
Abstract
Keywords
Introduction
Psychotherapeutic interventions should prioritize assisting individuals in managing their maladaptive trait expressions rather than attempting to alter their fundamental personality traits (Bach & Presnall-Shvorin, 2020). Maladaptive personality traits are risk factors for social and occupational difficulties, contribute to the onset and chronicity of mental disorders, and reduce treatment efficacy (Haehner et al., 2024, 2023; Hengartner, 2015; Fowler et al., 2022). The classical trait perspective posits that personality traits in adulthood are biologically based temperaments that remain stable over time and are not influenced by environmental factors (McCrae et al., 2000). However, more recent research suggests that personality traits can change over time (Hampson & Goldberg, 2020), particularly maladaptive traits (Bleidorn et al., 2022), and that such changes can occur in response to different types of interventions (Roberts et al., 2017).
In recent years, the conceptualization of personality pathology has shifted from categorical to dimensional models, as reflected in the Alternative Model for Personality Disorders (AMPD) of the DSM-5-TR (APA, 2022) and the ICD-11 (WHO, 2022). The AMPD framework conceptualizes personality disorders based on psychosocial functioning (Criterion A) and maladaptive personality traits (Criterion B). Within this framework, the Personality Inventory for DSM-5 (PID-5; Krueger et al., 2012) was developed to assess maladaptive personality traits, which are organized into five broad domains: Negative Affectivity, Detachment, Antagonism, Disinhibition, and Psychoticism. These domains encompass 25 specific trait facets (APA, 2022). Notably, these five maladaptive trait domains represent dysfunctional variants of the well-established personality dimensions in the Big Five model (Goldberg, 1993) or the Five-Factor Model (FFM; Digman, 1990). Following the development of the original PID-5, which consists of 220 items, several alternative versions have been created to facilitate assessment in different contexts. These include the PID-5-SF with 100 items (Maples et al., 2015), the PID-5-BF with 25 items (Krueger et al., 2013), the PID-5-BF+ with 34 items (Kerber et al., 2020), and the PID-5-BF+M with 36 items (Bach et al., 2020). In addition to serving as efficient screening tools for maladaptive personality domains, the brief versions plus offer the advantage of assessing Anankastia, a domain introduced in the ICD-11, thereby expanding their clinical and research utility.
However, maladaptive personality traits are not exclusive to personality disorders (Gonçalves et al., 2021; Von Schrottenberg et al., 2024), different levels of these traits are present in other mental health disorders and subclinical levels in a substantial proportion of the general population (Gleason et al., 2014). Personality traits exist on a continuum, meaning that all individuals can be placed along the spectrum of trait dimensions rather than being categorized as having or lacking specific traits.
Given this perspective, personality trait change can be conceptualized differently, with two primary approaches being widely examined: differential stability and absolute change (Hopwood & Bleidorn, 2018). Differential stability refers to the extent to which individuals maintain their relative rank on a given trait over time (Anusic & Schimmack, 2016), typically assessed using test-retest correlations, where effect sizes of 0.10 are considered small, 0.30 moderate, and 0.50 large (Cohen, 1988). In contrast, absolute change reflects systematic increases or decreases in trait expression within a population, regardless of individual rank-order stability (Wagner et al., 2016). This form of change is commonly quantified using Cohen’s d, where values of 0.20 indicate small changes, 0.50 moderate changes, and 0.80 large changes (Cohen, 1988).
A growing body of research suggests that personality trait change is not only possible but can be facilitated through structured interventions. A systematic review by Roberts et al. (2017) examined personality trait changes following different types of interventions, with a specific focus on clinical treatments. Their findings indicate that supportive therapy, Cognitive Behavioral Therapy (CBT), and psychodynamic therapy all yielded significant personality trait modifications, with CBT demonstrating slightly larger effect sizes. Notably, patients with anxiety and personality disorders exhibited the most substantial changes, particularly in reductions in neuroticism (Roberts et al., 2017).
CBT has evolved towards a process-based approach targeting underlying psychological mechanisms, thus aligning well with dimensional frameworks like DSM-5 AMPD and ICD-11, which conceptualize personality pathology as continuous rather than categorical (Hopwood, 2018; Pavlacic & Young, 2020; Sauer-Zavala et al., 2022). Its empirical grounding and cross-diagnostic flexibility further position CBT as suitable for examining dynamic personality changes over time (David et al., 2018; Hoffman et al., 2012).
Further supporting these findings, a randomized controlled trial (RCT) by Rek et al. (2022) comparing Schema Therapy (ST) and CBT found that maladaptive trait domains decreased throughout treatment regardless of the intervention type, indicating that both ST and CBT are effective in promoting pathological personality change. Another RCT (Niemeijer et al., 2023) investigated the association between changes in maladaptive personality domains and anxiety and depression symptoms in a clinical sample undergoing CBT. Their findings showed that decreases in Negative Affectivity predicted lower levels of both depression and anxiety symptoms, while reductions in Detachment were specifically associated with decreases in depression symptoms.
Despite numerous studies investigating personality trait change (Hopwood et al., 2009; Kennair et al., 2020; Norman et al., 2024; Roberts et al., 2017), there remains a significant gap in the systematic monitoring of maladaptive personality domains throughout psychotherapy (Kiel et al., 2024) to evaluate their impact on psychosocial functioning and clinical outcomes. The variability of personality expression across different time points and how these fluctuations may influence treatment trajectories remains underexplored (Roberts et al., 2017). Additionally, longitudinal studies examining personality trait change with larger clinical samples are still scarce (Hopwood & Bleidorn, 2018). Addressing this gap requires research designs that incorporate multiple assessment points and sufficient statistical power to capture within-person changes over time, ultimately contributing to the development of more targeted and effective interventions.
Aims, Research Questions & Hypotheses
Building on these considerations, this preregistered study Ocera et al. (2025) aims to investigate the relationship between CBT, maladaptive personality domains, and clinical outcomes through a longitudinal design with different time points. Specifically, it seeks to answer the following key research questions: (1) Do patients with higher maladaptive domains also have lower functioning and worse clinical symptoms? (1a) Do maladaptive personality domains decrease over time in the overall sample, indicating a general group-level change? (2) Do patients who exhibit higher maladaptive domains than their average also have worse functioning and clinical symptoms at the same time? (3) Do changes in maladaptive personality domains during therapy lead to improvements in functioning and symptom severity? (4) Do patients tend to change the personality domain they struggle with the most as a function of CBT?
We hypothesize that maladaptive personality domains, particularly Negative Affectivity, will be associated with poorer functioning and more severe clinical symptoms (Hengartner, 2015). Consistent with previous similar studies (Hashworth et al., 2022; Niemeijer et al., 2023; Torres-Soto et al., 2021), we expect all personality domains to significantly decrease over time. In particular, we anticipate that a reduction in Negative Affectivity will be associated with decreases in anxiety and depression (Niemeijer et al., 2023), while a reduction in Detachment will be specifically associated with decreased depressive symptoms (Niemeijer et al., 2023).
Methods
Ethics
The present study is part of the “Protocol for accessing and analyzing clinical data gathered at InTherapy for developing experimental research projects, epidemiological studies, and validation of new psychotherapy efficacy monitoring instruments for adults” a research project that aims to create an automated data collection protocol for conducting epidemiological studies, treatment efficacy verification, and instrument validation. The project has received ethical approval from the Sigmund Freud University - Wien Ethics Committee (Protocol Number: CD9THAHBC8SG@G91206). Participants will receive detailed written and oral study information before providing written informed consent. All procedures will be performed in accordance with Italian privacy law (Decree No. 196/2003) and the 1964 Helsinki Declaration and its later amendments.
Participants
Participants will be recruited from inTHERAPY a psychotherapy service specializing in CBT. Eligible individuals must be at least 18 years old, fluent in Italian, capable of providing informed consent, and have a diagnosed mental disorder. Individuals with no clinical diagnosis, organic brain disease, developmental disorders, or intellectual disabilities will be excluded. Recruitment will begin in June 2025 and will follow the clinic’s standard intake procedures (see Figure 1). inTHERAPY patients’ clinical path.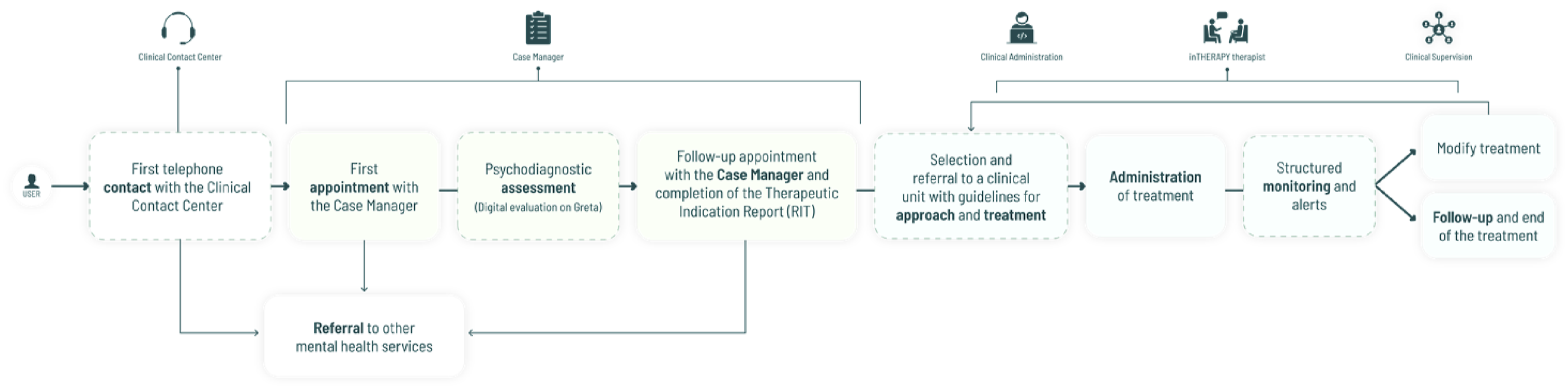
Covariates
Relevant covariates will be collected to account for potential confounding factors and better capture individual differences in baseline levels and change trajectories. These covariates include dropout status, therapy modality (in-person vs. online therapy), gender, age, and the presence or absence of a personality disorder diagnosis (as assessed with the SCID-5-PD; Somma et al., 2017). Additionally, information will be collected regarding whether the patient is concurrently receiving pharmacological treatment, as well as the therapist’s years of clinical experience and their specific CBT orientation (e.g., ACT, DBT, MBCT). They will be modeled as time-invariant predictors in the statistical analyses, allowing us to assess their influence on both the initial levels and the development of maladaptive personality domains and clinical outcomes over time.
Measures
During the psychodiagnostic assessment phase, patients will also be administered a questionnaire that contains basic medical information in a narrative format, which may be subject to further exploration in the feedback meeting. The following instruments will be administered to participants during the assessment phase and subsequently throughout psychotherapy for monitoring purposes. This set of instruments is part of the standard assessment and monitoring protocol used at inTHERAPY, which is committed to implementing the English Improving Access to Psychological Therapies (IAPT; Clark, 2011) model within a private Italian clinical setting.
Maladaptive personality Domains
As part of the initial assessment at baseline, the Personality Inventory for DSM-5 (PID-5; Krueger et al., 2012; Italian version Fossati et al., 2017) will be administered, as it is included in the standard psychodiagnostic protocol of the inTHERAPY clinical service at Studi Cognitivi. The PID-5 is a comprehensive 220-item instrument designed to assess maladaptive personality traits across five broad domains: Negative Affectivity, Detachment, Antagonism, Disinhibition, and Psychoticism. Each item is rated on a four-point Likert scale, ranging from 0 (very false or often false) to 3 (very true or often true). However, for longitudinal analyses, only the 36 items corresponding to the Personality Inventory for DSM-5 - Brief Form Plus Modified (PID-5-BF+M; Bach et al., 2020) will be extracted and scored from the baseline data.
To monitor changes throughout therapy, the PID-5-BF+M will be directly administered at subsequent time points. The PID-5-BF+M is a 36-item instrument that retains the five core maladaptive personality domains of the original PID-5 while also incorporating the Anankastia domain from the ICD-11 model of personality disorders. This version offers a practical and time-efficient assessment of personality pathology, making it suitable for repeated measurements throughout treatment. Each item is rated on a scale from 1 (very false or often false) to 3 (very true or often true).
Clinical Outcomes
Generalized Anxiety Disorder – 7 (GAD-7; Spitzer et al., 2006; Italian version Ivziku et al., 2018). The GAD-7 consists of 7 items, each assessing symptoms of anxiety (such as worry, difficulty relaxing, irritability) on a scale from 0 (never) to 3 (nearly every day). The total score provides a measure of anxiety severity, aiding in the identification of clinical risk levels.
Patient Health Questionnaire – 9 (PHQ-9; Kroenke et al., 1999; Italian version Rizzo et al., 2000). This nine-item tool is designed to screen, diagnose, and monitor depression. Items are on a 4-point Likert scale ranging from 0 (not at all) to 3 (nearly every day).
Work and Social Adjustment Scale (WSAS; Mundt et al., 2002; Italian version Rossi et al., 2005). The WSAS measures the impact of mental or physical health problems on an individual’s work and social life. The scale includes 5 items that assess levels of impairment in areas such as work, home management, social relationships, private life, and leisure activities. Each item is rated on a scale from 0 (not at all) to 8 (very severely), with higher scores indicating greater levels of difficulty or impairment. The total aggregate score will be used as a global index of psychosocial functioning.
Statistical Analyses
Descriptive statistics will be conducted to provide an overview of the sample characteristics and trends over time.
First, we will evaluate longitudinal measurement invariance for all repeated measures to ensure that observed changes over time reflect true change rather than changes in the meaning of the constructs. Configural, metric, and scalar invariance will be tested through stepwise confirmatory factor analysis. Changes in model fit will be assessed using ΔCFI and ΔRMSEA criteria, following Putnick and Bornstein (2016).
Second, before model estimation, we will assess potential multicollinearity among the instruments by computing Pearson correlations and Variance Inflation Factors (VIFs) for each predictor. VIF values exceeding 5 will be considered indicative of problematic collinearity (Kim, 2019; O’brien, 2007). If substantial multicollinearity is detected, we will explore model adjustments, including residualization or dimension reduction strategies, to ensure the stability and interpretability of parameter estimates.
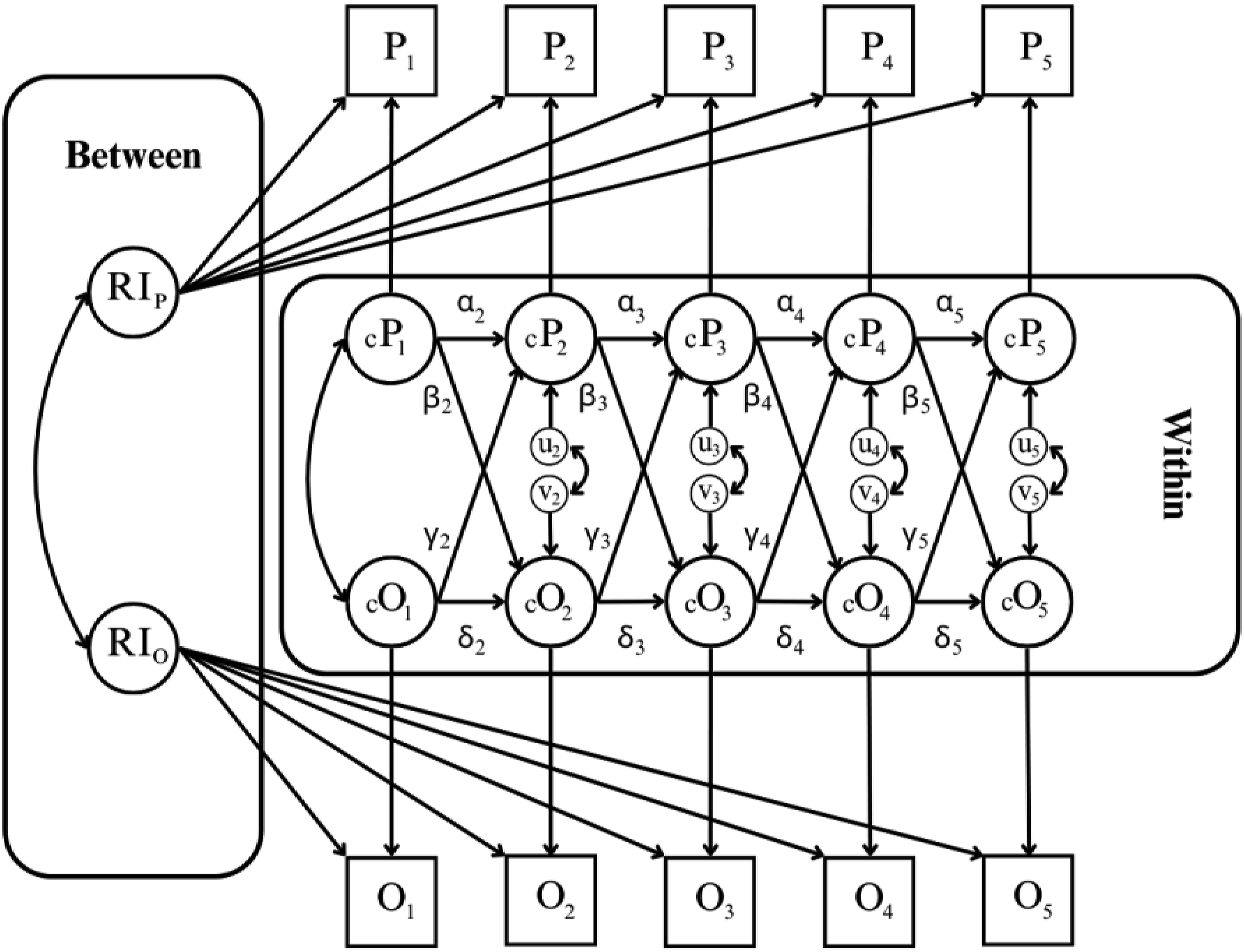
Inferential analyses will include Random Intercept Cross-Lagged Panel Models (RI-CLPM; Hamaker et al., 2015) to examine the reciprocal associations between maladaptive personality domains and clinical outcomes across multiple time points (Research Questions 1, 2 and 3). This modeling approach (Figure 2) distinguishes between stable between-person differences and within-person fluctuations over time, providing a more precise examination of dynamic relationships. Specifically: (1) Autoregressive associations (α, δ) assess the extent to which an individual’s deviation from their expected score on maladaptive personality domains (PID-5-BF+M) or clinical outcomes (GAD-7, PHQ-9, WSAS) at a given time point influences their score on the same variable at the subsequent measurement occasion. (2) Within-wave associations (correlation between u and v) capture the concurrent relationship between fluctuations in maladaptive personality domains and clinical outcomes within the same measurement occasion, reflecting short-term interdependencies. (3) Cross-lagged associations (β, γ) estimate the extent to which deviations from an individual’s expected score on one variable (e.g., maladaptive personality domains) predict subsequent deviations in another variable (e.g., clinical outcomes) across different time points while controlling for temporal stability. Illustration of the Random-Intercept Cross Panel Model (Hamaker et al., 2015) of the relationship between maladaptive personality domains and clinical outcomes during therapy across five waves. Note. P: personality domains; O: outcomes; α/δ autoregressive associations; u/v: within-wave associations; β/γ: cross-lagged associations.
We will estimate Latent Growth Curve Models (Duncan & Duncan, 2009) to examine group-level (absolute) change in maladaptive personality domains across five time points (Research Question 1a). This model is defined by two latent factors representing the intercept (initial level) and slope (linear rate of change) of each maladaptive personality domain over time.
Furthermore, we will compute latent test–retest correlations between the first and the last measurement occasions to estimate and compare the rank-order stabilities (differential stability) of maladaptive personality trait domains.
To address Research Question 4, we will conduct an exploratory analysis to examine whether patients tend to show the greatest reduction in the maladaptive personality domain that was most elevated at baseline. For each participant, we will identify the dominant personality domain, defined as the highest-scoring domain on the PID-5 at T1. We will then compare scores at T1 and T5 in the dominant domain to the mean scores at T1 and T5 observed in the remaining domains within each participant. A 2 × 2 mixed ANOVA (dominant vs. non-dominant traits and T1 vs. T5 PID-5 scores) will be used to determine whether the dominant traits show significantly greater change compared to non-dominant traits across participants.
To control for family-wise error rate due to multiple statistical comparisons across personality domains and outcome measures, Holm’s correction will be applied where appropriate (Aickin & Gensler, 1996). All analyses will be conducted in R using the lavaan package (Rosseel, 2012) for structural equation modeling and semTools (Jorgensen et al., 2022) for model evaluation. A significance level of α = .05 will be applied to all statistical tests.
Sample Size and Time Points
A priori power analysis for the RI-CLPM using Monte Carlo simulations (Mulder, 2022) could not be conducted, as no previous studies have examined the relationship between maladaptive personality domains (PID-5) and clinical outcomes (e.g., anxiety, depression, psychosocial functioning) using this modeling approach. However, several studies have applied this model with sample sizes ranging between 100 and 200 participants (Simkin et al., 2022). Therefore, we plan to recruit a minimum of 200 participants. The following time points will be considered: T1 (baseline assessment), T2 (after 3 months from the start of the treatment), T3 (after 6 months), T4 (after 9 months), and T5 (after 12 months). Quarterly assessments were chosen to balance the need for sufficient granularity in capturing within-person dynamics with the practical feasibility of longitudinal monitoring in a clinical setting. Moreover, compared to previous studies that typically assess only pre- and post-treatment outcomes (e.g., Hashworth et al., 2022; Kerber et al., 2021; Torres-Soto et al., 2021), the present design offers a more detailed view of trait and symptom trajectories over time.
Drop out and Missing Data Management
Given the longitudinal design, we anticipate some degree of dropout and missing data across the five assessment points. Missing data will be handled using Full Information Maximum Likelihood (FIML) estimation under the assumption of Missing at Random (MAR), which allows the use of all available data without imputing missing values and ensures unbiased parameter estimation when missingness depends only on observed variables (Cham et al., 2016). Additionally, where appropriate, imputation models will be used to ensure the robustness of estimates in analyses (Wijesuriya et al., 2025). These approaches will allow us to retain all available data and minimize bias due to attrition.
Location
Recruitment will be entirely voluntary. Patients will be recruited from inTHERAPY, the private clinical service of Studi Cognitivi, which specializes in CBT. inTHERAPY operates in multiple cities across Italy and offers both in-person and online psychotherapy services. All therapists at inTHERAPY are CBT-trained psychotherapists who have completed their four-year training at the Studi Cognitivi School of Specialization in Cognitive Behavioral Psychotherapy. The therapists will be responsible for recruiting participants among new patients initiating therapy, ensuring they meet the inclusion and exclusion criteria. They will explain the research project to potential participants and, if they agree to take part, obtain their informed consent.
Discussion
Maladaptive personality traits predispose individuals to treatment resistance, poor response, or relapse (Hengartner, 2015). Beyond treatment efficacy, maladaptive traits significantly impact quality of life and overall functioning (Hobbs et al., 2023). High scores on pathological personality dimensions are associated with lower quality of life (QoL) and greater disability/functional impairment across various domains. Individuals with elevated maladaptive traits are more likely to experience socio-occupational difficulties, such as unemployment, interpersonal conflicts, and early retirement due to disability. Additionally, they tend to exhibit lower recovery capacity and impaired social functioning, even while receiving treatment for other mental disorders (Hobbs et al., 2023). These findings underscore the clinical importance of assessing patients’ personality structures, as severe maladaptive traits can compromise treatment outcomes, contribute to residual symptomatology, and hinder functional recovery in daily life.
Maladaptive personality domains demonstrate a transdiagnostic nature, extending beyond personality disorders to a wide range of mental health conditions. For instance, patients with depressive or bipolar disorders tend to score higher on Detachment in the PID-5 compared to individuals with psychotic disorders or substance use disorders (Heath et al., 2018). Conversely, patients with alcohol use disorder exhibit higher Disinhibition and lower Psychoticism relative to other clinical groups (Heath et al., 2018). These variations suggest that pathological personality traits can be measured across different psychiatric diagnoses, delineating distinct personality profiles for each clinical population. Conceptually, this dimensional approach helps explain the high rates of comorbidity and diagnostic overlap observed in clinical practice. Traditional categorical models often struggle to account for the substantial co-occurrence of mental disorders, whereas a trait-based dimensional model more effectively captures underlying personality factors shared across different conditions (Hobbs et al., 2023).
Longitudinal monitoring of maladaptive traits and personality domains provides a crucial added value in psychotherapy. Tracking these traits over time allows clinicians to observe not only reductions in clinical symptoms but also the evolution of patients’ maladaptive personality profiles. From a clinical perspective, identifying changes in personality traits throughout therapy can help assess treatment progress more comprehensively. For instance, a lack of improvement in key personality traits may indicate the need to adjust therapeutic strategies, whereas reductions in maladaptive traits - beyond symptom reduction - may predict more stable treatment outcomes and a lower risk of relapse.
This study aims to investigate the role of maladaptive personality domains in CBT by examining their relationship with clinical outcomes and their trajectory over time. The strengths of this research include the use of a clinical sample in a naturalistic setting and the systematic monitoring of personality domains alongside clinical outcomes throughout therapy. However, certain limitations must be acknowledged. First, while we include a covariate indicating whether patients are undergoing concurrent pharmacotherapy, we do not have access to more detailed information such as medication type, dosage, or adherence. This limits our ability to fully isolate the effects of psychotherapy from those of medication and should be considered when interpreting the results. Additionally, the variability in therapeutic protocols adopted at inTHERAPY - including different third-wave CBT approaches such as Acceptance and Commitment Therapy (ACT), Dialectical Behavior Therapy (DBT) and Mindfulness-Based Cognitive Therapy (MBCT) - may introduce heterogeneity into the findings. Another significant challenge involves recruitment and longitudinal follow-up: patients with severe maladaptive traits may be more prone to dropping out of treatment (Berghuis, Bandell, & Krueger, 2021), potentially leading to selection biases.
Another limitation concerns the outcome measures selected for monitoring clinical change. Specifically, the PHQ-9 and GAD-7 - while widely used and well-validated - are strongly associated with the Big Five trait of Neuroticism (Navrady et al., 2017; Yang et al., 2023), which is related to the Negative Affectivity domain of the PID-5. Nonetheless, these instruments are embedded in routine clinical assessment protocols, including those adopted by inTHERAPY. Notably, both measures are also integral to the IAPT model implemented within the UK’s National Health Service, which systematically tracks treatment outcomes for depression and anxiety within stepped-care interventions (Clark, 2011). While the IAPT model does not account for comorbid personality pathology, it provides a scalable framework for outcome monitoring in large-scale clinical contexts. In line with this rationale, PHQ-9 and GAD-7 have been retained as outcome measures in the present study. Moreover, participants will be recruited from a private psychotherapy clinic in Italy, which may limit the generalizability of the findings to more diverse clinical populations, including those receiving care within public healthcare systems. Future studies should aim to replicate the present design in public or mixed-service contexts to enhance external validity. Finally, future studies would benefit from incorporating an additional follow-up time point after therapy completion to assess the stability of personality trait changes over time.
In conclusion, this study represents an important step toward a more nuanced understanding of the relationship between maladaptive personality domains and psychotherapy. It has practical implications for improving clinical interventions. Identifying key personality domains associated with treatment outcomes may facilitate the development of personalized therapeutic approaches, ultimately enhancing the effectiveness of psychotherapy for patients with maladaptive personality domains.
Footnotes
Authors’ Contributions
Conceptualization: AO, CJH, and GC; Methodology: AO, CJH, and GM; Writing - original draft: AO; Writing - review & editing: CJH, GM, RP, MF and GC. All authors contributed to the article and approved the submitted version.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
The present study is part of the “Protocol for accessing and analyzing clinical data gathered at InTherapy for developing experimental research projects, epidemiological studies, and validation of new psychotherapy efficacy monitoring instruments for adults”, a research project that aims to create an automated data collection protocol for conducting epidemiological studies, treatment efficacy verification, and instrument validation. The project has received ethical approval from the Sigmund Freud University - Wien Ethics Committee (Protocol Number: CD9THAHBC8SG@G91206).
Informed Consent
Participants will receive detailed written and oral study information before providing written informed consent. All procedures will be performed in accordance with Italian privacy law (Decree No. 196/2003) and the 1964 Helsinki Declaration and its later amendments.
Data Availability Statement
Data sharing does not apply to this article as no datasets were generated or analyzed during the current study.