
Abstract
Obsessive Compulsive Disorder (OCD) and Autism Spectrum Disorder (ASD) have similar characteristics. People with one of these disorders are more likely to meet the diagnosis of the other disorder than the general population. This study mainly investigated whether autistic traits predicted obsessive-compulsive symptom subtypes after controlling for some demographic features and clinical variables. This study included 460 university students from two universities and their family members. The subjects were asked to complete a sociodemographic and clinical data form, the Vancouver Obsessional Compulsive Inventory (VOCI), the Autism-Spectrum Quotient (AQ), the Beck Depression Inventory (BDI) and the Beck Anxiety Inventory (BAI). The relationship between autistic symptoms and obsessive-compulsive symptoms was assessed using linear regression analysis, controlling for age, sex, depression, anxiety scores, and a history of frequent childhood upper respiratory tract infections (URTIs). The AQ attention-switching score was associated with hoarding (β = 0.135, p = .002), just-right (β = 0.087, p = .026), indecisiveness (β = 0.101, p = .006), and total VOCI (β = 0.080, p = .038) score. AQ subscale scores other than attention-switching were not associated with VOCI scores. Age was negatively associated with obsessions (β = −0.133, p = .001), just-right (β = −0.129, p = .002), indecisiveness (β = −0.214, p < .001), and total VOCI score (β = −0.109, p = .006). BDI and BAI total scores were positively associated with all VOCI scores (all β in between 0.114 and 0.318, all p in between 0.033 and <0.001). Checking (p = .025), just-right (p = .038), and total VOCI scores (p = .046) were significantly higher in the group with a history of frequent childhood URTIs compared to the group without. Individuals with OCD symptoms may exhibit attention-switching deficits similar to those of individuals with ASD symptoms, suggesting a subgroup of OCD that shares features with ASD. Attention-switching deficits should be further investigated in terms of the relationship between ASD and OCD.
Introduction
Obsessive-compulsive disorder (OCD) and autism spectrum disorder (ASD) are common disorders in the general population and cause significant functional impairment. These disorders share several common characteristics, including cognitive inflexibility, repetitive behaviours, and impaired social skills (Jiujias et al., 2017). Meier et al. (2015) reported that people diagnosed with ASD were twice as likely to be subsequently diagnosed with OCD, and people diagnosed with OCD were four times as likely to be subsequently diagnosed with ASD. Furthermore, a study conducted by Russel et al. (2005) found that obsessive-compulsive symptoms are frequently observed in patients with Asperger syndrome and high-functioning autism, and these symptoms are significantly associated with higher distress. Bejerot et al. (2001) reported that using a video recording method, 20% of OCD patients showed pronounced autistic traits (4). Tumkaya et al. (2014) also found that patients with OCD, like patients with ASD Jellema et al. (2009), exhibit impaired spontaneous attention to social cues through a behavioral task and an eye-tracking method (Tumkaya et al., 2020). All these findings support the hypothesis that there is a relationship between OCD and ASD.
It has been suggested that the phenomenological similarities between OCD and ASD are one of the reasons OCD was moved from the anxiety disorders category to the obsessive-compulsive and associated disorders category in the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) (American Psychiatric Association, 2013). In particular, the repeated behaviors seen in OCD patients more closely resemble symptoms of ASD than anxiety disorders, even though the anxiety experienced by many OCD patients is similar to that of anxiety disorders. These behaviors in OCD often include ordering and symmetry compulsions, as well as actions driven by a “not-just-right' feeling (Ivarsson & Melin, 2008). Furthermore, it has been suggested that OCD patients who exhibit the above traits may constitute a distinct subgroup distinguished by more severe OCD symptoms and higher depression and anxiety levels (Calamari et al., 1999). These observations raise the possibility that there may be a subgroup who have autistic-like traits within the OCD spectrum (La Buissonniere-Ariza et al., 2018; Storch et al., 2016).
On the other hand, some OCD patients, even if they do not meet the DSM-5 criteria for hoarding disorder, may have some hoarding symptoms and abnormal object attachment (Yap et al., 2020), similar to the patients with ASD often developing abnormal attachment to objects (Spikins et al., 2018). According to research on autistic children with anxiety symptoms, 25%–34% exhibit hoarding behavior (La Buissonniere-Ariza et al., 2018; Storch et al., 2016).
Wakabayashi et al. (2012) examined the relationship between autistic traits and OCD symptoms using the Padua Inventory in university students; they found that impaired control of mental activities and impulsiveness subscales predicted the total AQ score. In a more recent study focusing on the relationship between OCD symptom severity and autism symptoms, it was reported that the Yale-Brown Obsessive Compulsive Scale (Y-BOCS) total score showed positive correlations with the AQ total score, and the social skills, attention-switching, communication, and imagination subscales in a clinical sample of 106 OCD patients (Doi et al., 2021). Barnard-Brak et al. (2021) found that the severity of obsessions and compulsions was equally associated with ASD symptoms in a sample of 217 community-dwelling individuals, but when analyses were restricted to individuals meeting the ASD threshold, only the severity of compulsions was found to predict the severity of ASD symptoms. Based on these findings, the authors emphasized the importance of compulsions as a treatment target in individuals with ASD symptoms (Barnard-Brak et al., 2021). To our knowledge, only one study in the literature has examined the relationship between specific OCD symptom dimensions and ASD symptoms. This study, using a clinical sample including 109 OCD patients, found that attention-switching deficits, one of the ASD symptoms were associated with all OCD symptom subtypes (aggression/checking, symmetry/ordering, and contamination/washing) except hoarding (Anholt et al., 2010). However, this study did not take into account the effects of anxiety and depressive symptoms. In addition, there may be other variables that affect OCD symptoms. For example, it has been proposed that several autoantibodies, thought to be triggered by upper respiratory tract infections (URTIs), may induce or increase OCD symptoms by affecting the basal ganglia (Vreeland et al., 2023). It has also been reported that the severity of some OCD symptom subtypes may differ between men and women (Labad et al., 2008). Therefore, the current study aimed to investigate the relationship between specific obsessive-compulsive symptom subtypes and ASD symptom dimensions, controlling for possible confounding effects of some demographic features and clinical variables in a large community-based sample.
Based on all these findings, this study aimed to examine the relationships between specific obsessive-compulsive and autism spectrum symptom dimensions in a large community-based sample. The main hypothesis of this study was that autistic traits would predict OCD symptoms, especially those characterized by repetitive behaviors, independently of the effects of other possible confounding variables. As a secondary aim, this study also aimed to collect preliminary data on a history of frequent URTIs in childhood, which has been suggested in the literature to play a role in the etiology of OCD and to investigate its relationship with OCD symptoms (Descalço et al., 2023; Orlovska et al., 2017).
Methods
Participants
This is a cross-sectional, community-based study using convenience sampling. To represent a wide age range of participants, the study sample included medical students from Pamukkale University and Gazi University in Turkey, or first-degree relatives (mother, father, or sibling) of these students. Two researchers—AOY and VA—who are actively involved in student organizations, coordinated the survey distribution of under the supervision of FK and ST. Each potential participant was approached individually and invited to participate, either themselves or through their relatives.
Materials
Data were collected through an online survey via Google Forms.
The survey link was distributed directly via email and instant messaging platforms such as WhatsApp; no public advertisements were utilized. The survey form was tested for functionality prior to data collection. The invitation message explained the study’s purpose and included a link to the survey. Participants began by checking a box to indicate their voluntary consent to participate in the study. They were then asked if they were a student or a relative and, if a relative, how close their relationship was.
The survey form consisted of five sections: one section for sociodemographic information and four psychometric scales for screening anxiety, depression, obsessive-compulsive symptoms, and autistic traits. The number of total items was 190, taking approximately 20–30 min to complete.
Participation in the survey required the completion of all items, but participants had the option to review or modify their previous responses. To prevent duplicate entries, we enabled the “Limit to 1 response per user” option, which required participants to log in using a Google account; no additional measures, such as IP tracking or cookies, were used. No incentives were offered for participation. The final sample included 181 students, 128 mothers, 110 fathers, and 41 siblings. Ethical approval was obtained from the Non-Interventional Research Ethics Committee of Pamukkale University’s Faculty of Medicine (Date: February 22, 2024, No: 185844). The study was conducted following the principles of the Declaration of Helsinki.
Sociodemographic and Clinical Data Form
Participants were asked about their age, sex, and whether they had frequent URTIs in childhood. The frequency of URTIs history in childhood was asked as “Did you have frequent URTIs with tonsil infections or coughing in childhood (two or more per year)?”. Participants responded to this question by selecting either the “Yes” or “No” option.
The following self-report scales were used to determine the levels of obsessive-compulsive symptoms, autistic traits, anxiety, and depressive symptoms of the participants:
Vancouver Obsessional Compulsive Inventory (VOCI)
It is a 5-point Likert-type scale consisting of 55 items. The scale consists of contamination, controlling, obsessions, hoarding, not just-right and indecisiveness subscales. Higher scores on the scale indicate higher symptom severity (Thordarson et al., 2004). The Turkish version of the scale was reported to be valid and reliable (İnözü & Yorulmaz, 2013). In the current study, the Cronbach alpha value of the scale was found to be 0.96.
Autism-Spectrum Quotient (AQ)
It is a four-point Likert-type questionnaire with a total of 50 questions assessing five different domains. The areas assessed are social skill, attention-switching, attention to detail, communication, and imagination. A score of 1 point is given for answering some questions of the questionnaire as ‘definitely agree’ or ‘slightly agree’, and 1 point is given for answering other questions as ‘slightly disagree’ or ‘definitely disagree’ (Baron-Cohen et al., 2001). The reliability study of the questionnaire was conducted by Köse et al. (2010). In the current study, the Cronbach alpha value of the scale was found to be 0.86.
Beck Depression Inventory
It is a 21-point, four-point Likert-type scale measuring the level of depressive symptoms (Beck et al., 1961). Turkish validity and reliability study was conducted by Hisli (1989) (28). In the current study, the Cronbach alpha value of the scale was found to be 0.92.
Beck Anxiety Inventory
It is a 21-item four-point Likert-type scale developed by Beck et al. to determine the severity of anxiety symptoms (Beck et al., 1988). The validity and reliability study of the Turkish version was conducted by Ulusoy et al. (1998). In the current study, the Cronbach alpha value of the scale was found to be 0.92.
Sample Size Calculation
A post-hoc power analysis was performed using G*Power 3.1, a free software tool. This analysis examined a linear multiple regression model with ten predictors, which included five subscale scores from the Autism-Spectrum Quotient (AQ), along with scores from the Beck Depression Inventory (BDI) and Beck Anxiety Inventory (BAI), as well as factors such as age, gender, and a history of frequent childhood upper respiratory tract infections.
Based on the assumption of a medium effect size (f2 = 0.15), an alpha level of 0.05, and a target power of 0.80, the analysis determined that at least 118 participants were necessary to identify a medium effect. Ultimately, the study included 460 participants, which provided acceptable statistical power and minimized the likelihood of a Type II error.
Statistical Analyses
The relationships between VOCI total score and subscale scores and age and other scale scores used in the study (AQ, BDI, BAI) were evaluated by Pearson correlation analysis, and the possible confounding effect of sex was investigated by univariate statistical analysis (Student-t test). A similar procedure was carried out for participants with and without a history of childhood URTI.
In the next step, the variables that found to have a statistically significant relationship with VOCI subscale scores in correlation analyses and univariate analyses were included in linear regression analyses using the stepwise method as independent variables. In all analyses, a p-value less than .05 was accepted as an indicator of statistical significance.
Results
The study group consisted of 460 participants, of whom 256 were women (55.7%) and 204 were men (44.3%). The mean age of the group was 37.14 ± 14.79 years. The mean scores on the VOCI were as follows: contamination 8.97 ± 8.48, checking 4.64 ± 5.29, obsessions 7.19 ± 8.00, hoarding 3.56 ± 4.83, just-right 9.01 ± 8.23, indecisiveness 5.28 ± 4.80, and total VOCI score 38.68 ± 32.93. The mean scores on AQ were as follows: social skills 3.88 ± 2.75, attention-switching 4.79 ± 1.95, attention to detail 4.87 ± 2.04, communication 4.07 ± 2.76, imagination 4.24 ± 2.16, and total AQ score 21.86 ± 8.40. The mean score of BDItotal was 8.67 ± 8.60, and BAI total was 8.36 ± 9.47.
Correlations Between VOCI Subscale Scores and Age, AQ, BDI, and Bai Scores.
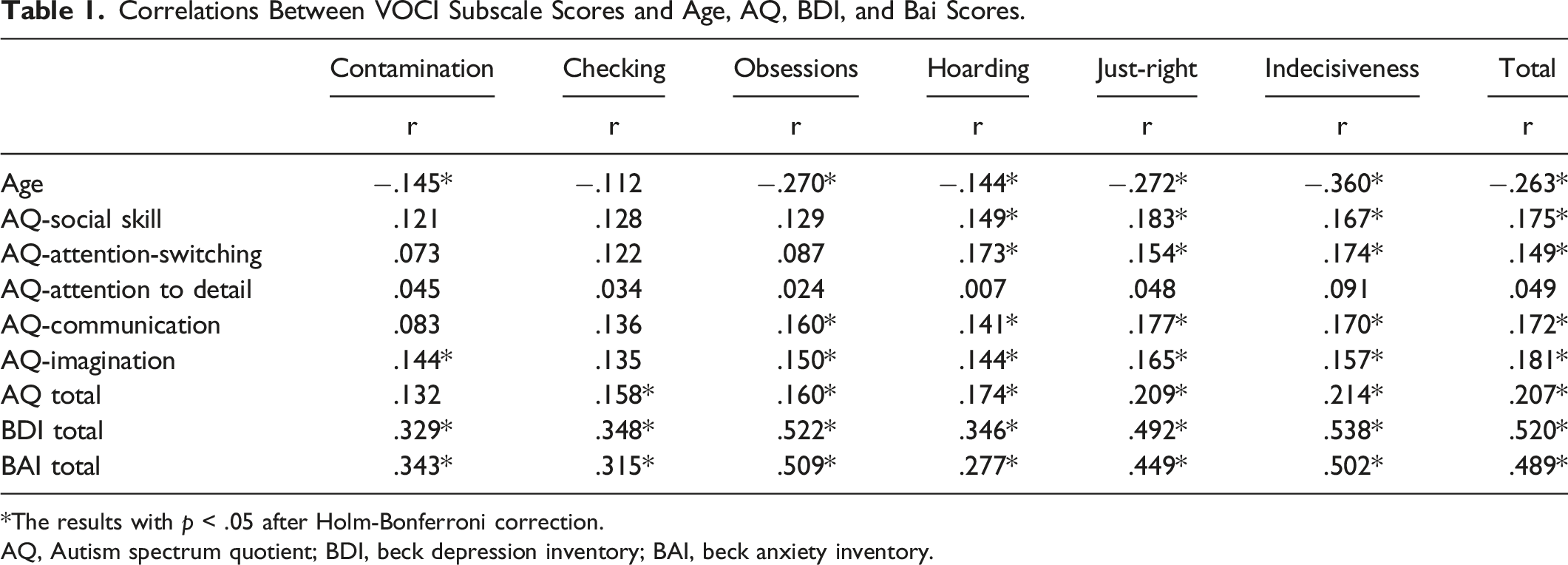
*The results with p < .05 after Holm-Bonferroni correction.
AQ, Autism spectrum quotient; BDI, beck depression inventory; BAI, beck anxiety inventory.
Comparison of VOCI Scores Between Female and Male Groups.
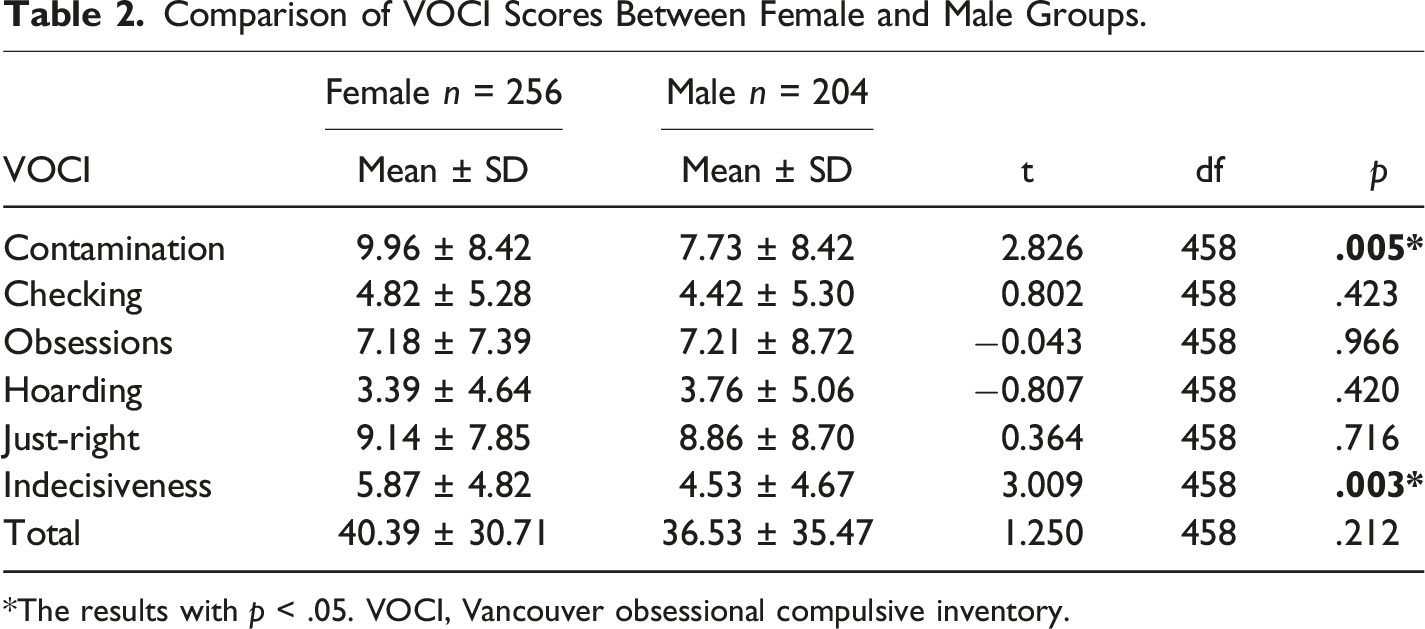
*The results with p < .05. VOCI, Vancouver obsessional compulsive inventory.
Comparison of VOCI Scores Between the Groups With and Without a History of Childhood URTIs.
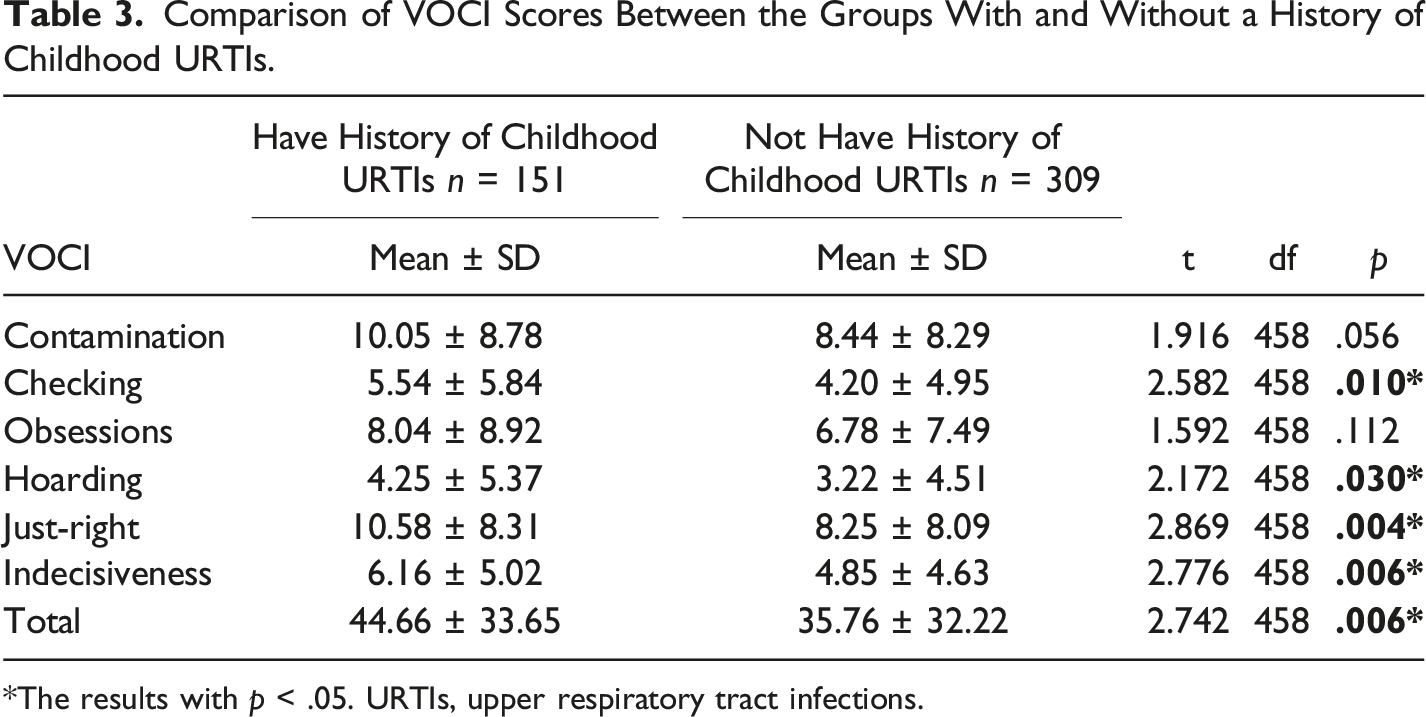
*The results with p < .05. URTIs, upper respiratory tract infections.
Because of the relationships between age, BDI total and BAI total scores, and VOCI scores (Table 3) and taking into account that VOCI scores differed according to sex and the history of childhood URTI (Table 2), all these variables were added as independent variables in the linear regression analyses performed to find the AQ scores predicting VOCI scores.
Multiple Linear Regression Analysis Results, Predictor Factors for VOCI Total and Subscale Scores.
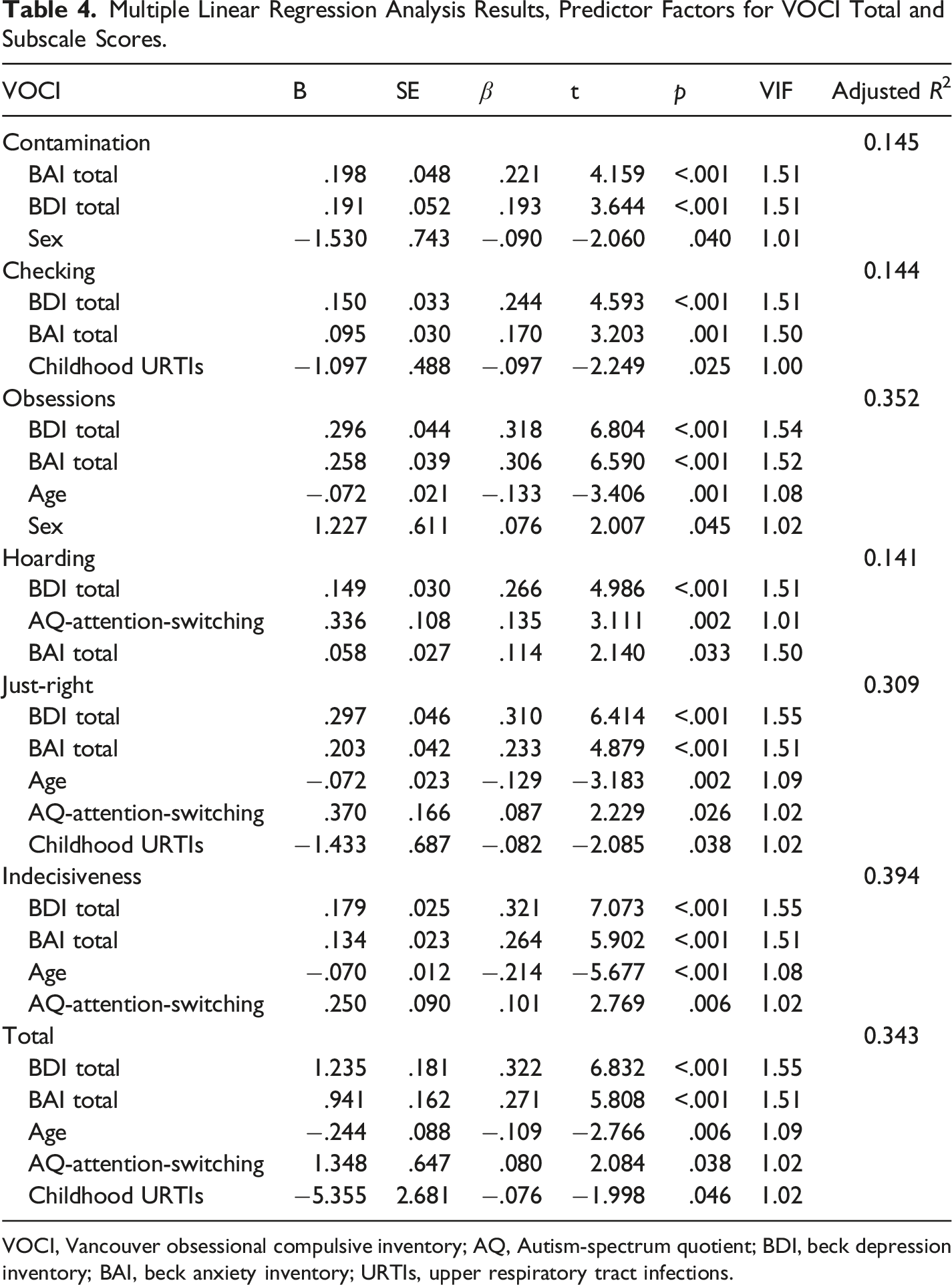
VOCI, Vancouver obsessional compulsive inventory; AQ, Autism-spectrum quotient; BDI, beck depression inventory; BAI, beck anxiety inventory; URTIs, upper respiratory tract infections.
Discussion
This study investigated whether ASD symptoms predicted obsessive-compulsive symptoms in a community-based sample and found that attention-switching problems seen in ASD predict hoarding, just-right, indecisiveness, and total VOCI scores. It is noteworthy that the unique autism symptom that predicts these OCD symptom dimensions is attention-switching problems.
In people with ASD, this problem is seen as concentrating too much on a situation or object and having difficulty shifting their attention to another social or nonsocial stimulus, which distinguishes them from other children with developmental delay (Baranek et al., 2013; Dawson et al., 1998). The findings of this study suggest that obsessive-compulsive symptoms should also be questioned in ASD patients with attention-switching problems. In addition, these results suggest that attention-switching deficits may be a factor exacerbating some aspects of OCD symptomatology. Therefore, it seems important to further investigate this deficit in the context of OCD pathophysiology.
There are other studies in the literature that support the findings of this study. Tumkaya et al. found that OCD patients directed their attention to social cues that were not required for this task (the head region of the cartoons) less than healthy subjects in a task in which they had to judge the distance between two cartoons (Jellema et al., 2009; Tumkaya et al., 2020). Moreover, it was reported that ASD patients showed similar impairments in the same task (Tumkaya et al., 2014). These findings reveal the importance of attention-switching disorders in the relationship between OCD and ASD. Pinto-Gouveia et al. found that attention-switching and attention to detail predicted 36% of OCD symptoms in OCD patients and suggested that these attention problems prevented ignoring repetitive thoughts and extinguishing repetitive behaviors (Pinto-Gouveia et al., 2021). Anholt et al. (2010) also showed that attention-switching problems predicted the severity of OCD symptoms in adults with OCD. The unique prediction of obsessive-compulsive symptoms by attention-switching deficits, one of the ASD symptoms, reveals the importance of attention-switching deficits in the relationship between OCD and ASD pathophysiology. Indeed, phenomenologically, many similarities between OCD patients and ASD patients may be caused by attention-switching deficits. For example, a patient with symmetry obsessions may have difficulty switching attention away from asymmetrical objects, a patient with not-just-right experiences may have difficulty switching attention away from an event that he/she feels is not complete, or a patient with hoarding symptoms may have difficulty switching attention away from an object with which he/she has an attachment. For these reasons, it seems important to investigate the mechanisms of attention-switching deficits both in ASD and OCD and in comorbid conditions.
While the current study did not yield such a finding, certain results reported in the literature may help to better interpret its outcomes. Current scientific evidence has shown that the prefrontal cortex is an important brain region for focusing attention on a task-related area (Miller & Cohen, 2001). The basal ganglia are thought to be involved in controlling the direction of attention (van Schouwenburg et al., 2015). The basal ganglia are brain regions that are thought to be very important in the pathophysiology of both ASD and OCD (Rapoport, 1990; Subramanian et al., 2017). For these reasons, dysfunctions related to basal ganglia may be one of the causes of attention-switching deficits seen in ASD and OCD. A finding supporting this idea is that repetitive behaviors, which are one of the most important phenomenological similarities between ASD and OCD and are suggested as one of the clinical manifestations of attention-switching disorders (Courchesne et al., 1994), are associated with basal ganglia dysfunction in both disorders (Subramanian et al., 2017; Isobe et al., 2022). These findings suggest that it would be useful to add functional imaging methods to studies investigating the mechanisms of attention-switching in these disorders.
On the other hand, according to our findings, attention-switching deficits are associated with a group of not-just-right experiences, indecisiveness, and hoarding rather than obsessive-compulsive symptoms such as cleaning, control, and unwanted thoughts. It has been suggested that the difference between OCD from anxiety disorders is that it shows symptoms similar to autism spectrum disorder (Ivarsson & Melin, 2008). Our findings suggest that this similarity may be valid for a subgroup of OCD patients showing these symptoms. Hoarding disorder has long been classified as a different disorder from OCD (American Psychiatric Association, 2013) due to its distinctive features and it has been reported that attention-related deficits may play a role in the pathophysiology of this disorder (Grassi et al., 2023). In this respect, a comparative study of attention deficits seen in hoarding disorder and ASD seems to be important in determining the similarities and differences of these disorders. It has been indicated that not just-right experiences may be closely related to the symptoms of sequencing, symmetry, and organization in OCD (Ferrão et al., 2012; Rosario et al., 2009; Smith et al., 2012; Starcevic et al., 2011). It has also been reported that these experiences are associated with the severity (Apa et al., 2022) and age of onset of the disorder (Rosario et al., 2009) and are common in parents of children with autism (Kloosterman et al., 2013). All these findings suggest that not-just-right experiences are an important sensory symptom in OCD and the relationship between OCD and autism. One speculation is that prolonged repetitions of an object or event in people with attention-switching deficits may lead to an increase in not-just-right feelings. It has been previously reported that increased repetitions may increase feelings of uncertainty about the repeated event (van den Hout & Kindt, 2003). On the other hand, indecisiveness, another symptom predicted by attention-switching deficit, has been associated with perfectionism and pathological responsibility in OCD. According to this idea, people with OCD who try to make the most accurate decision and not to make the wrong decision, especially in situations with high responsibility are unable to make decisions or postpone the decision-making process (Frost & Shows, 1993). It has also been previously reported that perfectionism and attention-switching problems may be related (Tonta et al., 2019).
Our finding that a frequent history of childhood upper respiratory tract infections (URTIs) with specific OCD symptom dimensions—such as checking, not-just-right experiences, and indecisiveness. This aligns with recent literature, including the nationwide cohort study (Orlovska et al., 2017), which found a heightened risk of OCD following streptococcal and non-streptococcal throat infections, implying the potential involvement of post-infectious immune mechanisms. Additionally, Pol-Fuster et al. (2025) noted that shared familial and genetic factors can partly account for the relationship between severe childhood infections and OCD, suggesting that early-life infections may predispose certain individuals to OCD. These results also suggested that early life infections may involve similar neuropsychiatric outcomes, aligning with the broader PANS (Pediatric Acute-onset Neuropsychiatric Syndrome) framework. To our knowledge, there is no study addressing the relationship between childhood infection and the risk of OCD or specific symptom dimensions in adulthood. Our dimension-specific findings suggest that such mechanisms might influence both of overall risk of OCD and its symptomatic expression in adulthood. While our results align with those from registry-based studies, the retrospective assessment of infection history via a single self-report item remains our limitation, introducing potential recall bias and a lack of pathogen-specific information. Future studies should consider clinically verified infection data, such as medical records, microbiological tests, or serological markers, as well as genetic factor within well-characterized clinical samples, to clarify the role of childhood infections in OCD etiology and symptomatology.
This study has several limitations. First, its cross-sectional design may limit the establishment of a conclusive causal relationship. Additionally, the use of self-reported symptom scales may introduce concerns about their validity and reliability. Drawing the sample from the general population may also limit the ability to generalize the results to clinical populations. Future longitudinal studies that utilize clinician-administered assessments in clinical groups are required to understand better the complex relationship between autistic traits and obsessive-compulsive symptoms. Furthermore, the absence of a systematic evaluation of potential confounding factors—such as current or past psychiatric history, substance use, and psychotropic medication—is another significant limitation of our study.
Conclusion
In conclusion, this study shows that attention-switching deficits, one of the ASD symptoms, can predict not just-right experiences, indecisiveness, and hoarding symptoms. Individuals with OCD symptoms may exhibit attention-switching deficits similar to those of individuals with ASD symptoms, suggesting a subgroup of OCD that shares features with ASD. Attention-switching deficits should be further investigated in terms of the relationship between ASD and OCD.
Footnotes
Author Contributions
Conceptualization: Filiz Karadag, Selim Tumkaya; Data curation: Filiz Karadag, Selim Tumkaya, Bengu Yucens; Formal analysis: Filiz Karadag, Selim Tumkaya, Bengu Yucens; Investigation: Filiz Karadag, Selim Tumkaya; Methodology: Filiz Karadag, Selim Tumkaya; Project administration: Selim Tumkaya, Aslihan Özdemir Yasaran, Volkan Akmehmetoglu; Resources: Selim Tumkaya, Aslihan Özdemir Yasaran, Volkan Akmehmetoglu; Software: Filiz Karadag, Selim Tumkaya, Bengu Yucens; Supervision: Filiz Karadag, Selim Tumkaya; Validation: Filiz Karadag, Selim Tumkaya; Visualization: Aslihan Özdemir Yasaran, Volkan Akmehmetoglu; Writing – original draft: Selim Tumkaya; Writing – review & editing: Filiz Karadag.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
Data Availability Statement
Data available upon request due to legal/ethical reasons. The data supporting the findings of this study are available from the corresponding author upon reasonable request.