post-intervention for the NDNA group. Average NA scores decreased post-intervention for the comorbid group (1 point) (see Table 4 and Supplemental Material for NA item scores).
Trait Rumination
Average TR scores did not change post-intervention for the NDNA group. Average TR scores decreased post-intervention for the comorbid group (9 points) (see Table 4). Three participants (i.e., Depressed 1, Comorbid 1, and Comorbid 3) reported clinically-relevant score changes post-intervention as RC scores of >1.96 were computed (see Table 3 and Supplemental Material Table S8. for individual RC scores).
Depression
Average depression scores did not change post-intervention for the NDNA group (see Table 4). Average depression scores reduced post-intervention for the comorbid group (2 points). Two participants (Comorbid 1 and Comorbid 3) reported clinically-relevant score changes post-intervention when using literature-based thresholds of 5 points (Kroenke, 2012) and 2 standard deviations of the non-clinical participants’ average depression score (Yang et al., 2015).
Anxiety
Average anxiety scores did not change post-intervention for the NDNA group and comorbid group (see Table 4). Two participants (Comorbid 1 and Comorbid 3) reported clinically-relevant score changes post-intervention when using a literature-based threshold of 4 points (Toussaint et al., 2020).
Attentional Biases
Emotional-Neutral Pairings
Sad Faces
RPDT on sad faces increased post-intervention for the NDNA group (7%). RPDT on sad faces did not change post-intervention for the comorbid group (see Table 4).
Angry Faces
RPDT on angry faces increased post-intervention for the NDNA group (2%) and comorbid group (6%) (see Table 4).
Negative-Happy Pairings
Sad Faces
RPDT on sad faces increased post-intervention for the NDNA group (6%) and comorbid group (2%) (see Table 4).
Angry Faces
RPDT on angry faces reduced post-intervention for the NDNA group (10%) and the comorbid group (1%) (see Table 4).
Exploratory Analyses
Exploratory non-parametric analyses were conducted due to the small sample. Wilcoxon signed rank tests showed that the difference between T1 and T2 PA, NA, and AB scores were non-significant for each group (see Supplemental Material S6. and S7. for non-significant test data).
Individual Biases
As the groups comprised individuals with baseline AB towards and away from negative faces, which affects group averages, individual AB data were plotted to examine the direction of AB change (see Figure 4(a)–4(d)). Individual Baseline and Post-intervention Relative Percentage Dwell Times For Emotional-Neutral and Emotional-Emotional pairings Notes. NDNA = non-depressed/non-anxious. Relative percentage dwell time = proportion of total dwell time on the negative face relative to the total dwell time on the negative face and its corresponding neutral/happy face. Negative-neutral and negative-happy pairings are shown in Figures 4(a) and (b), and Figures 4(c) and (d), respectively. AB attenuated, reversed, or became more pronounced post-intervention. Only NDNA 2, Comorbid 1, and Comorbid 3 showed consistent AB change directions in negative-neutral and negative-happy pairings (Figures 4(a)-4(d)).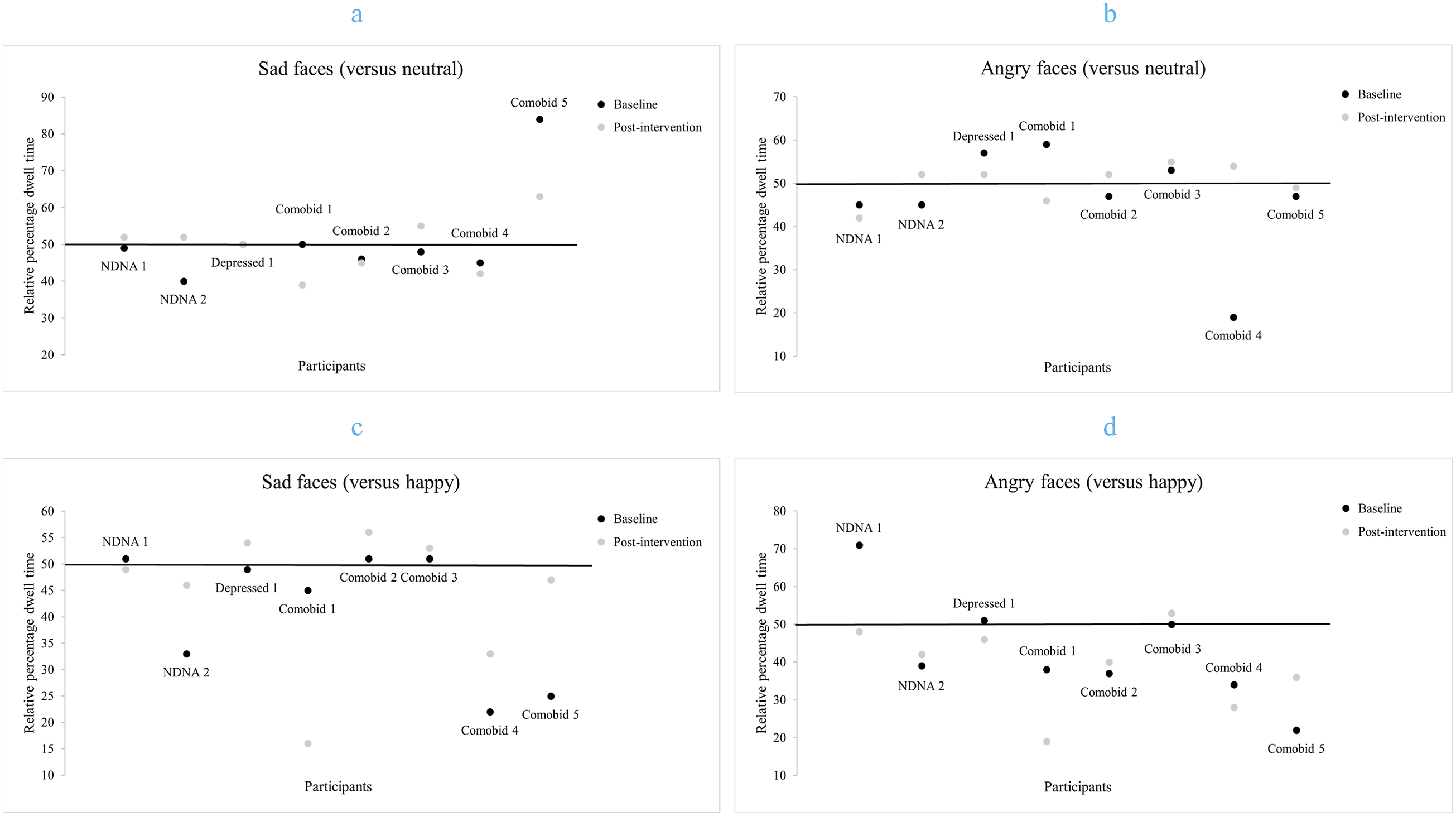
Negative Attentional Biases
In negative-neutral pairings, no NDNA participants displayed baseline NAB (an AB score above 50%) (see Figures 4(a) and 4(b)). Baseline NAB attenuated/reversed post-intervention for the depressed and comorbid participants (except Comorbid 3 for angry faces) (see Figures 4(a) and 4(b)).
In negative-happy pairings, baseline NAB reversed post-intervention for the NDNA and depressed participants (see Figures 4(c) and 4(d)). Baseline NAB were more pronounced for the comorbid participants (see Figures 4(c) and 4(d)).
Avoidant Attentional Biases
In negative-neutral pairings, baseline avoidant AB (an AB score below 50%) reversed for the NDNA participants (except NDNA 1 for angry faces). Baseline avoidant AB attenuated/reversed for the comorbid participants (except Comorbid 2 and Comorbid 4 for sad faces) (see Figures 4(a) and 4(b)).
In negative-happy pairings, baseline avoidant AB attenuated/reversed for the NDNA and depressed participants (see Figures 4(c) and 4(d)). Baseline avoidant AB attenuated for comorbid participants (except Comorbid 1 for sad and angry faces, and Comorbid 4 for angry faces) (see Figures 4(c) and 4(d)).
Study 2 Discussion
The aims of Study 2 were to assess whether GCM-ABM could be done and should continue to be explored in a larger study as it was unknown whether participants would engage in multiple sessions of exposure to the paradigm, and changes in PA, NA, TR, depression, anxiety, and NAB after four daily sessions would be found. Our findings show that GCM-ABM can be done (i.e., participants attended all sessions, completed all self-report measures, and there were no dropouts), and should be further explored (i.e., reductions in TR, depression, anxiety, and NAB were found post-intervention in comorbid participants’ [some individuals and/or group] descriptive data).
We generally found reductions in PA scores post-intervention, even for the participants reporting lower depression and anxiety scores. The largest reductions were seen in ‘enthusiasm’ and ‘active’ which could be in line with literature (Beard et al., 2012; Chan et al., 2022; Kuckertz et al., 2020) outlining participant boredom and fatigue/tiredness when taking part in ABM interventions. NA scores were largely unaffected post-intervention (i.e., no change seen for the NDNA group/four of the eight participants).
TR reduction was more evident in comorbid participants (seen in four out of the five participants). The comorbid participants (Comorbid 1, and Comorbid 3) with clinically-relevant reductions in TR also showed clinically-relevant reductions in depression and anxiety. The participant with a clinically-relevant increase in TR also showed a 1-point increase in their anxiety score. This participant completed three of the four GCM-ABM sessions due to researcher absence so it is unknown whether post-intervention TR and/or symptoms would have been higher or lower after the full number of GCM-ABM sessions.
Only three participants (NDNA 2, Comorbid 1, and Comorbid 3) showed a consistent AB change direction across emotional-neutral and emotional-emotional pairings. NAB were reduced post-intervention in the majority of instances. While increases in RPDT on negative faces were found post-intervention for avoidant AB, there were also findings in-keeping with traditional ABM responding (i.e., more pronounced AB away from negative faces) (Eldar et al., 2012). Although it is undesirable to increase avoidance, as avoidance is associated with poor outcomes (Eldar et al., 2012; Waters & Kershaw, 2015), our findings show that an individual can show NAB in negative-neutral pairings, but avoidance in negative-happy pairings (and vice versa) (e.g., NDNA 1 and Comorbid 5). As such, future research should explore which emotional contrasts (negative-neutral or negative-happy) are more closely associated with an individual’s depression and anxiety symptoms/post-intervention changes.
GCM-ABM Evaluation
The findings from Study 1 and 2 showed that GCM-ABM was feasible. As such, an evaluation (i.e., what did and did not work) was performed to guide how to proceed further.
Music Switch, Its Contingency, and Use
All of the participants were aware of the dissonant version/a change occurring across the studies demonstrating that having consonant and dissonant versions of a track in one trial can work. Moreover, some participants were indeed motivated to look towards the more positive faces to avoid hearing the dissonant version/s. However, only a minority of participants were aware of the contingency and used deliberate gaze-control to avoid the dissonant versions. Consequently, allowing the participants to discern the contingency and their control over the music, and understand they could override the explicit task instructions did not work so well. Further, deliberate gaze-control to avoid the dissonant versions may, for some, be linked to how aversive the dissonant track was to the participant (i.e., the less aversive dissonant version was tolerated or played with and so viewing of the negative faces proceeded).
As such, the following research questions could be addressed to better understand how to proceed with GCM-ABM: (1) Does explicit instructions regarding gaze-control and the music effect mood and NAB post-intervention? (2) Would the use of the participant’s most disliked dissonant version across the GCM-ABM blocks have a positive effect on mood and NAB post-intervention?
Point 2 raises a more general questions about the number of tracks to be used moving forward. One participant liked both tracks and found their dissonance versions ‘interesting’ rather than aversive. The music tracks used in these studies were specifically created with the intention to control their dissonance level. While it may be too difficult/time consuming to create a dissonant version of each participant’s own choice of music, their preference/most disliked/discernible in terms of change could potentially be obtained/selected from a wider range of created tracks. Thus, a music selection phase would need to be incorporated into the study design.
Number of Sessions
While it was encouraging that some participants reported lowered NA, SR, TR, depression, and anxiety scores after single- and/or multi-session GCM-ABM (Study 1 and 2, respectively), clinically-relevant reductions in depression and anxiety were seen in only two participants (Study 2). One explanation could be that the low number of sessions did not work so well, and more than four training sessions are required to reduce TR and symptom levels in some participants. The number of training sessions, which can vary across interventions, has been shown to be a significant moderator in ABM (Hang et al., 2021; Jones & Sharpe, 2017). As such, the following research questions could be addressed to better understand how to proceed with GCM-ABM: (1) Should the number of GCM-ABM sessions be personalised (i.e., participant response-led)? (2) Should the number of GCM-ABM sessions be defined from a GCM-ABM study-specific average or be literature-based?
Point one would necessitate multiple/periodic depression and anxiety assessments across the intervention to assess whether to continue or discontinue the GCM-ABM sessions. Alternatively, eight sessions have been used and produced clinically-relevant results in another music-based study, thus eight GCM-ABM sessions with a mood assessment in session 4 and 8 is a justifiable procedural change.
Additional Study Design Changes
In these initial stages of GCM-ABM exploration (Study 1 and 2), convenient sampling was used, participants were classified as depressed and/or anxious based on scale cut-off levels, and clinical history was not assessed. However, as symptom type and clinical history can effect AB presentation, symptom type may effect ABM response, and ABM efficacy may be effected/partially mediated by bias presence and change (Beevers et al., 2021; Clarke, Notebaert, & MacLeod, 2014; Hankin et al., 2010; Kishimoto et al., 2021; LeMoult & Joormann, 2012; Martinelli et al., 2022), participants in subsequent GCM-ABM studies will have a clinical assessment to establish history and symptom type/s (including primary diagnosis where there is comorbidity) and will be screened for the presence of negative AB. The inclusion criteria will be extended to include 1) participants with negative AB, 2) participants with a clinical diagnosis of only depression (MDD), only anxiety (GAD), and comorbid depression and anxiety (MDD and GAD).
Additionally, there is a potential for cognitive load to be a contributing/explanatory factor when comparing our descriptive findings with previous research (Knight et al., 2007). As such, a measure of cognitive load would be incorporated into the study design. Pupil size (dilation), a metric associated with cognitive load/effort, will be analysed in subsequent GCM-ABM studies and the next GCM-ABM design version will include baseline pupil size measures with minimal effort for the participant (e.g., recording the pupil for 500 ms before the target slide onset to establish a baseline pupil diameter) (Lisi et al., 2015; van der Wel & van Steenbergen, 2018) (see Mathôt and Vilotijevic (2023) for example cognitive pupillometry study design and analyses considerations and recommendations).
Overall Discussion
Two feasibility studies (Study 1 and 2) were conducted with the aims of identifying whether GCM-ABM could be done, whether GCM-ABM should continue to be explored, and if so, how. Previous studies examining music and visual attention (Arriaga et al., 2014; Bonin & Smilek, 2016) have exposed participants to either positive or negative music when viewing stimuli in a single trial – not both. Our finding show that GCM-ABM can be done as there was an awareness of the consonant and dissonant track versions(/a change) and their contingency, deliberate gaze-control was attempted (Study 1 and 2), and participants adhered to the study with no participant dropout (Study 2). Further, GCM-ABM should continue to be explored as reduced negative affect (or no change) (Study 1 and 2), state rumination (Study 1), trait rumination (TR), depression, anxiety (Study 2), and baseline negative attentional biases (NAB) (Study 1 and 2) were found post-intervention for some individuals in the descriptive data.
However, these changes were not significant and the factor/s (e.g., GCM-ABM, cognitive load, and/or the music) associated with these changes is/are yet to be determined. Additionally, the lowered positive affect scores reported by the majority of participants post-intervention may possibly be attributed to general feelings about ABM procedures (e.g., fatigue) (Beard et al., 2012; Chan et al., 2022; Kuckertz et al., 2020). Participants reported having less energy/fatigue after GCM-ABM, therefore GCM-ABM did not overcome this issue. Still, participants found the GCM-ABM blocks more engaging/increased engagement compared to the dot-probe blocks. All-in-all, GCM-ABM was deemed feasible. As such, an evaluation of the findings from Study 1 and 2 was conducted to guide how to proceed with GCM-ABM. The outcome of this evaluation was that our research design requires modification (e.g., task instructions, dissonant track selection, and the number of sessions to be administered).
Our findings contribute to the limited emotional-emotional (e.g., angry-happy) AB data as the majority of AB research stems from emotional-neutral experimental paradigms (Blanco et al., 2019). Our findings also highlight the need to examine different types of contrasts. ABM avoidance training for individuals who do not display a NAB, or show attentional avoidance, is not ideal as avoidance is associated with poor interventional outcomes (Eldar et al., 2012; Waters & Kershaw, 2015). While an avoidant AB may reduce distress in the short term, it is maladaptive in the long term (Mogg & Bradley, 2018). However, a participant could display no baseline NAB and a post-intervention NAB within emotional-neutral pairings, but a baseline NAB which was reduced post-intervention within emotional-emotional pairings in the current studies. Examining emotional-neutral alongside emotional-emotional contrasts may lead to a better understanding of the relationship between AB and symptoms, and ABM therapeutic effects (Lazarov et al., 2017).
Limitations and Future Studies
The significant limitations of these studies include the small and predominantly female convenience samples recruited using minimal inclusion criteria, the lack of a clinical diagnoses of neuropsychiatric symptoms, and that clinical history was not assessed. Additionally, a control condition (e.g., non-contingent music and/or traditional ABM) to isolate the effect of GCM-ABM was not included, the exploratory analyses were underpowered, confounding factors (e.g., baseline symptoms and gender) were not controlled, and our conclusions rely on descriptive data as the interpretation of AB and affective changes lacks statistical support. These limitations effect the generalisability, external validity, and strength of our findings and conclusions. Future GCM-ABM studies will 1) be conducted with larger samples, 2) screen and select participants based on AB presentation and clinically assessed neuropsychiatric status, 3) include control condition/s, and 4) conduct subgroup (e.g., single, primary, and comorbid diagnosis, and first episode vs. multiple episodes) and controlled analyses.
Another potential limitation of our study is the number of training sessions as it has been shown to be a significant moderator in ABM (Hang et al., 2021; Jones & Sharpe, 2017). It is possible that more than four training sessions are required to reduce TR, depression, and anxiety levels in some participants. Additionally, a longer stimuli presentation duration will be incorporated within the GCM-ABM and AB measurement tasks. It may be possible that a longer stimuli presentation time is required for GCM-ABM, and longer stimuli presentation durations within AB measures are more reliable and demonstrate strong test-retest reliability (Lazarov et al., 2016; Sears et al., 2019).
Clinical/Research Implications
Our descriptive findings suggest that the same emotional expression can show opposing AB direction (towards or away) at baseline in negative-neutral pairings and negative-happy pairings, and AB change (i.e., pronounced/attenuated/reversed) can be opposing for the same expression in negative-neutral pairings compared to negative-happy pairings following an intervention. Consequently, emotional-neutral and emotional-emotional contrasts should be examined in future. GCM-ABM was deemed feasible and was found to be more engaging than the dot-probe AB task. However, as only two of the six participants classified as depressed or comorbid (Study 2) showed clinically-relevant reductions in symptoms, GCM-ABM in its current form has questionable efficacy. GCM-ABM will therefore be modified based on our evaluation outcomes (e.g., increasing the number of sessions) and further explored with larger samples of clinically-assessed individuals to determine what effect, if any, GCM-ABM has on mood and AB through appropriate analyses.
Supplemental Material
Supplemental Material - Gaze-Contingent Musical Attentional Bias Modification: Exploring Feasibility and Clinically-Relevant Changes in Mood
Supplemental Material for Gaze-Contingent Musical Attentional Bias Modification: Exploring Feasibility and Clinically-Relevant Changes in Mood by Anne-Marie Greenaway, Faustina Hwang, Slawomir Nasuto, Aileen K. Ho in Psychological Reports
Supplemental Material
Supplemental Material - Gaze-Contingent Musical Attentional Bias Modification: Exploring Feasibility and Clinically-Relevant Changes in Mood
Supplemental Material for Gaze-Contingent Musical Attentional Bias Modification: Exploring Feasibility and Clinically-Relevant Changes in Mood by Anne-Marie Greenaway, Faustina Hwang, Slawomir Nasuto, Aileen K. Ho in Psychological Reports
Footnotes
Acknowledgements
This project has been supported by a University of Reading Strategic PhD Studentship and by the School of Biological Sciences. Thanks to the Hilda Martindale Educational Trust and Funds for Women Graduates Educational Charity for their non-project student awards.
Declaration of Conflicting Interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Considerations
The study was reviewed in accordance with the procedures of the University of Reading’s Research Ethics Committee and received a favourable ethical opinion for conduct (UREC 19/71).
Consent to Participate
Consent was provided during study enrolment (written), at the start of the online survey (checked tick box), and at the start of the lab-based session (written).
Data Availability Statement
The authors confirm that the data supporting the findings of this study are available within the article and its Supplemental Materials.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.