
Abstract
This cross-sectional, psychometric validation and comparative analysis study investigates the associations between mental health and Psychological Capital (PsyCap) in persons with stuttering (PWS; n = 60) and fluent speakers (FS; n = 60), while validating the Tamil translations of the Mental Health Continuum-Short Form (MHC-SF) and Psychological Capital Questionnaire (PCQ). Exploratory Factor Analyses, Cronbach’s alphas, and item-total correlations were used to evaluate the scales with a sample size of 120 participants. The conducted factor analyses demonstrated that the translated MHC-SF aligns structurally with prior studies, as compared to the PCQ, which diverged in factor loadings. The study also applied Independent Samples t-tests, revealing significant differences among comparison groups. PWS reported lower mental health and PsyCap levels than FS, emphasizing psychosocial challenges as stuttering as inversely correlated with mental health and PsyCap dimensions—hope, self-efficacy, resilience, and optimism. In conjunction with offering preliminary validated tools, the study findings advocate for increased, holistic mental health approaches within traditional speech therapy to enhance the quality of life for PWS. Furthermore, this study underscores the importance of addressing cultural considerations when conducting future research and therapeutic practices with this population.
Stuttering is a speech disorder characterized by the consistent presence of disfluencies, often leading to discomfort such as embarrassment for those who stutter (Bloodstein et al., 2021). Despite advancements in understanding, etiology remains unclear, likely influenced by multifactorial causes, including genetic and environmental factors (Singh & Kumar, 2022). In tandem with speech disruptions, persons who stutter (PWS) frequently navigate negative societal perceptions, social isolation, and reduced quality of life (Boyle, 2020; Chu et al., 2022). These challenges underscore the need for holistic approaches that address both speech and psychological well-being.
Recent scholarship in positive psychology offers a valuable perspective for supporting PWS (Manivannan et al., 2023). Psychological Capital (PsyCap), encompassing hope, self-efficacy, resilience, and optimism, is a framework designed to evaluate and enhance well-being and buffer against stress in various populations (Luthans & Youssef-Morgan, 2017). Although researchers illuminate the positive association of acknowledging the strengths of PWS and their mental health (Boyle et al., 2019; Medina & Perez, 2022), exploring the usefulness of PsyCap in stuttering populations remains largely underexplored. This study assesses the psychological assets (i.e., HERO dimensions of PsyCap; Luthans et al., 2007b) and overall well-being (Keyes, 2009) of PWS. It also seeks to cross-culturally adapt and evaluate the Psychological Capital Questionnaire (PCQ) and the Mental Health Continuum – Short Form (MHC-SF) for Tamil-speaking individuals who stutter. In conjunction with creating a holistic profile of PWS, this study aims to provide meaningful dialogue emphasizing how strengths-based interventions and perspectives promote flourishing.
Review of Literature
Etiology of Stuttering
The etiology of stuttering remains elusive, with significant variability in its prevalence across populations, influenced by factors such as subpopulations (e.g., those with phonological or other compounding disorders or delays), gender, and age (Yairi & Seery, 2015). These variations have direct implications for understanding stuttering’s underlying causes. Stuttering is typically categorized as developmental or acquired, with potential origins ranging from organic pathology to environmental influences. For example, theorists’ conceptualizations continue to encompass psychogenic causes including lack of coordination between speech neurological subsystems (Yairi & Seery, 2015), to the role of parental misdiagnosis and communicative pressures of developmentally appropriate disfluencies (Bloodstein et al., 2021). Regardless of the specific origin, PWS often report the onset of stuttering as an encroaching sense of anticipation followed closely by feeling stuck or a loss of control (Tichenor & Yarus, 2018). The extensive body of theoretical and empirical evidence highlights the complex, multifactorial nature of stuttering, underscoring the need to address more than just the disorder itself.
Psychosocial Implications of Stuttering
The psychological impact of stuttering can be profound and lifelong. PWS report experiences of bullying, stigma, and low self-esteem, often conditioning avoidant behaviors and increased fears of negative evaluation (Blood & Blood, 2007; Mulcahy et al., 2008). Repeated social injuries reinforce psychological distress and contribute to the cyclical nature of speech disfluency.
Alongside general psychological distress, literature associates stuttering with a range of negative emotional experiences and affects, including guilt and shame (Boyle, 2020), embarrassment (Tran et al., 2021), and anxiety (Craig & Tran, 2014). Cognitive patterns also reflect internalized stigma. PWS often develop maladaptive beliefs surrounding their self-worth and societal value based on communication abilities (Iverach et al., 2016). For instance, a previously conducted study found that over eighty percent of their total participants (n = 987) perceived stuttering as an obstacle to educational and occupational achievement (Boyce et al., 2022). This finding is congruent with previous literature indicating the negative correlation of speech disfluency with probability of attending college and overall job satisfaction (Parsons et al., 2022). In response to these psychological and psychosocial implications, PWS might attempt to conceal their stuttering (e.g., avoiding speech, word substitutions) as an attempt to appear fluent (Gerlach et al., 2021).
Positive Psychological Outcomes
Few studies have explored positive psychological outcomes for PWS. For example, Manivannan et al. (2023) found that adults who stutter identified personal development, coping strategies, and support from others as positive outcomes of stuttering. Studies also show that knowledge of speech production can increase self-confidence in PWS (Crichton-Smith, 2002; Lucey et al., 2019). Plexico et al. (2019) suggest that resilience serves as a protective factor, promoting life satisfaction and buffering against reduced self-acceptance. Resilience and coping mechanisms have also been found to protect against diminished quality of life (Plexico et al., 2019). This emphasizes the need to not only address speech improvement but also to promote mental health through resources such as Psychological Capital, which can foster optimism and resilience in overcoming stuttering (Singh & Misra, 2009).
A positive psychology framework is crucial for addressing the complex nature of stuttering. Positive psychology focuses on strengths and well-being, shifting attention from deficits to assets, aligning with the multifaceted nature of stuttering (Seligman & Csikszentmihalyi, 2000). Central to this approach is well-being (Ryan & Deci, 2001), which includes both hedonic aspects (e.g., happiness) and eudaimonic aspects (e.g., meaning and self-actualization). Well-being is seen as the presence of positive functioning rather than merely the absence of illness (Keyes, 2002). Psychological Capital—comprising hope, efficacy, resilience, and optimism—emerges as a key resource that enhances both personal and professional performance (Luthans et al., 2007a). PsyCap promotes strengths that buffer against stress, contributing to individual flourishing and better life satisfaction (Avey et al., 2011a, 2011b; Luthans & Youssef-Morgan, 2017).
Purpose of the Study
To holistically understand the condition of individuals who stutter, it is crucial to consider their mental health status, including well-being and psychosocial factors that contribute to positive mental health. Despite significant research on the negative psychological outcomes of stuttering, there is comparatively less research on factors that may positively influence mental health from a positive psychological paradigm. This study aims to document a holistic profile of PWS, focusing on their current level of psychological assets (i.e., HERO dimensions of PsyCap; Luthans et al., 2007b) and emotional, social, and psychological well-being (Keyes, 2009). Additionally, the study seeks to cross-culturally adapt and psychometrically evaluate the Psychological Capital Questionnaire (PCQ) and the Mental Health Continuum – Short Form (MHC-SF) in Tamil for those diagnosed with stuttering. Given the complex interplay between language, culture, and psychological experience, adapting these scales for the Tamil-speaking population was essential to ensure linguistic clarity, cultural appropriateness, and conceptual validity. Cultural norms in Tamil communities influence how individuals experience and express constructs such as well-being, hope, resilience, and optimism, which may differ from Western perspectives embedded in the original versions of the PCQ and MHC-SF (Keyes, 2013; Luthans & Youssef-Morgan, 2017). Without cultural and linguistic adaptation, assessment tools may yield invalid results, particularly when psychological strengths are interpreted through a sociocultural lens that emphasizes collectivism, familial expectations, or spiritual values. For individuals who stutter, the added stigma and sociocultural silence around speech disorders in some Tamil-speaking communities necessitate the use of validated, culturally sensitive tools. Cross-cultural translation and normalization of the instruments, following best-practice guidelines, allows researchers and practitioners to produce more accurate findings and deliver interventions that are both evidence-based and culturally responsive (Sousa & Rojjanasrirat, 2011; World Health Organization [WHO], 2023).
Along with validating these translated measures, the study addresses the following research questions and hypothesis:
What factor structure arises for the Tamil versions of MHC-SF and PCQ?
What is the internal consistency of the T-MHC-SF and PCQ-T?
There is a significant difference in PsyCap and MHC-SF scores between PWS and FS.
Methods
The researchers completed the study investigation in three phases. First, we translated and adapted the Psychological Capital Questionnaire (PCQ; Luthans et al., 2007a) and Mental Health Continuum Short Form (MHC-SF; Keyes, 2009) to Tamil. Following the adaptation of the converted assessments, we followed the recommendations of Luthans et al. (2007b) and initiated an Exploratory Factor Analysis (EFA) to examine the construct validity and reliability of the translated versions. Lastly, we applied a non-randomized, cross-sectional research design to examine the potential statistical implications between native Tamil-speaking individuals who stutter and those who are fluent speakers. This methodological approach allows researchers to determine prevalence, or the percentage of individuals in a population with an observable characteristic at a specific timepoint (Mann, 2003).
Participants
The researchers conducted this study at a university located in the southern region of India. Following institutional ethics committee’s approval, we used purposeful and criterion-based sampling methods and recruited PWS from various clinics, hospitals, rehabilitation centers, and schools within the region. FS participants identified as residents of the same region. Inclusion criteria necessary to participate in this study involved the following: (a) participants must be native speakers of Tamil; (b) received a low impact to very severe stuttering diagnosis through the Stuttering Severity Instrument (SSI – 4) by a qualified Speech Language Pathologist (SLP); and (c) no known history of neurological, psychological, hearing, or other speech and language disorder. To minimize the risk of compounding variables between comparison groups, we also sought to maintain equal sample sizes and recruited individuals who concurrently did not hold a dual medical diagnosis or who took prescription medication. For a PWS to participate in this study, inclusion criteria also required that stuttering occurred as a gradual onset in childhood alongside reported normal speech and language development. Lastly, to avoid unintentional exploitation arising from the limited knowledge of social determinants of health and cultural factors, we attended to various aspects (i.e., language, literacy, and cultural barriers) during the recruitment and data collection phases (Fazal, 2021). Following these recruitment strategies, a final total of 120 Tamil-speaking participants agreed to partake in the study. The researchers divided individuals into two groups, PWS (n = 60), and FS (n = 60).
Regarding demographics of individuals who stutter, the majority self-identified as male (n = 37, 61.67%) with 23 (38.33%) identifying as female. The group’s mean age was 28.62 (SD = 6.08) with ages ranging from 19 to 48. Using the OASES assessment to comprehensively measure the negative impact that stuttering has on a person, two participants (3.33%) indicated a mild degree, 29 (48.33%) moderate, 19 (31.67%) severe, and with the remaining 10 participants (16.67%) falling into the very severe category. For level of education, 33 (55%) participants indicated completing an undergraduate degree, sixteen (26.67%) a postgraduate degree, and seven (11.67%) currently working towards obtaining either of the two degree paths. All other participants have received either their diploma (n = 2; 3.33%), Class 12th Certificate (n = 1; 1.67%), or High School Leaving Certificate (n = 1; 1.67%). Lastly, most individuals within this study’s group indicated being currently employed (n = 50; 83.33%), two (3.33%) identifying as a Home Maker, seven (11.67%) relaying currently not working, and one participant (1.67%) preferring not to answer.
Of those participating in this study without a stutter, 38 (63.33%) identified as male, with the remaining 22 (36.67%) self-identifying as female. Participants’ ages ranged from 19 to 46 with a mean age of 30.1 (SD = 7.74). All individuals (n = 60; 100%) received a low impact score on the OASES, indicating minimal to no concern for stuttering. Regarding level of education, a large majority relayed completing an undergraduate (n = 39; 65%) or postgraduate (n = 11; 23.33%) degree, while others designated either currently completing a post-secondary degree (n = 4; 6.67%) or having obtained their diploma (n = 2; 3.33%) or Class 12th Certificate (n = 1; 1.67%). Most participants specified current employment (n = 47; 78.33%), with one individual (1.67%) identifying as a Home Maker, 11 (18.33%) stating not being employed, and one (1.67%) preferring not to answer.
Instrumentation
Tamil - Mental Health Continuum - Short Form (T-MHC-SF)
The Tamil - Mental Health Continuum - Short Form (T-MHC-SF) is a self-administered questionnaire designed to assess wellbeing. This translated version was developed from the Mental Health Continuum - Short Form (MHC-SF; Keyes, 2009) and provides a nuanced understanding of an individual’s psychological functioning as the questionnaire rapidly captures both hedonic and eudaimonic mental health aspects (Keyes, 2013). The scale accommodates the complexity and diversity of human experiences as it delineates mental health along a continuum rather than offering a binary classification of either healthy or unhealthy. The structure of the T-MHC-SF assessment mirrors the MHC-SF (Keyes, 2013) and integrates 14 validated items measuring emotional (EWB; Diener et al., 1985), psychological (PWB; Ryff, 1989), and social (SWB; Keyes, 1998) wellbeing. Responding to questions referencing monthly frequency on a 6-point Likert scale (1 = Never; 6 = Every Day), individuals’ complete items such as, “How often in the past month did you feel that you had warm trusting relationships with others?” and “How often in the past month did you feel satisfied with your life?”. The assessment offers an overall wellbeing score and a score for each subdomain. Based on the collected scores, individuals are categorized as having flourishing, moderate, or languishing wellbeing.
The authors chose to adapt the MHC-SF to Tamil as the tool demonstrates adequate psychometric properties across countries, including the United States (Franken et al., 2018), Italy (Petrillo et al., 2014), South Korea (Lim, 2014), and South Africa (Keyes, 2009). For instance, Żemojtel-Piotrowska et al. (2018) conducted a multigroup confirmatory analysis of the MHC-SF from over 38 countries and found that the assessment maintained an average Cronbach’s alpha coefficient of .89 (n = 8066). For this study, the calculated Cronbach’s alpha coefficient of the total score was 0.968 (n = 120). A further description of the survey’s consistency and validity is provided in the subsequent results sections.
Psychological Capital Questionnaire - Tamil (PCQ-T)
Derived and translated from the Psychological Capital Questionnaire (PCQ; Luthans et al., 2007a), the Psychological Capital Questionnaire – Tamil (PCQ-T) is a cross-cultural adaption of the PCQ that helps evaluate respondent’s positive psychological Capital, a developmental state that emphasizes positivity in an individual. The self-reported assessment consists of 24, validated and established items categorized into four scales: hope (Snyder et al., 1996), self-efficacy (Luthans et al., 2007a), resilience (Wagnild & Young, 1993), and optimism (Scheier & Carver, 1985) Each subdomain consists of six items that are answered using a 6-point Likert scale ranging from (1 = strongly disagree; 6 = strongly agree). Confirmatory factor analysis of the PCQ demonstrated high factorial and discriminant validity (Luthans et al., 2007b). Following the original publication of the study, the PCQ has been adapted and developed to cater to diverse populations and contexts. For instance, researchers continue to translate and examine the validity of the PCQ in diverse languages and nationalities such as Portuguese (Antunes et al., 2017) and Polish (Lipinska-Grobelny & Zwardón-Kuchiak, 2023). Results from these two studies support satisfactory factorial validity, internal consistency, and construct validity of the translated versions. For the present study, the PCQ-T yielded an internal consistency reliability of .952 (n = 120).
Data Collection Procedures
To begin the cross-cultural adaption of the PCQ and MHC-SF to Tamil, we followed the procedures and recommendations of provided by the World Health Organization (WHO, 2023) and affiliated research (Sousa & Rojjanasrirat, 2011). Specifically, a psychologist, who is a native speaker of Tamil and proficient in English, independently translated both assessments to the Tamil language. An expert panel comprised of two additional bilingual psychologists then analyzed the translation for any discrepancies. Following these initial steps, the assessments were blind translated back to English by two linguists and psychologists. The four retranslated English versions of the assessments were compared with the original version. Of the adaptions, the items that were translated most accurately from Tamil to English and then back to Tamil were selected for inclusion in the final version of the questionnaire. To maximize cultural relevance and maintain psychometric rigor, two psychologist and five SLPs rated the resulting Tamil versions for consensus. All questions that met group agreement were placed in the final translated assessments, while the panel of experts met to resolve discrepancies in remaining scale items. This included engaging in a collaborative and structured discussion process to agree on item phrasing and refinement. This sequence resulted in the final T-MHC-SF and PCQ-T versions that were used in the present study.
After the translation of the two assessments, participants in the comparison groups read and responded to the T-MHC-SF and PCQ-T questionnaires. A subjective translator was available to clarify and explain any ambiguities before the participants began the assessment to address any potential biases or misunderstandings in the translated questionnaire items. Participants completed 14 questions in the T-MHC-SF, and 24 questions in the PCQ-T questionnaires. After all individuals submitted their questionnaires, the researchers compiled responses for data analysis.
Data Analysis
This cross-sectional, psychometric validation and comparative analysis study utilized EFA and Independent Samples t test to validate the translated MHC-SF and PCQ while also examining potential differences between PWS and fluent speakers. With the intention of ensuring that the translated versions measure the same construct factors as the original assessments, we intentionally chose EFA as a methodological approach as cultural and linguistic differences might influence item loading and factor structure (Caro et al., 2014). When conducting an EFA, it is recommended to recruit at least five participants per assessment item (Costello & Osborne, 2005). Based on the number of T-MHC-SF and PCQ-T items, we recruited a total of 120 native Tamil speakers. This sample size met group data saturation needed to infer a medium effect size (d = .5; Cohen, 1992) with a 95% confidence interval for a one-tailed, independent samples t test (n = 59). We also utilized G*Power to verify our requited number of participants. The software tool paralleled our set sample size with a power level to .85, indicating an 85% likelihood of detecting an existing effect. After calculating the required sample size, we uploaded and evaluated collected assessment data through the Statistical Package for Social Sciences (SPSS; Version 24). We screened the completed T-MHC-SF and PCQ-T for missing items. After verifying that all study participants had completed both assessments, we scored them in congruence with their respective test manuals. T-MHC-SF and PCQ-T scores were calculated by taking the means for each respective subscale and total assessment items. After scoring the two instruments, we initiated Bartlett’s Test of Sphericity and Kaiser-Meyer-Olkin Test (KMO) to determine data suitability for conducting an EFA. These tests provide a measure of the statistical probability that the correlation matrix for each scale has significant correlations among its components. For the T-MHC-SF, both the Barlett’s Test (χ2 = 1607.915, df = 91, p < .001) and KMO (=.96) conveyed sufficient common variance to justify an EFA. Similarly, the PCQ-T demonstrated good common variance with a Barlett’s Test of (χ2 = 1922.217, df = 276, p < .001) and KMO measure of = .931.
To answer the second research question regarding internal consistency, we determined Cronbach’s alpha for each assessments’ total and subscales, regardless of items that may have either been eliminated or factor loaded differently following the EFA. This avenue provides clarity surrounding the reliability of the cross-cultural adaption and how participants answer items. Following the recommendations of Nunnally (1978), an alpha value of >.7 is considered acceptable while a value of >.9 indicating excellent internal consistency. Additionally, we analysed the item-total correlations to identify any items that did not correlate well with the total scores.
Lastly, we conducted a one-tailed independent samples t test to compare the mental health and psychological capital of PWS and fluent speakers. To measure the outcome variables of collected T-MHC-SF and PCQ-T assessments between these two groups, all data was subjected to statistical analysis using Levene Test for Equality of Variances and t test.
Results
After observing the overall significance of the correlation matrix, we initiated the EFA using a principal axis factoring analysis and Promax oblique rotation for each assessment. Principal Axis Factoring identifies constructs by emphasizing shared variance among items, while oblique rotation allows for an underlying relationship between factors, reflecting their potential interconnections. We used a minimum factor loading criterion of .40 to examine for moderate correlations between factors and items. Factor loading is a statistical method that helps to clarify complex variables or items and explains the relationships among these underlying constructs (Tavakol & Wetzel, 2020). Additionally, we assessed the communality of the T-MHC-SF and PCQ-T, indicating the variance in each dimension. For the T-MHC-SF, all communalities were over .64, inferring acceptable levels of explanation. In a similar way, items of the PCQ-T had communality values over .64, except for question 16, with a value of .151. The lower proportion of variance of this resilience subscale item suggests that the question does not strongly contribute to the overall factor structure therefore prompting potential removal from the scale.
T-MHC-SF
Exploratory Factor Analysis
Pattern Factor Loadings for Exploratory Factor Analysis of the Tamil-Mental Health Continuum-Short Form (N = 120).
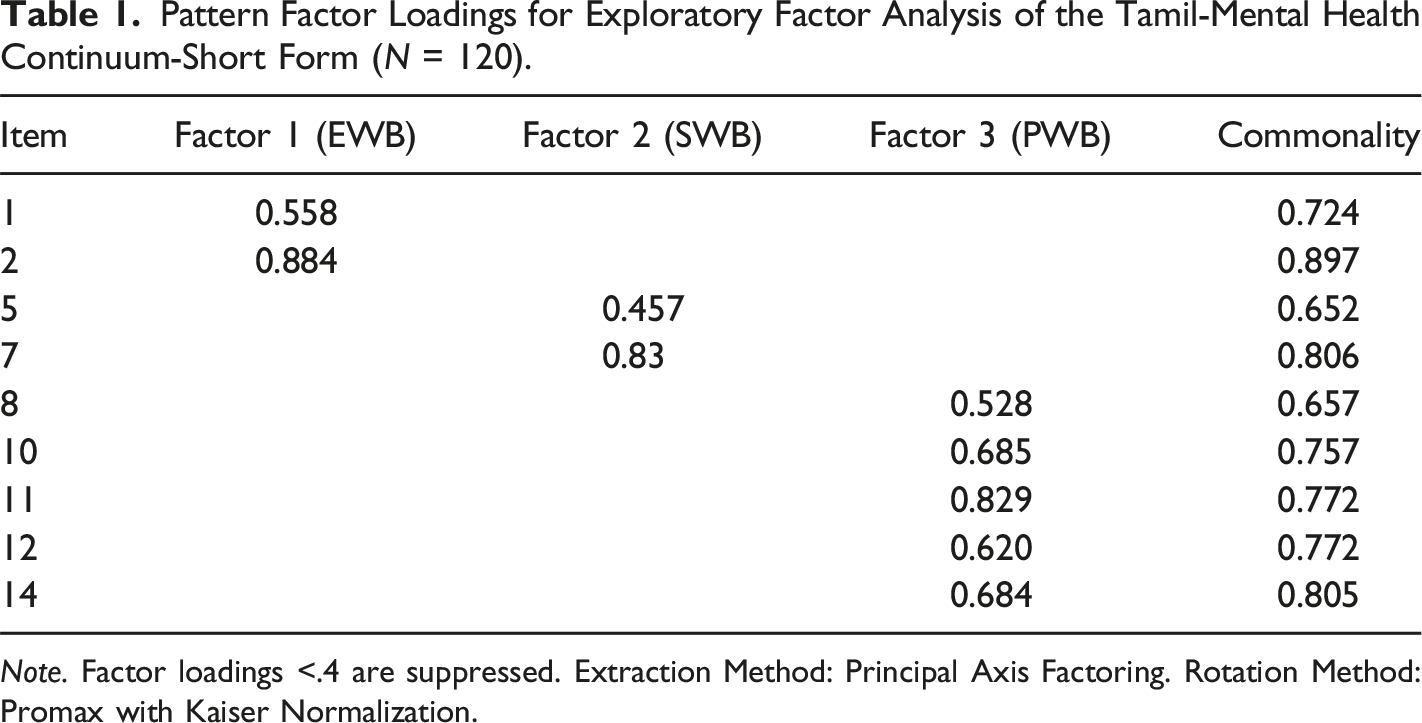
Note. Factor loadings <.4 are suppressed. Extraction Method: Principal Axis Factoring. Rotation Method: Promax with Kaiser Normalization.
Reliability
We assessed T-MHC-SF total and subscale internal consistencies using Cronbach’s Alpha. Calculating Cronbach’s Apha assists in comparing the amount of shared variance among items, helping illuminate the scale’s reliability. For the T-MHC-SF, the total scale demonstrated high internal consistency (α = .968). Each subscale also indicated good reliability with emotional wellbeing (α = .903), social wellbeing (α = .914), and psychological wellbeing (α = .938). From the gathered results, we consider the T-MHC-SF total scale and affiliated subscales as reliable as high alpha values were observed.
To further evaluate the internal consistency, we examined the item-total correlations for with the total scale to measure the degree to which each item correlates with the total score of its respective subscale. We found that all T-MHC-SF items exhibited strong correlations, with the lowest item being question 10 (.764), which measures psychological wellbeing. The item-total correlation analysis supports the reliability of our scale’s subscales, affirming internal homogeneity and that the assessment items contribute meaningfully to their respective constructs.
Between-Subjects Comparison
After analyzing the Exploratory Factor Analysis and reliability measures of the T-MHC-SF, we conducted an independent samples t test to compare the overall mental health scores, and cluster scores (i.e., EWB, SWB, PWB) of PWS and FS. Between the two groups, results showed statistically significant differences for all observed comparisons. Specifically, each mental health cluster illustrated significant differences in the EWB scores of PWS (M = 10.37, SD = 2.68) and FS (M = 15.05, SD = 1.34); t (118) = −12.095, p < .001, Cohen’s d = 2.21; SWB scores of PWS (M = 17.13, SD = 3.88) and FS (M = 24.62, SD = 2.72); t (118) = −12.213, p < .001, Cohen’s d = 2.24; and PWB scores of PWS (M = 20.00, SD = 4.24) and FS (M = 29.65, SD = 2.8); t (118) = −14.699, p < .001, Cohen’s d = 2.68. Similarly, FS scored higher total scores on the T-MHC-SF (M = 69.57, SD = 9.83) as compared to PWS (M = 49.21, SD = 11.43); t (118) = −14.741, p < .001, Cohen’s d = 1.85. Results gathered indicate that as a variable, stuttering affects Tamil individuals’ emotional, social, and psychological wellbeing.
PCQ-T
Exploratory Factor Analysis
Pattern Factor Loadings for Exploratory Factor Analysis of the Psychological Capital Questionnaire - Tamil (N = 120).
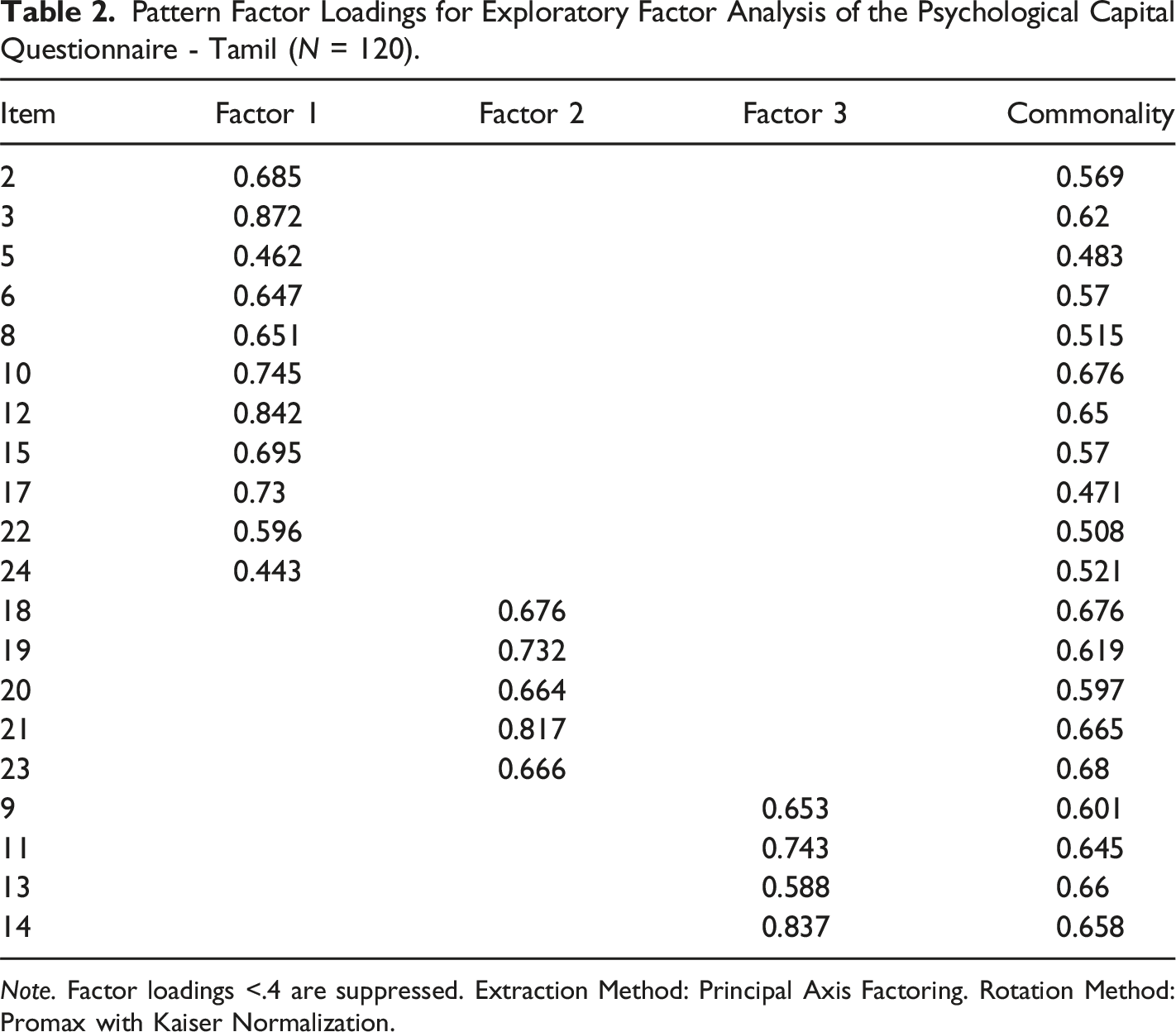
Note. Factor loadings <.4 are suppressed. Extraction Method: Principal Axis Factoring. Rotation Method: Promax with Kaiser Normalization.
Reliability
Observing Cronbach’s alpha, we assessed the internal consistencies of the PCQ-T total and subscales. Before analyzing the data, we attended to the assessment’s three reverse-coded items and verified that all variables were positively directed. The total scale yielded a strong internal consistency reliability of (α = .952). Each subscale also indicated good or moderate reliability with efficacy (α = .873), hope (α = .861), resilience (α = .717), and optimism (α = .878).
We then examined the item-total correlation of the PCQ-T. We found that most items exhibited strong correlations with their respective subscale totals, indicating good internal homogeneity and consistency. For example, items within efficacy showed item-total correlations ranging from 0.63 to 0.779, hope ranged from 0.655 to 0.767, resilience from .59 to .744, and items gauging optimism ranged from 0.655 to 0.751. While these findings suggest that items within each subscale are cohesive and commonly measure the respective theme, item 16, which helps measure a participant’s resilience, showed a lower item-total correlation of .09. This lower correlation suggests that the specific item may not effectively differentiate between high- and low-performing participants. If removed, the alternative Cronbach’s alpha would increase slightly to (α = .957).
Between-Subjects Comparison
When examining potential differences in PCQ-T total and HERO dimensions, FS obtained statistically significant scores in all categories when observed to PWS. Those designated as fluent speakers indicated a meaningful difference in psychological capital scores (M = 114.12, SD = 14.07) compared to PWS (M = 92.20, SD = 18.11); t (118) = −7.401, p < .001, Cohen’s d = 1.35. Similarly, significant differences were noted in HERO dimensions including scores of hope of FS (M = 28.87, SD = 2.50) and PWS (M = 24.02, SD = 5.23); t (118) = −6.479, p < .001, Cohen’s d = 1.18; self-efficacy scores of FS (M = 30.12, SD = 11.78) and PWS (M = 22.13, SD = 4.67); t (118) = −4.878, p < .001, Cohen’s d = .89; resilience scores of FS (M = 26.85, SD = 2.48) and PWS (M = 22.92, SD = 4.59); t (118) = −5.828, p < .001, Cohen’s d = 1.07; and optimism scores of FS (M = 28.28, SD = 2.57) and PWS (M = 23.1, SD = 5.19); t (118) = −6.888, p < .001, Cohen’s d = 1.26. Results obtained from the independent samples t test of the PCQ-T suggests that as a group, PWS hold a decreased positive psychological state of development and perception of internal resources compared to FS.
Discussion
This study aimed to examine the psychological well-being of PWS by analyzing their psychological assets, such as HERO, and their emotional, social, and psychological well-being. We also evaluated the cross-cultural adaptation and reliability of the PCQ and the MHC-SF for Tamil-speaking individuals. The findings provide a preliminary understanding of how stuttering impacts mental health, particularly within the Tamil-speaking population.
The EFA revealed that the T-MHC-SF factor structure aligns with previous studies, reinforcing the three-factor model across different cultural contexts (Petrillo et al., 2014; Pir et al., 2023). Nine of the original 14 items maintained their connections to their respective factors (EWB, SWB, PWB), but five items were excluded due to low factor loadings, suggesting they did not adequately reflect the constructs. The retained items demonstrated strong loadings, supporting the construct validity. Notably, item eight, intended to measure social coherence, loaded onto social well-being instead of psychological well-being, which may reflect cultural differences in how the construct is interpreted.
The EFA of the PCQ-T supported the original four-factor PsyCap model (Luthans et al., 2007a), but further analysis led to a three-factor solution, with overlap among dimensions. While the structure largely aligns with the theoretical model, it suggests cultural nuances may influence how participants interpret certain constructs, particularly optimism and resilience, which may overlap in this context. Further research is needed to explore whether a hierarchical factor structure is more appropriate in this cultural context (Avey et al., 2008; Lupsa & Virga, 2018).
Next, comparisons of PWS and FS revealed that PWS tend to perceive lower psychological well-being across all measured dimensions. FS scored higher than PWS on both the T-MHC-SF and PCQ-T, indicating a stronger sense of overall well-being and psychological resources. FS reported higher psychological capital scores across all HERO dimensions, and rated their mental health more positively, with significant differences observed in emotional, social, and psychological well-being, highlighting the negative impact of stuttering on mental health. These results align with previous studies showing that stuttering negatively affects personal relationships, work dynamics, personality, education, physical health, and self-acceptance (Bleek et al., 2012; Craig et al., 2009; Yaruss & Quesal, 2006). The impact on these aspects can significantly lower life quality for individuals who stutter.
Implications
Implications for Mental Health Professionals
The findings of this study have substantial implications for mental health professionals working with PWS. The lower PsyCap and mental health scores observed in PWS underscore the importance of incorporating evidence-based psychological interventions into treatment. Positive psychology interventions, such as PsyCap training programs, have been shown to improve well-being, resilience, and emotional functioning in various populations (Avey et al., 2008; Luthans et al., 2007a). Specifically, interventions that target the HERO components can buffer against stress and improve self-regulation and performance. Additionally, psychoeducation initiatives can help individuals who stutter better understand the relationship between stuttering, mental health, and their psychological strengths, enabling them to manage their condition more holistically.
Evidence-based therapeutic methods such as Acceptance and Commitment Therapy (ACT) and Cognitive Behavioral Therapy (CBT) are particularly promising for PWS. ACT has demonstrated efficacy in reducing anxiety and improving psychological flexibility, which are often compromised in individuals who stutter due to chronic psychosocial stress (Ataabadi et al., 2024; Beilby et al., 2012). CBT, likewise, has been effective in reducing social anxiety and enhancing self-perception among individuals with fluency disorders (Craig & Tran, 2014; Menzies et al., 2008). These therapies can serve as foundational approaches, particularly in severe cases where psychological distress is more pronounced.
Given the inverse correlation between stuttering severity and PsyCap scores, mental health professionals should integrate stuttering severity assessments that uses both subjective (e.g., self-reports) and objective (e.g., frequency counts) tools into intervention planning. Therapy goals can then be appropriately sequenced: beginning with anxiety management and confidence-building in severe cases and progressing to the enhancement of psychological strengths as fluency and comfort increase.
Furthermore, intervention intensity and modality should be customized to individual needs. For example, those with mild or moderate stuttering may benefit from group-based positive psychology programs or resilience workshops, while individuals with severe stuttering may require frequent one-on-one therapy sessions and trauma-informed care. Ongoing monitoring of both stuttering severity and PsyCap development is essential to guide treatment progression. A flexible, individualized approach that addresses the psychological and communicative dimensions of stuttering can ultimately enhance both therapy engagement and quality of life.
Implications for Allied Health Professionals
For allied health professionals, particularly SLPs, these findings highlight the importance of a comprehensive approach to stuttering treatment. Addressing the psychological well-being of PWS in addition to speech fluency is critical. Collaborative care models involving mental health professionals can integrate both speech and mental health support, thereby providing a more holistic intervention framework. Tailoring interventions based on stuttering severity is also essential, with more intensive support for severe cases.
Other allied health professionals, such as occupational therapists (OTs), physical therapists, and special education teachers, can also play key roles. For instance, OTs can support functional communication in various settings and offer stress management techniques, such as mindfulness or relaxation exercises, which positively influence PsyCap and overall well-being (Luthans et al., 2007a). Physical therapists can address physical tension associated with stuttering by teaching relaxation techniques to reduce stress-related exacerbations. Special education teachers can foster inclusive classroom environments and provide tailored learning strategies to accommodate the needs of children with stuttering, collaborating with SLPs to align interventions effectively. By adopting a multidisciplinary, tailored approach, allied health professionals can address both the speech-related and psychological challenges of PWS, enhancing their overall quality of life.
Implications for Policy
In light of the findings, there is a critical need for healthcare policies that recognize and support holistic interventions for PWS. Instead of fluency-based outcomes, health care policies must emphasize integrating mental health and PsyCap development into standard care (Constantino, 2023a, 2023b; Plexico et al., 2019). Policymakers should advocate for interdisciplinary funding opportunities that encourage collaboration between SLPs, psychologists, occupation therapists, counselors, as well as other related allied health professionals (Croft & Byrd, 2020; Yaruss & Quesal, 2004). Insurance reimbursement policies could also be expanded to cover psychological assessments and positive psychology interventions as part of comprehensive treatment plans (Luthans & Youssef-Morgan, 2017). Additionally, public health initiatives should include awareness campaigns that reduce stigma and promote strengths-based understandings of stuttering, further supporting societal inclusion and mental well-being (Boyle, 2020; Gerlach et al., 2021).
Limitations
Several limitations are worth considering following the implementation of this study. While the non-randomized sample size of 120 participants is adequate for EFA (Costello & Osborne, 2005), it may impact the robustness and generalizability of the factor structure. A larger participant pool gathered from randomized sampling methods would enhance statistical power, ensure more stable factor solutions, and minimize the potential of sampling bias (Khorsan & Crawford, 2014). Increasing the collected data would also assist in evaluating whether the translated scales meet the required criteria for further confirmation testing (i.e., Confirmatory Factor Analysis). In addition to the gathered sample, although FS shared homogeneity with minimal to no stuttering following the OASES, PWS participants were divided into various severities of stuttering. The lack of consistency among severity of PWS might have created an unintentional variable, impacting study results. For instance, literature relays how stuttering severity impacts perceived differences in the quality of life of PWS including occupation (Parsons et al., 2022), education (Khasawneh, 2021), and physical health (Jacobs et al., 2021). The use of self-report measures also raises concerns about response biases, such as social desirability and recall bias, potentially impacting data accuracy. In addition to the methodological limitations noted above, the study may be influenced by potential confounding variables that were not controlled for during data collection. For instance, social anxiety may have independently affected participants’ psychological capital and mental health scores, thereby complicating the interpretation of group differences (Iverach et al., 2016). Similarly, participants’ prior therapy experiences, including speech therapy or psychological counseling, could have influenced their current levels of resilience, optimism, and self-efficacy. Other unmeasured factors, such as socioeconomic status, family support, or comorbid conditions like depression or learning difficulties, may also have had a moderating effect on the outcomes. Future studies should incorporate measures that assess and statistically control for such variables to provide a more nuanced understanding of the relationship between stuttering, mental health, and PsyCap.
Additionally, despite employing translation and back-translation procedures (Sousa & Rojjanasrirat, 2011; WHO, 2023), cultural and linguistic differences may have influenced participants’ and researchers’ interpretations, leading to semantic misinterpretations. Given that the present findings are established from limited translated comparisons, the results should be viewed with caution as prospective literary inaccuracies could prompt question confusion or the participant feeling culturally misunderstood (Fazal, 2021), ultimately influencing the validity of the translated scales. The homogeneity of the sample further limits the generalizability of the findings to other Tamil-speaking populations or demographic groups.
Other methodological constraints include the cross-sectional design, preventing causal inferences and the examination of temporal relationships between psychological constructs. For instance, while internal consistency of the assessments was evaluated, test-retest reliability and other forms of reliability could not be determined. Moreover, the use of EFA to explore the T-MHC-SF and PCQ-T factor structures necessitates cautious interpretation, as EFA relies on subjective decisions regarding rotation methods and factor retention. Unlike other factor analysis methods that test hypothesized models, EFA primarily uncovers data patterns, and does not examine for pre-existing theoretical models. Further research is needed to validate the factor structures of the initial and translated assessments, and to better understand their reliability and validity across diverse populations.
Recommendations for Future Research
Future research should also explore the long-term impact of PsyCap development in PWS using longitudinal study designs. Such research can track changes in hope, efficacy, resilience, and optimism over time in relation to stuttering severity and mental health outcomes. This would provide empirical support for the incorporation of PsyCap-enhancing interventions into routine care. Additionally, Research should also evaluate the effectiveness of interventions aimed at enhancing PsyCap in PWS, with randomized controlled trials comparing approaches such as cognitive-behavioral therapy (CBT), positive psychology exercises, and group therapy. Additionally, future studies could compare the mental health and PsyCap of PWS with other groups facing communication challenges (e.g., individuals with aphasia or voice disorders) to determine whether the findings are specific to stuttering or applicable to a broader population.
Next, a larger sample size and confirmatory factor analysis (CFA) are recommended for further validation of the T-MHC-SF and PCQ-T, assessing their fit with the foundational model and factorial structure. Investigating the correlation between a PWS’s OASES severity score and their mental health could provide a further nuanced understanding of the disorder’s psychological impact. Qualitative researchers should explore the lived experiences of PWS, using interviews or focus groups to delve into how stuttering uniquely impacts their mental health and PsyCap, while simultaneously exploring specific coping strategies PWS find most effective.
Additionally, future studies should investigate the implementation and outcomes of policy changes that promote integrated and holistic care for PWS. For example, research could examine how multidisciplinary treatment models that involve collaboration among SLPs, mental health professionals, and allied health providers influence therapy adherence, patient satisfaction, functional communication, and overall quality of life. Moreover, incorporating stakeholder perspectives, such as those of clinicians, policymakers, individuals who stutter, and advocacy groups, can offer a more comprehensive understanding of the practical barriers and facilitators to integrated care. This type of participatory research enhances the relevance and feasibility of proposed interventions and informs policy recommendations that are culturally responsive, contextually grounded, and more likely to be adopted and sustained over time. Lastly, exploring the influence of sociodemographic and cultural factors on the relationship between stuttering, mental health, and PsyCap would add depth to the findings. Factors such as age, gender, and ethnicity warrant examination, potentially through cross-cultural studies to understand variations in PWS from diverse backgrounds.
Conclusion
This study aimed to understand the psychological capital and overall well-being of Tamil-speaking individuals who stutter, focusing on a variety of constructs such as the HERO dimensions. Our intention of exploring these constructs was based in shifting away from a deficit-based narrative to a positive psychological framework, highlighting the psychological strengths contributing to a flourishing mental health. The gathered findings provide nuanced understanding of how communication difficulties impact the perceived mental health and psychological strengths of PWS, and offer preliminarily reliability and validity evidence of the T-MHC-SF and PCQ-T. These tools enable culturally relevant assessments of mental health among Tamil-speaking individuals, especially those who stutter. While additional research is warranted to ensure psychometric properties, the study emphasizes incorporating PsyCap-based interventions in mental health and speech therapy, encouraging clinicians to prioritize hope, self-efficacy, resilience, and optimism over fluency to enhance therapeutic outcomes.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.